Expression of Hypoxia-Inducible Factors in Different Stages of Pancreatic Tumor Progression

 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients and Specimens
2.2. Ethical Statement
2.3. Immunohistochemical (IHC) Staining for HIF-1α and -2α
2.4. Immunoreactivity Scoring System (IRS)
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| HIF | hypoxia inducible factor |
| PDAC | pancreatic ductal adenocarcinoma |
| NET | neuroendocrine tumor |
| IPMN | intraductal papillary mucinous neoplasm |
| PanIN | pancreatic intraepithelial neoplasia |
| NT | non-tumor |
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer Statistics, 2017. CA Cancer J. Clin. 2017, 67, 7–30. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Han, G.; Zhai, H.; Zhang, F.-M.; Wang, J.; Li, X.; Huang, S.; Wang, X.; Fan, D. Expression and Clinical Significance of CacyBP/SIP in Pancreatic Cancer. Pancreatology 2008, 8, 470–477. [Google Scholar] [CrossRef] [PubMed]
- Isaacs, J.S.; Jung, Y.J.; Mole, D.R.; Lee, S.; Torres-Cabala, C.; Chung, Y.-L.; Merino, M.; Trepel, J.; Zbar, B.; Toro, J.; et al. HIF overexpression correlates with biallelic loss of fumarate hydratase in renal cancer: Novel role of fumarate in regulation of HIF stability. Cancer Cell 2005, 8, 143–153. [Google Scholar] [CrossRef] [PubMed]
- Semenza, G.L. Targeting HIF-1 for cancer therapy. Nat. Rev. Cancer 2003, 3, 721–732. [Google Scholar] [CrossRef]
- Birner, P.; Schindl, M.; Obermair, A.; Plank, C.; Breitenecker, G.; Oberhuber, G. Overexpression of hypoxia-inducible factor 1alpha is a marker for an unfavorable prognosis in early-stage invasive cervical cancer. Cancer Res. 2000, 60, 4693–4696. [Google Scholar]
- Talks, K.L.; Turley, H.; Gatter, K.C.; Maxwell, P.H.; Pugh, C.W.; Ratcliffe, P.J.; Harris, A.L. The Expression and Distribution of the Hypoxia-Inducible Factors HIF-1α and HIF-2α in Normal Human Tissues, Cancers, and Tumor-Associated Macrophages. Am. J. Pathol. 2000, 157, 411–421. [Google Scholar] [CrossRef]
- Zhong, H.; De Marzo, A.M.; Laughner, E.; Lim, M.; Hilton, D.A.; Zagzag, D.; Buechler, P.; Isaacs, W.B.; Semenza, G.L.; Simons, J.W. Overexpression of hypoxia-inducible factor 1alpha in common human cancers and their metastases. Cancer Res. 1999, 59, 5830–5835. [Google Scholar]
- Forsythe, J.A.; Jiang, B.H.; Iyer, N.V.; Agani, F.; Leung, S.W.; Koos, R.D.; Semenza, G.L. Activation of vascular endothelial growth factor gene transcription by hypoxia-inducible factor 1. Mol. Cell. Biol. 1996, 16, 4604–4613. [Google Scholar] [CrossRef]
