Abstract
Objective: To perform a systematic review assessing the impact of the different management options on health- related quality of life (HRQoL) of patients with localized renal masses or renal cell carcinomas (LRM/LRCC). Materials and Methods: Searches covering PubMed, Embase (Ovid), CENTRAL, PsycINFO (Ovid), CINAHL (EBSCO), and Cochrane Central Register of Controlled Trials (CENTRAL) databases was conducted for papers published up to 25 April 2021. Methods as per Cochrane Handbook were followed. “Modality” of treatment included radical nephrectomy (RN), nephron-sparing surgery (NSS), thermal ablation (TA), and active surveillance (AS). “Approach” was categorized as open incision and minimally invasive surgery (MIS). Risk of bias was assessed by ROBINS-I and Cochrane RoB 2 for observational studies and randomized controlled trials, respectively and certainty of the evidence by GRADE. Results: Sixteen observational studies and 1 randomized controlled trial (2.370 patients) met inclusion criteria. Fifteen different patient reported outcome measures (PROMs) were identified. Heterogeneity prevented quantitative analysis. Generic HRQoL decreases after RN and NSS, recovers within 6 to 12 months, and mostly overlaps with baseline values, irrespective of modality. Cancer-specific HRQoL improves faster after open-NSS than open-RN. The detrimental effect of RN may persist long-term in cross-evaluations. QoL scales significantly decrease after open surgery and MIS during the first weeks but improve faster after MIS. They are similar for both approaches at 1 year. Long-term cancer-specific QoL is similar for MIS and open procedures. Fear of recurrence is lower in older patients and affected by