Abstract
Background/Objectives: Introducing new transformative surgical technology involves navigating a complex process from design to implementation, often hindered by various barriers that delay the transition into clinical practice. This review critically examines the barriers, proposes a unified guide for medical device implementation in the Australian healthcare system utilising the validated Medtech Innovation Guide, and compares regulatory frameworks in Australia, the United Kingdom, and the United States of America. Methods: We conducted a literature review using MEDLINE and EMBASE with MeSH terms or emtree terms and keywords “new OR novel” AND “surgical device OR medical device OR health technology OR surgical technology OR surgical instrument OR transformative technology OR technological innovation OR technological change” AND “implementation OR adoption OR innovation adoption” AND “surgery OR surgical” AND “Australia”. We also assessed governmental websites (gov.au) and documents as well as the Royal Australasian College of Surgeons (RACS) website, policies, and position statements. Furthermore, Australian medical technology start-up companies were asked for any published roadmaps. Results: Four key stakeholder groups were identified: medical professionals, government, hospitals, and patients/consumers. Barriers include surgeon scepticism, regulatory hurdles (e.g., Australian Register of Therapeutic Goods), hospital clearance processes, and meeting patient expectations. To address these challenges, we propose a five-phase system: surgical device development (phase one), compliance with regulatory processes (phase two), research and experimentation (phase three), finalisation for product launch (phase four), and product launch and assessment (phase five). Conclusions: By following our five-phase guide, innovators may better navigate the complexities of integrating transformative surgical technologies into Australian healthcare. Although there are limitations, this approach is based on the validated Medtech Innovation Guide and may help both experienced and inexperienced practitioners better implement innovative technology; however, real-world validation is required.
1. Introduction
The rapid pace of technological innovation has simplified and organised our lives. Among these advancements, transformative technology stands out. This refers to scientifically proven hardware and/or software that positively impacts the human social experience and enhances our lives [1]. All technology adoption follows a lifecycle: research and development, experimental use, innovation, general use, and eventual obsolescence [2]. For this article, we will be using the terms “surgical/medical technology” and “surgical/medical devices” interchangeably. In Australia, the Therapeutic Goods Administration (TGA) regulates therapeutic goods, ensuring safety through formal certifications. The TGA, part of the Department of Health (DoH), maintains the Australian Register of Therapeutic Goods (ARTG) and uses a risk-based approach to classify devices. Median TGA processing times for medical devices are 156 working days for new devices, and for higher risk devices, additional non-compulsory (average 57 working days) and compulsory (81 working days) audits are required, given 90% already use overseas certification [3]. Once a product is approved, the TGA continues to regulate, ensuring acceptable safety standards are met. As of January 2025, over 95,000 products, ranging from bandages to robotic surgical instruments, are searchable on the ARTG [4,5].
When introduced to Australia in 2003, the DaVinci Robotic Surgical System (Intuitive Surgical, Sunnyvale, CA, USA) was a groundbreaking transformative technology [6]. However, its implementation was not without rigorous testing and development. Although robots have existed for many years, their medical use is relatively new. In the 1980s and 1990s, the Ames Research Center and Stanford University collaborated to develop an advanced telemanipulator, which would serve as the building block of the modern robotic surgical system [7]. Food and Drug Administration (FDA) approval led to a telemanipulator with a foot pedal to steady the operating field view, which evolved into a separate surgeon and patient hub with robotic arms. The DaVinci Robotic Surgical System comprised three main parts in a master-slave composition (the surgeon’s console, the patient’s “trolley” [robot itself], and the imaging system). Whilst the first system had two robotic operating arms and one camera holder, later systems utilised three robotic operating arms, one camera holder, and a three-dimensional, high-definition view, with an installation cost of AUD 3 million. However, being a transformational technology, education and training required significant resources, and there was limited evidence-based benefit to the patient, surgeon, hospital, and government. Despite its potential, the DaVinci system faced significant barriers to adoption, including scepticism, high start-up costs, education and training requirements, and limited evidence-based benefits. Approved by the TGA in October 2003, it remains more common in private than public hospitals largely due to funding constraints [8,9]. The DaVinci Robotic Surgical System highlights several barriers to the introduction of new surgical technology in Australia, whilst this review will focus on new transformative technologies in Australia overall.
Given the lack of studies critically analysing the barriers to surgical technology implementation in Australia, the lack of Australian evidence-based guides to adoption practices, and almost 4000 new ARTG registered devices published annually since 2021, we believe it a prudent topic for review and synthesis [5]. This review aims to critically analyse the barriers to introducing new surgical technology in Australian healthcare, with an emphasis on stakeholders. Additionally, we propose a unified guide for introducing new surgical technology in Australian healthcare.
2. Materials and Methods
We conducted a literature review using MEDLINE and EMBASE with MeSH terms or emtree terms and keywords “new OR novel” AND “surgical device OR medical device OR health technology OR surgical technology OR surgical instrument OR transformative technology OR technological innovation OR technological change” AND “implementation OR adoption OR innovation adoption” AND “surgery OR surgical” AND “Australia”. We also assessed governmental websites (gov.au) and documents as well as the Royal Australasian College of Surgeons (RACS) website, policies, and position statements. Furthermore, Australian medical technology start-up companies were asked for any published roadmaps.
We identified 107 peer-reviewed and published studies, which were included if they described barriers to new technology introduction in Australia and were in the English language. Studies were excluded if they did not meet these criteria. After article assessment, several barriers to surgical technology implementation in Australia were identified, which are summarised through the lens of key stakeholders (medical professionals, government, health services, and patients and consumers) for a comprehensive review.
3. Barriers to Introduction of New Surgical Technology in Australian Healthcare
3.1. Medical Professionals
Medical professionals often approach new technology with scepticism, relying on evidence-based practices and opinions from specialty leaders to guide clinical decisions [10]. Opinions from fellow surgeons, conferences, and publications also influence adoption [11]. Another barrier is the perceived risk of negative clinical outcomes and reputational damage. Adopting new technology involves overcoming technical skill challenges and adjusting established practices, leading to a steep learning curve (the rate one acquires a new skill) and missed opportunity costs (potential benefits when choosing one alternative over another) [12]. For example, robotic urological procedures require 12 to 140 patients to overcome the learning curve, as noted in an international systematic review in 2019, which is comparable to a recent Australian study that identified 65 cases for robotic-assisted radical prostatectomy (RARP) [13,14]. However, learning curve assessment methods are heterogenous and often lack statistical validation. New skills involving transformative technology, such as robotic surgery, often require sub-specialty training, commonly a Fellowship, which involves time, money, resources, and sometimes international relocation. Some surgical techniques require interdisciplinary efforts, adding logistical barriers like organisational structure, defined boundaries, resource allocation, and remuneration structures [11]. Additionally, clinician-innovators must apply for patents to protect intellectual property. The invention must be novel, useful, and sufficiently different from existing technologies. Medical and biotechnology products can be patented for up to 20 years; however, applications may take months to years [15]. Without patents, developers may rush products without ensuring technical and safety specifications and clinical effectiveness.