- Lee, S.H.; Wolf, P.L.; Escudero, R.; Deutsch, R.; Jamieson, S.W.; Thistlethwaite, P.A. Early Expression of Angiogenesis Factors in Acute Myocardial Ischemia and Infarction. N. Engl. J. Med. 2000, 342, 626–633. [Google Scholar] [CrossRef]
- Maxwell, P.H.; Wiesener, M.S.; Chang, G.-W.; Clifford, S.C.; Vaux, E.C.; Cockman, M.E.; Wykoff, C.C.; Pugh, C.W.; Maher, E.R.; Ratcliffe, P.J. The tumour suppressor protein VHL targets hypoxia-inducible factors for oxygen-dependent proteolysis. Nat. Cell Biol. 1999, 399, 271–275. [Google Scholar] [CrossRef]
- Bruick, R.K. A Conserved Family of Prolyl-4-Hydroxylases That Modify HIF. Science 2001, 294, 1337–1340. [Google Scholar] [CrossRef]
- Wang, M.; Chen, M.; Guo, X.; Jian, J. Expression and significance of HIF-1α and HIF-2α in pancreatic cancer. Acta Acad. Med. Wuhan 2015, 35, 874–879. [Google Scholar] [CrossRef] [PubMed]
- Zhao, J.; Du, F.; Shen, G.; Zheng, F.; Xu, B. The role of hypoxia-inducible factor-2 in digestive system cancers. Cell Death Dis. 2015, 6, e1600. [Google Scholar] [CrossRef] [PubMed]
- Qin, N.; De Cubas, A.A.; Garcia-Martin, R.; Richter, S.; Peitzsch, M.; Menschikowski, M.; Lenders, J.W.; Timmers, H.J.L.M.; Mannelli, M.; Opocher, G.; et al. Opposing effects of HIF1α and HIF2α on chromaffin cell phenotypic features and tumor cell proliferation: Insights from MYC-associated factor X. Int. J. Cancer 2014, 135, 2054–2064. [Google Scholar] [CrossRef]
- Zheng, S.-S.; Chen, X.-H.; Yin, X.; Zhang, B.-H. Prognostic Significance of HIF-1α Expression in Hepatocellular Carcinoma: A Meta-Analysis. PLoS ONE 2013, 8, e65753. [Google Scholar] [CrossRef] [PubMed]
- Kimura, S.; Kitadai, Y.; Tanaka, S.; Kuwai, T.; Hihara, J.; Yoshida, K.; Toge, T.; Chayama, K. Expression of hypoxia-inducible factor (HIF)-1α is associated with vascular endothelial growth factor expression and tumour angiogenesis in human oesophageal squamous cell carcinoma. Eur. J. Cancer 2004, 40, 1904–1912. [Google Scholar] [CrossRef]
- Lu, X.-G.; Xing, C.-G.; Feng, Y.-Z.; Chen, J.; Deng, C. Clinical Significance of Immunohistochemical Expression of Hypoxia-Inducible Factor–1α as a Prognostic Marker in Rectal Adenocarcinoma. Clin. Color. Cancer 2006, 5, 350–353. [Google Scholar] [CrossRef]
- Roig, E.M.; Yaromina, A.; Houben, R.; Groot, A.J.; Dubois, L.; Vooijs, M. Prognostic Role of Hypoxia-Inducible Factor-2α Tumor Cell Expression in Cancer Patients: A Meta-Analysis. Front. Oncol. 2018, 8. [Google Scholar] [CrossRef]
