Abstract
This study directly compared blood flow and oxygenation during six treatment parameters used with vertical and side alternating whole body vibration (WBV). Twenty-seven healthy adults were randomized into the vertical or side-alternating (vibration type) WBV group. Participants completed three WBV sessions a week apart, 5 sets of 1 min on/off, at 3 conditions (Vertical: 30 Hz and 4 mm, 40 Hz and 2 mm, 45 Hz and 4 mm; Side-alternating: 10 Hz and 4 mm, 18 Hz and 3 mm and 26 Hz and 2 mm). Blood flow velocity and popliteal artery diameter, muscle oxygenation, skin temperature, heart rate and blood pressure were assessed. Muscle oxygenation was significantly increased for all vibration frequencies and types following two minutes of WBV (14.78%, p = 0.02) and continued until immediately after the cessation of WBV (24.7%, p < 0.001). WBV also increased heart rate (23.9%, p < 0.001) and systolic blood pressure (8.9%, p < 0.001) regardless of frequency and vibration type. Side-alternating and vertical WBV increased muscle oxygenation and heart rate in healthy participants completing an isometric squat. Muscle oxygenation was not increased until the second vibration set indicating the amount of time spent on the platform may have a significant effect on increases in blood flow.
1. Introduction
Whole body vibration (WBV) is a low intensity exercise performed on an oscillating platform that produces sinusoidal vibrations. The commercially available devices include two mechanically different platforms (vibration type): (1) a vertical platform which provides tri-axial acceleration with most of the vibration in the vertical direction, uniformly lifting the body; and (2) a side-alternating (also called horizontal) oscillating platform that uses a fulcrum to alternatively lift the left and right side of the body. Amplitude (size of the oscillatory motion) and frequency (cycle repetition rate) are manipulated on both platforms to adjust the intensity of the vibration.
WBV has become popular as both a clinical and performance enhancement tool. Multiple studies have highlighted the benefits of including WBV as a low intensity exercise for its ability to increase bone mineral density in osteoporosis patients [1], while simultaneously reducing fall risk through an increase in balance and strength [1,2]. WBV has also been used for patients with cerebral palsy to increase motor development and muscular strength [3,4]; been reported to increase proprioception, strength, and balance in participants with anterior cruciate ligament reconstruction [5,6] and chronic ankle instability in physically active populations [7,8,9]; and shown to increase muscle strength, [10] vertical jump height [10,11], and flexibility in young healthy adults [10,11]. Several studies have investigated the influence of WBV on blood flow and muscle oxygenation, critical for repair and remodeling during skeletal muscle healing, with confounding results [12]. Some research suggests WBV increases both blood flow [13,14,15,16] and muscle oxygenation [13,14]; while other studies have found small or no changes in muscle oxygenation [17,18] and blood flow [19] after WBV exposure.
The conflicting outcomes in research on physiological changes resulting from WBV are likely due to differences in vibration type (vertical or side-alternating) and parameters (amplitude and frequency). Vibration parameters may influence skeletal muscle physiology in different ways. Thus, different combinations of these parameters are likely needed to optimize specific training and treatment outcomes. To date, few studies have compared the frequency and amplitudes combinations commonly available with vertical and side-alternating platforms in a healthy population. The purpose of this study was to directly compare six commonly available combinations of treatment parameters used with vertical and side alternating whole body vibration (WBV) platforms for influence on blood flow and muscle oxygenation.
2. Materials and Methods
A randomized control trial (Figure 1) evaluated three sets of frequencies and amplitudes with side-alternating and vertical vibration platforms on blood flow, skin temperature, heart rate and blood pressure. A member of the research team informed participants of the study procedures. Informed consent was obtained from all study participants. This study was approved by Auburn University Institutional Review Board protocol number 19-211.
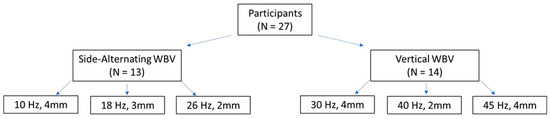
Figure 1.
Study Design. Note: Hz, hertz; mm, millimeters; WBV, whole body vibration; the terms horizontal and side-alternating are used interchangeably in the literature.