neither modality nor approach. Conclusions: Low quality evidence supports the use of MIS over the open approach when HRQoL is considered in the management of LRMs/LRCCs; data regarding the effect of the treatment modality of the LRM/LRCC show contradictory outcomes.
Introduction
Approximately 70% of renal cell carcinomas (RCC) are clinically diagnosed as localized renal masses (LRM) [1]. Of the latter, a non-negligible proportion— between 10% and 30%—will be ultimately confirmed as benign at histological examination [2,3,4]. The surgical management options include radical nephrectomy (RN) or nephron-sparing surgery (NSS), both of which can be performed by an open or minimally invasive approach (MIS). MIS includes laparoscopic and robotic (R) surgery as well as any modification of these approaches. Furthermore, patients with stage cT1a RCC can be offered active surveillance (AS) or interventional percutaneous thermal ablation (TA) [5].
A previous systematic review synthetising periopera- tive and quality of life (QoL) outcomes for the manage- ment of localized RCC (LRCC) showed inconclusive evidence about QoL while comparing partial nephrec- tomy (PN) with RN [6]. Although a significantly better short-term physical function was found for laparos- copy than for open approach, only 3 studies reported on generic or cancer-specific QoL measurements, stressing the need for future research [6].
Patient reported outcomes (PROM) are increas- ingly used in surgery as a practical tool for assessing outcomes [7,8]. Particularly when several management options with similar clinical efficacy coexist [2,8], the impact of a given treatment on patient QoL plays an important role in the clinical decision-making. Health- related