- Han, S.; Huang, T.; Li, W.; Liu, S.; Yang, W.; Shi, Q.; Li, H.; Ren, J.; Hou, F. Association Between Hypoxia-Inducible Factor-2α (HIF-2α) Expression and Colorectal Cancer and Its Prognostic Role: A Systematic Analysis. Cell. Physiol. Biochem. 2018, 48, 516–527. [Google Scholar] [CrossRef]
- Imamura, T.; Kikuchi, H.; Herraiz, M.-T.; Park, D.-Y.; Mizukami, Y.; Mino-Kenduson, M.; Lynch, M.P.; Rueda, B.R.; Benita, Y.; Xavier, R.J.; et al. HIF-1alpha and HIF-2alpha have divergent roles in colon cancer. Int. J. Cancer 2009, 124, 763–771. [Google Scholar] [CrossRef]
- Zhu, G.; Tang, Y.; Li, L.; Zheng, M.; Jiang, J.; Li, X.-Y.; Chen, S.-X.; Liang, X.-H. Hypoxia Inducible Factor 1 and Hypoxia Inducible Factor 2 Play Distinct and Functionally Overlapping Roles in Oral Squamous Cell Carcinoma. Clin. Cancer Res. 2010, 16, 4732–4741. [Google Scholar] [CrossRef]
- Rankin, E.B.; Giaccia, A.J. The role of hypoxia-inducible factors in tumorigenesis. Cell Death Differ. 2008, 15, 678–685. [Google Scholar] [CrossRef]
- Akakura, N.; Kobayashi, M.; Horiuchi, I.; Suzuki, A.; Wang, J.; Chen, J.; Niizeki, H.; Ki, K.; Hosokawa, M.; Asaka, M. Constitutive expression of hypoxia-inducible factor-1alpha renders pancreatic cancer cells resistant to apoptosis induced by hypoxia and nutrient deprivation. Cancer Res. 2001, 61, 6548–6554. [Google Scholar]
- Qin, R.; Smyrk, T.C.; Reed, N.R.; Schmidt, R.L.; Schnelldorfer, T.; Chari, S.T.; Petersen, G.M.; Tang, A.H. Combining clinicopathological predictors and molecular biomarkers in the oncogenic K-RAS/Ki67/HIF-1alpha pathway to predict survival in resectable pancreatic cancer. Br. J. Cancer 2015, 112, 514–522. [Google Scholar] [CrossRef]
- Katagiri, T.; Kobayashi, M.; Yoshimura, M.; Morinibu, A.; Itasaka, S.; Hiraoka, M.; Harada, H. HIF-1 maintains a functional relationship between pancreatic cancer cells and stromal fibroblasts by upregulating expression and secretion of Sonic hedgehog. Oncotarget 2018, 9, 10525–10535. [Google Scholar] [CrossRef]
- Colbert, L.E.; Fisher, S.B.; Balci, S.; Saka, B.; Chen, Z.; Kim, S.; El-Rayes, B.F.; Adsay, N.V.; Maithel, S.K.; Landry, J.C.; et al. High nuclear hypoxia-inducible factor 1 alpha expression is a predictor of distant recurrence in patients with resected pancreatic adenocarcinoma. Int. J. Radiat. Oncol. 2015, 91, 631–639. [Google Scholar] [CrossRef] [PubMed]
- Ye, L.-Y.; Zhang, Q.; Bai, X.-L.; Pankaj, P.; Hu, Q.-D.; Liang, T. Hypoxia-inducible factor 1α expression and its clinical significance in pancreatic cancer: A meta-analysis. Pancreatology 2014, 14, 391–397. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, A.-C.; Mori, R.; Vallbohmer, D.; Brabender, J.; Klein, E.; Drebber, U.; Baldus, S.E.; Cooc, J.; Azuma, M.; Metzger, R.; et al. High Expression of HIF1a Is a Predictor of Clinical Outcome in Patients with Pancreatic Ductal Adenocarcinomas and Correlated to PDGFA, VEGF, and bFGF. Neoplasia 2008, 10, 674–679. [Google Scholar] [CrossRef] [PubMed]