3.2. Government
Several federal regulations and guidelines govern the introduction of new surgical technology, acting as gateways to the healthcare system. Figure 1 highlights the overall steps to navigating the Australian medical device regulatory framework. The TGA defines a medical device as one used for diagnosing, preventing, monitoring, predicting outcomes, treating, or easing symptoms of medical conditions [16]. This definition also includes devices for body part replacement/enhancement, conception control/support, and examining human specimens. Devices are classified by risk level from Class I (low risk) to Class III (high risk), with higher classifications requiring stricter standards. Several questions are considered prior to classification, relating to the intent and duration of use, location of use in the body, and the device’s invasiveness. Examples include surgical retractors (Class I) and prosthetic heart valves (Class III) [17]. The TGA ensures compliance with six general and nine design and construction principles, named the Essential Principles, with application fees ranging from AUD 602 to 1483.
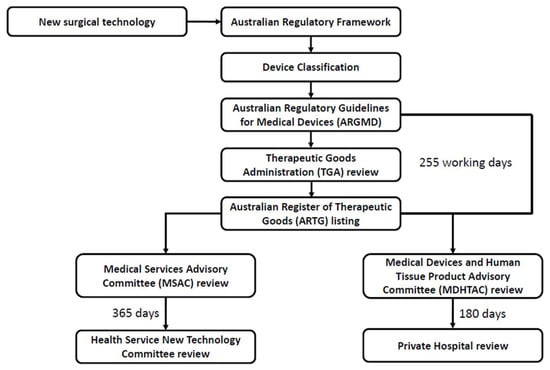
Figure 1.
Regulatory flowchart of new surgical device implementation in Australian public and private health services.
The Australian Regulatory Guidelines for Medical Devices (ARGMD) provide information on importing, exporting, and supplying medical devices in Australia. These guidelines include the Essential Principles, as above, and an additional conformity assessment to ensure devices meet safety and performance standards, with fees ranging from AUD 62,380 to 86,903 for partial to full assessments [18,19]. Compliance with these principles and assessments is required before inclusion in the ARTG. Once included, devices must continue meeting standards, and failures are systematically investigated to prevent further issues [18]. Overall, the regulatory framework for medical devices includes pre-market authorisation, inclusion in the ARTG, and post-market monitoring. Additionally, there are legislative requirements to complete device evaluation in the standard pathway within 255 working days, with a median of 161 working days, delaying development [20].
At the state level, the Victorian DoH offers policy guidance on health technology in public healthcare. Key components include the Victorian Health Technology Program (VHTP), VHTP Advisory Group, Highly Specialised Therapies program, and Nationally Funded Centres program [21]. The Victorian DoH defines “health technology” as a prosthesis, implantable device, diagnostic test, medical procedure, surgical procedure, clinical program or highly specialised therapy or service as defined by the 2020–25 National Health Reform Agreement. The VHTP reviews new and existing technologies for safety, clinical effectiveness, cost-effectiveness, budget impact, and implementation [22]. Advisory Groups are health service-dependent, provide expert advice to the Victorian DoH, and consist of health service “new technology committees” that offer local governance for new technologies, reporting progress every six months for two years. However, individual healthcare systems have separate policies, creating a lack of unified guidelines for technology adoption. Additionally, guidelines for public healthcare may not apply to the private sector.
The Industry Growth Program, funded by the Australian Government, involves the support of small to medium enterprises and start-ups for the commercialisation of ideas [23]. The National Reconstruction Fund prioritises medical science aiming to provide cost-effective and safe technologies [24]. Importantly, adequate funding to the healthcare system ensures appropriate utilisation of resources and efficient workflow to provide the best possible care. Effective healthcare workflow depends on the collaboration of patient, caregiver, and technology [25,26]. Resource allocation from the government and the individual healthcare networks has an impact on the care of the patient. New technology adoption requires significant initial resources for safe and efficient use. Without financial, commercial, and developmental support, innovative technologies may struggle to improve healthcare.
Appropriate remuneration systems are essential for surgical technology adoption. Without funding, new devices are unlikely to reach general use. The Medicare Benefits Schedule (MBS), managed by the Australian Government DoH, provides rebates for public healthcare services rendered but does not cover all services, like private hospital care. Private health insurance covers these costs, but policies and practitioner remuneration vary widely [27,28].
The Medical Services Advisory Committee (MSAC), established by the Australian Government Minister for Health in 1998, is an independent non-statutory committee that appraises new medical services proposed for public funding. MSAC provides advice to the Minister for Health on the safety, effectiveness, and cost-effectiveness of new medical technologies and procedures and informs Australian Government decisions for public funding [29]. Applications to the Department for MSAC can be made for medical services not currently covered under the MBS, such as with new surgical technology. Generally, whilst most applicants seek reimbursement under the MBS, MSAC can provide advice in regards to non-MBS funding. Without remuneration, the cost of new surgical technology usage falls on the hospital and the patient, thereby preventing adoption in public healthcare, with medical ethics and indemnity being additional concerns. Overall, therapeutic goods, such as medical devices, are able to acquire MSAC approval post-market authorisation (i.e., listing on the ARTG), which can take 12 months and include two consultation rounds and a final MSAC review on the Standard pathway (involving population, intervention, comparator, outcome [PICO] health technology assessment) [30].
3.3. Health Services
To ensure the appropriate utilisation of funds, each health service establishes a set of relationships and responsibilities among the DoH, governing body, executive members, workforce, patients, consumers, and other stakeholders through clinical governance. This is integral to the success of a health care service, ensuring good clinical practice and outcomes [31]. Figure 2 demonstrates the implementation of a new surgical device in a health service. The National Model Clinical Governance Framework (2017) was developed to ensure consistent implementation of key clinical governance processes across health service organisations. It supports shared accountability among all healthcare workers, from frontline clinicians to governing body members, in providing safe, effective, integrated, high-quality, and continuously improving healthcare [31]. Continuous improvement includes introducing new technology or procedures, requiring staff education and training, researching clinical effectiveness, and regular auditing. However, this depends on the funding provided to the health service, which may not always align with community needs or best medical practice. Therefore, each health service must ensure adequate research on community needs to tailor the experience for their region.