QoL (HRQoL) is subjective, multidimensional, and influenced by the nature of the histological diag- nosis. Patients diagnosed with a cancer are likely more tolerant of a negative impact of treatment on QoL than patients found to have a benign condition. This is rele- vant in the management of localized renal masses because a proportion are benign [2,3,4].
Parallel to the increasing incidence of LRM [9], integration of patient’s perception and values in the process of care becomes imperative [7,8] and a number of comparative reports on QoL using PROMs have been published in the last 5 years. Data compilating the current knowledge in the subject seems indicated.
The aim of this systematic review was to critically appraise and synthesise the comparative evidence on HRQoL measured by PROM among the differ- ent management approaches in patients with LRMs or LRCCs.
Materials and Methods
Data Sources and Searches
A search for relevant literature published in English was conducted up to 4 April 2019 and updated on 25 April 2021. The following databases were searched: PubMed, Embase (Ovid), CENTRAL, PsycINFO (Ovid), CINAHL (EBSCO) and CENTRAL. The search strategy is included in Supplementary Appendix 1 (available at siuj.org). We followed the PRISMA guidance and the Cochrane Handbook [10,11]. The protocol was registered with PROSPERO (CRD 42019107456).
Study Selection, Data Extraction and Analysis
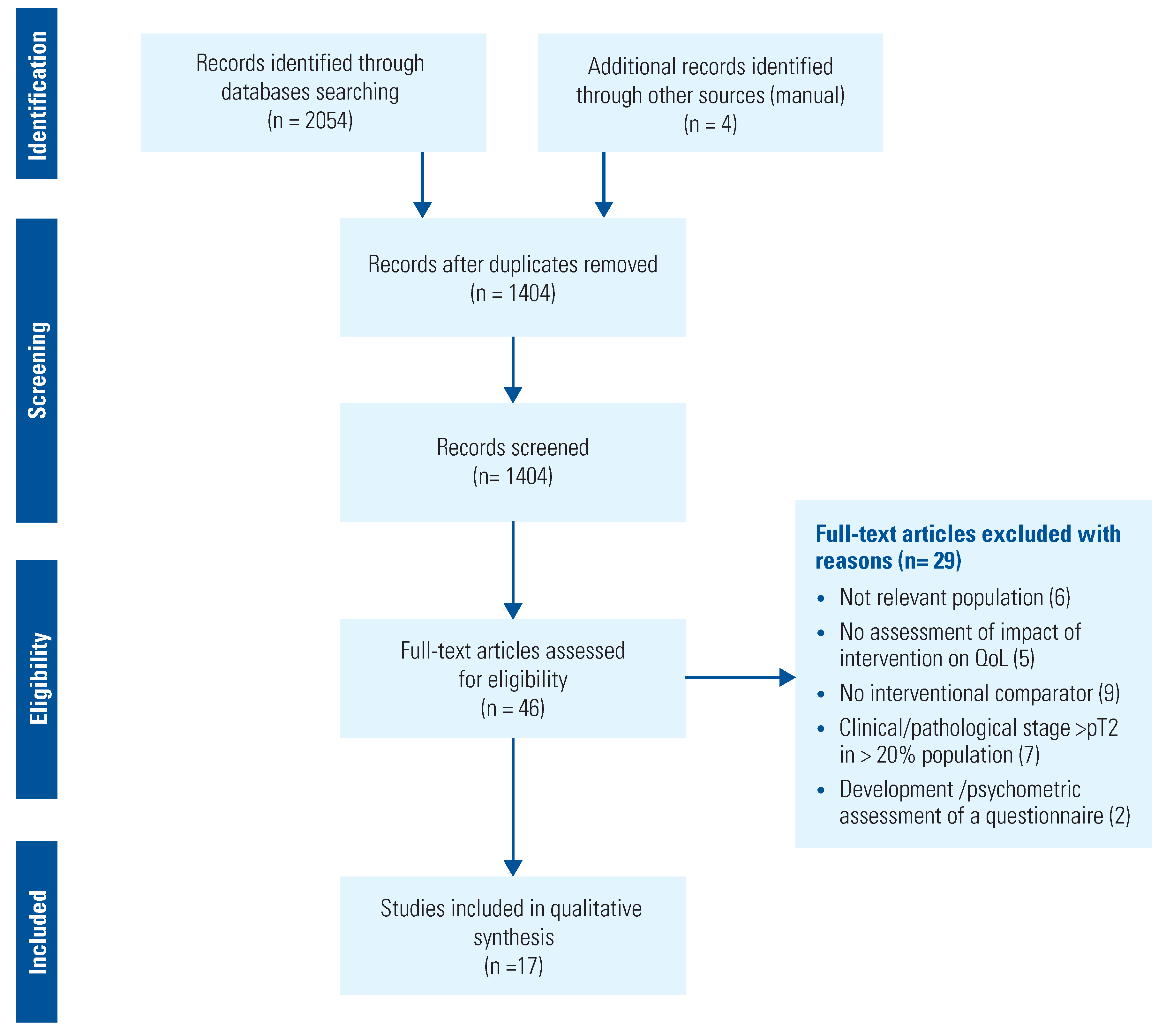
Study selection was based on predefined criteria according to the PICO (population, intervention, comparison, outcomes) constructed for this systematic review (Table 1).

Table 1.
PICO search strategy for the systematic review.
