Cell-Based Bladder Markers
Several cell-based urine markers are available, including conventional urinary cytology, ImmunoCyt/ uCyt + (Scimedx, Denville, US), fluorescence in situ hybridization (FISH) UroVysion (Abbott Molecular, des Plaines, US) and Cell Detect (Zetiq Technologies Ltd., Tel Aviv, Israel) (
Table 1).
Urine cytology remains the gold standard and the only urine marker that is recommended by the European Association of Urology (EAU) and the American Urological Association (AUA) [
1,
2] for the diagnosis and surveillance of high-grade BC (in combination with cystoscopy).
Overall, the reported sensitivity ranges from 20% to 97.3%; specificity ranges from 74% to 99.5% [
6,
7,
8]. Urine cytology has an excellent specificity with few false-positive cases for high-grade bladder cancer (HGBC) and carcinoma in situ (specificity 83% to 99%) [
1,
9]. Historically, urine cytology had a high sensitivity for HG disease, but more contemporary series reported sensitivity for cytology at 40.8% and 54.3% for HG [
10,
11]. Furthermore, a low sensitivity in low-grade tumors represents a main downside of conventional cytology; therefore, it is not used to replace cystoscopy.
Immunocytology (Immunocyt [UCyt+], Scimedx, US) is based on immunoassays for detection of tumor- associated cell-based antigens. The global sensitivity of immunocytology ranges between 78% and 90% and is higher than that of cytology, especially for low-grade cancers, whereas its specificity has been reported as 68% to 87% and therefore tends to be lower than that of cytology [
12,
13,
14] (
Table 2).
ImmunoCyt/uCyt+ in patients whose cytology was atypical has been frequently discussed as a reflex test to avoid cystoscopy in patients with low-grade cancer since the test has a NPV of 83.7% [
1,
15]. Nevertheless, Immunocyt/uCyt+ has been recently removed from the market.
Fluorescence in situ hybridization (multi-target multicolor FISH—UroVysion) (Abbott Molecular, US) allows the detection of chromosomal abnormalities that are frequently observed in malignant urothelial cells (gains in chromosomes 3, 7, 17 or deletions of chromosome 9). These assays have been shown to be more sensitive than cytology in detecting BC at the cost of a lower specificity. Sensitivity ranges from 50% to 88% and specificity from 78% to 92% [
12,
13,
14], depending on the BC prevalence in the cohort of the study (
Table 3) and also on the criteria of positive tests. FISH sensitivity was reported to be twice as high as cytology for non- muscle invasive bladder cancer (NMIBC) (50.9% versus 29.8%) [
16,
17] and triple (73% versus 24%) when scoring criteria have been modified. Notably the scoring algorithm of the manufacturer was developed for voided urine but was modified for bladder washings [
17,
18].
In patients with atypical cytology or indeterminate cystoscopy, UroVysion may help to identify those who would need further evaluation since 2 prospective studies found a higher likelihood of cancer in patients with positive markers with a reasonable positive predictive value [
19,
20]. This role has been included in the AUA guidelines as a potential use of urine markers. There is evidence from various sources that anticipatory false-positive results exist. Patients with positive FISH but no visible tumor in cystoscopy were reported to be at increased risk for recurrence and progression [
21,
22]. Persisting positive FISH during Bacillus Calmette- Guérin (BCG) immunotherapy increased the risk of recurrence and progression [
23]. Recently, 2 multicenter prospective studies confirmed the predictive value of FISH in detecting recurrence and progression in HGBC treated with BCG [
10,
25]. A positive FISH at initiation or completion of BCG is associated with 3-fold higher rate of recurrence but results in individual patients vary, which makes it challenging to make clinical decisions on the basis of FISH results [
26].
The platform CellDetect (Zetiq Technologies, Israel) uses a proprietary plant extract and 3 dyes that enable color discrimination between malignant (red) and benign (green) cells on the basis of specific metabolic alterations associated with BC. In a multicenter validation study, the test reached a sensitivity of 84% (
Table 3) (78% for detecting LG NMIBC). The specificity was 84% in patients undergoing surveillance by cystoscopy [
24].
DNA-Based Markers
Various types of DNA alterations can occur in, B.C.; such as mutations, copy number alterations, and genomic rearrangements. In general, BC is known to have a high mutational burden [
27,
28]. Until now, none of the DNA-based urine assays that are based on detection of mutations have been FDA approved for use in clinic. Prospective validation of most urine assays is still awaited.