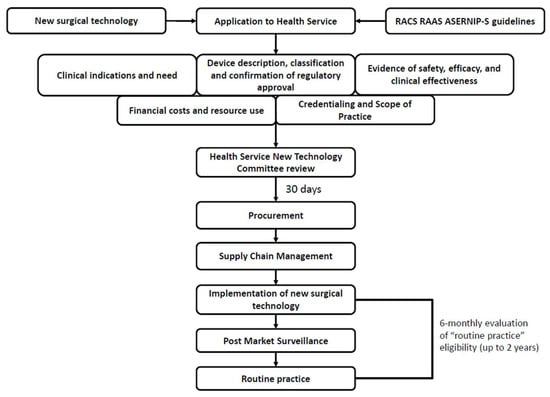
Figure 2.
Public health service flowchart of new surgical device implementation in Australian healthcare. Legend: RACS, Royal Australian College of Surgeons; RAAS, Research Audit and Academic Surgery; ASERNIP-S, Australian Safety and Efficacy Register of New Interventional Procedures—Surgical.
The Research, Audit, and Academic Surgery (RAAS) division of RACS evaluates new and emerging surgical procedures and technologies. Through Health Technology Assessment, they systematically evaluate clinical safety, efficacy, and cost-effectiveness, among other areas. Their aim is to synthesise evidence to bridge the gap between primary evidence and health policy. For new procedures, the Australian Safety and Efficacy Register of New Interventional Procedures—Surgical, established in 1998, is part of RAAS and works with MSAC, advising the Australian Minister for Health on new surgical procedures for public funding [32,33]. Assessments and clinical recommendations are disseminated to key stakeholders. This division serves as an independent advisor for health policy and can significantly influence the implementation of new surgical technology based on scientific evidence [34]. Additionally, RACS provides a guide for introducing new techniques and technologies into a health service to overcome the aforementioned and following obstacles [34].
Introducing new technology or clinical practice requires oversight by a “new technology committee” as stipulated by the Victorian DoH. The Austin Health New Technology/Clinical Practice (NTCP) Committee ensures that new technology, clinical practices, or other interventions are appropriately assessed [35]. This involves evaluating the risks and benefits, care outcomes, clinical and occupational risks, and potential costs. The NTCP Committee defines new technology/clinical practice as any therapeutic intervention, diagnostic procedure, or variation in existing equipment, procedures, or treatments [35]. They meet six times a year, with applications closing two weeks prior, and continue six-monthly evaluation for two years after implementation to determine “routine practice” eligibility. NTCP Committee results are provided two weeks after the meeting. Thus, new technology aiming to be implemented in multiple healthcare systems must undergo rigorous testing, which can take years to adopt due to a decentralized approach.
After hospital approval, the next step is procurement, which encompasses buying goods and services. The process includes identifying a need, deciding to purchase, assessing risks, evaluating alternatives, and awarding a contract [36]. Healthcare systems also follow this procurement approach and employ a “perioperative services inventory and equipment manager” such as at Austin Health. At an executive level, the Chief Financial Officer of the health service holds overall responsibility for procurement. However, identifying who makes the actual purchase—whether it is the surgeon, the hospital, the procurement officer, or another person—remains challenging.
Once procurement approval and a contractual relationship with the vendor are established, additional barriers arise from logistics and supply chains. Effective communication ensures that the appropriate product is ordered in the correct quantity and delivered to the right site at the right time. Proper distribution, timely transport, and the appropriate receiving of goods are essential [37]. Hospital storage, usage, sterilisation, and disposal are also critical to successful device implementation [38].
Comparing the public and private healthcare systems reveals notable differences in the implementation of transformative surgical technology. The public health system must notify the Victorian DoH through “new technology committees” to implement new devices. In contrast, the private healthcare system operates independently, utilising equipment without the funding restrictions of public healthcare but relying on Private Health Insurance funds for remuneration. The Prescribed List of Medical Devices and Human Tissue Products (formally known as the Prosthesis List) is a collection of approved health technologies, ensuring that privately insured patients have access to clinically effective medical devices and human tissue products [39,40]. Under the Private Health Insurance Act 2007, private health insurers must pay benefits for patients who receive medical devices during hospital treatment if a Medicare benefit is payable [39]. Reimbursement is determined by the clinical effectiveness of the medical device; hence, devices with better clinical effect are better reimbursed. Health professionals are essentially encouraged to utilise devices on the Prescribed List through improved remuneration for devices with known clinical effectiveness, ensuring safe and clinically proven care. The Prescribed List is updated three times a year (March, July, and November) and is regulated by the Medical Devices and Human Tissue Product Advisory Committee (MDHTAC), with application cut-offs 6 months prior [41].
The MDHTAC assesses the clinical effectiveness of medical devices and their proposed benefits to inform reimbursement decisions by private health insurers. New technology intended for use in the private health system requires Prescribed List approval for translation into practice. Without listing, the cost would likely be passed to the patient due to the lack of reimbursement by the health insurer. Strict criteria for general listing include ARTG inclusion, use as part of hospital treatment, Medicare benefit payable for the associated product, and non-inferiority compared to existing devices. There may be medico-legal implications for new technology not supported by the Prescribed List. However, without clinical data, it can be challenging for the MDHTAC to advise the Minister for Health to support its addition to the Prescribed List [39,42]. Additional fees for application, listing, and ongoing retention of a medical device range from AUD 1422 to 34,305, with an additional AUD 151 Prescribed List levy, further adding to the barriers of implementation [43].
3.4. Patients and Consumers
Recommending new technology in healthcare involves discussion with the community, comprising key stakeholders. Public approval is essential for successful technology adoption. As clinicians, we must meet our patients’ expectations and uphold our ethical principles of autonomy, beneficence, non-maleficence, and justice [44]. This means respecting a person’s right to self-determination, having a duty to do good, to not do harm, and treat all people equally and equitably.
There are also community and patient expectations with regards to evolving technology: the need to test new theories, scepticism of new devices and their safety profile, and the avoidance of untested products [45]. Balancing these expectations with bioethical principles ensures risk minimisation [46]. Before applying new technology in a test population, the Human Research and Ethics Committee (HREC) must approve the experiment to ensure safety; additionally informed consent must be sought under the Mental Health and Wellbeing Act [47]. Requirements for informed consent include the person’s capacity, adequate information provided, and the opportunity to decide. Consent must be given freely without coercion and can be withdrawn at any time. Interestingly, public acceptance of novel health technologies can be alleviated with consumer understanding, while others actually prefer new technology in specific situations [48].
In new technology trials, clear indications for the procedure must be highlighted, including differences from standard treatment, potential and specific risks, areas of uncertainty, alternative treatment options, data recording and deidentification, access to research materials, and the right to withdraw [47]. Bioethical principles and patient/community expectations are challenges to new technology implementation that require forethought and clinical robustness.