We sought a response to 2 questions: (1) Is HRQoL after NSS better than after RN? (2) Is HRQoL better after MIS than after open approach? A comparison between surgical management, TA, or AS in small renal masses was planned.
Only studies using original or cross-validated PROMs comparing 2 or more management options for LRMs/ LRCCs were included. Studies that reported on surgical or interventional management for other kidney condi- tions were excluded.
Two reviewers (L.S. and L.O.) independently performed abstract and full-text screening and data extraction. Information collected included patient characteristics, PROM distribution and response, miss- ing data, time-points for evaluation, outcomes and confounders analysis, and interpretation of results. Two senior authors acted as arbitrator (M.P.L. or M.I.O.) in case of disagreement.
“Modality” of treatment included RN, NSS (PN, tumorectomy), TA, and AS. “Approach” was categorized as open incision (any), MIS (laparoscopic or robotic), and percutaneous. Management strategies included all possible combinations of modality of treatment and approach. Studies with response rate ≥70% were consid- ered as “data available for all or nearly all participants.”
Evidence synthesis was primarily categorized according to modality or approach. We identified a variety of instruments for measuring HRQoL across studies, and comparisons were based on the use of the same PROM. Study design (longitudinal or cross-sectional) was taken into account in the evidence synthesis.
Risk of Bias Assessment and Strength of Body of Evidence
Two reviewers independently assessed the risk of bias. ROBINS-I tool [12] was used for comparative observational studies, and the Cochrane RoB 2 [13] for RCTs. The quality of the evidence was assessed using GRADE [14]. Discrepancies were resolved by senior authors.
