
Are There Differences in Postural Control and Muscular Activity in Individuals with COPD and with and Without Sarcopenia?

 , and
, and
Abstract
Highlights
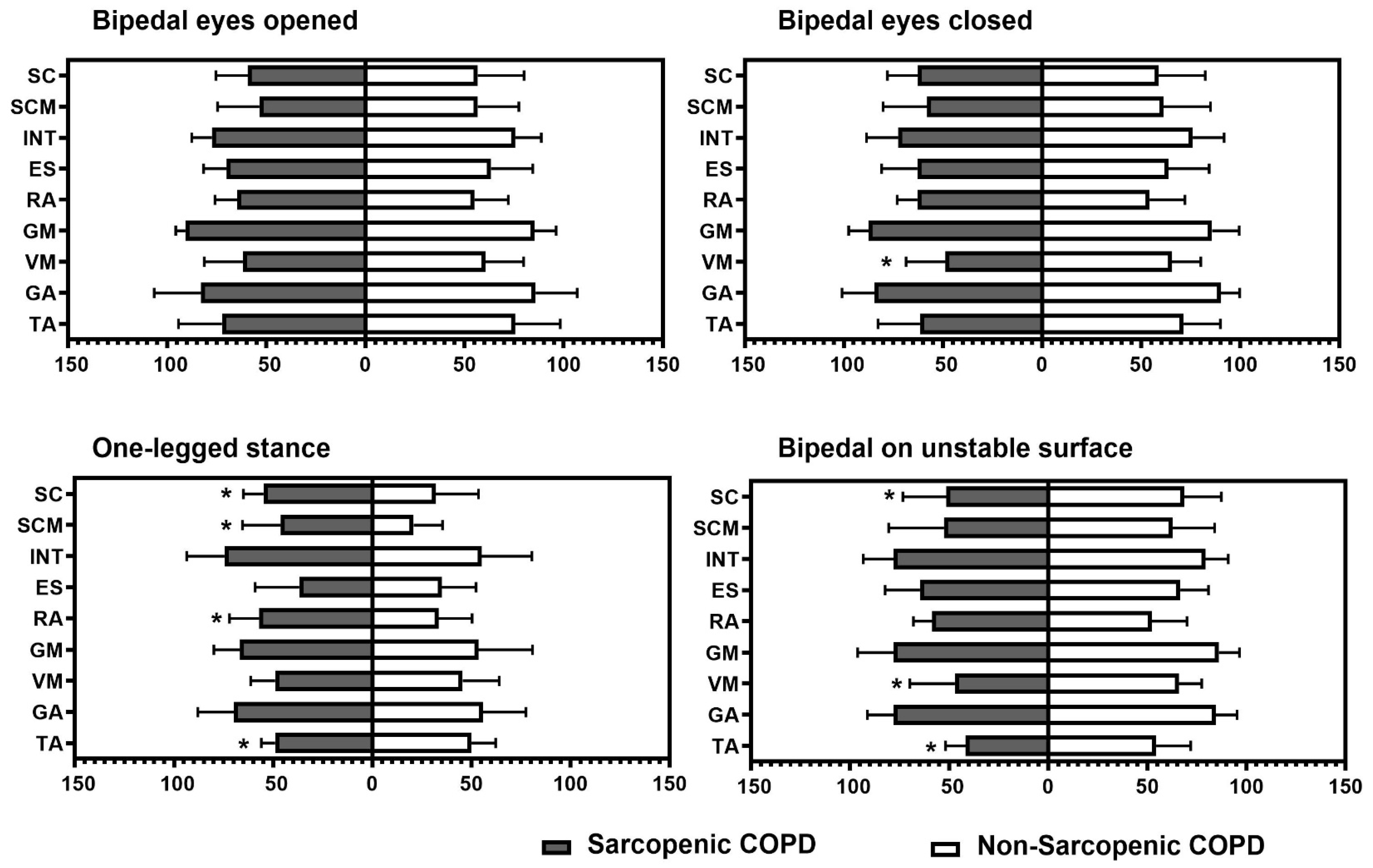
- Individuals with COPD and sarcopenia exhibit poorer balance performance and reduced activation of lower limb muscles compared to those without sarcopenia.
- It is crucial to implement prevention and management strategies that include strengthening exercises for patients with COPD and sarcopenia to reduce the risk of falls.
- There is a need for more detailed assessments and specific rehabilitation programs to improve balance and muscle strength in patients with COPD and sarcopenia.
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Sample
2.2. Sarcopenia Diagnosis
2.3. Static Balance
2.4. Muscular Activation
2.5. Functional Balance
2.6. Dynamic Balance
2.7. Pulmonary Function
2.8. Comorbidities
2.9. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- The Global Strategy for Diagnosis, Management and Prevention of COPD (Updated 2025), the Pocket Guide (Updated 2025) and the Complete List of References Examined by the Committee is Available on the GOLD Website. Available online: www.goldcopd.org (accessed on 15 November 2024).