4. How to Implement New Devices in Surgical Practice
Introducing new transformative technology into Australian healthcare involves navigating a complex process, highlighted by significant barriers. Utilising the Medtech Innovation Guide, we propose a simplified five-phase guide to new surgical technology implementation in the Australian healthcare system to improve device adoption [49]. Imagine you are a clinician who identifies an unresolved clinical problem and is developing a novel transformative surgical device for clinical practice. There are several phases detailed below (Table 1):

Table 1.
Introducing new surgical technology into Australian healthcare.
- Development of the device.
Includes device creation, from problem identification, conceptualisation, market analysis and consumer review, finances, patents, and International Organisation for Standardisation (ISO) certification.
- 2.
- Compliance with regulatory processes.
Primarily refers to the TGA regulations, which include the Essential Principles, ARGMD guidelines, and conformity assessment certification. MSAC approval can only be gained after market authorisation (unless exempt), generally post ARTG listing [30].
- 3.
- Research clinical benefits compared to standard care.
Clinicians are most familiar with this phase, which includes HREC approval and clinical trials. However, surgical device refining, consumer and patient reviews, and public and private healthcare applications are also important.
- 4.
- Finalise device for product launch.
Completion of patents, product branding, regulatory clearance, and device refinement are important to ensure a successful launch. Additionally, finalising public and private hospital reimbursement strategies and Prescribed List approval is essential for rapid uptake.
- 5.
- Launch device and assessment.
Successful product launch requires appropriate marketing, sales and distribution, and management of supply chains. Additionally, post-market surveillance and audits are essential for assessing the quality of surgical devices and ensuring proactive refinement.
Not every device will succeed due to the many barriers to implementing surgical technology. Technology implementation can be delayed or accelerated depending on various circumstances. Lottes et al. (2022) suggests that collaboration between clinicians, regulators, and industry is essential for successful innovative medical device translation to practice [50]. However, given the vast array of regulatory requirements from development to research and implementation, innovators may find it challenging to initiate technological advancement without adequate knowledge. Our proposed guide may help clinicians and innovators better understand the required processes and procedures in Australia. Notably, parts of each phase may occur simultaneously (e.g., consumer review and product branding) or may prevent progression due to legislative requirements (e.g., Essential Principles and conformity assessment).
While a one-size-fits-all approach may not be the most useful, given the lack of accessible published guides and the potentially secretive nature of medical technology enterprise implementation, we propose a clear, easy-to-understand guide for the inexperienced. It may also remind experienced practitioners of the necessary steps for new device introduction and the sequential and overlapping order of operations.
5. Discussion
We have identified several key barriers to introducing new surgical technology into Australian healthcare through the lens of medical professionals, government, health services, and patients and consumers. Recalling the DaVinci Robotic Surgical System, the diffusion of robotic surgery is an important example of how transformative technology can be controversial due to high healthcare costs, implementation despite early lack of evidence base, and marketing that thrives on surgeon and patient fear [51].
The installation cost of the DaVinci XI (Intuitive Surgical, Inc.) is over AUD 3 million, with additional consumable costs of AUD 1848 per operation, and service costs of AUD 621,245 for a 3-year contract [9]. Recent studies comparing robotic to laparoscopic and open radical prostatectomy demonstrated statistically significant findings for and against the robotic approach; nerve sparing procedures (85% vs. 95% vs. 90%, p < 0.001), lymphadenectomy (11% vs. 22% vs. 100%, p < 0.001), blood transfusion rates (4.5% vs. 1.8% vs. 21.0%, p = 0.001), median operating room time (235 min vs. 225 min vs. 198 min, p < 0.001), mean length of hospital stay (1 day vs. 2 days vs. 2 days, p < 0.0001), and median direct costs (USD 6752 vs. 5687 vs. 4437, p < 0.0001), respectively [52]. Findings demonstrate improved blood transfusion rates and shorter hospital stay at the expense of longer operating times and direct costs. However, the primary outcome investigated was cost and not related to oncologic or functional outcomes. The most pertinent randomised control trial is an Australian study comparing RARP to open radical retropubic prostatectomy (RRP), published more than 10 years after TGA approval, which demonstrated similar functional outcomes at 24 months [53,54].
Almost 10 years later, the first network meta-analysis comparing oncologic and functional outcomes of RRP, laparoscopic radical prostatectomy (LRP), and RARP demonstrated significantly lower biochemical recurrence (RARP vs. RRP 0.69; 95% confidence interval [CI] 0.52–0.90), and better 3-month erectile function recovery (RARP vs. LRP, odds ratio [OR] 2.45; 95% CI 1.52–3.78; RARP vs. RRP, OR 2.64; 95% CI 1.38–5.62) [55]. However, despite the clinical benefits lagging, there were immediate surgeon-specific benefits, such as three-dimensional vision, stable camera, improved surgeon ergonomics and accuracy, and better range of motion due to articulated robotic instruments [56,57]. In terms of early fear-mongering marketing, from a patient and consumer view, hearing about a new product that can improve surgeon precision and accuracy can lead to its demand due to fear of a lesser outcome. Whilst, surgeons potentially view the lack of “cutting edge” technology in their armamentarium as being seen as antiquated [51]. The robotic surgical experience is not an unusual story for medical technology implementation and highlights the significant start-up and ongoing costs, delay to evidence-based practice, and patient factors.
With the DaVinci patent expiring in 2019, there has been a surge in new robotic-assisted surgery alternatives, which have implications for affordability, access, improved surgeon experience, and niche operative robots [58]. However, the same challenges DaVinci encountered remain, which medical technology companies must overcome to ensure widespread adoption. In its pre-budget report, the Medical Technology Association of Australia (MTAA), which is the national association representing the medical technology industry, provided eight key recommendations, including a 50% increase in TGA medical device activity funding to ensure patient access to medical devices [59]. Announced in March 2025, the Australian 2025–26 budget failed to include new funding for medical device support, instead focusing on its systems, with AUD 207 million over 2 years for the Australian Securities and Investments Commission’s business registers and AUD 151 million over 4 years for the fraud detection information technology system in the National Disability Insurance Agency [60]. With a rising gross domestic product contribution of AUD 5.4 billion in the 2023/24 financial year, governmental medical technology funding is primarily through the Industry Growth Program (grants up to AUD 5 million) and National Critical Research Infrastructure initiative (AUD 600 million over the next 10 years) [23,61]. Additionally, the Medical Science Co-investment Plan emphasises collaboration between government, industry, and the National Reconstruction Fund and aims to facilitate Australian industrial capability and capacity, support commercialisation, and improve international competitiveness [62]. However, according to MTAA, there are significant bottlenecks to market access leading to regulatory delays and reimbursement approvals, a lack of clear policy and guidelines, and a talent shortage, highlighting the need for improved funding [63].