Results
From the 1404 identified citations, 16 observational comparative studies[15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30], and 1 RCT[31] met the inclusion criteria. The PRISMA diagram depicts the flow of the literature selection (Figure 1).
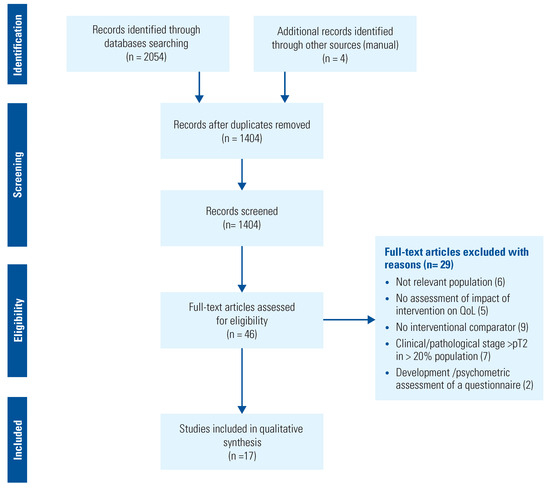
Figure 1.
Preferred reporting Items for systematic reviews and meta-analysis (PRISMA) flow diagram.
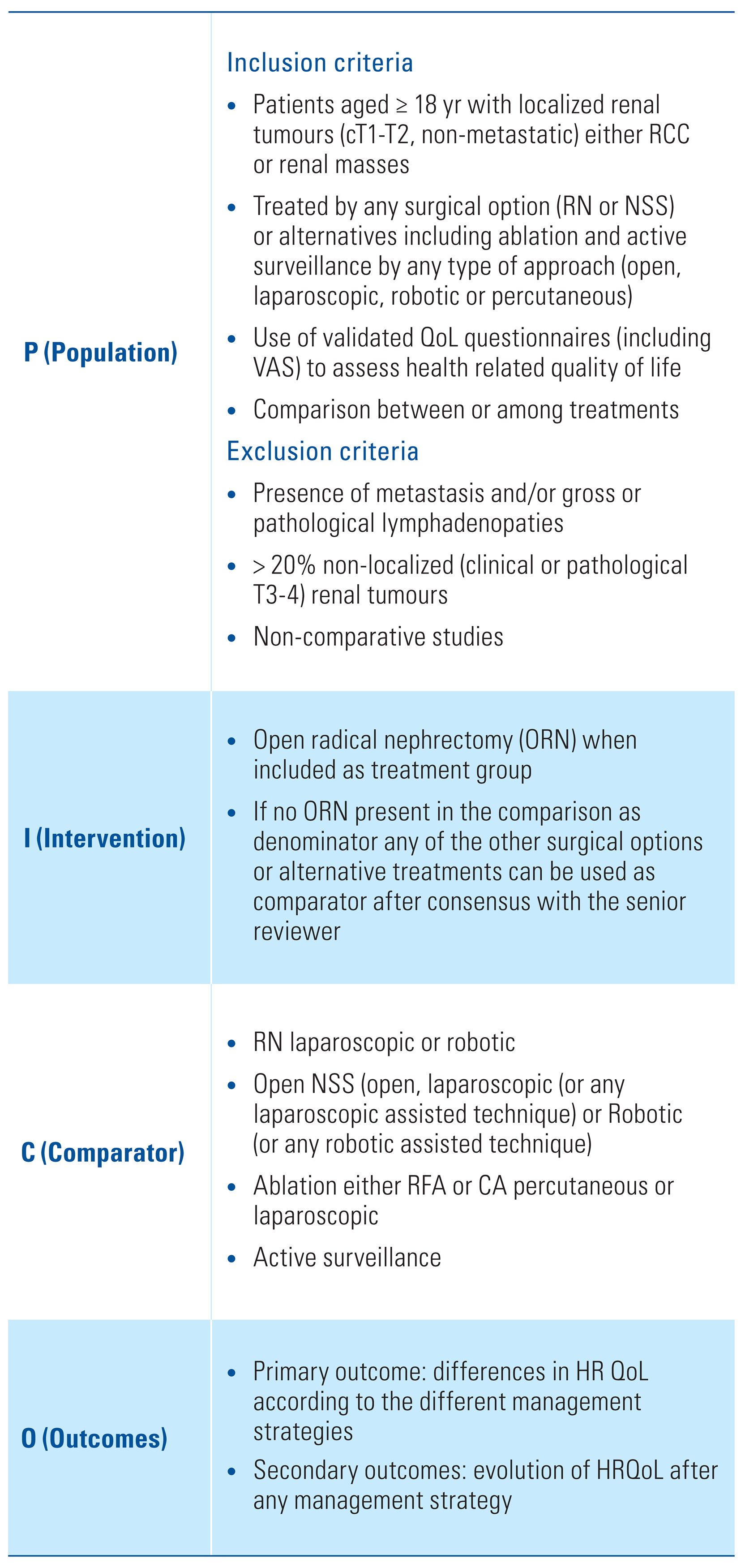
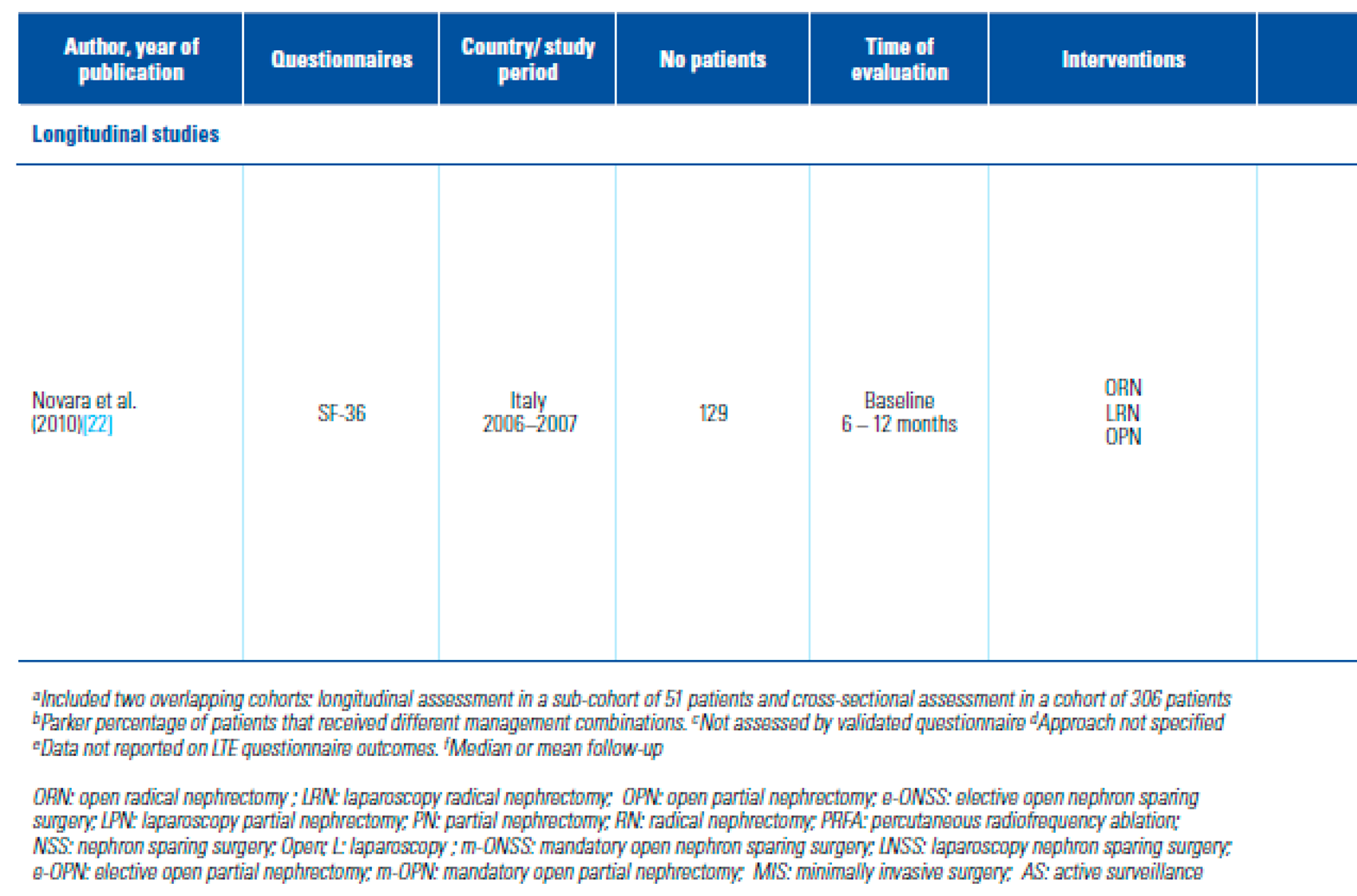
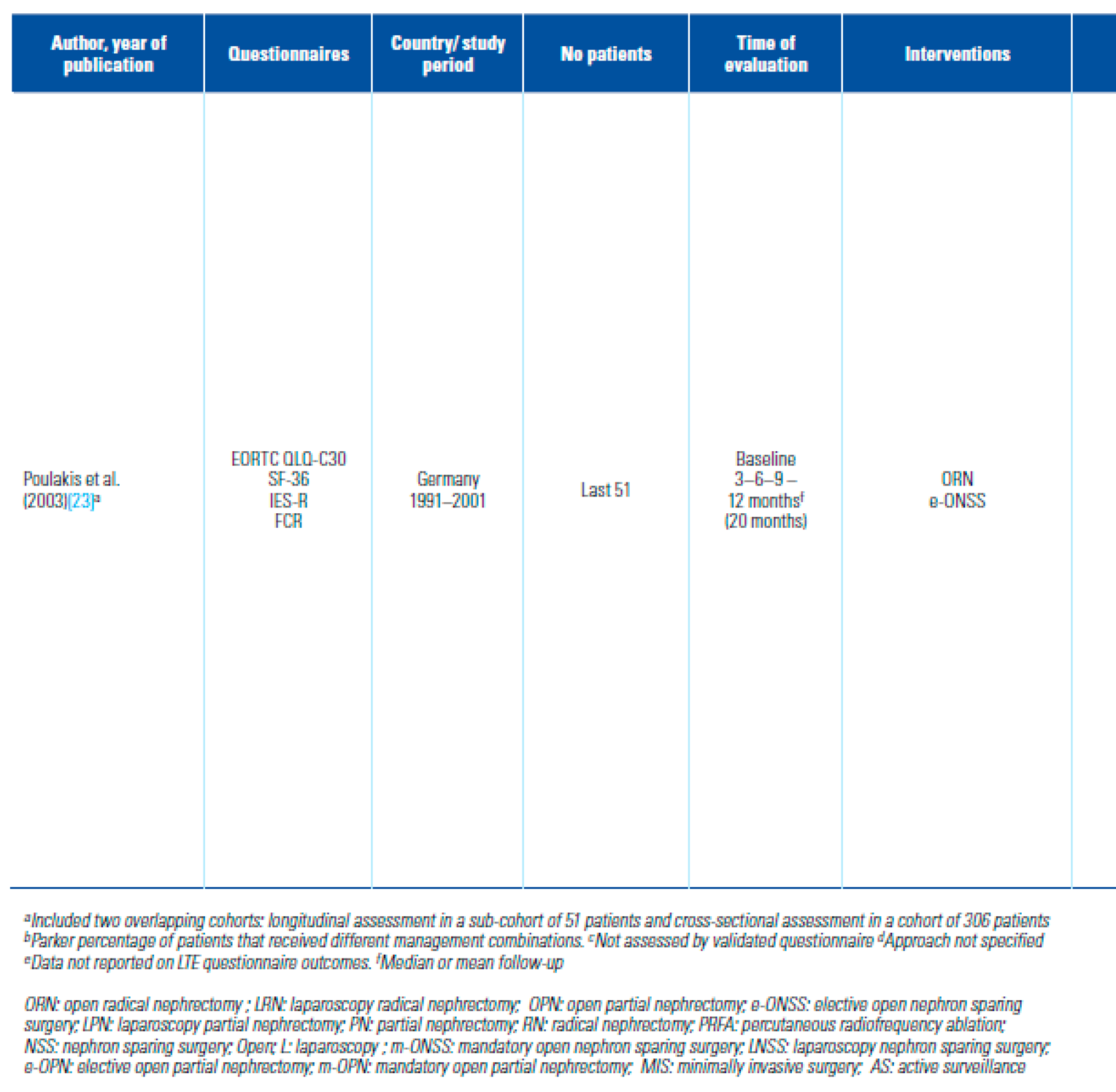
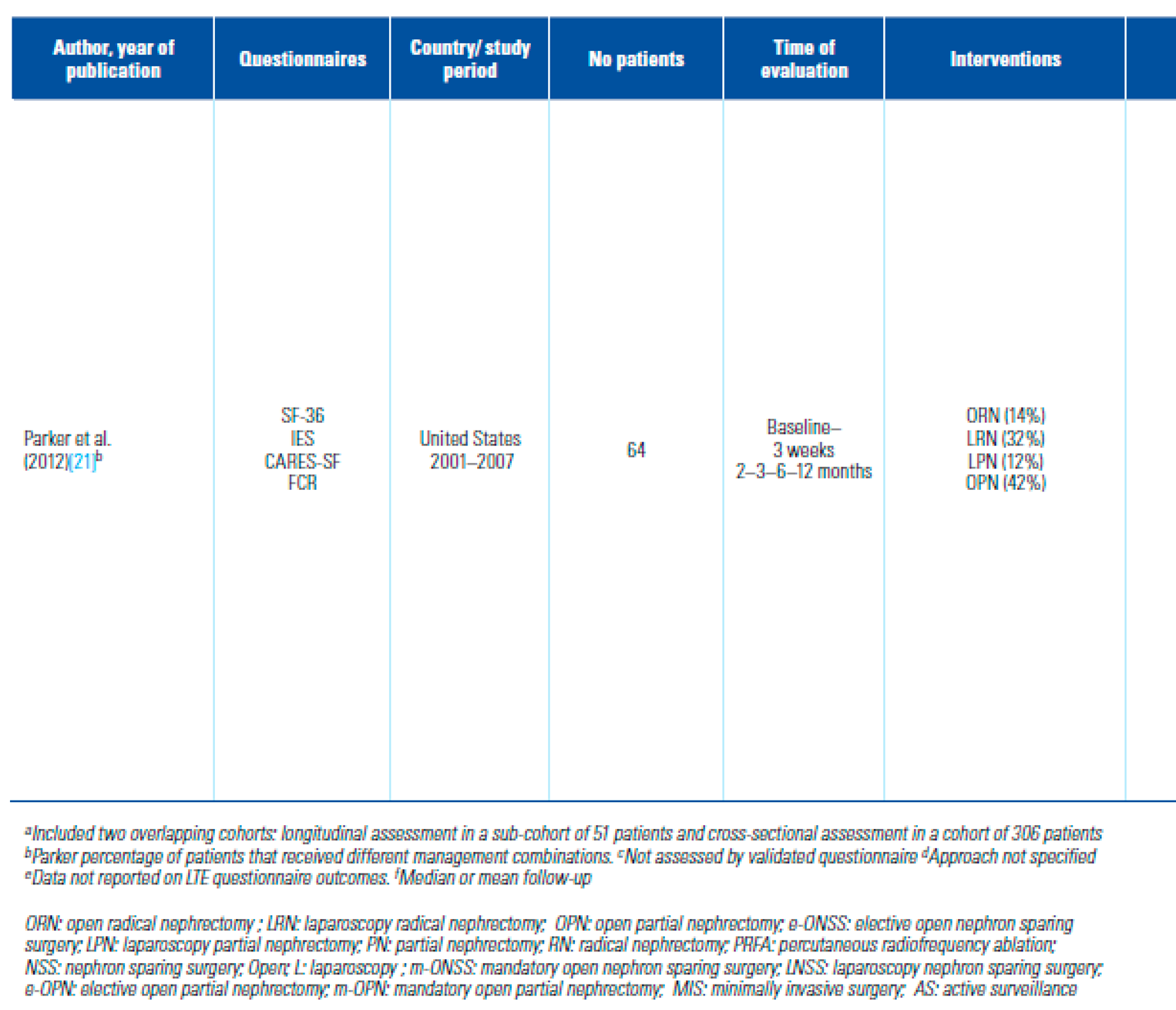
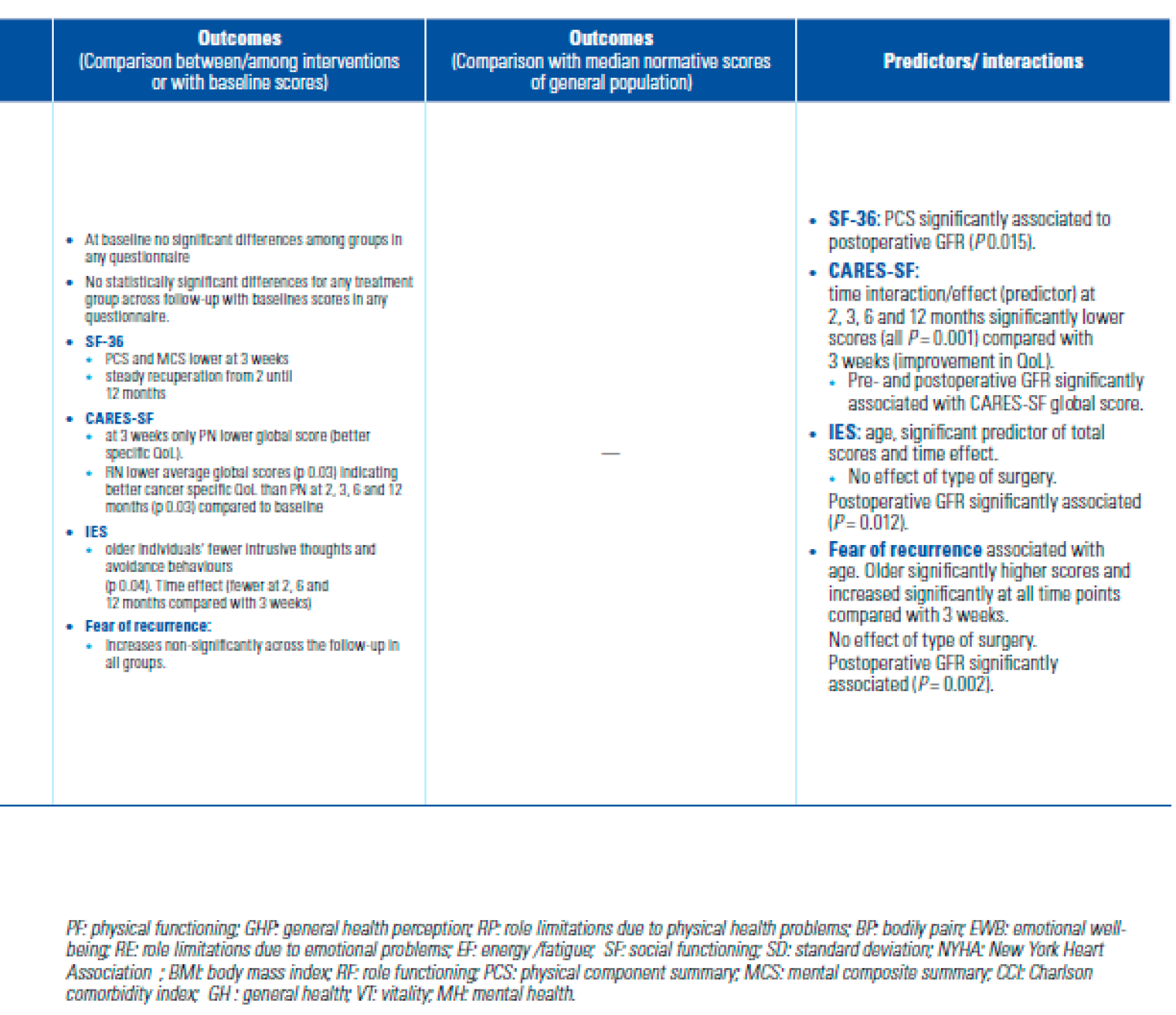
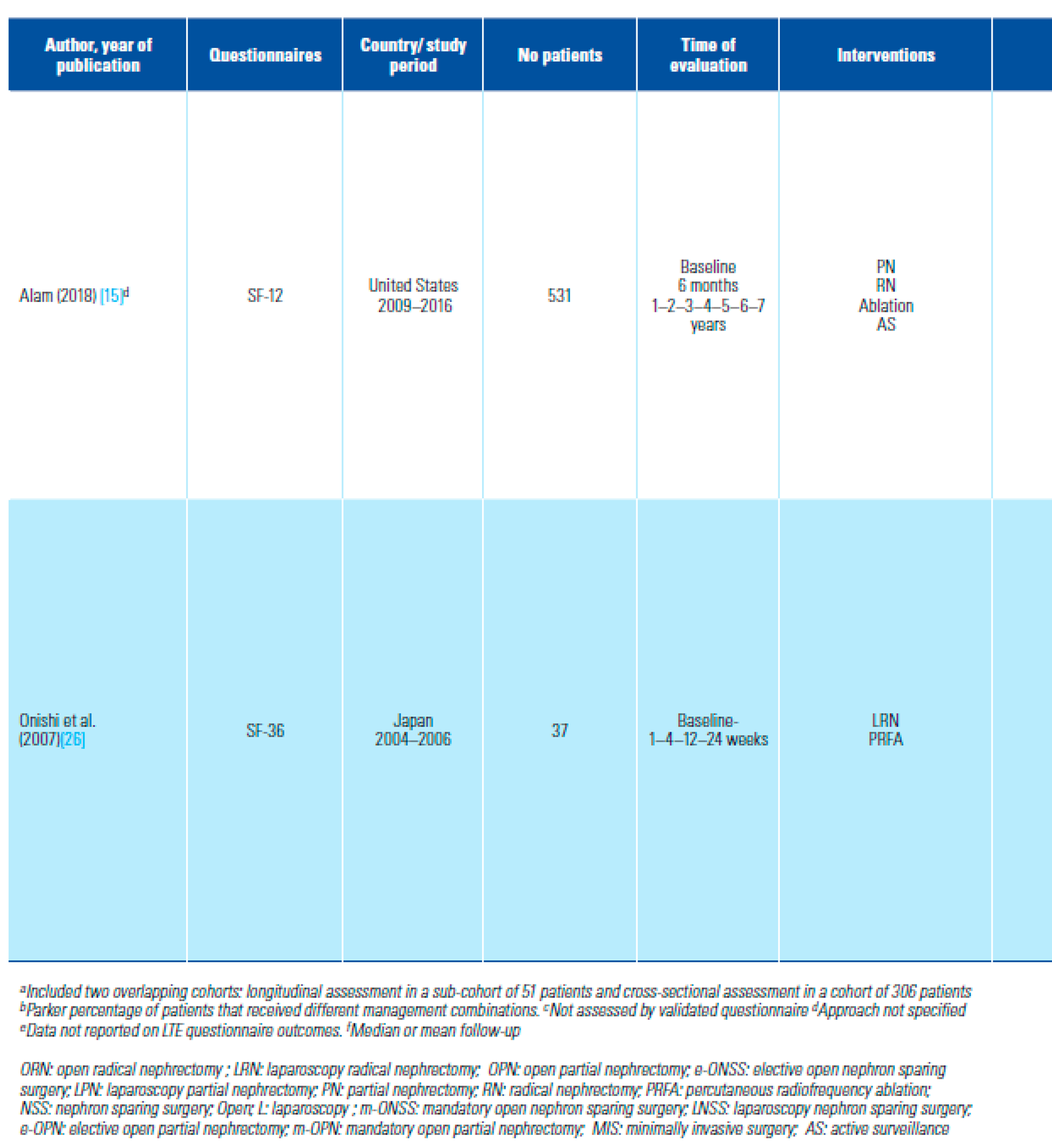
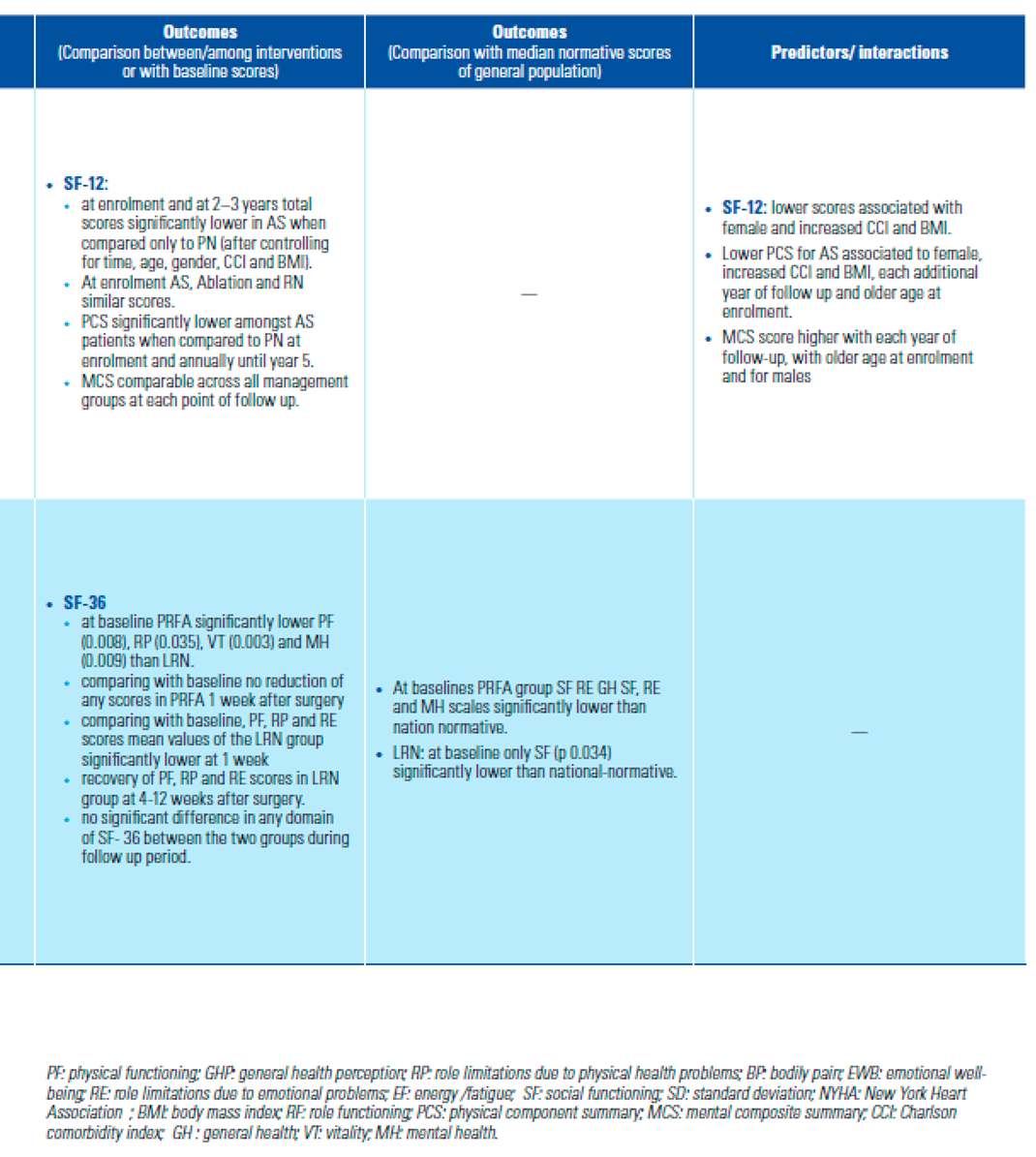
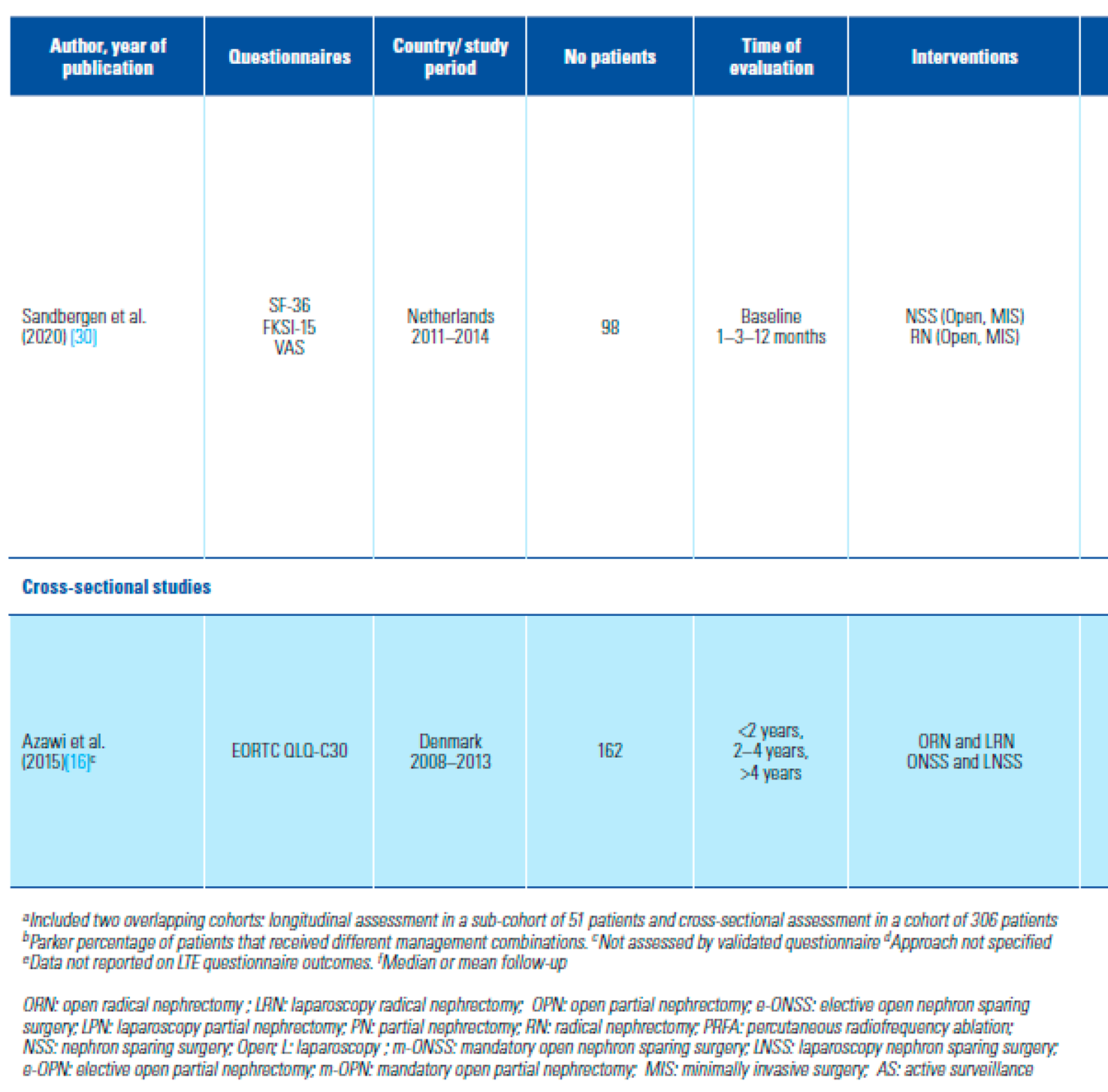
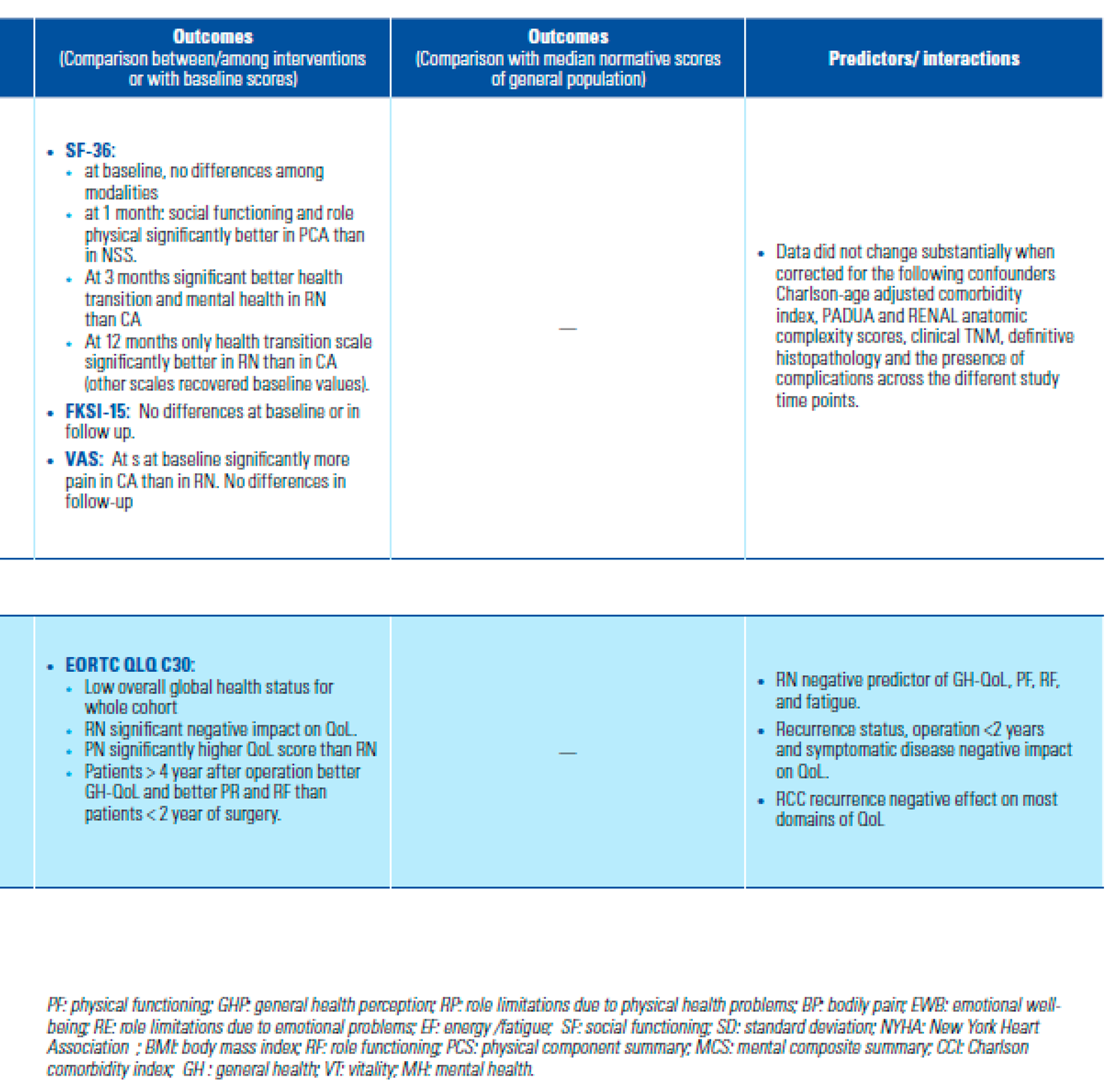
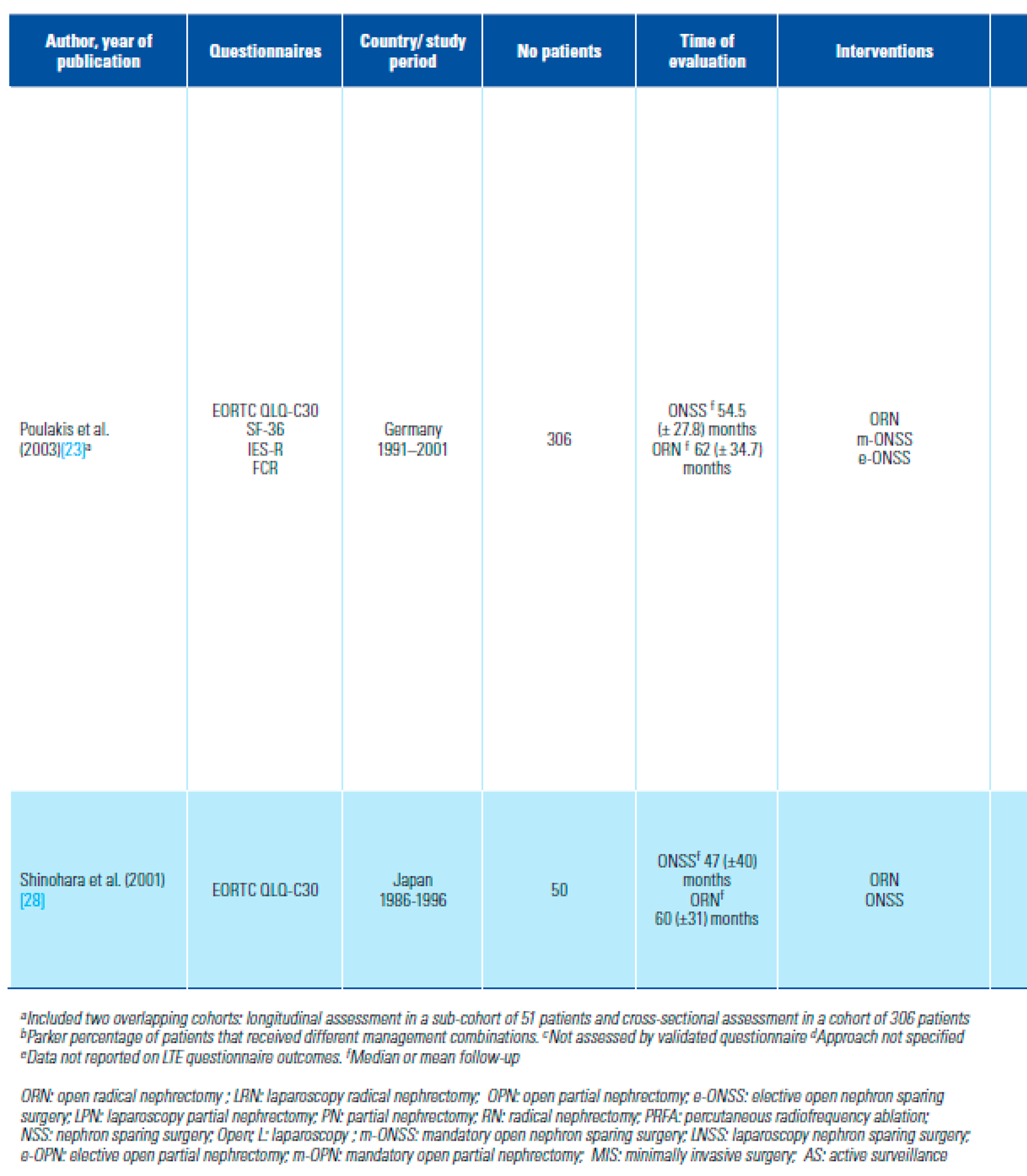
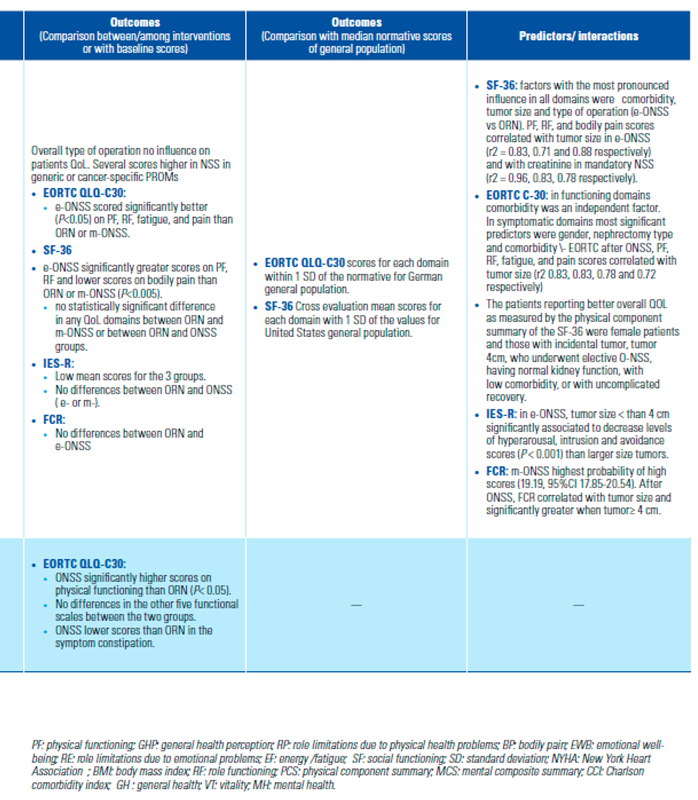
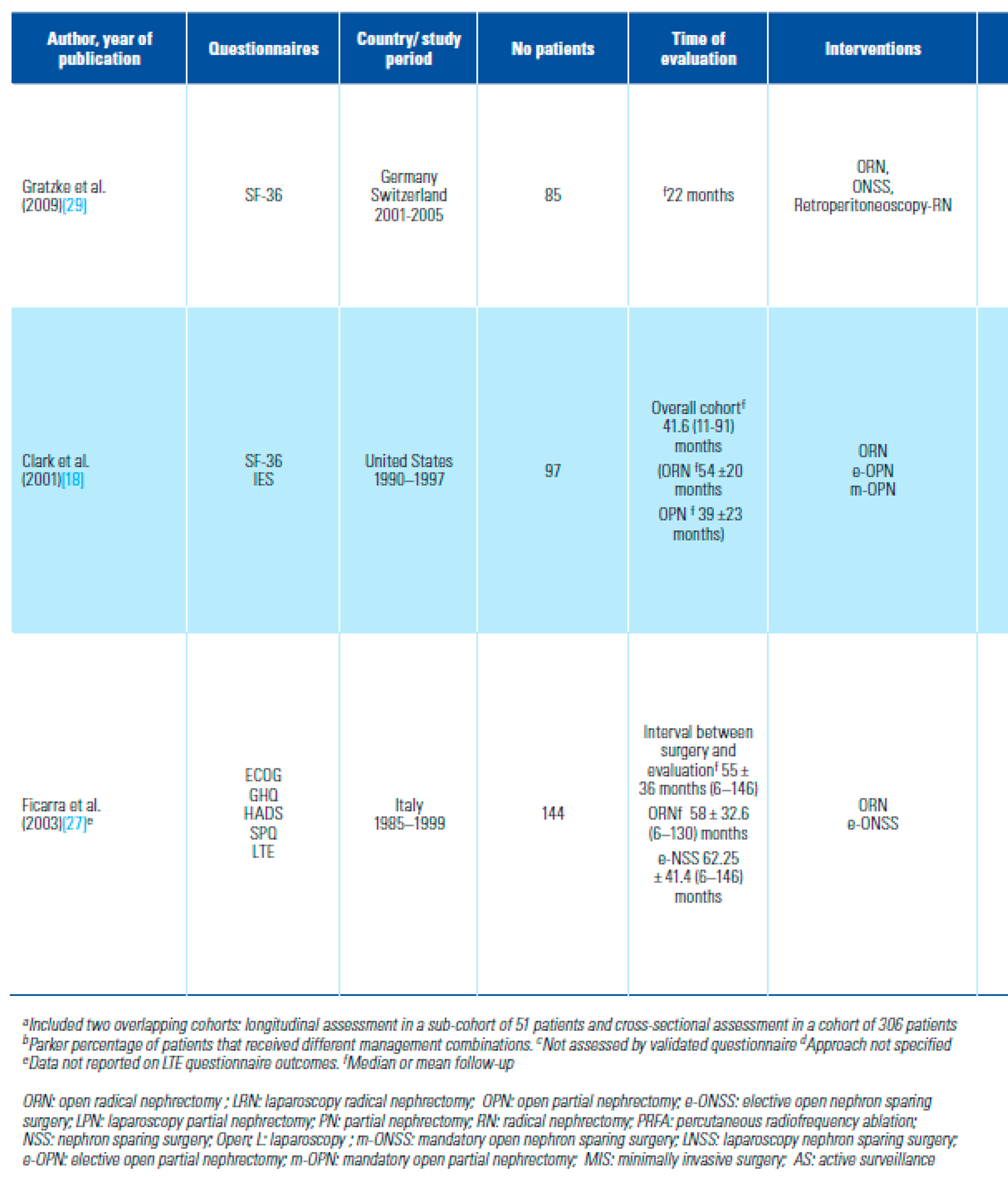
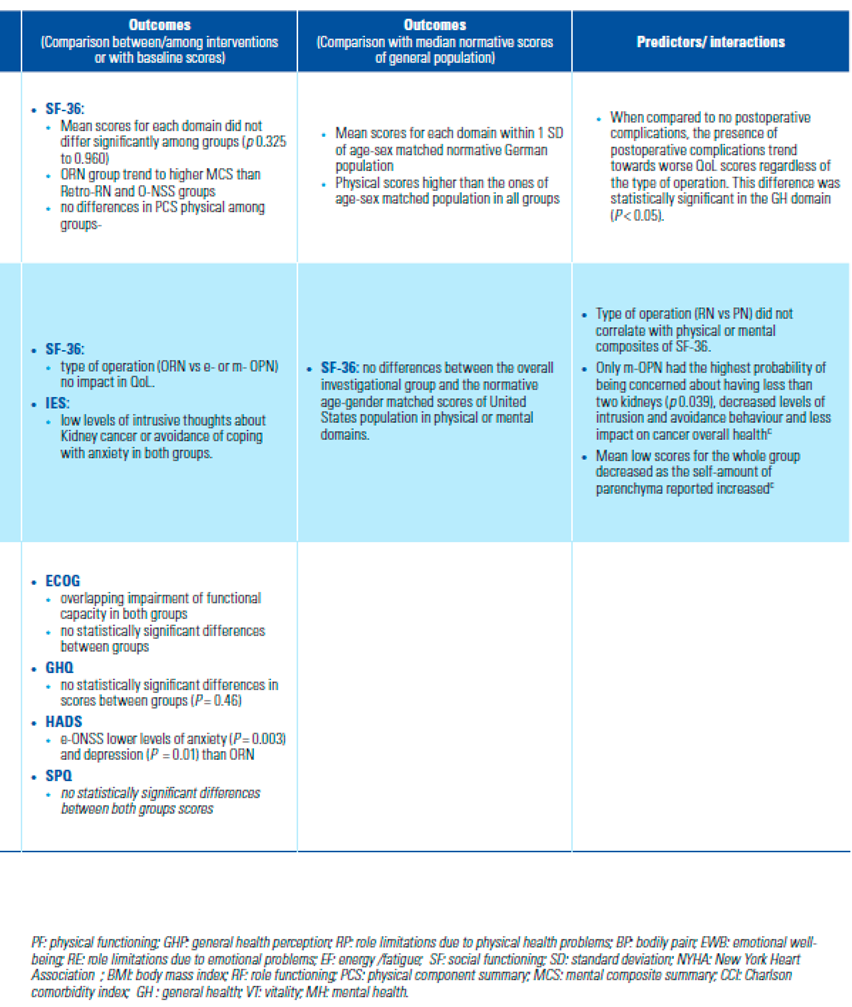
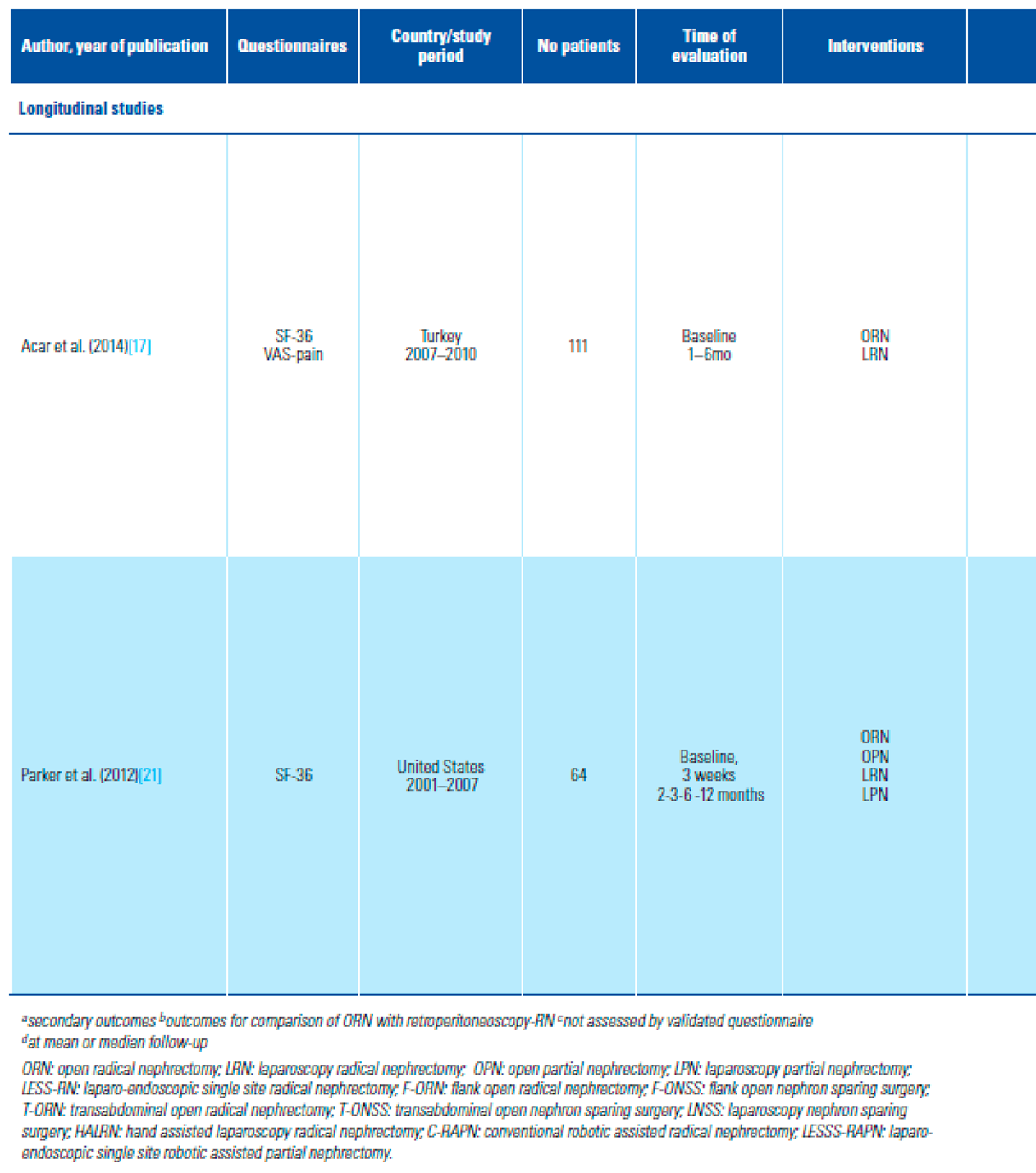
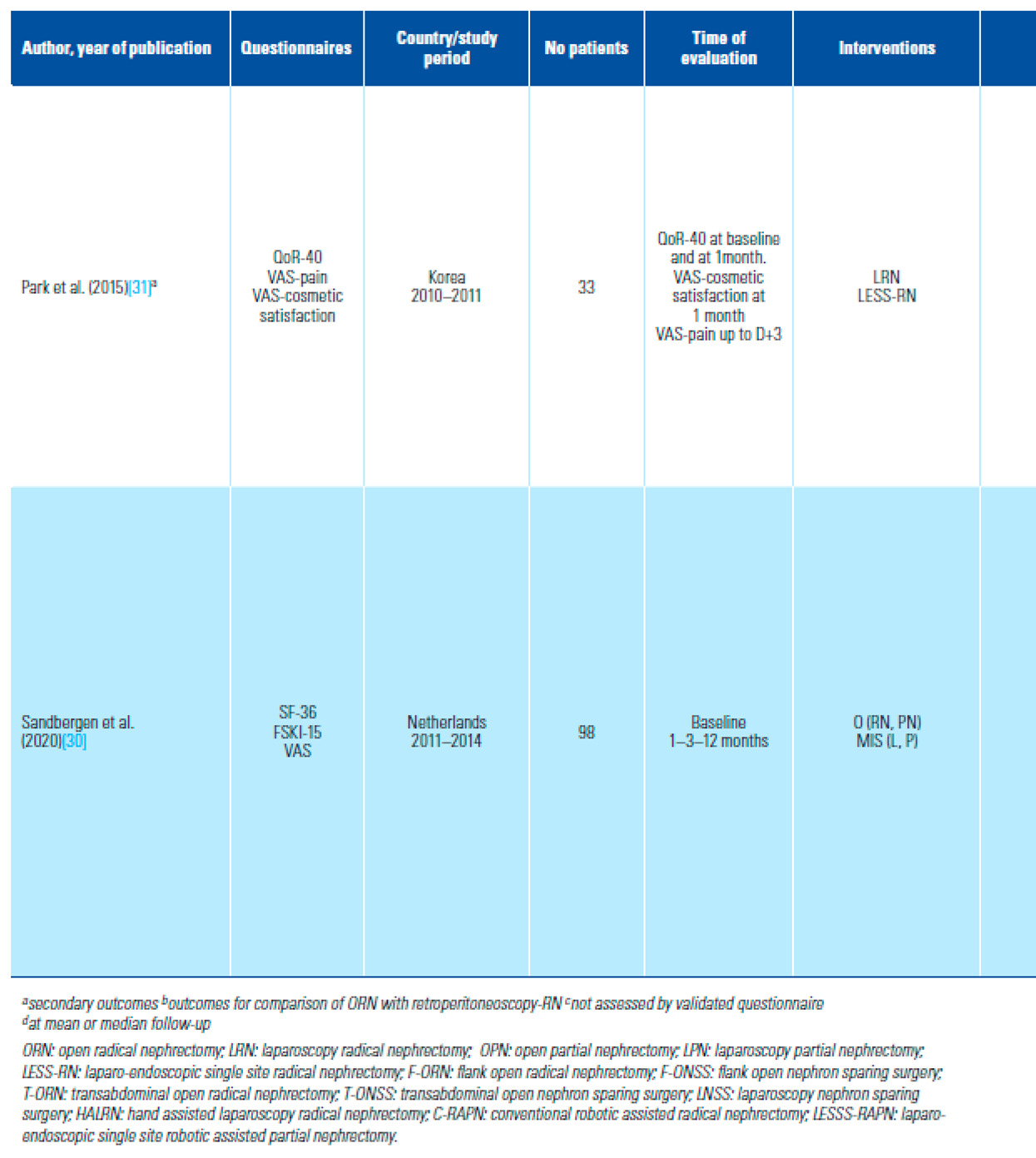
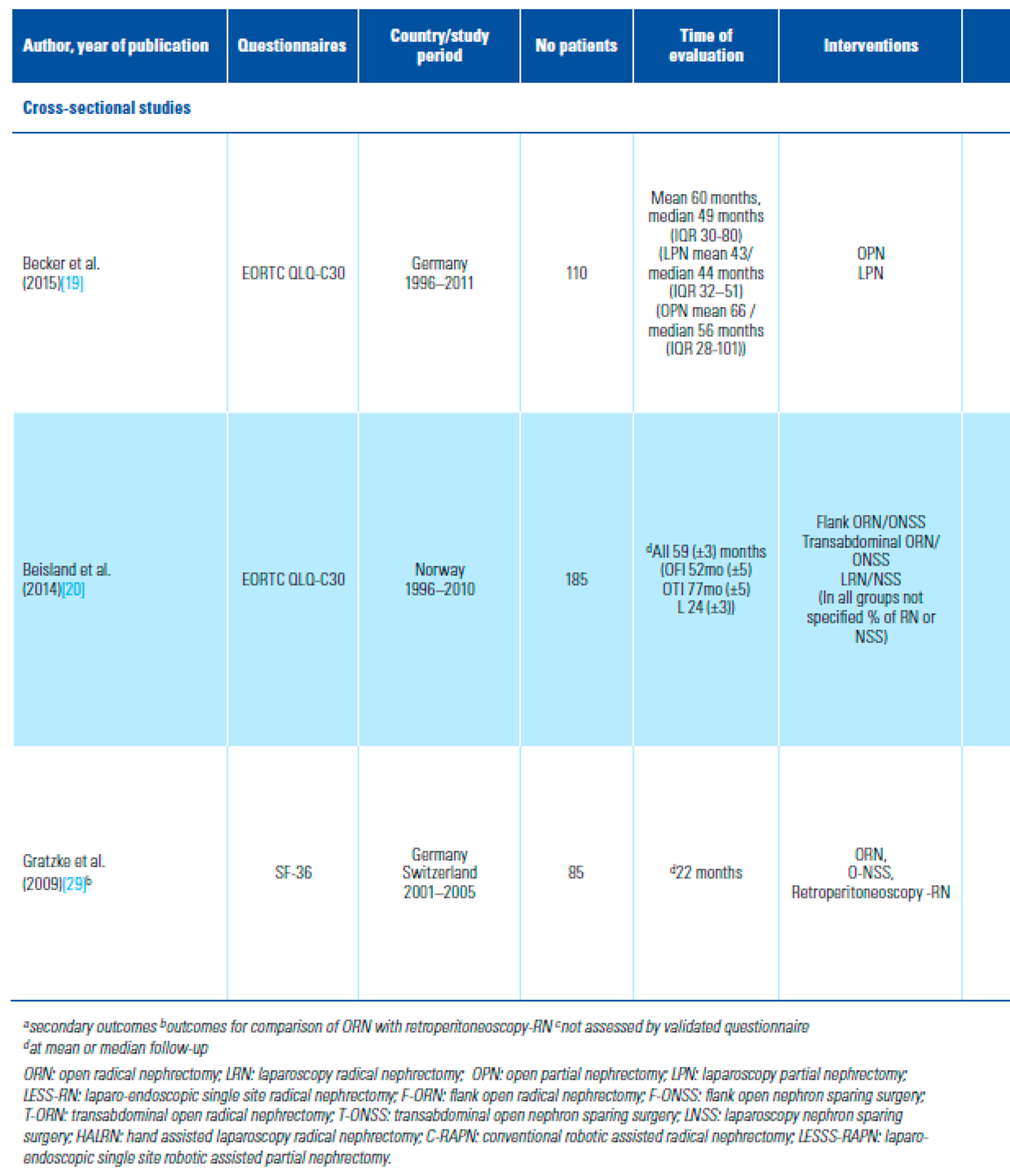
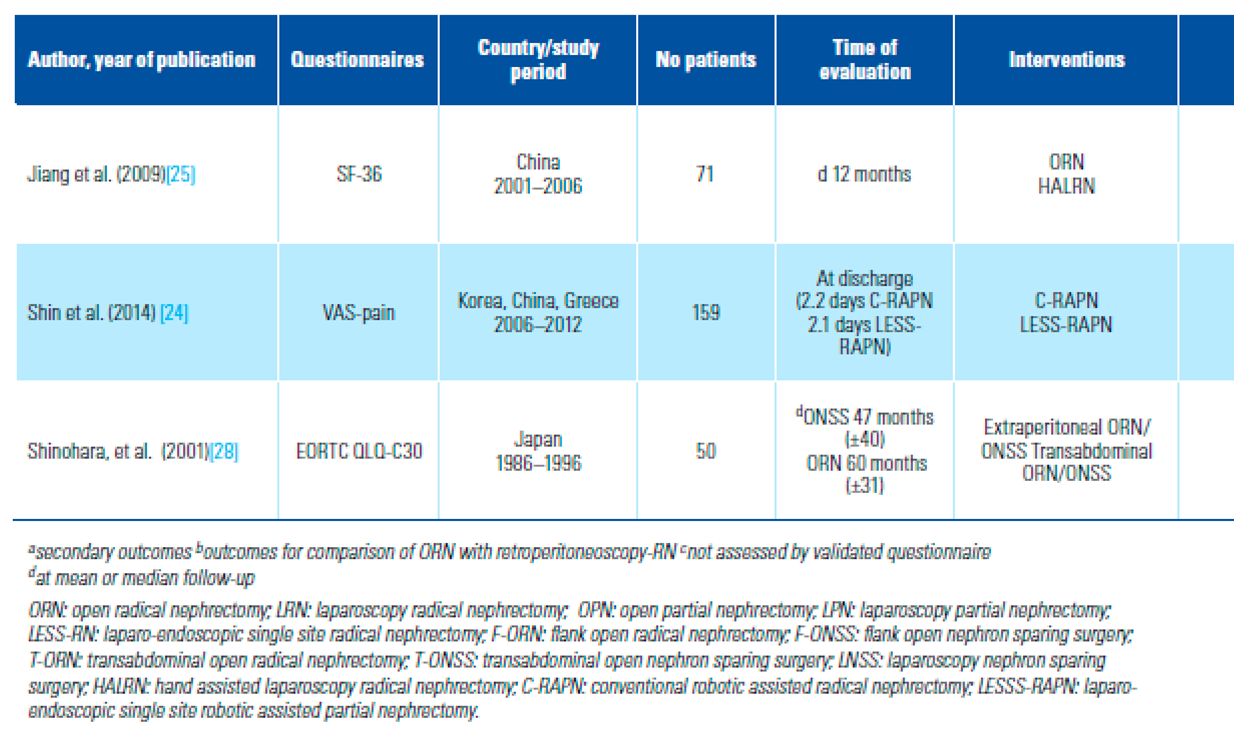
A total of 2370 patients were included. Characteristics of the studies and the patients, PROMs used, time-points of evaluation, outcomes, confounders, and variables of interest of the included studies are summarized in Table 2 and Table 3. Eleven studies included exclusively LRCCs [16,17,18,20,23,25,26,27,28,29,31] and 6 LRMs [15,19,21,22,24,30].
Table 2.
Comparative HRQoL outcomes between or among modalities of treatment.
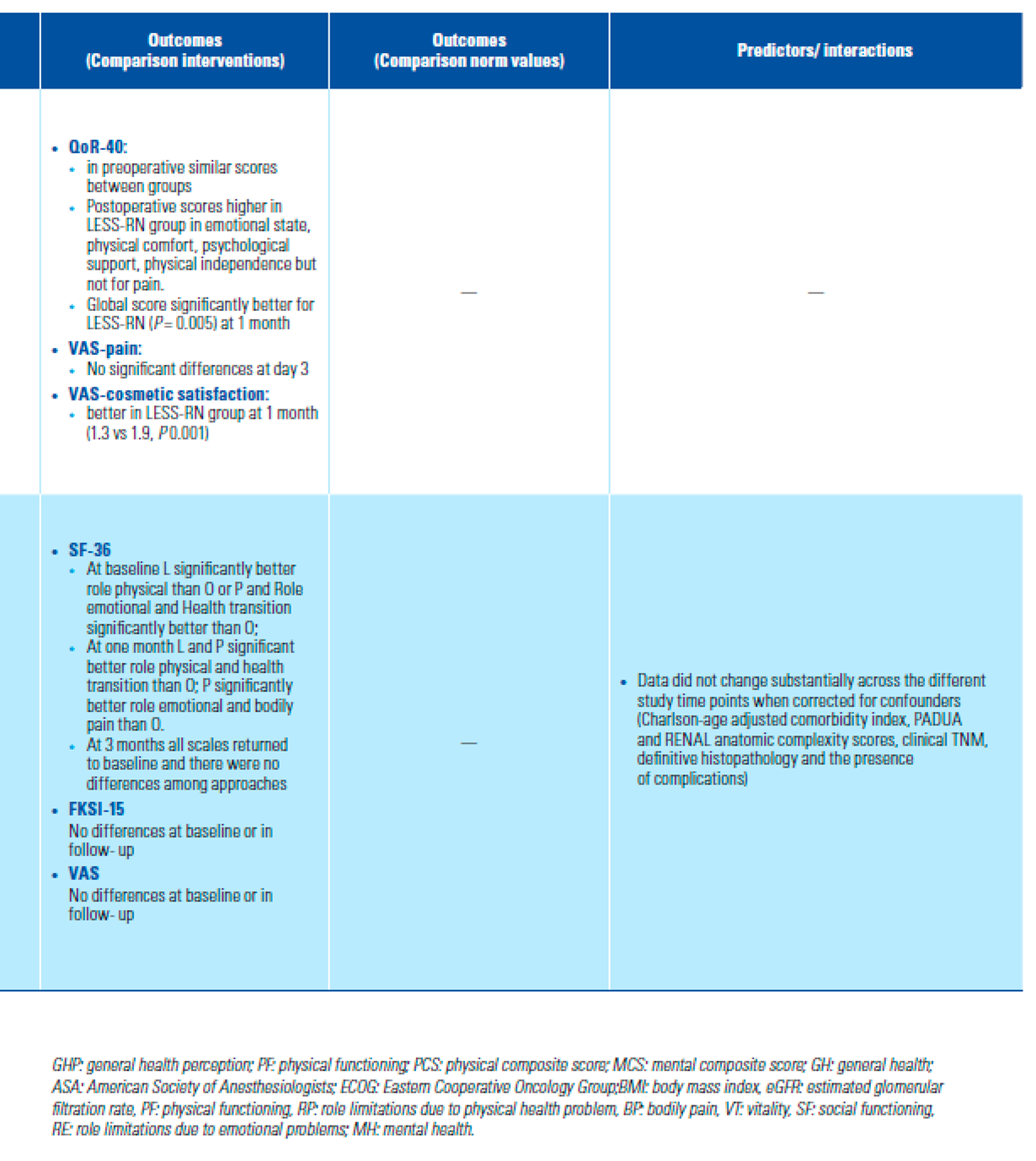
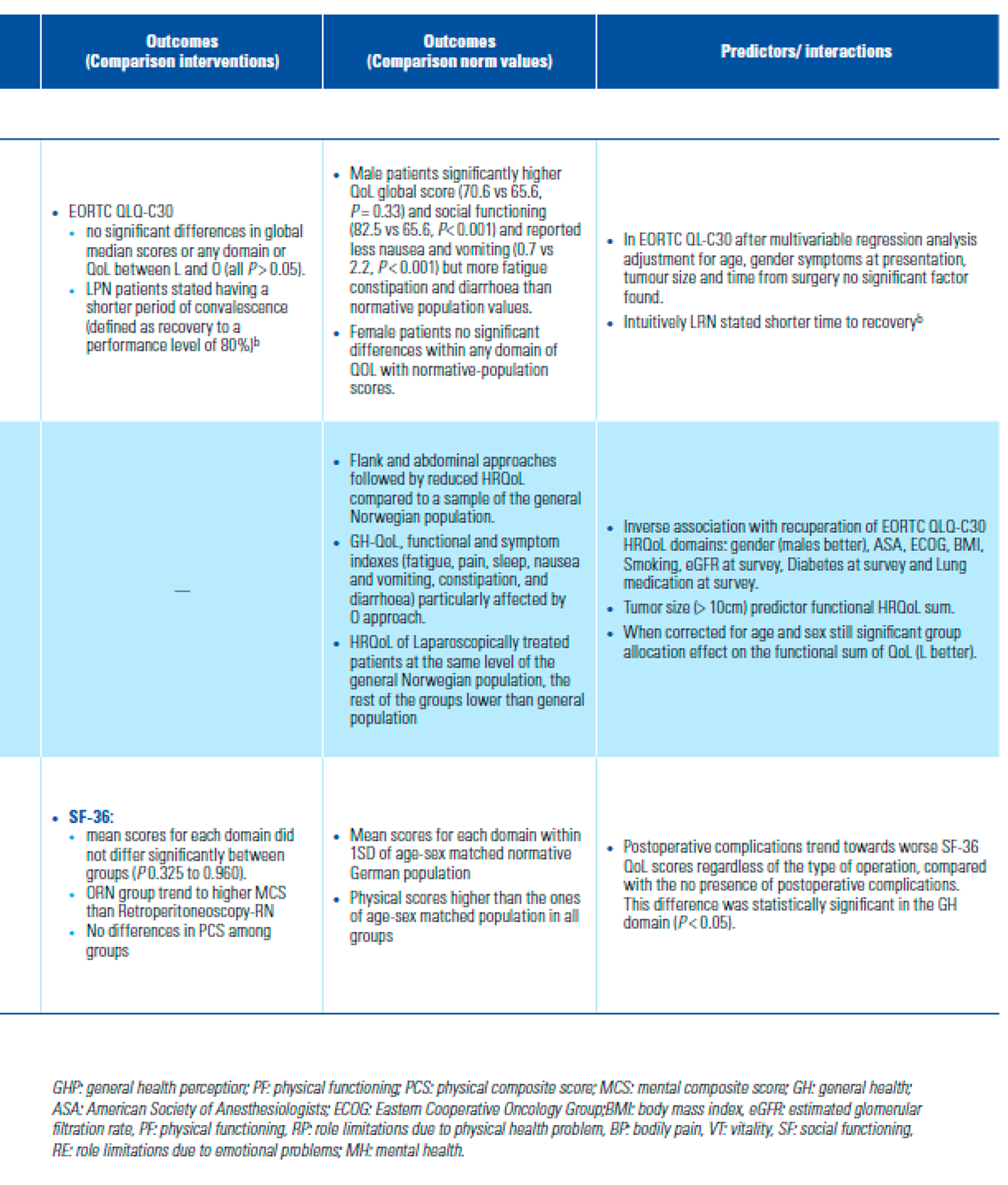
Table 3.