Twenty-seven young, healthy participants (12 female, 15 male) completed the three sessions of WBV. Demographics for each of the groups in located in Table 1.

Table 1.
Participant demographics.
A power calculation requiring 12 participants per group was completed prior to completion based on results of Games et al. [13], with an alpha level of 0.05 and power of 0.80. Participants were randomly divided into a side-alternating WBV group and a vertical WBV group. Participants in each group completed three WBV sessions within their respective vibration type using parameters commonly used for research and treatment. Parameters for the side-alternating WBV were set at 26 hertz (Hz) and 2 millimeters (mm) (peak acceleration = 2.71 g), 10 Hz and 4 mm (peak acceleration = 0.80 g), and 18 Hz and 3 mm (peak acceleration = 1.95 g) on a Galileo Med L Chip Sensor platform (Novotec Medical GmbH, Pforzheim, Germany). Parameters for the vertical WBV were set at 40 Hz and 2 mm (peak acceleration = 6.43 g), 30 Hz and 4 mm (peak acceleration = 7.23 g), and 45 Hz and 4 mm (peak acceleration = 16.28 g) on a PowerPlate Pro 7 platform (Performance Health Systems, Northbrook, IL, USA. Peak accelerations provided by the manufacturer). The order of vibration frequencies and amplitudes were randomized by participant. Participants flexed their knees to 45° and maintained this semi-squat position, with their bare feet flat on the platform while lightly holding on to the device’s handlebar for all WBV sessions. Participants were instructed to stand with feet shoulder width apart on the vertical vibration platform. On the side-alternating platform participants were instructed to stand with their feet on the platform marks for the specific vibration amplitude for the trial (feet farther apart result in a larger amplitude). The WBV sessions lasted for a total of 10 min; alternating one minute of vibration with one minute of rest for a total of five minutes of vibration.
Blood flow, popliteal artery diameter (in the popliteal fossa), heart rate, and skin temperature were measured prior, immediately following, and five minutes, 10 min, and 15 min following WBV treatment. Popliteal artery diameter and blood flow velocity were captured with the patient in the standing position on the non-vibrating platform using a GE Portable LOGIQ e R7 ultrasound with a L4-12t Ultrasound head (GE Healthcare, New York, NY, USA). The popliteal artery was selected to obtain blood flow measurements of the lower leg, and was located and marked behind the knee prior to beginning the vibration sessions. The marked location was used for all subsequent measurements. Skin temperature was taken using a FLIR thermal imaging camera (FLIR, Wilsonville, OR, USA). Five thermal images were captured to determine skin temperature changes on the dorsal foot, anterior lower leg, posterior lower leg, anterior thigh, and posterior thigh. All blood flow and skin temperature measurements were taken by the same researcher to reduce variation. A Zephyr Bioharness (Zephyr Performance Systems, Annapolis, MD, USA) was worn around the participant’s chest to capture heart rate changes during the WBV session.
Muscle oxygenation was measured throughout the WBV session. Muscle oxygenation was measured on the participants right rectus femoris using a Humon Hex (Humon, Cambridge, MA, USA). The Humon monitor has been previously validated for muscle oxygenation on the rectus femoris. Blood pressure was assessed using an automatic blood pressure cuff (ReliOn Bp200 Blood Pressure Monitor, Omron Health Care, Inc., Kyoto, Japan) on the participant’s right arm prior, immediately following and 15 min after the WBV session.
Statistical analyses were completed using Microsoft Excel (Microsoft Excel, Professional Plus 2016, Microsoft Corporation, Redmond, WA, USA), R statistical software [20], and R Studio [21]. A two-way multivariate analysis of variance (MANOVA) was used to determine the effect of the WBV parameters on blood flow, popliteal artery diameter, heart rate, and skin temperature. Follow-up Bonferroni post hoc comparisons were selected for main effect analysis. Assumption testing was completed prior to the two-way MANOVA. There is no indication of violation of independence of dependent variables. Shapiro–Wilk testing indicated a violation of normality for each variable. Multivariant normality testing found a violation of normality. For the assumption of variance and covariances homogeneity levene testing and box-m were used, respectively. Box-m testing indicated a violation of homogeneity (p < 0.001), however levene test indicated no violation of homogeneity for each individual variable.