- Aga, M.; Kondo, S.; Wakisaka, N.; Moriyama-Kita, M.; Endo, K.; Nakanishi, Y.; Murono, S.; Sugimoto, H.; Ueno, T.; Yoshizaki, T. Siah-1 is associated with expression of hypoxia-inducible factor-1α in oral squamous cell carcinoma. Auris Nasus Larynx 2017, 44, 213–219. [Google Scholar] [CrossRef]
- Fedchenko, N.; Reifenrath, J. Different approaches for interpretation and reporting of immunohistochemistry analysis results in the bone tissue—A review. Diagn. Pathol. 2014, 9, 221. [Google Scholar] [CrossRef]
- Cases, A.I.; Ohtsuka, T.; Kimura, H.; Zheng, B.; Shindo, K.; Oda, Y.; Mizumoto, K.; Nakamura, M.; Tanaka, M. Significance of expression of glucagon-like peptide 1 receptor in pancreatic cancer. Oncol. Rep. 2015, 34, 1717–1725. [Google Scholar] [CrossRef]
- Varghese, F.; Bukhari, A.B.; Malhotra, R.; De, A. IHC Profiler: An Open Source Plugin for the Quantitative Evaluation and Automated Scoring of Immunohistochemistry Images of Human Tissue Samples. PLoS ONE 2014, 9, e96801. [Google Scholar] [CrossRef]
- Mane, D.R.; Kale, A.D.; Belaldavar, C. Validation of immunoexpression of tenascin-C in oral precancerous and cancerous tissues using ImageJ analysis with novel immunohistochemistry profiler plugin: An immunohistochemical quantitative analysis. J. Oral Maxillofac. Pathol. 2017, 21, 211. [Google Scholar] [CrossRef]
- Denko, N.C. Hypoxia, HIF1 and glucose metabolism in the solid tumour. Nat. Rev. Cancer 2008, 8, 705–713. [Google Scholar] [CrossRef]
- Beck, R.; Röper, B.; Carlsen, J.M.; Huisman, M.C.; Lebschi, J.A.; Andratschke, N.; Picchio, M.; Souvatzoglou, M.; Machulla, H.-J.; Piert, M. Pretreatment 18F-FAZA PET Predicts Success of Hypoxia-Directed Radiochemotherapy Using Tirapazamine. J. Nucl. Med. 2007, 48, 973–980. [Google Scholar] [CrossRef]
- Rischin, D.; Hicks, R.J.; Fisher, R.; Binns, D.; Corry, J.; Porceddu, S.; Peters, L.J. Prognostic Significance of [18F]-Misonidazole Positron Emission Tomography–Detected Tumor Hypoxia in Patients With Advanced Head and Neck Cancer Randomly Assigned to Chemoradiation With or Without Tirapazamine: A Substudy of Trans-Tasman Radiation Oncology Group Study 98.02. J. Clin. Oncol. 2006, 24, 2098–2104. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Parameter | Groups (n) | |||
|---|---|---|---|---|