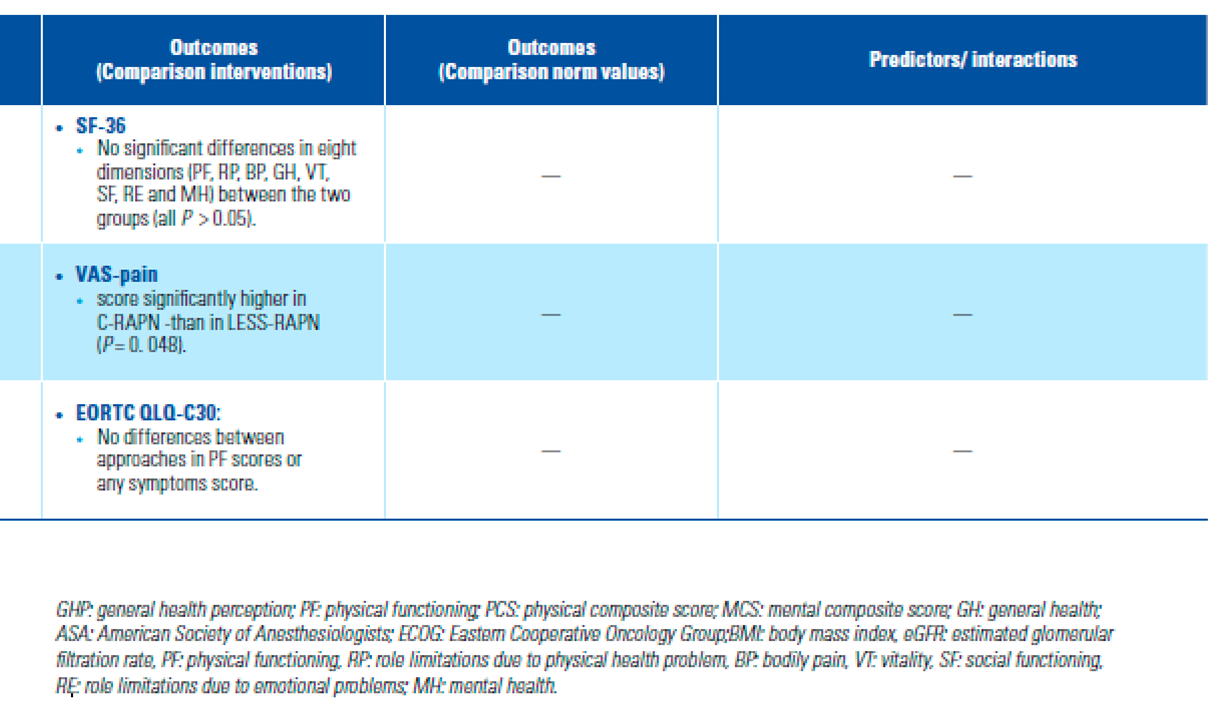
Comparative HRQoL outcomes between or among approaches.
9 cross-sectional studies [16,18,19,20,24,25,27,28,29]. In 1 study, cross-sectional and longitudinal cohorts over- lapped but outcomes were reported separately [23]. The RCT reported outcomes at 1 month [31]. Ten studies reported correction for possible confounders [15,16,17,18,19,20,21,22,23,30] using several statistical methods for adjustment, and 1 study considered only the effect of complications on HRQoL[29] (Table 2 and Table 3).
PROMs Used to Assess QoL and Distribution
Supplementary Table S1 (available at siuj.org) sum- marizes the intended measure and the targeted population of the 15 English original or cross-culturally validated PROMs used. Three were generic (SF-36, SF-12 and VAS), 3 cancer- specific, including one for kidney cancer, and 9 condition-specific, assessing aspects imbricated in HRQoL.
Ten studies used a single PROM [15,16,19,20,22,24,25,26,28,29] and 7 more than 1 [17,18,21,23,27,30,31] (3 and 2 studies used 2 and 3 PROMs respectively, 2 studies, 4 and 5 respectively). The most frequently used PROMs were SF-36, EORTC QLQ-C30, and IES by 8, 5, and 2 studies respectively. The remaining PROMs were used once each. VAS was used in 4 studies to evaluate pain or cosmetic outcomes.
In 10 studies, PROMs were distributed by mail [16,18,20,21,23-25,28–30], 5 were described as self- administered [15,17,22,26,27], and in 2 studies distribu- tion method was not described [19,31].
The response rate was reported in 16 studies [15–26, 28–31], and varied from 37.2% to 93.4%; it was >70% in all but 2 studies [19,21]. Rates of completeness of the questionnaire were reported in only 2 studies [16,21] and were 74% and 37.2%.
Standards for Comparison
There were 3 standards for comparison:
- head-to-head comparison between or among manage- ment strategies in 6 longitudinal [15,17,21,26,30,31] and 9 cross-sectional [16,18,19,20,24,25,27,28,29] studies.
- comparison with the corresponding baseline scores in 6 longitudinal cohorts [17,21,23,26,30].
- comparison with the age–sex normative scores of the country’s general population in 2 longitudinal [22,26] and 5 cross-sectional [18,19,20,23,29] studies.
Outcomes
Six studies presented comparative outcomes on modality [15,16,18,22,23,27], 6 on approach [17,19,20,24,25,31] and 4 reported separately outcomes stratified by modality or approach [21,28,29,30]. Two articles compared an open approach with MIS (RN, PN, or ablation by PCA or PRFA) [26,30].
- Is HRQoL after NSS better than after RN?
Follow-up in longitudinal studies was up to 1 year, although 1 reported up to 7 years [15,21,22,23,26,30]. The cross-sectional time-points evaluations ranged from 12 months to a mean of 40 to 62 months [16,18,23,27,28,29] (Table 2).
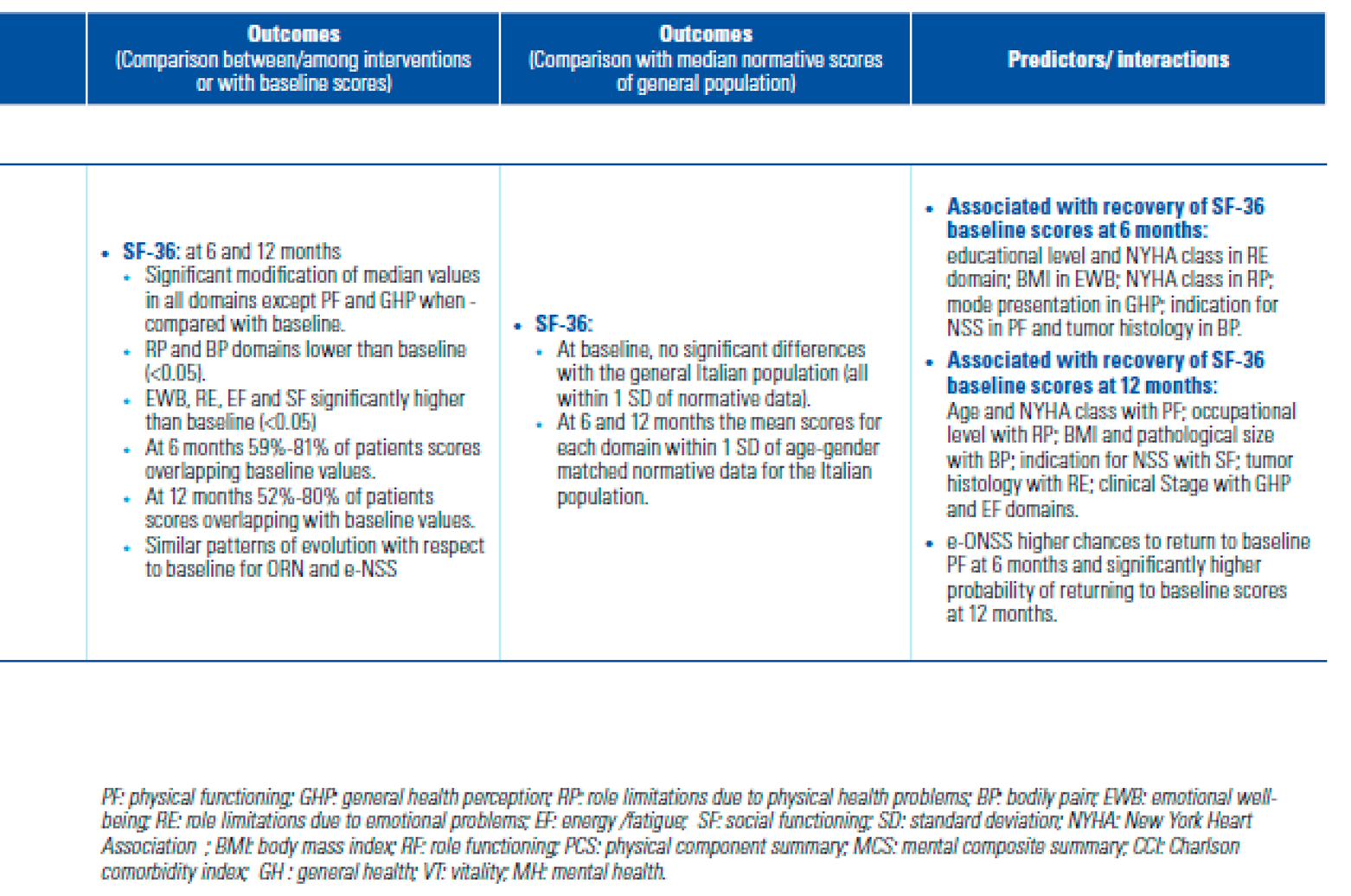
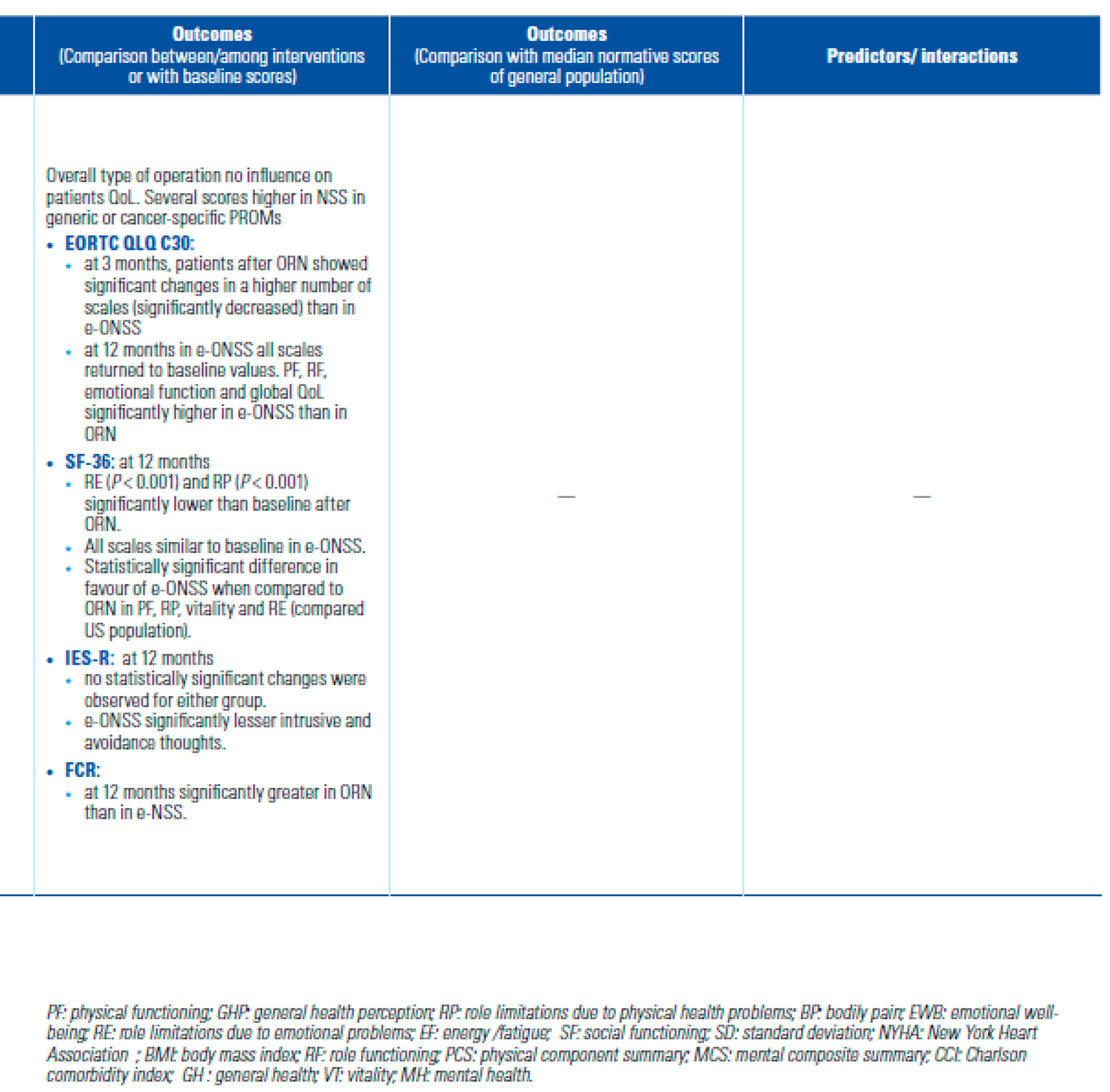
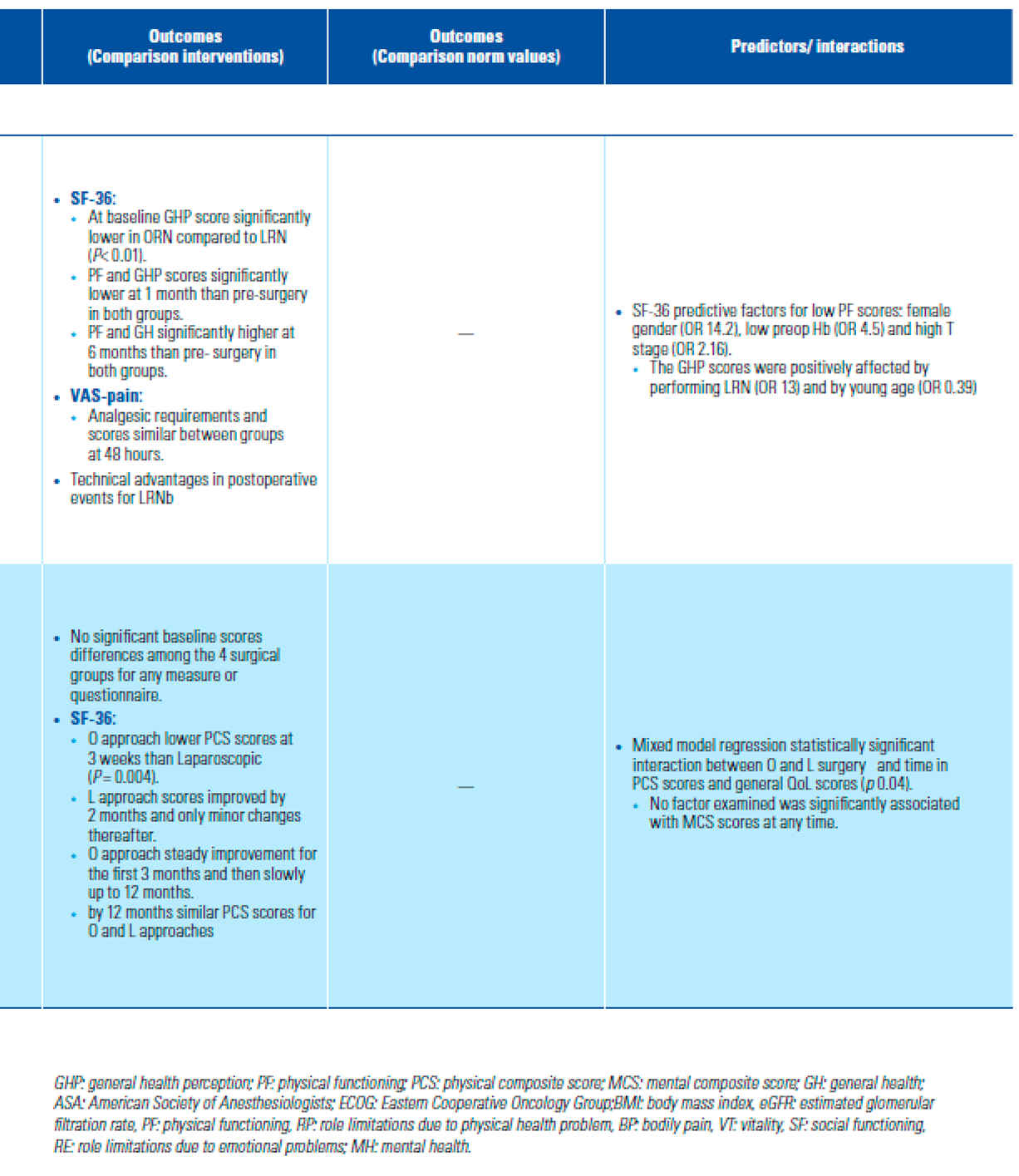
At baseline there was no statistically significant difference in generic or cancer-specific scores between open RN and open NSS [21,22,23,30]. Small but signif- icant changes were seen at 3 and 6 months in most of the scales compared with median baseline scores for RN (open/MIS) and open-NSS [22,23], with the exception of physical functioning, that was similar to baseline at 6 months [22]. At 1 year, all scales overlapped baseline values in 52% to 80% of patients [22] and no differences were seen in mean scores between open-RN and open- NSS or compared with baseline values [29,30]. There were no long-term differences between patients receiving open-RN and open-NSS [18,23], although several scores were higher in the subset of elective-NSS compared with RN or mandatory-NSS [23].