Some of the most frequently found DNA mutations in BC include mutations in the
FGFR3,
RAS,
PIK3CA, and
TERT genes. Approximately two-thirds of NMIBCs have activating
FGFR3 mutations. The number of activating mutations is much lower in MIBC [
29], (only <15% of tumors have
FGFR3 mutations); however, >40% of MIBCs overexpress FGFR3 [
30]. Tumors with an
FGFR3 mutation grow slowly and are less likely than
FGFR3 wild-type tumors to progress to MIBC [
30,
31,
32,
33]. Several hotspot mutations in the
FGFR3 gene have been identified as oncogenic.
In general, mutations in the
KRAS gene are most frequent in cancer. For instance,
KRAS is mutated in 90% of pancreatic cancers and 45% of colorectal cancers [
34]. In, B.C.; HRAS is the most commonly mutated RAS gene: HRAS mutations are present in approximately 5% of bladder tumors [
27].
Further, approximately 20% of BC tumors harbor a mutation in the
PIK3CA gene [
27]. PI3K can be activated by RTKs, or via crosstalk via the RTK-RAS-MAPK pathway. Finally, mutations in the telomerase reverse transcriptase (
TERT) gene are frequent in BC: >70% of bladder tumors harbor a
TERT promotor mutation [
35]. The presence of a
TERT mutation has been found to be more frequent in tumors that also harbored
FGFR3 mutations; however, it was not associated with stage or grade of the tumors [
35]. Overall, significant overlap between different mutations occurs.
Epigenetic studies, such as genome-wide methylation analyses, have identified several genes that are significantly hypermethylated in BC cells compared with normal urothelial cells [
45]. Methylation of several genes was found to be useful for the diagnosis of, B.C.; with some markers being highly specific for BC. Gene hypermethylation has also been proposed in predicting disease progression [
46,
47]. The EpiCheck platform (Nucleix, Israel) has been designed for detection of DNA methylation changes associated with BC in a panel of 15 biomarkers. The test has been validated in several studies that included mainly patients who were under surveillance for NMIBC [
39,
40]. Other assays that were validated in several cohorts have been designed to combine the analysis of both BC-relevant DNA gene methylations and mutations [
42,
49]. Assay results and clinical parameters (type of hematuria) have been incorporated in multivariate models to obtain optimal performance.
