1. Introduction
Muscular variations are common in the human body and are well-documented in the literature. These variants occur within the normal range of possibilities that may be comprised of morphometric changes, supernumerary elements, consistency and spatial orientation [
1,
2]. Muscular anomalies are much rarer, and anatomists observe them during routine cadaveric dissection or surgeons discover them inadvertently during surgical procedures [
3]. Anomalies are typically asymptomatic and may go unnoticed during the individual’s life. With the development of non-invasive imaging techniques and the increase in cadaveric studies, however, anatomic anomalies are being detected more frequently [
2].
In this case study, we observed a rare unilateral anomalous muscle in the left posterior neck of a human cadaver. It was located deep to the rhomboid muscles and coursed superior and medial to the serratus posterior superior (SPS) muscle. In addition, we found differences in the cervical origins of the right and left levator scapulae muscles (LSMs), resulting in muscular asymmetry in this individual. This anomalous muscular development is uncommon, and we were unable to find a description of such a case in the literature. Therefore, it is important to provide a detailed description of this rare anomalous muscle.
2. Materials and Methods
During cadaveric dissection, we detached the superficial extrinsic back muscles, including the trapezius, latissimus dorsi, and the rhomboid muscles from their proximal attachments and reflected them. The levator scapulae muscle was not reflected. This exposed the intermediate extrinsic back muscles, including