Two longitudinal studies showed earlier improvement in cancer-specific QoL in the NSS group than in the RN group [21,23]. However, better scores than at baseline were reached in RN at 2 months with a clear time-effect improvement up to 1 year [21,30]. At 1-year post procedure, RN was shown to have a detrimental effect on physical and emotional scores, although one series showed all scales returned to baseline levels in NSS [23].
Cross-sectional evaluations showed a negative impact of RN compared with NSS on cancer-specific QoL at 2 years. General health and physical and functional roles improved significantly in both modality groups at 4 years [16], although NSS patients reported better scores, mostly on physical scales [16,23,28].
There were no differences between RN and NSS groups on intrusive thoughts and fear of recurrence at baseline or at 6 months [21,23]. The significant trend to fewer intrusive thoughts about kidney cancer and avoidance behaviour at 1 year for open-NSS, was no longer apparent in the longer term [18,21,23].
Other less frequently used questionnaires showed overlap in the functional impairment for open-NSS and open-RN and a lower level of anxiety and depression in elective open-NSS than in open-RN [27].
- Is HRQoL better after MIS than after open approach?
Three longitudinal [17,21,30] and 3 cross-sectional [19,25,29] studies compared MIS with open approach. Two studies compared MIS with LESS [24,31], and 1 compared 2 open approaches [28] (Table 3). The time-points for evaluation varied from 1 week to 1 to 3 months, and 2 studies conducted an additional assessment at 6 and 12 months [17,21].
In 1 study, general health at baseline was significantly lower in patients undergoing open procedures than in those undergoing MIS-RN [17], whereas no differ- ence was found between MIS and open-RN/NSS in other studies [21,30]. A significant decrease in physical and general health scales occurred in both approaches during the first postoperative weeks, more so for open procedures [21,30]. Patients showed faster improve- ment on physical scales after MIS than after open approach, irrespective of modality (2 versus 3 months). At 6 and 12 months, scales were similar for open and MIS approach [21,25,29,30] and higher or similar to baseline [17,30]. Mental component scales remained unchanged across the follow-up in both groups [21].
At mid- and long-term, cancer-specific QoL was simi- lar between MIS and any open incision for either PN or RN [19,21,30], but patients who underwent MIS reported a short period of convalescence defined as recovery to a performance level of 80% [19].
A small RCT showed better postoperative recov- ery after LESS-RN than conventional LRN [30]. Short- postoperative VAS pain and analgesic requirements were similar between MIS and open approaches [17], while LESS approaches showed inconclusive pain outcomes compared with conventional MIS [24,30].
Overall, older individuals had significantly fewer intrusive thoughts and avoidance behaviour across the first year, regardless of surgical approach [21].
- Comparison with matched age–sex normative scores for the general population
Two longitudinal [22,26] and 3 cross-sectional [18,23,29] studies compared the impact of modality on HRQoL with the country normative population values (Table 2 and Table 3).
At baseline, general QoL median scores of RN (open/ MIS) or open-NSS patients were within 1 SD of the age– sex matched population scores [22]; however, the scales of patients receiving percutaneous TA were signifi- cantly lower [26]. Whether generic or cancer-specific QoL, median physical or mental scores of RN and NSS at 1-year or at long-term did not differ from those of the matched general population [18,22,23,29] with the excep- tion of 1 study that reported higher physical scores than those of the matched population in all groups [29].
Regarding approach, there were no differences at baseline or at 12 months in generic HRQoL between open and MIS (RN/NSS) [29]. Long-term cancer-spe- cific general health and social functioning were higher than in the normative population, irrespective of the approach, although one study reported that treated indi- viduals had more symptoms than the general population [19]. Others found that only laparoscopically treated patients (RN/NSS) scored at the same level as the norma- tive population, while those treated by an open approach experienced a detrimental impact on general health, as well as functional and symptom indices [20].
- HRQoL outcomes in clinical or pathological T1a
Four studies comparing treatment modality included exclusively cT1a RMs or pT1a RCCs [15,18,26,28] and 1 also approach [28]. Adjustment for confounders was tested in 2 studies [15,18] (Table 2 and Table 3).
At baseline, patients choosing AS or receiving subse- quent treatment by RN or TA had significantly lower generic QoL scores than those preferring upfront PN, after controlling for time, age, sex, CCI, and BMI [15]. Total scores remained significantly lower in AS than in RN for up to 2 years, while mental health scores were comparable across groups during follow-up [15].
Baseline scales of patients receiving PRFA were significantly lower than the national norm or than those of LRN patients[26]. After LRN, several physical and emotional scores were significantly lower than at base- line, while no changes occurred in PRFA patients. LRN scales recovered between 4 and 12 weeks. Overall, there were no significant differences in scales between the 2 groups during follow-up [26].
Two cross-sectional long-term comparisons between open-RN and PN did not show any impact of modal- ity in HRQoL or differences with the normative popu- lation whether generic or cancer-specific PROMs were used [18,28]. Nevertheless, the physical functioning scale was higher for the NSS group [28].
- Confounders and predictive factors
Overall, 25 covariables were considered across studies as interacting or confounding with general and cancer-specific HRQoL outcomes, or as predictive factors at different time-points in the management process [15,16,17,18,19,20,21,22,23,29,30] (Supplementary Table S2; available at siuj.org).
- Risk of Bias assessment and certainty of evidence
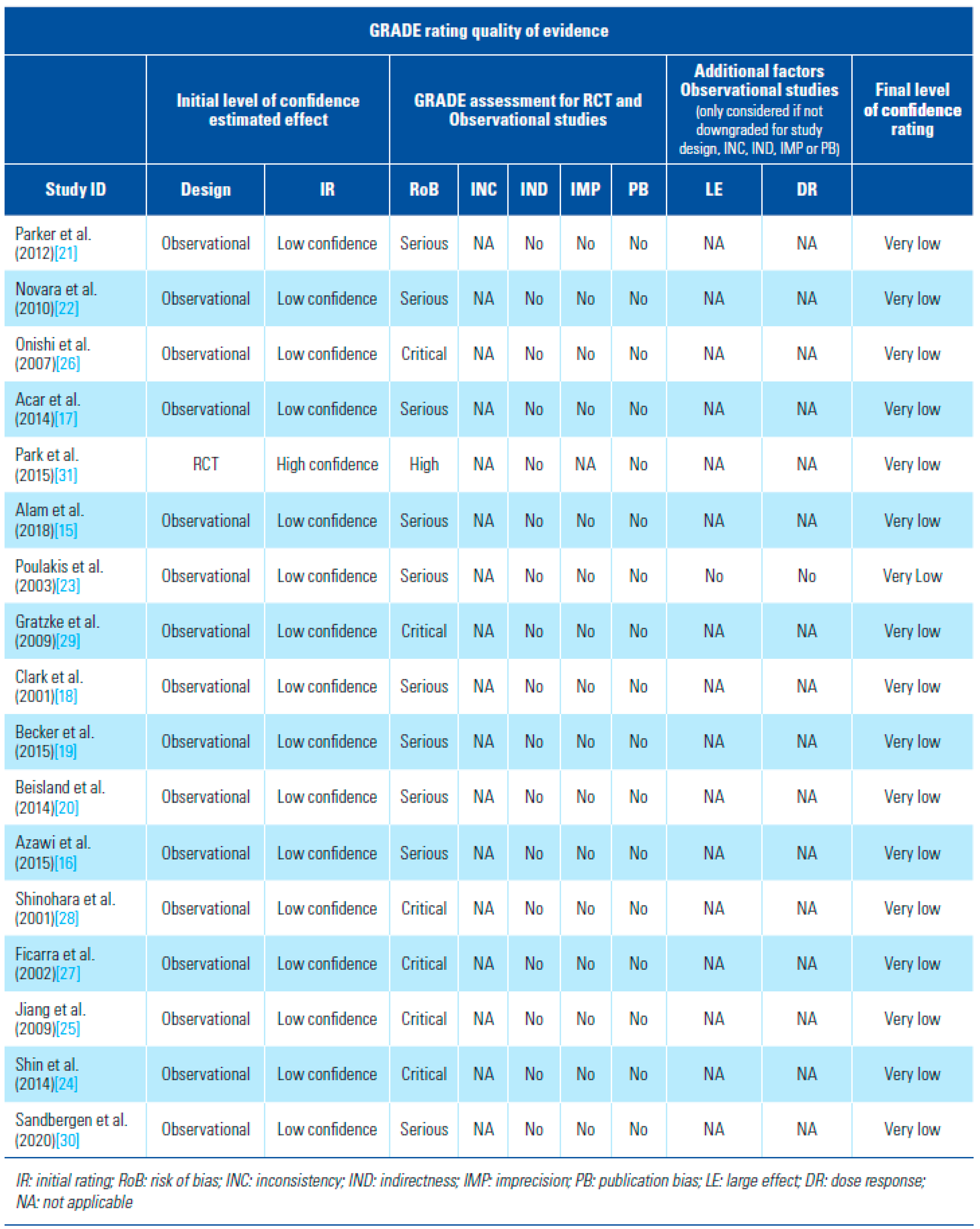
RoB assessment of the 16 observational studies was critical in 6[24,25,26,27,28] and serious in 10 [15,16,17,18,19,20,21,22,23,30] Supplementary Table S3; available at siuj.org). The RCT was judged at high risk of bias for all outcomes[31] (Supplementary Appendix 2a and b; available at siuj.org). Certainty of the evidence was very low for all studies (Table 4).
Table 4.
GRADE certainty of the evidence of the studies included in the systematic review.
Discussion
Our systematic review confirms the post-treatment deleterious effect of both RN and NSS on HRQoL of patients with LRMs/LRCCs during the early post- surgery phase. The effect is more pronounced for RN, mainly affecting the physical and emotional domains. Although the majority of patients in both modalities recover to baseline levels between 6 and 12 months post surgery, the impact of RN may be long-lasting. Reports are more consistent on the lower impact of MIS on QoL scores and on a faster recovery when compared with open approach, especially regarding the physical component scales. Overall, levels of intrusion and avoidance behaviour remained low across the follow-up, irrespective of modality or approach.
Studies comparing HRQoL between surgical manage- ment and AS or percutaneous ablation did not allow for a firm conclusion as in both cases a unique compara- tive study was available. Data on patient baseline QoL suggest a strong directional management selection bias for AS and ablation [15,26,30] in accordance with the clinical selection criteria established for both types of management [32].
Overall, the included studies were heterogenous, most of them with small cohorts, and a wide variety of PROMs were used to assess QoL. Although straightfor- ward comparisons of modality or approach were found, the diversity in reporting and the patient selection bias precluded meta-analysis [10].
As indications for modality depend on tumour and patient characteristics, selection bias may be unavoid- able in HRQoL assessments, even in longitudinal studies. However, the likelihood of bias in cross-sectional evaluations was high, not only because of the lack of baseline assessment but also because unforeseen new factors coexist at evaluation that mask causality even when adjusted analyses are conducted [33].
Apart from the previously mentioned reasons for apparent discordances in outcomes, with respect to modality comparisons, it is the lack of standardization in reporting that stands out as the most important when generic QoL PROMs are used (total global health score versus domain scales) [21,23,28]. For both modality and approach, the different composition of the cohorts with variable proportions of management combinations [17,20,21,30], the different percentage of responders [19,21,23,30], and the lack of adjustment for confounders justified differences in generic and cancer-specific HRQoL outcomes across reports. In some cases, comparison was disparate with respect to modality and approach, so precluding any sound conclusion [26]. A specific questionnaire was used only in a single study [31], or comparisons were conducted between modifications of a unique conceptual approach [24,31].
Importantly, minimal clinically relevant difference in scales or scores was not pre-specified in any study, which precluded any sound comparison and raised the question of whether the QoL values of the norma- tive population should be used as the standard for comparison [34,35].
Regarding cancer-specific HRQoL, different outcomes among studies were mainly related to the use of PROMs designed to measure different aspects of HRQoL [16,23,28]. While EORTC QLQ-C30 measures cancer patients’ physical, psychological, and social functions in general [36], SFKI-15 focuses on renal cancer-specific symptoms and concerns [37] and CARES- SF assesses rehabilitation needs and day-to-day problems of cancer patients [38]. Each instrument has strengths and weakness, but so far there is no evidence on the equivalence among them, and notably none is designed for the specific population of our review.
The strength of this systematic review is the robust and transparent methodological approach, as well as the critical assessment of the risk of bias of the observational studies [13]. The limitations are related to the heteroge- neity in the design, methodology, and reporting of the studies assessing HRQoL in LRMs or LRCC.
Although we considered only reports using cross-cul- tural validated PROMs, there was a surprising variety of instruments used across studies, and this compli- cated data interpretation and weakened possible differ- ences in comparative outcomes either in modalities or approaches [33]. Although most of them investigated dimensions related to QoL, conclusions are restricted to those used in the majority of studies (SF-36 and EORTC QOL-C30) when used optimally [39,40].
Lastly, although most of the papers reviewed were published relatively recently, none of them adhered to contemporary checklists or guidelines to report on HRQoL assessed by PROMs [41,42,43,44] (in some cases because the guidelines were published even more recently).
Although the study limitations confer a critical risk of bias on our review and the quality of evidence is low, we have identified important shortcomings that can help to guide future research. There is no PROM specifically designed to measure HRQoL of patients with LRMs, raising the question of whether one is needed. On the rationale that cure rate and competing risk of death are high in the majority of patients with LRMs [45], the goal might very well be to reach age–sex adjusted normative HRQoL scores. The decision belongs to the consen- sus among the different stakeholders involved in the process of care of LRMs and the increasing acceptance of evaluate outcomes beyond the clinical frame [8,46]. Furthermore, some benefits of MIS approaches that may have a meaningful impact on patient perception of QoL—eg, decreased effect on body image dysmorphism and/or enhanced cosmetic aspect—are difficult to ascer- tain in the current PROMs.
When designing studies on HRQoL, a strict meth- odology should be followed [43,45,47,48], which has not been the case so far with LRMs. Precise, valid, reli- able, responsive, and user-friendly PROMs combined with robustly designed studies and computer adap- tative testing offer the chance to include large cohort populations and minimize the burden for patients and physicians [44,48].