Repeated measures analysis of variances (ANOVA) were used to determine the effect of WBV on muscle oxygenation and systolic and diastolic blood pressure. Assumption testing completed prior to ANOVA testing indicated a violation of normality and no violation of homogeneity.
3. Results
This section may be divided by subheadings. It should provide a concise and precise description of the experimental results, their interpretation, as well as the experimental conclusions that can be drawn.
3.1. Heart Rate, Blood Flow Velocity, Popliteal Diameter, and Skin Temperature
The effect of WBV on blood flow velocity, heart rate and popliteal diameter across frequencies is illustrated in Figure 2. Multivariate testing indicated no interaction between session frequency and time for heart rate, blood flow velocity, popliteal diameter or skin temperature [Wilkes-lambda = 0.68, F (160, 2277) = 0.76, p = 0.98]. Multivariate testing for main effects indicated a main effect for time [Wilkes-lambda = 0.69, F (32, 1119) = 3.75, p < 0.001] and session frequency [Wilkes-lambda = 0.77, F (40, 1,323) = 1.99, p < 0.001]. Univariate testing indicated a main effect of time on popliteal artery diameter [F (4, 310) = 3.54, p = 0.008]. Post hoc comparisons indicated popliteal artery diameter was significantly increased five minutes after vibration compared to pre-vibration measurements [t (356) = −2.79, p = 0.04], however no difference was found for any other time point. There was a main effect of time on heart rate [F (4, 310) = 15.56, p < 0.001]. Heart rate was significantly elevated immediately following WBV as compared to prior to WBV [t (359) = −7.64, p < 0.001], five minutes following [t (359) = 6.44, p < 0.001], 10 minutes following [t (359) = 6.64, p < 0.001], and 15 min following WBV [t (359) = 6.74, p < 0.001]. There was no main effect of time on blood flow velocity [F (4, 310) = 1.93, p = 0.10]. Additionally, there was no effect of time on any of the skin temperature locations; foot [F (4, 310) = 1.10, p = 0.36], posterior lower leg [F (4, 310) = 0.22, p = 0.93], anterior lower leg [F (4, 310) = 0.52, p = 0.72], posterior upper leg [F (4, 310) = 0.08, p = 0.99], anterior upper leg [F (4, 310) = 1.57, p = 0.18]. Lastly, there was a main effect of session frequency on posterior lower leg [F (5, 310) = 2.98, p = 0.01], anterior lower leg [F (5, 310) = 2.32, p = 0.04], posterior upper leg [F (5, 310) = 5.83, p < 0.001], and anterior upper leg skin temperature [F (5, 310) = 3.01, p = 0.01] (Figure 3). In regard to skin temperature of the anterior lower leg, post hoc testing indicated that skin temperature was lower at 40 Hz as compared to 26 Hz [t (344) = 2.97, p = 0.05] and 18 Hz [t (344) = 1.70, p = 0.02]. Post hoc testing indicated that skin temperature for the upper anterior leg was greater at 18 Hz, as compared to 10 Hz [t (336) = −2.97, p = 0.05], 30 Hz [t (336) = 3.06, p = 0.04], 40 Hz [t (336) = 3.30, p = 0.02] and 45 Hz [t (336) = 3.70, p = 0.003]. Similarly, upper posterior leg skin temperature was higher at 18 Hz, as compared to 10 Hz [t (344) = −3.24, p = 0.02], 40 Hz [t (344) = 4.64, p < 0.001], and 45 Hz [t (344) = 4.76, p < 0.001]. Although main effect testing did indicate there was a significant effect of session frequency on the posterior leg skin temperature, post hoc testing did not indicate any differences. No main effect was present for session frequency on skin temperature on foot [F (5, 310) = 1.65, p = 0.15], blood flow velocity [F (5, 310) = 0.17, p = 0.97], popliteal artery diameter [F (5, 310) = 1.58, p = 0.17] or heart rate [F (5, 310) = 0.84, p = 0.52].