In the literature, various DNA-based urinary markers have been developed. For most of these, prospective validation is still lacking. The urine-based markers suggested in the literature can be subdivided into markers used for detection of primary tumors (e.g., in a patient with hematuria) and markers used for detection of recurrent tumors (e.g., patient previously treated for BC). Furthermore, markers based on cell pellet DNA exist, as well as cell-free DNA-based markers
Table 3. provides an overview of studies that combine various DNA marker assays.
RNA-Based Markers
A high number of RNA-based urinary gene panels are being validated, with the aim of improving diagnostic accuracy in BC without decreasing specificity [
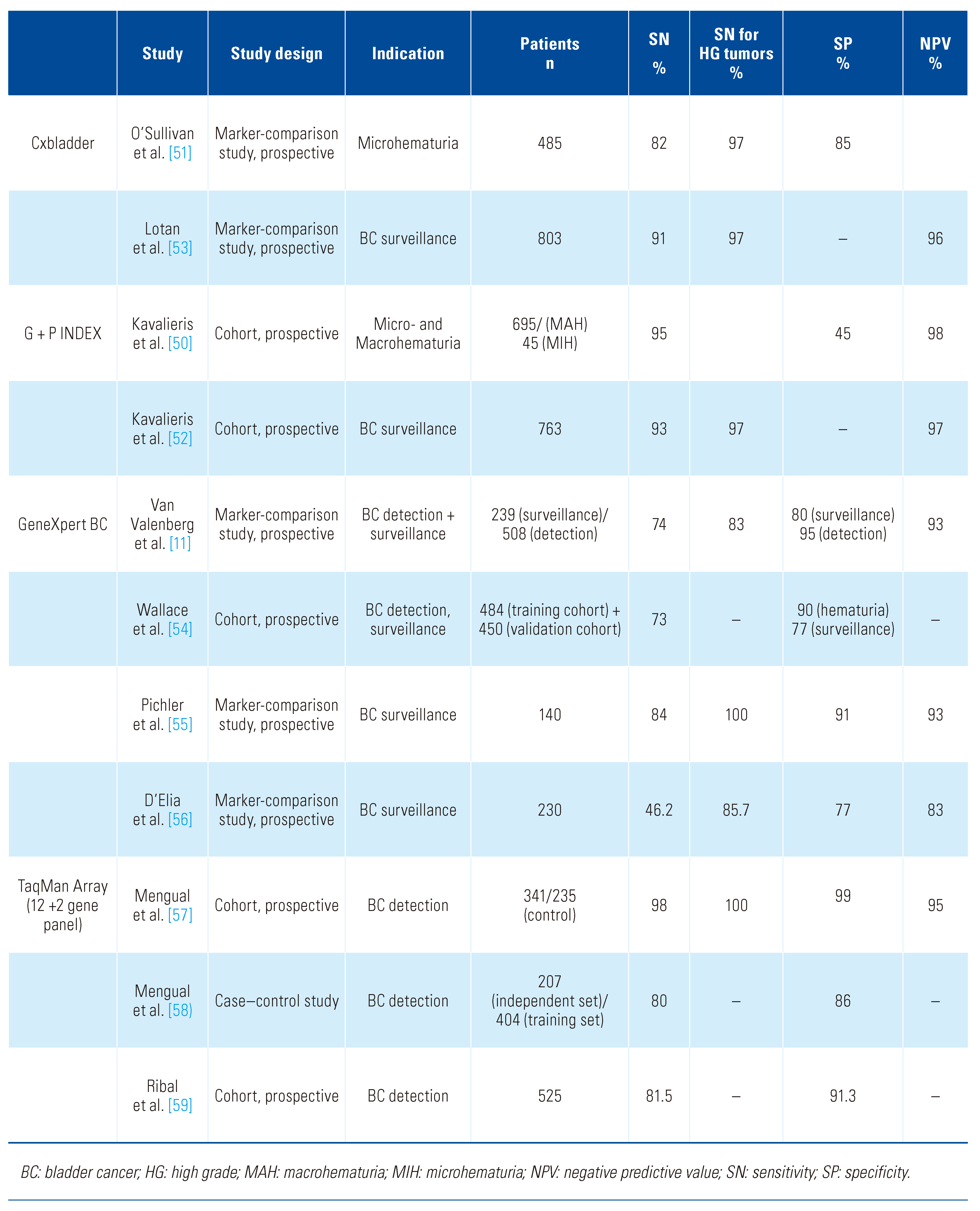
3]. Three messenger RNA (mRNA)-based urinary biomarkers (Cxbladder assay [Pacific Edge Diagnostics, US], GeneXpert BC [Cepheid, US], and TaqMan Array, [ThermoFisher, US]) and various microRNA (miRNA)-based urinary targets (e.g., members of the miRNA-200 family and miRNA-145) are currently tested in clinical trials for BC detection or surveillance.
In detail, 5 published studies [
50,
51,
52,
53] on different clinical scenarios (detection of BC in risk population, and surveillance for recurrent BC) consistently confirmed promising diagnostic performances with a high sensitivity (even in LG tumors on surveillance) and NPV of the Cxbladder assay at the expense of a lower specificity than cytology. For BC screening and detection, the Cxbladder has the potential to reduce the frequency of diagnostic and invasive procedures in patients presenting with hematuria; however, further prospective validation studies are necessary. The GeneXpertBC test has shown 83% to 100% sensitivity for HG tumors and up to 77% sensitivity for LG tumors, and overall sensitivity ranged between 46.2% and 84%. Whereas the specificity in the BC detection population was very high (90% to 95%), in homogeneous data specificity was confirmed for BC surveillance (77% to 91%) [
11,
54,
55,
56].The training and validation study analyzing the diagnostic accuracy of a specific 12 + 2 gene set (TaqMan Array) panel on bladder washings and voided urine samples showed consistently high sensitivities and specificities in BC detection (sensitivity: 70%, 80%, and 98%; specificity: 86%, 96%, and 99%) and for discrimination between LG and HG tumors (sensitivity: 75% to 79%; specificity: 75% to 92%) [
50,
51]. These findings were confirmed in a prospective, blinded multicenter trial [
59]. An overview of the diagnostic performance characteristics of the 3 mRNA-based urine assays for detection/surveillance of BC is shown in
Table 4.