Medical technology remains essential to the economy and to contemporary medical practice [62,64]. Therefore, guidelines, such as our five-phase guide, simplifying systems and processes, are important to improving implementation. As clinicians, we are actual users of medical technology and must focus on its evidence base and not fall prey to marketing. Furthermore, we must be stringent with its introduction into our surgical repertoire, whilst being cognisant of our bioethical responsibilities to our patients [64,65]. With the gold standard of double-blind randomised control trials, “sham surgery” poses an unacceptable risk to patients through infection, general anaesthesia, pain, and stress, without actual treatment in a control population, and alternatives must be pursued [50,66].
Australia’s medical device regulatory framework compares to the United Kingdom (UK) and the United States of America (USA) [67]. Legislative requirements for UK medical devices include the Consumer Protection Act 1987, Medical Device Regulations 2002 based on the Medical Device Directive of the European Union, and General Product Safety Regulations (2005) [68,69,70,71]. The USA has the Food, Drug and Cosmetic Act 1938, which includes the 21 Code of Federal Regulations [72]. Similarities between the Australian, UK, and USA frameworks include a distinct government regulator (TGA vs. Medicines and Healthcare Products Regulatory Agency vs. FDA, respectively) [73,74], principle-based regulation [67], and a risk-based Medical Device Classification System [67]. Differences include a lack of government regulatory review and product approval for market use in the UK as well as an acceptance of third-party reviews in both the UK (in accordance with the device directives) and the USA (still subject to FDA final approval) [67].
Given the similarities in UK and USA regulatory frameworks, the TGA has an expedited Priority Review pathway for medical devices, with overseas conformity assessments and successful priority applicant determination [75]. The medical device must meet three major criteria: intends to treat, prevent, or diagnose a life-threatening/debilitating condition; no devices with the intended purpose are in the ARTG or there is substantial evidence of significant improvement compared to existing devices; there is a major clinical/public health benefit [75]. Whilst there is no legislated timeframe, the TGA aims to assess applicants for eligibility in the Priority Review pathway within 20 working days, with subsequent addition to the “front of the queue” ARTG listing consideration. This may significantly shorten the 255 working day Standard Pathway; however, an additional AUD 11,641 is required [75].
Our five-phase guide was developed as a simplified version of the Medtech Innovation Guide and is specifically designed for the Australian healthcare system. The Medtech Innovation Guide is a Swedish empiric model to support medical technology innovation [49]. Published in 2022, it utilises several themes, including “Conceptualisation”, “Concept validation”, “Product development”, and “Product launch”, which mirrors our “Development”, “Compliance”, “Research”, “Finalise”, and “Launch” phases. Additionally, the Swedish guide has been externally validated through implementation research such as MediGate, describing case studies that include an albumin strip test, an artificial intelligence platform for depression detection, and a 3D-printed patient-specific implant [76]. However, it provides a general overview rather than focusing on specific markets and regulatory frameworks. Utilising Figure 1 and Figure 2, a conservative estimate to reach the procurement phase from a regulatory application is over 700 days or almost 2 years (Phase two) and does not include development (Phase one—2 to 3 years), research (Phase three—2 to 3 years), finalisation (Phase four—1 to 2 years), and launch (Phase five—1 year), which add an additional 6 to 10 years [77,78,79]. Therefore, when adding up the potential time to bringing a medical device from concept to implementation, a conservative estimate is 10 to 15 years. To date, we believe no study provides an Australian-specific review of barriers and an associated guide to new surgical technology implementation.
6. Limitations
Given the review format of our study, limitations include a heavy reliance on governmental documents over academic literature. With a scarcity of peer-reviewed articles critically analysing the Australian regulatory process and barriers to implementing new medical devices, it is difficult to comprehensively examine the topic without referencing important governmental articles. Additionally, much of the work may be considered speculative, and without validation, it is difficult to determine our guide’s true impact. However, given the paucity of literature and development based on the validated Medtech Innovation Guide, this may be a first step to improving academic guidelines to navigate the Australian health technology system, though real-world validation is required.
7. Conclusions
Transformative surgical technology leads healthcare innovation, aiming to provide more efficient, safe, and improved solutions to everyday problems. Implementing this technology in Australian healthcare requires navigating a complex system involving surgeon preferences and training, governmental regulations, hospital policies, and consumer expectations. The dual emphasis on public and private systems in Australia adds further complexity. Although there are limitations, our five-phase guide is based on the validated Medtech Innovation Guide and may help both experienced and inexperienced practitioners better implement innovative technology in Australian healthcare; however, real-world validation is required.
Author Contributions
Writing—original draft preparation, review and editing, and conceptualisation M.A.; writing—review and editing, J.X. and O.P.; conceptualisation, supervision, and methodology, D.B. and J.I. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
No specific data is presented.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript in order of appearance:
| TGA | Therapeutic Goods Administration |
| DoH | Department of Health |
| ARTG | Australian Register of Therapeutic Goods |
| FDA | Food and Drug Administration |
| RACS | Royal Australasian College of Surgeons |
| RARP | Robotic Assisted Radical Prostatectomy |
| ARGMD | Australian Regulatory Guidelines for Medical Devices |
| VHTP | Victorian Health Technology Program |
| MBS | Medicare Benefits Schedule |
| MSAC | Medical Services Advisory Committee |
| PICO | Population, Intervention, Comparator, Outcome |
| ASERNIP-S | Australian Safety and Efficacy Register of New Interventional Procedures—Surgical |
| RAAS | Research, Audit, and Academic Surgery |
| NTCP | New Technology/Clinical Practice |
| MDHTAC | Medical Devices and Human Tissue Product Advisory Committee |
| HREC | Human Research and Ethics Committee |
| ISO | International Organisation for Standardisation |
| RRP | Radical Retropubic Prostatectomy |
| LRP | Laparoscopic Radical Prostatectomy |
| CI | Confidence Interval |
| OR | Odds Ratio |
| MTAA | Medical Technology Association of Australia |
| UK | United Kingdom |
| USA | United States of America |
References
- Jarvenpaa, S.L.; Ives, B. Introducing Transformational Information Technologies: The Case of the World Wide Web Technology. Int. J. Electron. Commer. 1996, 1, 95–126. [Google Scholar] [CrossRef]
- Mytton, O.T.; Velazquez, A.; Banken, R.; Mathew, J.L.; Ikonen, T.S.; Taylor, K.; Painter, F.; Jean-Baptiste, R.; Poon, A.; Ruelas, E. Introducing new technology safely. Qual. Saf. Health Care 2010, 19 (Suppl. 2), i9–i14. [Google Scholar] [CrossRef]
- Department of Health, Disability, and Ageing AG. Understanding Processing Timeframes for Medical Device Applications. 2022; (updated 1 October 2024). Available online: https://www.tga.gov.au/resources/guidance/understanding-processing-timeframes-medical-device-applications (accessed on 18 May 2024).