the serratus posterior superior (SPS). We detached the SPS from the spinous processes at the C7-T2 vertebral level. We observed the anomalous muscle during the detachment of the SPS at its proximal attachments. Delicate dissection of the anomalous muscle allowed us clear definition and further examination of its attachment sites. We detached the deep intrinsic muscle, the splenius muscle, proximally from the nuchal ligament and spinous processes of C7-T6 vertebrae. We conducted this dissection bilaterally.
3. Case Report
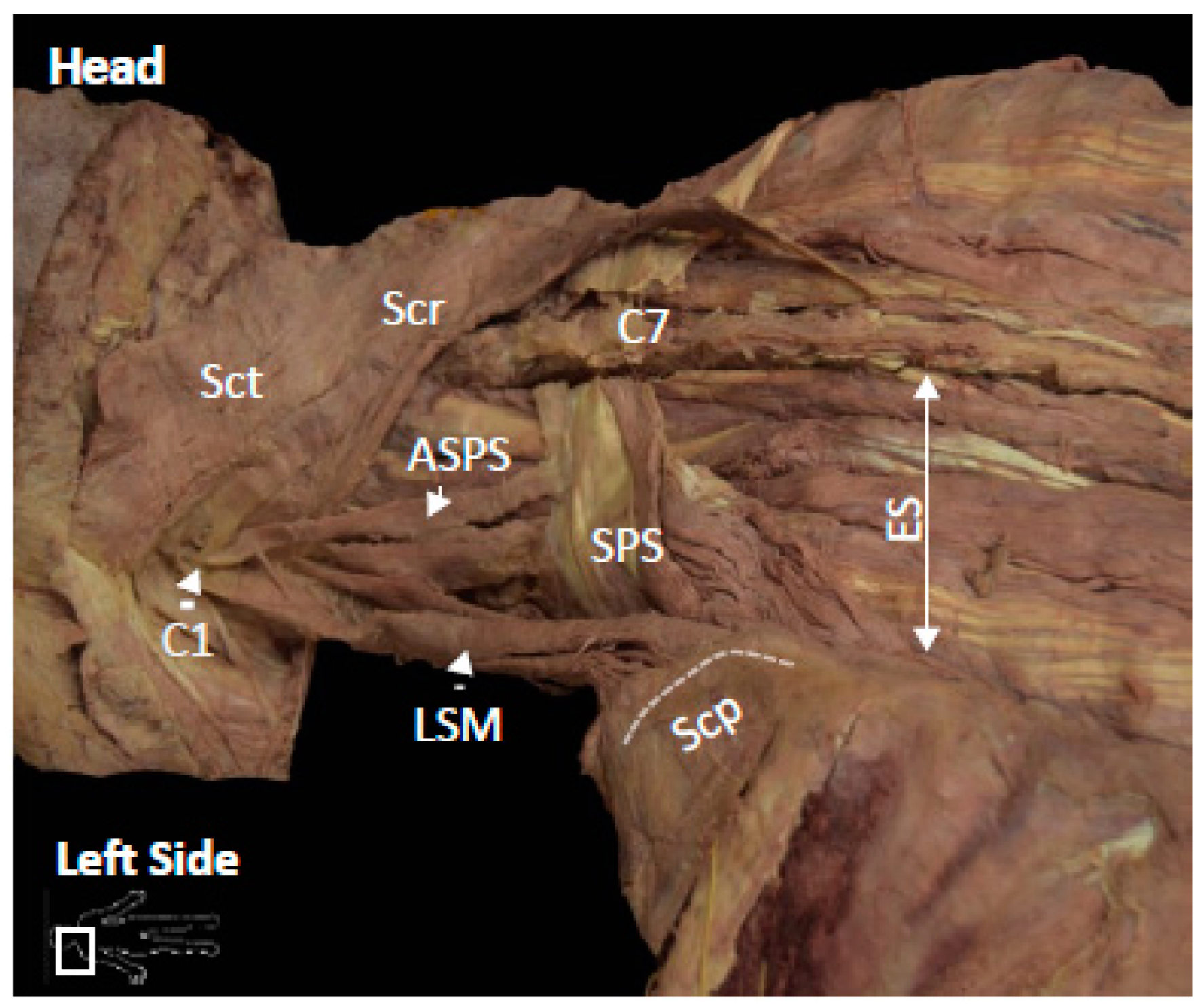
During routine dissection of the neck and back regions, we found a unilateral anomalous muscle occurring within a 73-year-old Caucasian male human cadaver. The anomalous muscle originated from the left transverse process of the atlas and extended inferiorly to insert onto the SPS (
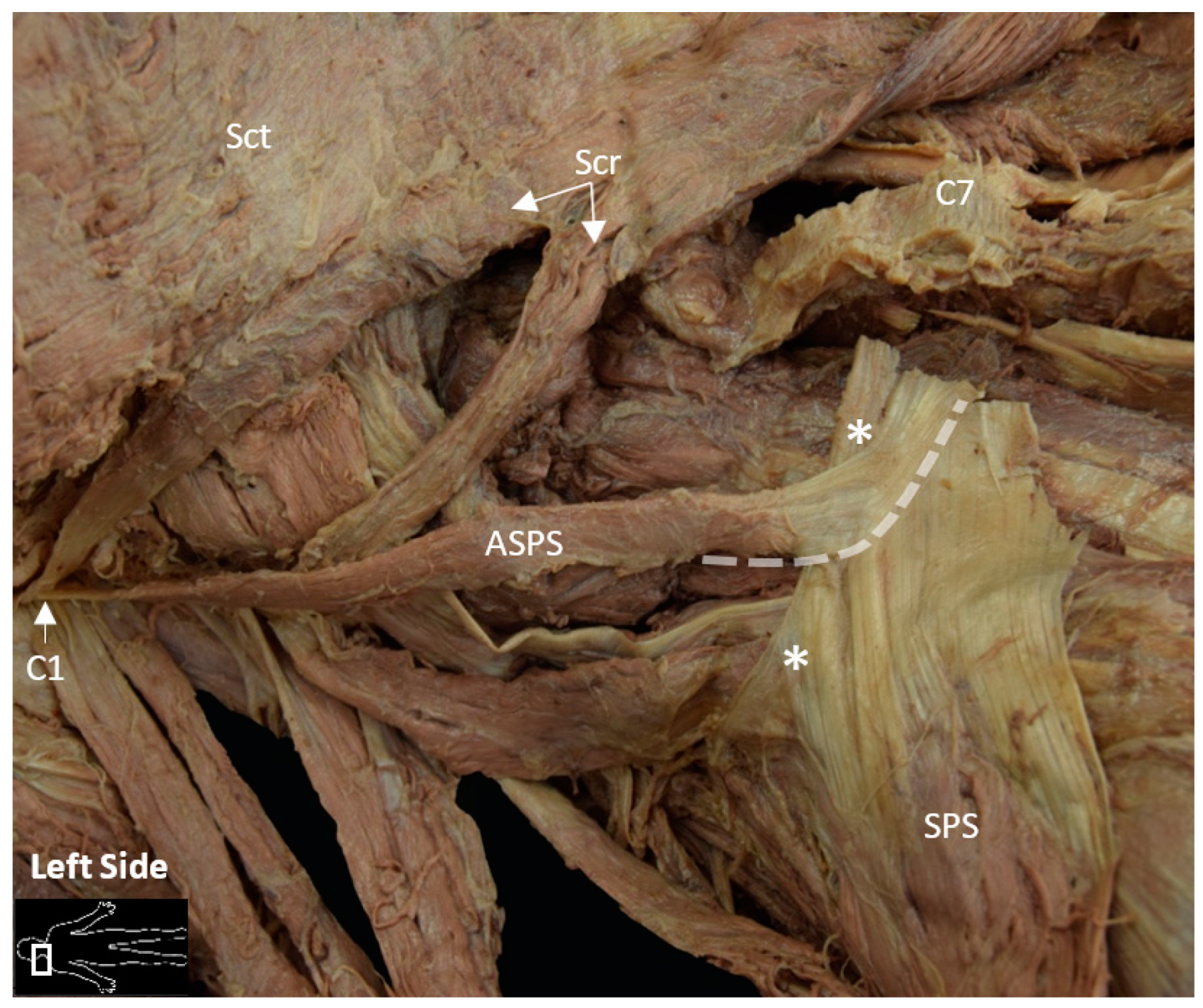
Figure 1). The left SPS presented its common anatomy: proximal attachments from the spinous processes of C7-T2 vertebrae and its distal attachments to the superior borders of the second through fifth ribs. The tendinous fibers of the anomalous muscle inserted superficially, and slightly perpendicular onto the left SPS proximal end. The fused fibers of the two muscles attached to the spinous process of the C7 vertebra (
Figure 2). The anomalous muscle shared a common attachment at the transverse process of the atlas with the upper portion of the splenius cervicis muscle and two of the upper muscular slips of the left LSM (
Figure 2). In length, the anomalous muscle measured 12.5 cm and 0.65 cm wide with a consistent width throughout its muscle belly.