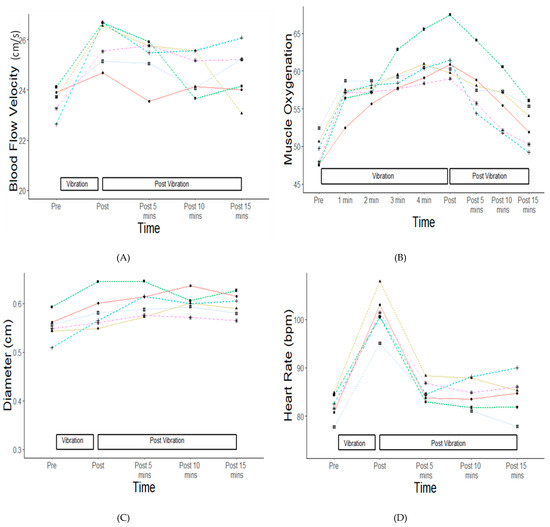
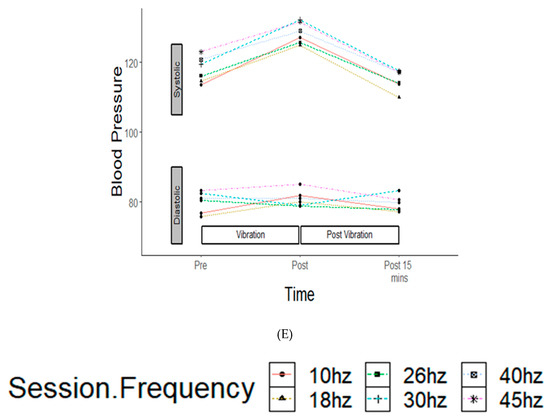
Figure 2.
Changes in blood flow velocity, muscle oxygenation, popliteal diameter, heart rate and blood pressure at study vibration frequencies. Centimeters per second (cm/s), percent (%), centimeter (cm), bpm (beats per minute), millimeters of mercury (mmHg). (A). Bloodflow velocity changes across time, (B). Muscle oxygenation changes across time, (C). Artery diameter changes across time, (D). Heart rate changes across time, (E). Blood pressure changes across time.

Figure 3.
Changes in skin temperature. Degrees Celsius (°C). (A). Foot, (B). Anterior lower leg, (C). Posterior lower leg, (D). Anterior upper leg, (E). Posterior uppper leg.
3.2. Muscle Oxygenation
Figure 2 illustrates the effects of WBV on muscle oxygenation across frequencies. There was no interaction between session frequency and time for muscle oxygenation [F (40, 671) = 0.22, p = 1.00]. There was no main effect of session frequency on muscle oxygenation [F (5, 671) = 1.64, p = 0.15]. There was a main effect of time on muscle oxygenation [F (8, 671) = 5.06, p < 0.001]. Muscle oxygenation was significantly higher after the second WBV minute [t (671) = −3.37, p = 0.02], third WBV minute [t (671) = −4.11, p = 0.001], fourth WBV minute [t (671) = −4.76, p < 0.001], and immediately following WBV [t (671) = −5.03, p < 0.001] as compared to prior to WBV. Muscle oxygenation was significantly elevated at the end of the fourth minute [t (671) = 3.31, p = 0.03] and immediately following WBV [t (671) = 3.58, p = 0.01] as compared to 15 min after WBV.
3.3. Blood Pressure
Figure 2 shows the effects of WBV on blood pressure across frequencies. Multivariate testing indicated no interaction between session frequency and time for systolic and diastolic blood pressure [Wilkes-lambda = 0.96, F (20, 446) = 0.43, p = 0.98]. Multivariate testing for main effects indicated a main effect for time [Wilkes-lambda = 0.87, F (4, 446) = 8.27, p < 0.001], but not for session frequency [Wilkes-lambda = 0.95, F (10, 446) = 1.21, p = 0.28]. Univariate testing indicated that there was a main effect of time on systolic blood pressure [F (2, 224) = 16.35, p < 0.001], but not diastolic blood pressure [F (2, 224) = 0.54, p = 0.58]. Post hoc comparisons indicated that immediately after vibration systolic blood pressure was significantly increased from pre-measurements [t (224) = 4.26, p = 0.001] and from 15 min post-vibration [t (224) = −5.426, p < 0.001]. Table 2 provides a summary of significant findings.
Table 2.
Summary of significant results.