- Ghosh, D.; Skinner, M.; Ferguson, L.R. The role of the Therapeutic Goods Administration and the Medicine and Medical Devices Safety Authority in evaluating complementary and alternative medicines in Australia and New Zealand. Toxicology 2006, 221, 88–94. [Google Scholar] [CrossRef] [PubMed]
- Department of Health, Disability, and Ageing AG. Australian Register of Therapeutic Goods (ARTG). 2024. Available online: https://www.tga.gov.au/resources/artg (accessed on 18 May 2024).
- Costello, A.J.; Haxhimolla, H.; Crowe, H.; Peters, J.S. Installation of telerobotic surgery and initial experience with telerobotic radical prostatectomy. BJU Int. 2005, 96, 34–38. [Google Scholar] [CrossRef] [PubMed]
- Shah, J.; Vyas, A.; Vyas, D. The History of Robotics in Surgical Specialties. Am. J. Robot. Surg. 2014, 1, 12–20. [Google Scholar] [PubMed]
- Royal Australasian College of Surgeons (RACS). Robot-Assisted Surgery Working Party [Electronic Book]. 2023. Available online: https://www.surgeons.org/-/media/Project/RACS/surgeons-org/files/Marketing/Robot-Assisted-Surgery-Working-Party-Final-Report-and-Recommendations_June-2023.pdf?rev=de2285127fc84b038b21bde393e5f3cb&hash=78350E31C5DBF7AB1A500D59878400A0 (accessed on 11 July 2024).
- McBride, K.; Steffens, D.; Stanislaus, C.; Solomon, M.; Anderson, T.; Thanigasalam, R.; Leslie, S.; Bannon, P.G. Detailed cost of robotic-assisted surgery in the Australian public health sector: From implementation to a multi-specialty caseload. BMC Health Serv. Res. 2021, 21, 108. [Google Scholar] [CrossRef]
- Safi, S.; Thiessen, T.; Schmailzl, K.J. Acceptance and Resistance of New Digital Technologies in Medicine: Qualitative Study. JMIR Res. Protoc. 2018, 7, e11072. [Google Scholar] [CrossRef]
- Konda, N.N.; Lewis, T.L.; Furness, H.N.; Miller, G.W.; Metcalfe, A.J.; Ellard, D.R. Surgeon views regarding the adoption of a novel surgical innovation into clinical practice: Systematic review. BJS Open 2024, 8, zrad141. [Google Scholar] [CrossRef]
- Hopper, A.N.; Jamison, M.H.; Lewis, W.G. Learning curves in surgical practice. Postgrad. Med. J. 2007, 83, 777–779. [Google Scholar] [CrossRef]
- Soomro, N.A.; Hashimoto, D.A.; Porteous, A.J.; Ridley, C.J.A.; Marsh, W.J.; Ditto, R.; Roy, S. Systematic review of learning curves in robot-assisted surgery. BJS Open 2020, 4, 27–44. [Google Scholar] [CrossRef]
- Perera, S.; Fernando, N.; O’Brien, J.; Murphy, D.; Lawrentschuk, N. Robotic-assisted radical prostatectomy: Learning curves and outcomes from an Australian perspective. Prostate Int. 2023, 11, 51–57. [Google Scholar] [CrossRef] [PubMed]
- IP Australia AG. What Are Patents? 2024. Available online: https://www.ipaustralia.gov.au/patents/what-are-patents (accessed on 15 July 2024).
- Department of Health, Disability and Ageing AG. Therapeutic Goods Act 1989. Available online: https://www.legislation.gov.au/C2004A03952/latest/text/2 (accessed on 15 July 2024).
- Department of Health, Disability and Ageing AG. Medical Devices Overview. 2022. Available online: https://www.tga.gov.au/products/medical-devices/medical-devices-overview#classification (accessed on 18 May 2024).
- Department of Health, Disability and Ageing AG. Australian Regulatory Guidelines for Medical Devices (ARGMD). 2023. Available online: https://www.tga.gov.au/resources/resource/guidance/australian-regulatory-guidelines-medical-devices-argmd#essential-principles (accessed on 18 May 2024).
- Australian Government. Fees and Charges: Summary; Department of Health and Aged Care; Therapeutic Goods Administration: Woden, ACT, Australia, 2025.
- Department of Health and Aged Care AG. Health Technology Assessment Policy and Methods Review: Australian Market Authorisation, Funding and Assessment Pathways and Timelines. 2024. Available online: https://www.health.gov.au/sites/default/files/2024-07/hta-policy-and-methods-review-australian-market-authorisation-funding-and-assessment-pathways-and-timelines.pdf (accessed on 19 February 2025).
- Department of Health VG. Health Technology Program. 2023. Available online: https://www.health.vic.gov.au/patient-care/health-technology-program (accessed on 18 May 2024).
- Department of Health VG. Victorian Health Technology Program. 2023. Available online: https://www.health.vic.gov.au/patient-care/victorian-health-technology-program (accessed on 18 May 2024).
- Department of Industry, Science and Resources AG. Industry Growth Program. 2024. Available online: https://www.industry.gov.au/science-technology-and-innovation/industry-innovation/industry-growth-program (accessed on 1 July 2024).
- Department of Industry, Science and Resources AG. Promoting and Protecting Critical Technologies. 2024. Available online: https://www.industry.gov.au/science-technology-and-innovation/technology (accessed on 1 July 2024).
- Davis, M.M.; Gunn, R.; Cifuentes, M.; Khatri, P.; Hall, J.; Gilchrist, E.; Peek, C.J.; Klowden, M.; Lazarus, J.A.; Miller, B.F.; et al. Clinical Workflows and the Associated Tasks and Behaviors to Support Delivery of Integrated Behavioral Health and Primary Care. J. Ambul. Care Manag. 2019, 42, 51–65. [Google Scholar] [CrossRef]
- Bowens, F.M.; Frye, P.A.; Jones, W.A. Health information technology: Integration of clinical workflow into meaningful use of electronic health records. Perspect. Health Inf. Manag. 2010, 7, 1d. [Google Scholar] [PubMed]
- Department of Health, Disability and Ageing AG. MBS Online. 2024. Available online: https://www.mbsonline.gov.au/internet/mbsonline/publishing.nsf/Content/Home (accessed on 18 May 2024).
- Department of Health, Disability and Ageing AG. About Private Health Insurance. 2021. Available online: https://www.health.gov.au/topics/private-health-insurance/about-private-health-insurance (accessed on 18 May 2024).
- Department of Health, Disability and Ageing AG. What We Do 2024. Available online: https://www.msac.gov.au/about-us/what-we-do (accessed on 4 March 2025).