Conclusions
Our systematic review on HRQoL following management of LRMs /LRCC shows evidence that the impact of surgery is considerable during the first weeks and months, although this rarely persists in the longer term. There is no conclusive evidence supporting the superiority of NSS over RN. Nevertheless, there is low evidence to support the use of MIS approaches over open surgery on the basis of earlier postoperative recovery. The impact of surgical management on global mental health seems to be negligible in the long term.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/2563-6499/3/4/209/s1, Figure S1: title; Table S1: title; Video S1: title.
Funding
L.S. received funding from Cure for Cancer.
Acknowledgments
We would like to thank Professor Christian Beisland (Norway) and Professor Abhay Rane (United Kingdom) for responding to our queries on their studies.
Conflicts of Interest
None declared.
Abbreviations
| AS | active surveillance |
| HRQoL | health-related QoL |
| LRCC | localized renal cell carcinoma |
| LRM | localized renal mass |
| MIS | minimally invasive surgery |
| NSS | nephron-sparing surgery |
| PN | partial nephrectomy |
| PROM | patient reported outcome measures |
| RCC | renal cell carcinoma |
| RCT | randomized controlled trial |
| RN | radical nephrectomy |
| TA | thermal ablation |
| VAS | visual analog scale |
References
- Saad, A.M.; Gad, M.M.; Al-Husseini MJRuhban, I.A.; Sonbol, M.B.; Ho, T.H. Trends in renal cell carcinoma incidence and mortality in the US in the last two decades; SEER-based study. Clin. Genitourin. Cancer 2019, 17, 46–57.e5. [Google Scholar] [CrossRef] [PubMed]
- Bhindi, B.; Thompson, R.H.; Lohse, C.M.; Mason, R.J.; Frank, I.; Costello, B.A.; et al. The probability of aggressive versus indolent histology based on renal tumor size: implications for surveillance and treatment. Eur Urol. 2018, 74, 489–497. [Google Scholar] [CrossRef] [PubMed]
- Patel, H.D.; Smerjian, A.; Gupta, M.; Pavlovich, C.P.; Johnson, M.H.; Gorin, M.A.; et al. Surgical removal of renal tumours with low metastatic potential based on clinical radiographic size: a systematic review of the literature. Urol Oncol. 2019, 37, 519–524. [Google Scholar] [CrossRef] [PubMed]
- Johnson, D.C.; Vukina, J.; Smith, A.B.; Meyer, A.M.; Wheeler, S.B.; Kuo, T.M.; et al. Preoperatively misclassified, surgically removed benign renal masses: a systematic review of surgical series and United States population level burden estimate. J Urol. 2014, 193, 30–35. [Google Scholar] [CrossRef] [PubMed]
- Pierorazio, P.M.; Johnson, M.H.; Patel, H.D.; Sozio, S.M.; Sharma, R.; Iyoha, E.; et al.; Management of Renal Masses and Localized Renal Cancer Effective Health Care Program. Comparative Effectiveness Review. No 167. Agency for Healthcare research and Quality (AHCQ publication No 16-EHC001-EF, February 2016). Available online: www.ahrq.gov. (accessed on 30 January 2021).
- McLennan, S.; Imamura, M.; Lapitan, M.C.; Omar, M.I.; Lam, T.B.; Hilvano- Cabungcal, A.M.; et al. Systematic review of perioperative and quality of life outcomes following surgical management of localised renal cancer. Eur Urol. 2012, 62, 1097–1117. [Google Scholar] [CrossRef] [PubMed]
- Laviana, A.A.; Pannell, S.C.; Huen, K.H.Y.; Huen, K.H.Y.; Bergman, J. Engaging patients in complex clinical decision-making: successes, pitfalls, and future directions. Urol Oncol. 2017, 35, 569–573. [Google Scholar] [CrossRef] [PubMed]
- Briffa, N. The employment of patient-reported outcome measures to communicate the likely benefits of surgery. Patient Relat Outcome Meas. 2018, 9, 263–266. [Google Scholar] [CrossRef] [PubMed]
- King, S.C.; Pollack, L.A.; Li, J.; King, J.B.; master, V.A. Continued increase in incidence of renal cell carcinoma, especially in young patients and high-grade disease: United States 2001 to 2010. J Urol. 2014, 191, 1665–1670. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA, group. Preferred reporting items for systematic reviews and metanalysis: the PRISMA statement. J Clin Epidemiol. 2009, 62, 1006–1012. [Google Scholar] [CrossRef]
- Knoll, T.; Omar, M.I.; McLennan SHernandez, V.; Canfield, S.; Yuan, Y.; et al. Key steps in conducting systematic reviews for underpinning clinical practice guidelines: methodology of the European Association of Urology. Eur Urol. 2018, 73, 290–300. [Google Scholar] [CrossRef]
- Sterne, J.; Hernan, M.A.; Reeves, B.C.; Savovic, S.; Berkman, N.D.; Viswanathan, M.; et al. ROBINS-I: a tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Altman, D.G.; Gotzsche, P.C.; Juni, P.; Moher, D.; Oxman, A.O.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [PubMed]
- Johnston, B.C.; Patrick, D.L.; Busse, J.W.; Schunemann, H.J.; Agarwal, A.; Guyatt, G.H. Patient-reported outcomes in meta-analyses–Part 1, assessing risk of bias and combining outcomes. Health Qual Life Outcomes. 2013, 11, 109. [Google Scholar] [CrossRef] [PubMed]
- Alam, R.; Patel, H.D.; Osumah, T.; Srivastava, A.; Gorin, M.A.; Johnson, M.A.; et al. Comparative effectiveness of management options for patients with small renal masses: a prospective cohort study. BJU Int. 2019, 123, 42–50. [Google Scholar] [CrossRef] [PubMed]
- Azawi, N.H.; Tesfalem, H.; Dahl, C. Lund L Do the different types of renal surgery impact the quality of life in the postoperative period? Int Urol Nephrol. 2015, 47, 263–269. [Google Scholar] [CrossRef] [PubMed]
- Acar, C.; Bilen, C.; Bayazit, Y.; Aslan, G.; Koni, A.; Basok, E.; et al. Quality of life survey following laparoscopic and open radical nephrectomy. Urol J. 2014, 11, 1944–1950. [Google Scholar] [PubMed]
- Clark, P.E.; Schover, L.R.; Uzzo, R.G.; Hafez, K.S.; Rybicki, L.A.; Novick, A.C. Quality of life and psychological adaptation after surgical treatment for localized renal cell carcinoma: impact of the amount of remaining renal tissue. Urology 2001, 57, 252–256. [Google Scholar] [CrossRef] [PubMed]
- Becker, A.; Pradel, L.; Kluth, L.; Schmid, M.; Eichelberg, C.; Ahyai, S.; et al. Laparoscopic versus open partial nephrectomy for clinical T1 renal masses: no impact of surgical approach on perioperative complications and long-term postoperative quality of life. World J Urol. 2015, 33, 421–426. [Google Scholar] [CrossRef] [PubMed]
- Beisland, C.; Beisland, E.; Hjelle, K.M.; Bostad, L.; Jensen Hedjermstad, M.; Aarstad, A.K.H.; et al. Health-related quality of life in long-term survivors after renal cancer treatment. Scand J Urol. 2014, 48, 52–64. [Google Scholar] [CrossRef]
- Parker, P.A.; Swartz, R.; Fellman, B.; Urbauer, D.; Li, Y.; Pisters, L.L.; et al. Comprehensive assessment of quality of life and psychosocial adjustment in patients with renal tumors undergoing open, laparoscopic and nephron sparing surgery. J Urol. 2012, 187, 822–826. [Google Scholar] [CrossRef]
- Novara, G.; Secco, S.; Botteri, M.; De Marco, V.; Artibani, W.; Ficarra, V. Factors predicting health-related quality of life recovery in patients undergoing surgical treatment for renal tumors: prospective evaluation using the RAND SF-36 Health Survey. Eur Urol. 2010, 57, 112–120. [Google Scholar] [CrossRef] [PubMed]
- Poulakis, V.; Witzsch, U.; de Vries, R.; Moeckel, M.; Becht, E. Quality of life after surgery for localized renal cell carcinoma: comparison between radical nephrectomy and nephron-sparing surgery. Urology 2003, 62, 814–820. [Google Scholar] [CrossRef] [PubMed]
- Shin, T.Y.; Lim, S.K.; Komninos, C.; Kim, D.W.; Han, W.K.; Hong, S.J.; et al. Laparoendoscopic single-site (LESS) robot-assisted partial nephrectomy (RAPN) reduces postoperative wound pain without a rise in complication rates. BJU Int. 2014, 114, 555–561. [Google Scholar] [CrossRef] [PubMed]
- Jiang, J.; Zheng, X.; Qin, J.; Zheng, M.; Mao, Q.; Zhang, Z.; et al. Health-related quality of life after hand-assisted laparoscopic and open radical nephrectomies of renal cell carcinoma. Int Urol Nephrol. 2009, 41, 23–27. [Google Scholar] [CrossRef] [PubMed]
- Onishi, T.; Nishikawa, K.; Hasegawa, Y.; Yamada y Soga, N.; Arima, K.; et al. Assessment of health-related quality of life after radiofrequency ablation or laparoscopic surgery for small renal cell carcinoma: a prospective study with medical outcomes Study 36-Item Health Survey (SF-36). Jpn J Clin Oncol. 2007, 37, 750–754. [Google Scholar] [CrossRef] [PubMed]
- Ficarra, V.; Novella, G.; Sarti, A.; Novara, G.; Galfano, A.; Cavalleri, S.; et al. Psycho-social well-being and general health status after surgical treatment for localized renal cell carcinoma. Int Urol Nephrol. 2002, 34, 441–446. [Google Scholar] [CrossRef] [PubMed]
- Shinohara, N.; Harabayashi, T.; Sato, S.; Hioka, T.; Tsuchiya, K.; Koyanagi, T. Impact of nephron-sparing surgery on quality of life in patients with localized renal cell carcinoma. Eur Urol. 2001, 39, 114–119. [Google Scholar] [CrossRef]
- Gratzke, C.; Seitz, M.; Bayrle, F.; Schlenker, B.; Bastian, P.J.; Haseke, N.; et al. Quality of life and perioperative outcomes after retroperitoneoscopic radical nephrectomy (RN), open RN and nephron-sparing surgery in patients with renal cell carcinoma. BJU Int. 2009, 104, 470–475. [Google Scholar] [CrossRef]
- Sandbergen, L.; Spriensma, A.S.; de la Rosette, J.J.; Laguna, M.P. Health- related quality of life in localized renal masses: a matter of sparing nephrons or minimizing the incision? Urol Oncol. 2020, 38, 43e1–43e11. [Google Scholar] [CrossRef]
- Park, Y.H.; Kim, K.T.; Ko, K.; Kim, H.H. Prospective randomized controlled trial of conventional laparoscopic versus laparoendoscopic single-site radical nephrectomy for localized renal cell carcinoma: a preliminary report regarding quality of life. World J Urol. 2015, 33, 367–72. [Google Scholar] [CrossRef]
- Chandrasekar, T.; Boorjian, S.A.; Capitanio, U.; Gershman, B.; Mir, M.C.; Kutikov, A. Eur Urol. Collaborative review: factors influencing treatment decisions for patients with a localized solid renal mass. Eur Urol. 2021. [Google Scholar] [CrossRef] [PubMed]
- Blome, C.; Augustin, M. Measuring change in quality of life: bias in prospective and retrospective evaluation. Value Health 2015, 18, 110–115. [Google Scholar] [CrossRef]
- Bakas T, McLennon SM, Carpenter JS, Buelow JM, Otte JL, Hanna KM, et al. Systematic review of health-related quality of life models. Health Qual Life Outcomes. 2012, 10, 134. [Google Scholar] [CrossRef]
- Samsa, G.; Edelman, D.; Rothman, M.L.; Williams, J.R.; Lipscomb, J.; Matchar, D. Determining clinically important differences in health status measures. A general approach with illustration to the Health Utilities Index Mark II. Pharmacoeconomics 1999, 15, 141–155. [Google Scholar] [CrossRef] [PubMed]
- Aaronson, N.K.; Ahmedzai, S.; Bergman, B.; Bullinger, M.; Cull, A.; Duez, N.J.; et al. The European Organization for research and Treatment of Cancer QLQ-C30, a quality-of-life instrument for use in international clinical trials in oncology. J Natl Cancer Inst. 1993, 85, 365–376. [Google Scholar] [CrossRef] [PubMed]
- Cella, D.; Yount, S.; Du, H.; Dhanda, R.; Gondek, K.; Langefeld, K.; et al. Development and validation of the functional Assessment of Cancer Therapy-Kidney Symptoms Index (FKSI). J Support Oncol. 2006, 4, 191–199. [Google Scholar] [PubMed]
- Coscarelli Schag, C.A.; Ganz, P.A.; Heinrich, R.L. Cancer Rehabilitation Evaluation System-Short Form (CARES-SF). Cancer 1991, 68, 1406–1413. [Google Scholar] [CrossRef]
- Hyland, M.E. A brief guide to the selection of quality of life instruments. Health Qual Life Outcomes 2003, 1, 24. [Google Scholar] [CrossRef]
- Briancon, S.; Gergonne, B.; Gullemin, F.; Emepereur, F.; Klein, S. Disease- specific versus generic measurements of health related quality of life in cross-sectional and longitudinal studies: an inpatient investigation of the SF-36 and four disease-specific instruments. In Statistical Methods for Quality of Life Studies; Mesbah, M., Cole, B.F., Lee, L.T., Eds.; Springer: Boston, MA, 2002; pp. 87–99. [Google Scholar] [CrossRef]
- Efficace, F.; Bottomley, A.; Osoba, D.; Gotay, C.; Fletchner, H.; D’haese, S.; et al. Beyond the development of health-related quality-of-life (HRQOL) measure: a checklist for evaluating HRQOL outcomes in cancer clinical trials-does HRQOL evaluation in prostate cancer research inform clinical decision making? J Clin Oncol. 2003, 21, 3502–3511. [Google Scholar] [CrossRef]
- Calvert, M.; Kyte, D.; Mercieca-Bebber, R.; Slade, A.; Chan, A.W.; King, M.T.; et al. Guidelines for inclusion of patient- reported outcomes in clinical trial protocols: the SPIRIT-PRO extension. JAMA 2018, 319, 483–494. [Google Scholar] [CrossRef]
- Prinsen, C.A.C.; Mokkink, L.B.; Bouter, L.M.; Alonso, J.; Patrick, D.L.; de Vet, H.C.W.; et al. COSMIN guidelines for systematic reviews of patient -reported outcome measures. Qual Life Res. 2018, 27, 1147–1157. [Google Scholar] [CrossRef] [PubMed]
- Lapin, B.R. Considerations for reporting and reviewing studies including health-related quality of life. Chest 2020, 158, S49–S56. [Google Scholar] [CrossRef] [PubMed]
- Kutikov, A.; Egleston, B.L.; Wong, Y.N.; Uzzo, R.G. Evaluating overall survival and competing risk of death in patients with localized renal cell carcinoma using a comprehensive nomogram. J Clin Oncol. 2010, 28, 311–317. [Google Scholar] [CrossRef]
- Ciani, O.; Baldassarre Federici, C. Value lies in the eye of the patients: the why, what, and how of patient-reported outcomes measures. Clin Ther. 2020, 42, 25–33. [Google Scholar] [CrossRef]
- Unger, J.M.; Vaidya, R.; Gore, J.L. Key design and analysis principles for quality of life and patient-reported outcomes in clinical trials. Urol Oncol. 2019, 37, 324–330. [Google Scholar] [CrossRef]
- Reeve, B.B.; Wyrwich, K.W.; Wu, A.W.; Velikova, G.; Terwee, C.B.; Snyder, C.F.; et al. ISOQOL recommends minimum standards for patient-reported outcome measures used in patient centered outcomes. Qual Life Res. 2013, 22, 1889–1905. [Google Scholar] [CrossRef] [PubMed]
This is an open access article under the terms of a license that permits non-commercial use, provided the original work is properly cited. © 2022 The Authors. Société Internationale d'Urologie Journal, published by the Société Internationale d'Urologie, Canada.