4. Discussion
WBV has been widely incorporated into rehabilitation and strength training programs for its ability to induce metabolic changes in skeletal muscle. However, a variety of machine specific parameters make choosing types of platforms, frequencies and amplitudes challenging. Often clinicians are limited by the selection or combinations of parameters they may choose. The purpose of this study was to directly compare common combinations of parameters for both vertical and side-alternating WBV platforms to assess if they influence blood flow and muscle oxygenation. The results of this study suggest improved muscle oxygenation of the quadriceps increased regardless of vibration type, frequency, or amplitude. Standing safely on a vibration platform typically uses a squat or semi-squat position to eliminate vibration traveling up the kinetic chain to the head where it can cause headaches, trigger migraines, and produce other negative effects. Figure 2 shows a steady increase in muscle oxygenation in the quadriceps muscle, followed by a steady decrease after treatment. A fairly large difference can be seen for the 26 Hz condition on the side-alternating platform. This condition provided the highest acceleration, the fast side-to-side movement of the platform made it the most challenging condition for participants to maintain the semi-squat stance. These challenges are a part of the treatment and likely contribute to the higher muscle oxygenation.
There was no statistically significant change in blood flow velocity at the popliteal artery. However, there was an overall significant effect of time on popliteal artery diameter (indicative of increased blood flow). The clinical changes were a small effect size for blood flow (ƞp2 = 0.021) and popliteal diameter (ƞp2 = 0.031). Further analysis showed no difference immediately post-vibration compared to prior to vibration, however a difference in popliteal diameter was present at 5 min following vibration as compared to prior to vibration. While there were overall differences between WBV frequencies for skin temperature, differences were not indicated across time points, either before or after WBV. Indicating that skin temperature was not altered with WBV, in the current study. There were, however, impacts on skin temperature at specific locations for individual treatment combinations (Figure 3).
Exercise increases the demand for muscle oxygenation. Tissue demands are met by increases in blood flow to the exercising muscle. The muscle oxygenation increases with little corresponding change in blood flow velocity is likely explained by the testing locations. Muscle oxygenation was completed on the rectus femorus muscle important during the squatting position used during the testing. Blood flow changes were assessed in the popliteal artery for quick standing access immediately after the WBV treatment. It may be that the muscles of the lower leg were not as challenged as the thigh muscles. Differences may also be explained by a difference in measurement time. During this study, muscle oxygenation was measured at the completion of each individual one-minute vibration treatment, while blood flow was measured only upon completion of all five vibration treatments. A similar study evaluating WBV effects on blood flow measuring blood flow during the vibration found that blood flow increased starting at 15 s of vibration and continued until completion of the vibration session [16]. At the end of the vibration blood flow velocity rapidly decreased until it was back to baseline at 75 s after vibration [16]. It is possible during the time needed to reposition the ultrasound head the blood flow may have already begun to rapidly decrease contributing to a smaller effect size. This hypothesis is further supported by an observable increase in heart rate and systolic blood pressure at the immediate cessation of WBV, as heart rate and systolic blood pressure increase to meet the tissue’s demand for blood. Importantly, systolic blood pressure was only elevated to an average of 128 mmHg, indicating that the WBV parameters used in this study do not increase blood pressure to unsafe levels.
Several studies have investigated blood flow changes with WBV at the femoral artery [16,19]. One study [22] also evaluated the effects of blood flow at the popliteal artery. The study found increases in blood flow velocity and decreases of peripheral resistance during and immediately after completing WBV exercise, likely from an increase in vessel diameter. Likewise, another study [13] investigating the effects of blood flow on the lower leg found increases in skin temperature lasting up to 20 min after WBV exercise, with skin temperatures peaking at five minutes after WBV. However, it is important to note that both the above studies [13,22] used different exercise duration and rest periods compared to the current study. Participants in the first study [22] completed an acute session of three minutes of WBV three times, while the second study [13] had only 10 s of rest between vibration treatments. In the current study as well as the study by Lythgo et al. [16], one minute of vibration with a corresponding one minute of rest was applied. This one-to-one variable time method showed an immediate decrease in blood flow at the completion of treatment. This may indicate that the amount of total time spent on the vibration platform combined with a decreased rest time between concentric-eccentric contraction cycles has greater influence on sustained blood flow than frequency and vibration parameters. More work needs to be done to investigate this.