- Department of Health, Disability and Ageing AG. Application Timelines. 2024. Available online: https://www.msac.gov.au/apply/before-you-apply/application-timelines (accessed on 2 April 2025).
- Australian Commission on Safety and Quality in Health Care. Clinical Governance. 2024. Available online: https://www.safetyandquality.gov.au/our-work/clinical-governance#:~:text=Clinical%20governance%20is%20the%20set,to%20ensure%20good%20clinical%20outcomes (accessed on 1 July 2024).
- Royal Australasian College of Surgeons (RACS). Research & Evaluation, Inc. ASERNIP-S. 2024. Available online: https://www.surgeons.org/research-audit/research-evaluation-inc-asernips (accessed on 10 July 2024).
- Maddern, G.; Boult, M.; Ahern, E.; Babidge, W. ASERNIP-S: International trend setting. ANZ J. Surg. 2008, 78, 853–858. [Google Scholar] [CrossRef]
- Royal Australasian College of Surgeons (RACS) A-S. General Guidelines for Assessing, Approving & Introducing New Surgical Procedures into a Hospital or Health Service. 2008. Available online: https://www.surgeons.org/-/media/Project/RACS/surgeons-org/files/position-papers/rea_ase_3103_p_general_guidelines_for_assessing_approving_introducing_new_surgical_procedures_into_a.pdf?rev=40cc6edcb50c40d3baf777bb2f98ad68&hash=F81D0558402F1F7229CC070E1647FA8C (accessed on 10 July 2024).
- Austin Health. Austin 2025 Clinical Services Plan. 2024. Available online: https://www.austin.org.au/Assets/Files/Austin%202025%20Clinical%20Services%20Plan.pdf (accessed on 1 July 2024).
- Department of Finance AG. What Is Procurement? 2024. Available online: https://sellingtogov.finance.gov.au/guide/introduction-a-guide-to-government-procurement#:~:text=Procurement%20is%20a%20term%20used,buy%20to%20meet%20this%20need (accessed on 1 July 2024).
- National Academy of Engineering (US) and Institute of Medicine (US) Committee on Engineering and the Health Care System. Building a Better Delivery System: A New Engineering/Health Care Partnership [Internet]; Reid, P.P., Compton, W.D., Grossman, J.H., Fanjiang, G., Eds.; National Academies Press (US): Washington, DC, USA, 2005. Available online: https://nap.nationalacademies.org/catalog/11378/building-a-better-delivery-system-a-new-engineeringhealth-care-partnership (accessed on 3 April 2025).
- Rutala, W.A.; Weber, D.J. Disinfection and Sterilization in Health Care Facilities: An Overview and Current Issues. Infect. Dis. Clin. N. Am. 2016, 30, 609–637. [Google Scholar] [CrossRef] [PubMed]
- Department of Health, Disability and Ageing AG. Medical Devices and Human Tissue Products Covered Under Private Health Insurance. 2017. Available online: https://www.health.gov.au/topics/private-health-insurance/what-private-health-insurance-covers/medical-devices-and-human-tissue-products-covered-under-private-health-insurance?language=und (accessed on 1 July 2024).
- Department of Health, Disability and Ageing AG. About the Prescribed List. 2025. Available online: https://www.health.gov.au/our-work/the-prescribed-list/about (accessed on 3 April 2025).
- Australian Government. The Prescribed List of Medical Devices and Human Tissue Products Guide—DRAFT; Department of Health and Aged Care: Phillip, ACT, Australia, 2023.
- Department of Health, Disability and Ageing AG. Medical Devices and Human Tissue Advisory Committee (MDHTAC). 2025. Available online: https://www.health.gov.au/committees-and-groups/medical-devices-and-human-tissue-advisory-committee-mdhtac (accessed on 3 April 2025).
- Australian Government. Cost Recovery Implementation Statement—Administration of the Prescribed List of Medical Devices and Human Tissue Products; Department of Health and Aged Care: Phillip, ACT, Australia, 2024.
- Varkey, B. Principles of Clinical Ethics and Their Application to Practice. Med. Princ. Pract. 2021, 30, 17–28. [Google Scholar] [CrossRef]
- Miller, M.E.; Siegler, M.; Angelos, P. Ethical issues in surgical innovation. World J. Surg. 2014, 38, 1638–1643. [Google Scholar] [CrossRef]
- Ravan, N.; Hasanzad, M.; Larijani, B.; Namazi, H. Ethical Concerns in Novel Medicine. In A Glimpse at Medicine in the Future; Hasanzad, M., Ed.; Springer Nature: Singapore, 2024; pp. 201–212. [Google Scholar]
- Department of Health VG. Informed Consent and Presumption of Capacity. 2022. Available online: https://www.health.vic.gov.au/mental-health-and-wellbeing-act-handbook/supported-decision-making/informed-consent-and-presumption (accessed on 3 July 2024).