Moreover, miRNAs may become biomarkers for BC detection and surveillance in the future. Nevertheless, identified miRNA signatures were found to be heterogenous in published studies, with few trials confirming their results by independent validation cohorts, resulting in a low degree of reproducibility in the clinical setting. Most trials included only a small number of patients (n = 47 to 207) [
60,
61]. Another controversial issue that is discussed controversially is the feasibility of implementation and application of different analytical platforms and bioinformatics in the clinical setting [
62].
In summary, RNA-based urinary markers are characterized by ease of handling, their brief hands-on sample preparation time, technical instrument systems that automate and integrate all complex PCR processes, and high-quality standards including in-sample quality controls [
55]. One of the major limitations of the application of RNA-based urinary techniques is the difficulty in obtaining sufficient quantity of “high- quality” RNA from voided urine compared with bladder washings. Studies using bladder washings and optimized specimen collection and handling may achieve results that are not attainable in real world practice [
57,
63]. It has been shown that bladder washing samples yielded higher amounts of better RNA-quality than voided urine samples [
57]. Another limitation is the fact that there is a wide variability in the cost of RNA-based urine tests. For widespread use in the future, these tests should be available at reasonable cost. Another challenge of RNA- based urinary markers in preanalytics is the mRNA instability, resulting in an advantage for commercial test systems (working with RNA-stabilizing tubes) compared with single urinary mRNA targets (CAIX or survivin). Standardized processes are indispensable for RNA analysis. According to the current EAU and AUA guidelines, RNA-based urinary biomarkers cannot be recommended for screening, detection of BC in patients with microscopic hematuria, or BC surveillance [
2,
64].
Protein Markers
In comparison with other-omics, the proteome can be directly linked to a phenotype, and hence represents a rich source of biomarkers and therapeutic targets (the latter, however, typically not in urine). On the downside, the extensive complexity and large dynamic range of protein components of a biological sample (in the case of urine, spanning at least 6 orders of magnitude) raise technical challenges, regularly encountered to some extent in proteome analysis and addressed, via the application of high-resolution mass spectrometry-based methodologies [
67]. A large number of proteins have been reported in association with BC phenotypes, for disease prognosis or treatment prediction [
68,
69,
70,
71].
Of the most widely studied, nuclear matrix protein 22 (NMP22), quantified by the point-of-care NMP22 BladderChek, and the NMP22 ELISA immunoassay (Alere/Abbott), has received approval by the FDA for application in BC surveillance (both tests) and detection of the disease in high-risk or symptomatic populations (for the NMP22 BladderChek test only). Similarly, the BTA TRAK immunoassay-based and BTA STAT point- of-care tests (Polymedco), detecting the complement factor H and complement factor H-related protein, have also been granted FDA approval for use in BC diagnosis and surveillance. Meta-analyses of existing studies demonstrate that the performance for both approved markers varies widely among the studies (ranging for the sensitivities and specificities from 47% to > 90%) [
65,
68,
69,
70,
71,
72] (
Table 5). The reported sensitivities are higher than those of cytology in the detection of low- grade disease, but hematuria, infections, presence of stones or instrumentation are frequent confounders, compromising the specificity of the assays [
73].
Besides the abovementioned FDA-approved tests, several additional exploratory protein biomarkers have been reported in primary diagnosis, and in cancer detection during surveillance and/or monitoring of treatment response. Among the most frequently reported are proteins of the extracellular and the nuclear matrix, apolipoproteins (apolipoprotein A-I, apolipoprotein A-II, apolipoprotein E) and other plasma proteins (alpha 1 anti-trypsin, heparin cofactor II), including angiogenic factors (such as angiogenin, vascular endothelial growth factor A-VEGFA), as well as inflammatory factors (such as interleukins 2, 6, 8, 10, TNFα) [
68,
70]. Commercially available assays for the measurement of some of these proteins have been established; these include the UBC Rapid, (IDL Biotech AB) or CYFRA 21-1 (Cisbio International) tests measuring cytokeratin fragments— mainly of cytokeratins 8 and 18 for the former [
74] and cytokeratin 19 for the latter [
75]—or ADXBLADDER, (Arquer Diagnostics Ltd.), quantifying the levels of the mini-chromosome maintenance-MCM 5 protein [
76], having being tested mainly in diagnostic contexts of use and, as essentially with all tests, exhibiting better performance in advanced than in early grade and stage tumors.