Our findings that WBV increases muscle oxygenation contradicts two previous studies [18,23] evaluating the effect of WBV on muscle oxygenation to the quadriceps muscles. However, differences in methods common across WBV studies could explain these varying results. In one study [18] participants were asked to complete a 10 min warm-up prior to beginning an acute session of WBV possibly increasing muscle oxygenation prior to beginning the WBV treatment. It is plausible these ergometer workouts may have masked otherwise observable changes in muscle oxygenation due to WBV. Additionally, the participants in both studies [18,23] were comprised solely of physically active participants, where participants from the current study were required to be merely healthy with no current injury or illness affecting lower leg blood flow. It has been shown that WBV is less effective in increasing measures of performance such as maximal voluntary force, power, and athletic performance in trained subjects [24,25]. This is likely because the stimulus provided by the WBV is much smaller in proportion to the stimulus provided by physical training in elite athletes. It is therefore reasonable to assume the influence of increases in muscle oxygenation are greater in subjects who are untrained and less active. Further investigation should evaluate the differences in metabolic changes in untrained versus trained athletes in an acute and chronic setting. Additionally, in both studies [18,23] a single acute bout of WBV for 110 s was completed; while in the current study participants completed a total of five vibrations sessions, one minute each in length. It was not until the second bout of WBV that the muscle oxygenation was significantly increased from baseline. This indicates that length of time spent on the vibration platform may be an important factor influencing changes in metabolic functions of skeletal muscle. Lastly, it is important to note that different measurement devices were used to evaluate muscle oxygenation [18,23]. In previous studies a NIRS probe [18] or 2-channel NIRO-300 Oximeter [23] was used, while our study utilized a Humon Hex to measured muscle oxygenation. However, the Humon Hex has been validated as a field measure of muscle oxygenation in comparison to NIRS, the gold standard measure of oxygenation [26].
Overall analysis found no differences for the outcome measures as assessed between the combinations of frequencies, amplitudes, or vibration type (vertical vs. side-alternating) used in this study. Recent literature has shown that lower frequencies (5–25 Hz) have been more effective in increasing blood flow in the lower leg [16,27]. Additionally, in a recent meta-analysis [27] side-alternating vibration was shown to have a greater effect on increasing blood flow. However, frequencies ranging from 10 to 50 Hz and both platforms have been shown to be effective in increasing blood flow [13,16,22]. Future work should investigate the blood flow changes over time, impact of time intervals, and in different participant positions.
The main limitation of this study was blood flow was not measured during vibration. It took one to two minutes to reposition the ultrasound head to complete the measurements. This time gap may have limited our ability to evaluate immediate blood flow changes from the vibration. This research study did not have a true control group to compare changes in muscle oxygenation and blood flow to isometric exercise alone, however this was not the study goal. Participants were included regardless of their level of physical activity to replicate a general population. WBV may have different effects on physical active versus sedentary participants, which was not accounted for in this study. Frequency and amplitude were selected based of common parameters used in research and rehabilitation for each type of platform. This study did not attempt to determine the effect of frequency and amplitude independently. The side-alternating and vertical platforms do not have overlapping frequencies, and g-forces were not similar from device to device. Future work should more deeply assess all the different type interactions between frequencies and amplitudes and the treatment effect on specific body locations.
5. Conclusions
Our findings indicate that WBV treatment increases muscle oxygenation of the upper leg, regardless of WBV type and parameters (frequency and amplitude). This finding may be more important in untrained individuals as compared to elite athletes and should be further investigated. Additionally, since muscle oxygenation on average was not increased until the second round of vibration, clinicians should consider length of time when utilizing WBV. Further research should investigate differences in blood flow measurements based on length of WBV treatment as a factor for creating sustained increases in muscle oxygenation and blood flow. Sustained changes in blood flow parameters may have a greater implication for rehabilitation and performance related outcomes than acute changes.