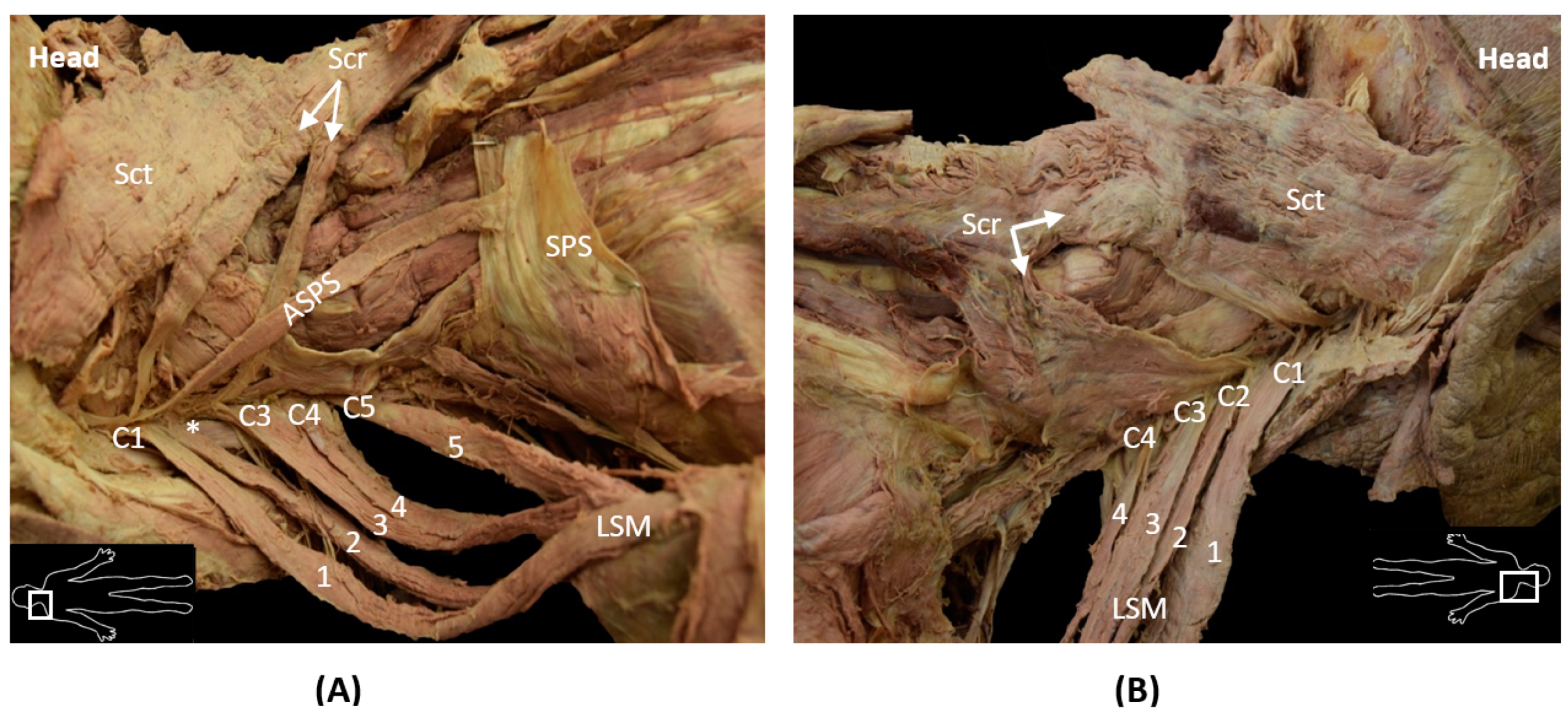
In combination with this rare finding, there were some noteworthy differences in the cervical origins of the left LSM compared to the right. The left sided LSM exhibited four main muscular slips with distal attachments to the superior angle of the scapula but varied in the number of muscular slips and cervical origins. The observed variabilities of the left LSM are as follows: (1) muscular slips 1 and 2 shared a common cervical origin at C1; (2) the third, broader muscular slip, bifurcated midway, with one muscular slip of cervical origin at C3 and the other at C4; and (3) the fourth muscular slip originated from C5; no LSM muscle slips originated from C2 (
Figure 3A). The right-sided LSM had four muscular slips that originated from the transverse processes of C1–C4 vertebrae, respectively, and were relatively consistent in size and shape (
Figure 3B). The muscular asymmetry in the present case produced a five-headed left LSM and a four-headed right LSM.