Applications in disease prognosis have also been described, including the recent examples of the shed ectodomains of epithelial cell adhesion molecule (EpCAM) and hepatocyte growth factor activator inhibitor-1 (HA-1), exhibiting a prognostic value for disease-specific death (in the range of 2 times increased risk at increased marker levels) in NMIBC [
77]; or various interleukins (such as IL12, TRAIL, TNFα) in response to BCG treatment [
78].
A clear consensus is emerging that combination of individual protein markers with clinicopathological information [
79,
80] in biomarker panels or multi- parametric classifiers results in increased accuracy rates. Examples include the CyPRIT (cytokine panel for response to intravesical therapy) measuring the levels of 9 cytokines, as a predictor of response to BCG treatment in intermediate- and high-risk NMIBC [
78]; or the simultaneous quantification of matrix metalloproteases and plasma proteins via ELISA-based assays in diagnostic contexts of use [
68,
81] (
Table 6). In addition, peptides mainly originating from extracellular matrix proteins (collagens, fibrinogen) but also plasma proteins quantified simultaneously via mass spectrometry-based assays and combined to a classifier (DiaPat) have shown diagnostic value in disease primary detection and surveillance [
82].
Collectively, several urinary protein markers in association with BC phenotypes and prognostic/ predictive contexts of use have been reported. Proper prospective validation is pending to define their added value (stand-alone or in combination) in disease management. Technology advancements allowing the simultaneous detection of marker panels provide a solid basis for future work in this direction.
Clinical Considerations for Use of Urinary Molecular Markers in Context of BC
The various marker tests differ regarding their potential applications in the diagnosis and surveillance of BC. Whereas FISH, immunocytology, and NMP22 have long been considered the most valuable alternatives to cytology, other DNA- and RNA-based assays have drawn broad attention within the last 10 years. With the advent of high-throughput analysis technologies there is the hope that performing multiple analyses in parallel with high resolution will improve the detection rate. Many of these test systems provide information on DNA, RNA, and protein levels. In the future, such information can be helpful not only in the detection of BC but also for the non-invasive monitoring of disease. One potential indication that has been investigated in the context of the UroVysion is the monitoring of patients treated with BCG. Because of the high risk of recurrence in these patients, a marker that provides evidence of response or failure of treatment would be of high value to prevent delay of cystectomy in patients who do not respond to BCG. The high level of complexity of new marker combination panels is associated with various challenges. One main challenge of any combination marker panel that is developed with the goal of achieving a high sensitivity will be to avoid false- positive test results, which has been a major issue in the development of many markers that have been discussed as potential alternatives for cytology.
Any marker or test system that is supposed to be broadly implemented in clinical practice requires prospective clinical trials to address the value of the test in the relevant clinical context. Case–control studies provide preliminary information on test characteristics but will not be sufficient for a broad clinical use. A common study design used for validation of promising markers is to analyze urine samples prospectively from patients undergoing cystoscopy because of suspicion of BC. One of the primary goals of urine biomarkers in this context is to replace cystoscopy, but the cohorts studied are typically too heterogenous with respect to the indication for evaluation (gross hematuria, microscopic hematuria, or irritative voiding symptoms), so that the study results are not adequate to change practice. Moreover, many studies include both patients undergoing primary diagnostic workup and those under surveillance. Such heterogeneity potentially explains the considerable differences of test performances between different validation studies. To avoid such heterogeneity of patient groups, it makes sense to test the potential of urine markers in specific clinical settings. Both clinicians and companies should make every effort to validate an assay in a prospective trial designed in cooperation with guideline panels and key opinion leaders. One example of a prospective trial that has been set up in a specific setting with a specific hypothesis is the Uro
Follow trial [
83]. In this trial, patients with low grade NMIBC are randomized to receive standard of care surveillance using cystoscopy versus regular measurement of urine markers (including cytology and UroVysion), with cystoscopies performed only in the case of a positive marker or clinical signs of recurrence. The hypothesis of the trial is that a urinary marker-based follow-up is non-inferior to a cystoscopy- based follow-up with respect to detection of recurrence and progression.
Another clinical trial (NCT03988309) is randomizing patients to a marker-based approach using Cxbladder versus a standard evaluation for patients with hematuria. The goal of the trial is to determine if a risk-based approach with the addition of a marker is superior to cystoscopy for all patients.
Such specific study designs will not only allow a better understanding of the performance of an assay but also provide data on the potential use of a specific test.