Author Contributions
Conceptualization, K.D.L. and J.M.S.; methodology, K.D.L. and J.M.S.; analysis, K.D.L.; investigation, K.D.L., A.G.P., O.D.D., P.A.M. and J.M.S.; resources, J.M.S.; data curation, K.D.L., A.G.P., O.D.D. and P.A.M.; writing—original draft preparation, K.D.L.; writing—review and editing, K.D.L. and J.M.S.; supervision, J.M.S.; project administration, K.D.L.; funding acquisition, J.M.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding, and was funded by the Auburn University Warrior Research Center.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Acknowledgments
The authors would like to thank all the Neuromechanics lab members and participants for their contributions to this study.
Conflicts of Interest
The authors declare no conflict of interest.
References
- De Zepetnek, J.O.T.; Giangregorio, L.M.; Craven, B.C. Whole-body vibration as potential intervention for people with low bone mineral density and osteoporosis: A review. J. Rehabil. Res. Dev. 2009, 46, 529–542. [Google Scholar] [CrossRef] [PubMed]
- Ma, C.; Liu, A.; Sun, M.; Zhu, H.; Wu, H. Effect of whole-body vibration on reduction of bone loss and fall prevention in postmenopausal women: A meta-analysis and systematic review. J. Orthop. Surg. Res. 2016, 11, 24. [Google Scholar] [CrossRef] [PubMed]
- Ahlborg, L.; Andersson, C.; Julin, P. Whole-body vibration training compared with resistance training: Effect on spasticity, muscle strength and motor performance in adults with cerebral palsy. J. Rehabil. Med. 2006, 38, 302–308. [Google Scholar] [CrossRef]
- Song, S.; Lee, K.; Jung, S.; Park, S.; Cho, H.; Lee, G. Effect of Horizontal Whole-Body Vibration Training on Trunk and Lower-Extremity Muscle Tone and Activation, Balance, and Gait in a Child with Cerebral Palsy. Am. J. Case Rep. 2018, 19, 1292–1300. [Google Scholar] [CrossRef]
- Moezy, A.; Olyaei, G.R.; Hadian, M.R.; Razi, M.; Faghihzadeh, S. A comparative study of whole body vibration training and conventional training on knee proprioception and postural stability after anterior cruciate ligament reconstruction. Br. J. Sports Med. 2008, 42, 373–385. [Google Scholar] [CrossRef] [PubMed]
- Costantino, C.; Bertuletti, S.; Romiti, D. Efficacy of Whole-Body Vibration Board Training on Strength in Athletes After Anterior Cruciate Ligament Reconstruction: A Randomized Controlled Study. Clin. J. Sport Med. 2018, 28, 339–349. [Google Scholar] [CrossRef] [PubMed]
- Sierra-Guzmán, R.; Jiménez-Diaz, F.; Ramírez, C.; Esteban, P.; Abián-Vicén, J. Whole-Body–Vibration Training and Balance in Recreational Athletes with Chronic Ankle Instability. J. Athl. Train. 2018, 53, 355–363. [Google Scholar] [CrossRef]
- Cloak, R.; Nevill, A.; Day, S.; Wyon, M. Six-Week Combined Vibration and Wobble Board Training on Balance and Stability in Footballers with Functional Ankle Instability. Clin. J. Sport Med. 2013, 23, 384–391. [Google Scholar] [CrossRef] [PubMed]
- Sierra-Guzmán, R.; Jiménez, J.F.; Ramírez, C.; Esteban, P.; Abián-Vicén, J. Effects of Synchronous Whole Body Vibration Training on a Soft, Unstable Surface in Athletes with Chronic Ankle Instability. Endoscopy 2017, 38, 447–455. [Google Scholar] [CrossRef]
- Fagnani, F.; Giombini, A.; Di Cesare, A.; Pigozzi, F.; Di Salvo, V. The Effects of a Whole-Body Vibration Program on Muscle Performance and Flexibility in Female Athletes. Am. J. Phys. Med. Rehabil. 2006, 85, 956–962. [Google Scholar] [CrossRef] [Green Version]
- Cochrane, D.J. Acute whole body vibration training increases vertical jump and flexibility performance in elite female field hockey players. Br. J. Sports Med. 2005, 39, 860–865. [Google Scholar] [CrossRef] [PubMed]