| PDAC (15) | NET (7) | IPMN (4) | PanIN (3) | |
| Age, years (mean) | 65.56 | 61.64 | 65.38 | 55.69 |
| Sex, n | ||||
| Male (%) | 8 (53.3) | 4 (57.1) | 1 (25.0) | 1 (33.3) |
| Female (%) | 7 (46.7) | 3 (42.86) | 3 (75.0) | 2 (66.7) |
| Combined disease (n) | ||||
| Diabetes mellitus | 5 | 1 | 1 | 1 |
| Hypertension | 7 | 7 | 1 | 1 |
| Dyslipidemia | 5 | 4 | 1 | 0 |
| Cancer (type) | 1 (papillary thyroid carcinoma) | 1 (colon cancer) & 1 (prostate cancer) | 0 | 1 (Hodgikin’s disease) |
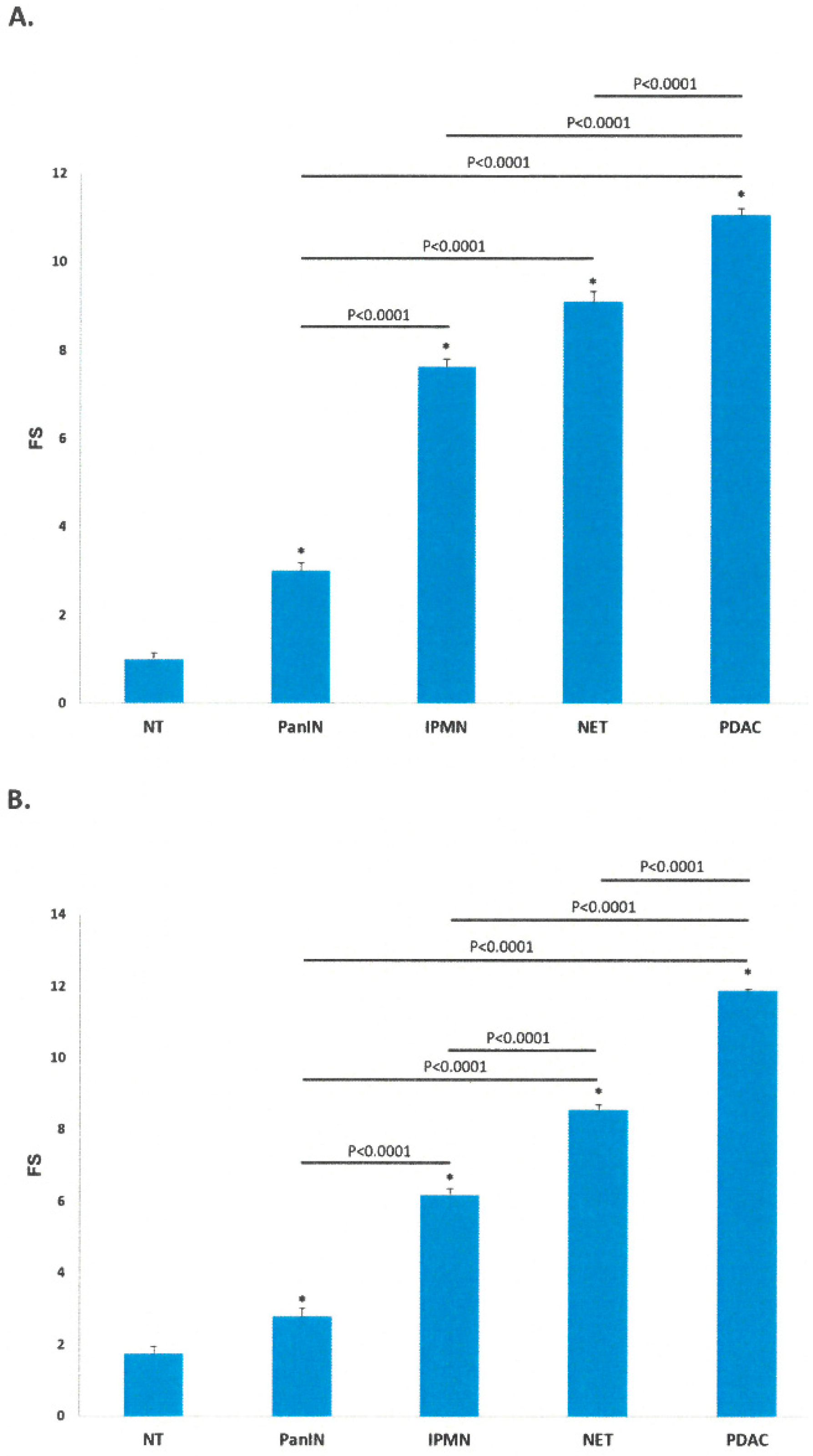
| Groups (n) | HIF-1α | HIF-2α |
|---|---|---|
| (Mean ± SEM) | (Mean ± SEM) | |
| NT (21) | 1.00 ± 0.13 | 1.75 ± 0.20 |
| PanIN (3) | 3.01 ± 0.17 | 2.79 ± 0.22 |
| IPMN (4) | 7.63 ± 0.18 | 6.19 ± 0.17 |
| NET (7) | 9.10 ± 0.23 | 8.56 ± 0.14 |
| PDAC (15) | 11.06 ± 0.15 | 11.88 ± 0.04 |
| Group | # Patients Stained | HIF-1α | HIF-2α | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Total Slides Stained | Total Pictures Analyzed | Strength of Immunoreactivity (%) | Total Slides Stained | Total Picture Analyzed | Strength of Immunoreactivity (%) | ||||||||
| Ⅰ | Ⅱ | Ⅲ | Ⅳ | Ⅰ | Ⅱ | Ⅲ | Ⅳ | ||||||
| NT | 21 | 21 | 84 | 90.5 | 9.5 | 0 | 0 | 12 | 48 | 66.7 | 33.3 | 0 | 0 |
| PanIN | 3 | 5 | 20 | 0 | 80 | 20 | 0 | 8 | 32 | 0 | 100 | 0 | 0 |
| IPMN | 4 | 6 | 24 | 0 | 0 | 50 | 50 | 9 | 36 | 0 | 11.1 | 66.7 | 22.2 |
| NET | 7 | 10 | 40 | 0 | 0 | 30 | 70 | 13 | 52 | 0 | 0 | 30.8 | 69.2 |
| PDAC | 15 | 21 | 84 | 0 | 0 | 9.5 | 90.5 | 23 | 92 | 0 | 0 | 0 | 100 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jung, J.H.; Sosnowska, D.; Weaver, J.; Parson, H.K.; Casellini, C.M.; Vinik, A.I. Expression of Hypoxia-Inducible Factors in Different Stages of Pancreatic Tumor Progression. Reports 2020, 3, 30. https://doi.org/10.3390/reports3040030
Jung JH, Sosnowska D, Weaver J, Parson HK, Casellini CM, Vinik AI. Expression of Hypoxia-Inducible Factors in Different Stages of Pancreatic Tumor Progression. Reports. 2020; 3(4):30. https://doi.org/10.3390/reports3040030
Chicago/Turabian StyleJung, Jung Hwa, Danuta Sosnowska, Jessica Weaver, Henri K. Parson, Carolina M. Casellini, and Aaron I. Vinik. 2020. "Expression of Hypoxia-Inducible Factors in Different Stages of Pancreatic Tumor Progression" Reports 3, no. 4: 30. https://doi.org/10.3390/reports3040030
APA StyleJung, J. H., Sosnowska, D., Weaver, J., Parson, H. K., Casellini, C. M., & Vinik, A. I. (2020). Expression of Hypoxia-Inducible Factors in Different Stages of Pancreatic Tumor Progression. Reports, 3(4), 30. https://doi.org/10.3390/reports3040030