4. Discussion
There are earlier reports of supernumerary and divergent muscular slips of the LSM with varying cervical origins and insertions [
4]. However, these descriptions always illustrated muscular or tendinous connections to the scapula and were characterized as deviant or rogue slips of the LSM. These deviant slips of the LSM fall within the normal range of possibilities and are true variants of the LSM. In the present case, however, the atypical muscle, Accessory Serratus Posterior Superior (ASPS), does not have any muscular or tendinous connections to the scapula. Its morphology is distinctly different from previous observations of deviant slips of LSM. Therefore, we consider this finding to be a true representation of a rare muscular anomaly and not a deviant or variant slip of the LSM. Furthermore, the insertion of the anomalous muscle onto the dorsal surface of the SPS suggests that it may have aided or reinforced the action of the SPS during elevation of the ribs, specifically the second rib, thus functioning as a possible accessory muscle to SPS. Its insertion does not support its action as an accessory LSM because it cannot elevate or rotate the scapula.
4.1. Embryological Implication of the ASPS
Muscle development is a complex and multistep process that involves a series of cellular events of cell fusion, migration and attachment [
5]. During myogenesis, myoblasts form into migrating myofibers that are guided towards specific tendon attachment sites to establish connection with the skeletal system [
5]. Errors may occur in migration that alter the attachment of muscle and tendon precursor cells, causing ectopic origins and insertions of muscular slips [
6]. Therefore, the presence of the ASPS muscle may be a result of errors in the migration of muscle progenitors or tendinous attachment progenitors at the C1 level [
7], due to alterations in the microenvironment through which the cells migrate, or Hox-gene related alterations in the axial identity of the progenitors [
8].
4.2. Muscular Variation Bias to One Side of the Body
While bilateral symmetry in the body’s topography is a central feature of vertebrate anatomy [
9], many studies demonstrate that asymmetry is not uncommon [
10]. In the present case, muscular variation biased toward the left side of the body suggests a disturbance during development may have affected the symmetry of the musculoskeletal system. In a recent study by Bang et al., 2015, multiple muscular variations from the neck to the lower extremities primarily on the left side were reported in a single cadaver [
6]. They attributed this lack of symmetry to momentary disturbances in the formation of the embryonic somites.
Somites, which give rise to the vertebrae, ribs and associated muscles and tendons, arise as bilaterally symmetric, paired blocks of paraxial mesoderm in a developing embryo’s left and right sides [
11]. Each somite pair carried a specific axial identity due to the expression of a unique combination of Hox genes [
8]. Interestingly, it has been found in several animal models that asymmetries in left–right somite pairs occur when Retinoic acid (RA) signaling is reduced, leading to developmental delay on one side [
11]. These findings suggest that RA signaling is essential to ensure symmetrical mesoderm segmentation and bilateral symmetry along the left–right axis [
11]. We speculate that environmental factor(s) acting during early embryonic development may have disturbed this synchrony, leading to a disturbance in the synchronicity of the left and right sides during somitogenesis, causing muscular variation bias in this individual. One such known disruptor of RA signaling is maternal consumption of alcohol [
12].