- Järvinen, T.; Järvinen, T.; Kääriäinen, M.; Kalimo, H.; Järvinen, M. Biology of muscle trauma. Am. J. Sports Med. 2005, 33, 745–766. [Google Scholar] [CrossRef] [PubMed]
- Games, K.E.; Sefton, J. Whole-body vibration influences lower extremity circulatory and neurological function. Scand. J. Med. Sci. Sports 2013, 23, 516–523. [Google Scholar] [CrossRef] [PubMed]
- Yamada, E.; Kusaka, T.; Miyamoto, K.; Tanaka, S.; Morita, S.; Tanaka, S.; Tsuji, S.; Mori, S.; Norimatsu, H.; Itoh, S. Vastus lateralis oxygenation and blood volume measured by near-infrared spectroscopy during whole body vibration. Clin. Physiol. Funct. Imaging 2005, 25, 203–208. [Google Scholar] [CrossRef] [PubMed]
- Maloney-Hinds, C.; Petrofsky, J.S.; Zimmerman, G. The effect of 30 Hz vs. 50 Hz passive vibration and duration of vibration on skin blood flow in the arm. Med. Sci. Monit. 2008, 14, 112–116. [Google Scholar]
- Lythgo, N.; Eser, P.; De Groot, P.; Galea, M. Whole-body vibration dosage alters leg blood flow. Clin. Physiol. Funct. Imaging 2009, 29, 53–59. [Google Scholar] [CrossRef]
- Coza, A.; Nigg, B.M.; Dunn, J.F. Effects of Vibrations on Gastrocnemius Medialis Tissue Oxygenation. Med. Sci. Sports Exerc. 2011, 43, 509–515. [Google Scholar] [CrossRef]
- Cardinale, M.; Ferrari, M.; Quaresima, V. Gastrocnemius Medialis and Vastus Lateralis Oxygenation during Whole-Body Vibration Exercise. Med. Sci. Sports Exerc. 2007, 39, 694–700. [Google Scholar] [CrossRef]
- Hazell, T.J.; Thomas, G.W.R.; DeGuire, J.R.; Lemon, P.W.R. Vertical whole-body vibration does not increase cardiovascular stress to static semi-squat exercise. Eur. J. Appl. Physiol. 2008, 104, 903–908. [Google Scholar] [CrossRef]
- Team, R.C. R: A Language Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2010. [Google Scholar]
- RStudio. Rstudio: Integrated Development Environment for R. 2014. Available online: https://www.rstudio.com/products/rstudio/ (accessed on 1 August 2021).
- Kerschan-Schindl, K.; Grampp, S.; Henk, C.; Resch, H.; Preisinger, E.; Fialka-Moser, V.; Imhof, H. Whole-body vibration exercise leads to alterations in muscle blood volume. Clin. Physiol. 2001, 21, 377–382. [Google Scholar] [CrossRef]
- Calvisi, V.; Angelozzi, M.; Franco, A.; Mottola, L.; Crisostomi, S.; Corsica, C.; Ferrari, M.; Quaresima, V. Influence of whole-body vibration static exercise on quadriceps oxygenation. In Oxygen Transport to Tissue Xxvii; Cicco, G., Bruley, D.F., Ferrari, M., Harrison, D.K., Eds.; Springer: Boston, MA, USA, 2006; Volume 578, pp. 137–141. [Google Scholar]
- Hortobágyi, T.; Lesinski, M.; Fernandez-del-Olmo, M.; Granacher, U. Small and inconsistent effects of whole body vi-bration on athletic performance: A systematic review and meta-analysis. Eur. J. Appl. Physiol. 2015, 115, 1605–1625. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rønnestad, B.R. Acute Effects of Various Whole-Body Vibration Frequencies on Lower-Body Power in Trained and Untrained Subjects. J. Strength Cond. Res. 2009, 23, 1309–1315. [Google Scholar] [CrossRef] [PubMed]
- Farzam, P.; Starkweather, Z.; Franceschini, M.A. Validation of a novel wearable, wireless technology to estimate oxygen levels and lactate threshold power in the exercising muscle. Physiol. Rep. 2018, 6, e13664. [Google Scholar] [CrossRef] [PubMed]
- Games, K.E.; Sefton, J.M.; Wilson, A.E. Whole-Body Vibration and Blood Flow and Muscle Oxygenation: A Meta-Analysis. J. Athl. Train. 2015, 50, 542–549. [Google Scholar] [CrossRef] [PubMed] [Green Version]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).