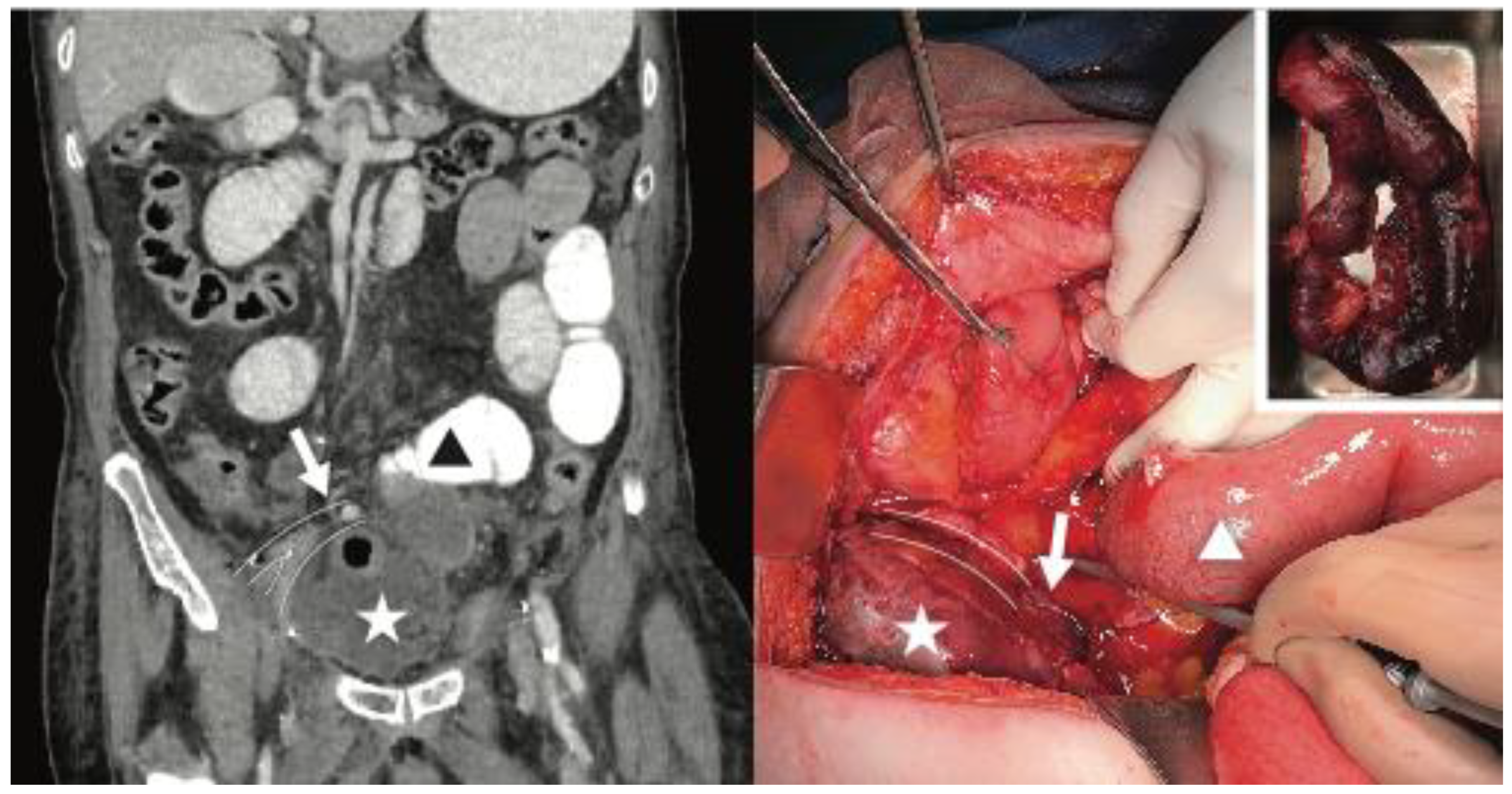
Incarcerated Internal Hernia Posterior to the Iliac Vessels After Uncomplicated Radical Cystectomy


{kind=link}
Conflicts of Interest
Patient Consent
References
- Gakis, G.; Efstathiou, J.; Lerner, S.P.; Cookson, M.S.; Keegan, K.A.; Guru, K.A.; Shipley, W.U.; Heidenreich, A.; Sagaloswky, A.I.; Soloway, M.S.; et al. ICUD-EAU International Consultation on Bladder Cancer 2012: Radical Cystectomy and Bladder Preservation for Muscle-Invasive Urothelial Carcinoma of the Bladder. Eur. Urol. 2013, 63, 45–57. [Google Scholar] [CrossRef] [PubMed]
- Hautmann, R.E.; De Petriconi, R.C.; Volkmer, B.G. Lessons learned from 1000 neobladders: The 90-day complication rate. J. Urol. 2010, 184, 990–994. [Google Scholar] [CrossRef] [PubMed]
This is an open access article under the terms of a license that permits non-commercial use, provided the original work is properly cited. © 2023 The Authors. Société Internationale d'Urologie Journal, published by the Société Internationale d'Urologie, Canada.
Share and Cite
Sparanese, S.; Chehroudi, C.; Black, P.C. Incarcerated Internal Hernia Posterior to the Iliac Vessels After Uncomplicated Radical Cystectomy. Soc. Int. Urol. J. 2023, 4, 71-72. https://doi.org/10.48083/ZJNE2733
Sparanese S, Chehroudi C, Black PC. Incarcerated Internal Hernia Posterior to the Iliac Vessels After Uncomplicated Radical Cystectomy. Société Internationale d’Urologie Journal. 2023; 4(1):71-72. https://doi.org/10.48083/ZJNE2733
Chicago/Turabian StyleSparanese, Sydney, Cyrus Chehroudi, and Peter C. Black. 2023. "Incarcerated Internal Hernia Posterior to the Iliac Vessels After Uncomplicated Radical Cystectomy" Société Internationale d’Urologie Journal 4, no. 1: 71-72. https://doi.org/10.48083/ZJNE2733
APA StyleSparanese, S., Chehroudi, C., & Black, P. C. (2023). Incarcerated Internal Hernia Posterior to the Iliac Vessels After Uncomplicated Radical Cystectomy. Société Internationale d’Urologie Journal, 4(1), 71-72. https://doi.org/10.48083/ZJNE2733