- Sauchelli, S.; Pickles, T.; Voinescu, A.; Choi, H.; Sherlock, B.; Zhang, J.; Colyer, S.; Grant, S.; Sundari, S.; Lasseter, G. Public attitudes towards the use of novel technologies in their future healthcare: A UK survey. BMC Med. Inform. Decis. Mak. 2023, 23, 38. [Google Scholar] [CrossRef]
- Mejtoft, T.; Lindahl, O.; Öhberg, F.; Pommer, L.; Jonzén, K.; Andersson, B.M.; Eklund, A.; Wåhlin, A.; Hallberg, P. Medtech innovation guide: An empiric model to support medical technology innovation. Health Technol. 2022, 12, 911–922. [Google Scholar] [CrossRef]
- Lottes, A.E.; Cavanaugh, K.J.; Chan, Y.Y.; Devlin, V.J.; Goergen, C.J.; Jean, R.; Linnes, J.C.; Malone, M.; Peat, R.; Reuter, D.G.; et al. Navigating the Regulatory Pathway for Medical Devices—A Conversation with the FDA, Clinicians, Researchers, and Industry Experts. J. Cardiovasc. Transl. Res. 2022, 15, 927–943. [Google Scholar] [CrossRef]
- Touijer, K. Marketing Versus Science: A Fight Between Necessary Evil and Stern Good Over the Adoption of New Technology in Medicine. Eur. Urol. 2010, 58, 522–524. [Google Scholar] [CrossRef] [PubMed]
- Bolenz, C.; Gupta, A.; Hotze, T.; Ho, R.; Cadeddu, J.A.; Roehrborn, C.G.; Lotan, Y. Cost comparison of robotic, laparoscopic, and open radical prostatectomy for prostate cancer. Eur. Urol. 2010, 57, 453–458. [Google Scholar] [CrossRef] [PubMed]
- Yaxley, J.W.; Coughlin, G.D.; Chambers, S.K.; Occhipinti, S.; Samaratunga, H.; Zajdlewicz, L.; Dunglison, N.; Carter, R.; Williams, S.; Payton, D.J.; et al. Robot-assisted laparoscopic prostatectomy versus open radical retropubic prostatectomy: Early outcomes from a randomised controlled phase 3 study. Lancet 2016, 388, 1057–1066. [Google Scholar] [CrossRef]
- Coughlin, G.D.; Yaxley, J.W.; Chambers, S.K.; Occhipinti, S.; Samaratunga, H.; Zajdlewicz, L.; Teloken, P.; Dunglison, N.; Williams, S.; Lavin, M.F.; et al. Robot-assisted laparoscopic prostatectomy versus open radical retropubic prostatectomy: 24-month outcomes from a randomised controlled study. Lancet Oncol. 2018, 19, 1051–1060. [Google Scholar] [CrossRef]
- Xu, M.-Y.; Zeng, N.; Ma, S.; Hua, Z.-J.; Zhang, S.-H.; Xiang, J.-C.; Xiong, Y.-F.; Xia, Z.-Y.; Sun, J.-X.; Liu, C.-Q.; et al. A clinical evaluation of robotic-assisted radical prostatectomy (RARP) in located prostate cancer: A systematic review and network meta-analysis. Crit. Rev. Oncol. Hematol. 2024, 204, 104514. [Google Scholar] [CrossRef]
- Ballantyne, G.H. Robotic surgery, telerobotic surgery, telepresence, and telementoring. Surg. Endosc. Other Interv. Tech. 2002, 16, 1389–1402. [Google Scholar] [CrossRef] [PubMed]
- Kumar, P.; Rammohan, R.; Chavan, M.; Ghyar, R.; Deshpande, S.; Kulkarni, J.N.; Bhansali, H.; Ravi, B. Surgeon perception of factors affecting the efficiency of conventional and robotic laparoscopy: A Pan India study. Heliyon 2022, 8, e12561. [Google Scholar] [CrossRef]
- Almujalhem, A.; Rha, K.H. Surgical robotic systems: What we have now? A urological perspective. BJUI Compass 2020, 1, 152–159. [Google Scholar] [CrossRef]
- Medical Technology Association of Australia. Strengthening Australia’s Health System. 2024. Available online: https://www.mtaa.org.au/sites/default/files/uploaded-content/field_f_content_file/mtaa_pre-budget_submission_2024_v6_clean_final_for_submission_2.pdf (accessed on 9 April 2025).
- Australian Government. Budget 2025-26: Building Australia’s Future; Commonwealth of Australia: Canberra, ACT, Australia, 2025.
- Department of Health, Disability and Ageing AG. About the National Critical Research Infrastructure Initiative. 2025. Available online: https://www.health.gov.au/our-work/mrff-national-critical-research-infrastructure-initiative?language=en#about-the-national-critical-research-infrastructure-initiative (accessed on 9 April 2025).
- Department of Industry, Science and Resources AG. Medical Science Co-Investment Plan. 2024. Available online: https://www.industry.gov.au/publications/medical-science-co-investment-plan#introduction-2 (accessed on 9 April 2025).
- Medical Technology Association of Australia. Annual Report FY23/24; Medical Technology Association of Australia: Sydney, Australia, 2024; p. 72. [Google Scholar]
- Little, M. The fivefold root of an ethics of surgery. Bioethics 2002, 16, 183–201. [Google Scholar] [CrossRef]
- Cardenas, D. Surgical ethics: A framework for surgeons, patients, and society. Rev. Col. Bras. Cir. 2020, 47, e20202519. [Google Scholar] [CrossRef]
- Citron, P. Ethics Considerations for Medical Device R&D. Prog. Cardiovasc. Dis. 2012, 55, 307–315. [Google Scholar] [PubMed]
- Wilkinson, A. Medical Device Regulation and Litigation: A Comparative Analysis of Australia, the United Kingdom and the United States of America. Ph.D. Thesis, Queensland University of Technology, Brisbane City, Australia, 2021. [Google Scholar]
- UK Government. Consumer Protection Act 1987; Department for Digital, Culture, Media, and Sport: London, UK, 1987.
- UK Government. The Medical Devices Regulations 2002; Department for Digital, Culture, Media, and Sport: London, UK, 2002.
- UK Government. The General Product Safety Regulations 2005; Department for Digital, Culture, Media, and Sport: London, UK, 2005.
- European Union. Council Directive 93/42/EEC of 14 June 1993 Concerning Medical Devices; European Union: Brussels, Belgium, 1993. [Google Scholar]
- Federal Food. Drug, and Cosmetic Act. Cal. West. Med. 1938, 49, 172–174. [Google Scholar]
- UK Government. Medicines and Healthcare Products Regulatory Agency. 2025. Available online: https://www.gov.uk/government/organisations/medicines-and-healthcare-products-regulatory-agency/about (accessed on 9 April 2025).
- US Food and Drug Administration. About FDA. 2025. Available online: https://www.fda.gov/about-fda (accessed on 9 April 2025).
- Therapeutic Goods Administration Department of Health, Disability and Ageing AG. Understanding Priority Applicant Determination Rules for Medical Devices Including In-Vitro Diagnostics (IVDs). 2018. Available online: https://www.tga.gov.au/resources/guidance/understanding-priority-applicant-determination-rules-medical-devices-including-vitro-diagnostics-ivds#the-two-types-of-priority-applicant-determinations (accessed on 9 April 2025).
- Kruachottikul, P.; Tea-makorn, P.; Dumrongvute, P.; Hemrungrojn, S.; Nupairoj, N.; Junchaya, O.; Vinayavekhin, S. MediGate: A MedTech product innovation development process from university research to successful commercialization within emerging markets. J. Innov. Entrep. 2024, 13, 71. [Google Scholar] [CrossRef]
- Van Norman, G.A. Drugs, Devices, and the FDA: Part 2: An Overview of Approval Processes: FDA Approval of Medical Devices. JACC Basic. Transl. Sci. 2016, 1, 277–287. [Google Scholar] [CrossRef]
- Kaplan, A.V.; Baim, D.S.; Smith, J.J.; Feigal, D.A.; Simons, M.; Jefferys, D.; Fogarty, T.J.; Kuntz, R.E.; Leon, M.B. Medical Device Development: From Prototype to Regulatory Approval. Circulation 2004, 109, 3068–3072. [Google Scholar] [CrossRef]
- Müllner, P.S.; Klinger, U. Medical Device Development. In Medical Devices and In Vitro Diagnostics: Requirements in Europe; Baumgartner, C., Harer, J., Schröttner, J., Eds.; Springer International Publishing: Cham, Switzerland, 2022; pp. 1–36. [Google Scholar]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Published by MDPI on behalf of the Société Internationale d’Urologie. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).