4.3. Clinical Significance
Embryonic development of the back and neck muscles is complex. Understanding this process is key to identifying congenital anomalies, diagnosing congenital abnormalities and discerning how and where during development they may occur. Anatomic anomalies and variations of the back and neck may contribute to pathological conditions of these regions such as myofascial syndrome and the need for radical neck dissection surgery. The presence of the ASPS may pose a challenge to surgeons and could result in erroneous diagnosis as a soft tissue tumor in radiologic evaluations. Hence, reporting is not only important for the medical literature and education, but to also help clarify unknown or controversial clinical presentations in the human body. Moreover, due to a limited medical report, there was no reported medical significance related to the anomaly and asymmetry in this individual nor was the cause of death related to our findings. This case report further supports clinical observations that muscular variations, anomalies and asymmetry can exist simultaneously in an individual and that they may occur more commonly than previously thought.
Author Contributions
Conceptualization, K.L.; investigation, K.L.; writing—original draft preparation, K.L.; visualization, K.L.; writing—review and editing, K.L. and G.G. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Ethical review and approval were waived for this study, given that the material used in this study is considered as a non-human subject; therefore, ethical approval was waived.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data sharing not applicable.
Acknowledgments
With great respect and honor, we thank our donor and his family for such an incredible gift. We thank Ronald W. Rivenburgh, CIV from the Anatomical Gift Program at USUHS, Osvaldo Bustos, Ayo P. Doumatey, Victor Taylor II and Sally Moody for their guidance, mentorship and appreciated contributions. Special thanks to Mohammed Ashraf Aziz for his unwavering support and inspiration.
Conflicts of Interest
The authors declare no conflict of interest.
Disclaimer
The opinions or assertions contained herein are the private ones of the authors/speakers and not to be construed as official or reflecting the views of the Department of Defense, the Uniformed Services University of the Health Sciences or any other agency of the U.S. Government.
References
- Yammine, K. Evidence-based anatomy. Clin. Anat. 2014, 27, 847–852. [Google Scholar] [CrossRef] [PubMed]
- Sookur, P.A.; Naraghi, A.M.; Bleakney, R.R.; Jalan, R.; Chan, O.; White, L.M. Accessory muscles: Anatomy, symptoms, and radiologic evaluation. Radiographics 2008, 28, 481–499. [CrossRef] [PubMed]
- Chotai, P.N.; Loukas, M.; Tubbs, R.S. Unusual origin of the levator scapulae muscle from mastoid process. Surg. Radiol. Anat. 2015, 37, 1277–1281. [Google Scholar] [CrossRef] [PubMed]
- Bergman, R.A.; Afifi, A.K.; Miyauchi, R. Anatomy Atlases an Anatomy Digital Library. Available online: http://www.anatomyatlases.org/ (accessed on 7 July 2020).
- Schnorrer, F.; Dickson, B.J. Muscle building; mechanisms of myotube guidance and attachment site selection. Dev. Cell 2004, 7, 9–20. [Google Scholar] [CrossRef] [PubMed]
- Bang, J.H.; Young-Chun, G.; Hee-Jun, Y.; Jeong-Doo, J.; Jae-Ho, L.; Hey-Yeon, L. Multiple muscular variations in the neck, upper extremity, and lower extremity biased toward the left side of a single cadaver. J. Korean Med. Sci. 2015, 30, 502–505. [Google Scholar] [CrossRef] [PubMed]
- Zelzer, E.; Blitz, E.; Killian, M.L.; Thomopoulos, S. Tendon-to-bone attachment: From development to maturity. Birth Defects Res. C Embryo Today 2014, 102, 101–112. [Google Scholar] [CrossRef] [PubMed]
- Deschamps, J.; Duboule, D. Embryonic timing, axial stem cells, chromatin dynamics, and the Hox clock. Genes Dev. 2017, 31, 1406–1416. [Google Scholar] [CrossRef] [PubMed]
- Blum, M.; Ott, T. Animal left-right asymmetry. Curr. Biol. 2018, 28, R301–R304. [Google Scholar] [CrossRef] [PubMed]
- Zaidi, Z.F. Body Asymmetries: Incidence, Etiology and Clinical Implications. Aust. J. Basic Appl. Sci. 2011, 5, 2157–2191. [Google Scholar]
- Brent, A.E. Somite Formation: Where Left Meets Right. Curr. Biol. 2005, 15, R468–R470. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Fainsod, A.; Bendelac-Kapon, L.; Shabtai, Y. Fetal Alcohol Spectrum Disorder: Embryogenesis Under Reduced Retinoic Acid Signaling Conditions. Subcell. Biochem. 2020, 95, 197–225. [Google Scholar] [CrossRef] [PubMed]
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).




{kind=link}
{kind=link}
{kind=link}