- Costa, T.M.d.R.L.; Costa, F.M.; Moreira, C.A.; Rabelo, L.M.; Boguszewski, C.L.; Borba, V.Z.C. Sarcopenia in COPD: Relationship with COPD severity and prognosis. J. Bras. Pneumol. 2015, 41, 415–421. [Google Scholar] [CrossRef] [PubMed]
- Rolland, Y.; Czerwinski, S.; Abellan Van Kan, G.; Morley, J.E.; Cesari, M.; Onder, G.; Woo, J.; Baumgartner, R.; Pillard, F.; Boirie, Y.; et al. Sarcopenia: Its assessment, etiology, pathogenesis, consequences and future perspectives. J. Nutr. Health Aging 2011, 12, 433–450. [Google Scholar] [CrossRef] [PubMed]
- Annegarn, J.; Meijer, K.; Passos, V.L.; Stute, K.; Wiechert, J.; Savelberg, H.H.; Schols, A.M.; Wouters, E.F.; Spruit, M.A.; Ciro+ Rehabilitation Network. Problematic activities of daily life are weakly associated with clinical characteristics in COPD. J. Am. Med. Dir. Assoc. 2012, 13, 284–290. [Google Scholar] [CrossRef] [PubMed]
- Weldam, S.W.M.; Schuurmans, M.J.; Liu, R.; Lammers, J.-W.J. Evaluation of Quality of Life instruments for use in COPD care and research: A systematic review. Int. J. Nurs. Stud. 2013, 50, 688–707. [Google Scholar] [CrossRef] [PubMed]
- Chuatrakoon, B.; Ngai, S.P.; Sungkarat, S.; Uthaikhup, S. Balance Impairment and Effectiveness of Exercise Intervention in Chronic Obstructive Pulmonary Disease—A Systematic Review. Arch. Phys. Med. Rehabil. 2020, 101, 1590–1602. [Google Scholar] [CrossRef]
- Araújo de Castro, L.; Morita, A.A.; Sepúlveda-Loyola, W.; da Silva, R.A.; Pitta, F.; Krueger, E.; Probst, V.S. Are there differences in muscular activation to maintain balance between individuals with chronic obstructive pulmonary disease and controls? Respir. Med. 2020, 173, 106016. [Google Scholar] [CrossRef]
- Pasten, J.G.; Aguayo, J.C.; Aburto, J.; Araya-Quintanilla, F.; Álvarez-Bustos, A.; Valenzuela-Fuenzalida, J.J.; Camp, P.G.; Sepúlveda-Loyola, W. Dual-Task Performance in Individuals With Chronic Obstructive Pulmonary Disease: A Systematic Review With Meta-Analysis. Pulm. Med. 2024, 2024, 1230287. [Google Scholar] [CrossRef]
- Beauchamp, M.K.; O’Hoski, S.; Goldstein, R.S.; Brooks, D. Effect of pulmonary rehabilitation on balance in persons with chronic obstructive pulmonary disease. Arch. Phys. Med. Rehabil. 2010, 91, 1460–1465. [Google Scholar] [CrossRef]
- Oliveira, C.C.; Annoni, R.; Lee, A.L.; McGinley, J.; Irving, L.B.; Denehy, L. Falls prevalence and risk factors in people with chronic obstructive pulmonary disease: A systematic review. Respir. Med. 2021, 176, 106284. [Google Scholar] [CrossRef]
- Zhou, J.; Liu, Y.; Yang, F.; Jing, M.; Zhong, X.; Wang, Y.; Liu, Y.; Ming, W.; Li, H.; Zhao, T.; et al. Risk Factors of Sarcopenia in COPD Patients: A Meta-Analysis. Int. J. Chronic Obstr. Pulm. Dis. 2024, 19, 1613–1622. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia in Older People 2 (EWGSOP2), and the Extended Group for EWGSOP2. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef] [PubMed]
- Sepulveda-Loyola, W.; Junior, P.S.P.; Fuenzalida, J.J.V.; Santillán-Zuta, M.; Probst, V.S. Impact of pre-sarcopenia and sarcopenia on biological and functional outcomes in individuals with chronic obstructive pulmonary disease: A cross-sectional study. Nutr. Clín. Diet. Hosp. 2024, 44, 295–302. [Google Scholar] [CrossRef]
- Sepúlveda-Loyola, W.; Osadnik, C.; Phu, S.; Morita, A.A.; Duque, G.; Probst, V.S. Diagnosis, prevalence, and clinical impact of sarcopenia in COPD: A systematic review and meta-analysis. J. Cachexia Sarcopenia Muscle 2020, 11, 1164–1176. [Google Scholar] [CrossRef] [PubMed]
- Álvarez-Bustos, A.; Rodríguez-Sánchez, B.; Carnicero-Carreño, J.A.; Sepúlveda-Loyola, W.; Garcia-Garcia, F.J.; Rodríguez-Mañas, L. Healthcare cost expenditures associated to frailty and sarcopenia. BMC Geriatr. 2022, 22, 747. [Google Scholar] [CrossRef]
- Miller, M.R.; Hankinson, J.; Brusasco, V.; Burgos, F.; Casaburi, R.; Coates, A.; Crapo, R.; Enright, P.; Van Der Grinten, C.P.M.; Gustafsson, P.; et al. Standardisation of spirometry. Eur. Respir. J. 2005, 26, 319–338. [Google Scholar] [CrossRef]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P.; STROBE Initiative. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. Ann. Intern. Med. 2007, 147, 573–577. [Google Scholar] [CrossRef]
- Kyle, U.G.; Genton, L.; Karsegard, L.; Slosman, D.O.; Pichard, C. Single Prediction Equation for Bioelectrical Impedance Analysis in Adults Aged 20–94 Years. Nutrition 2001, 17, 248–253. [Google Scholar] [CrossRef]
- Travassos, A.; Rodrigues, A.; Furlanetto, K.C.; Donária, L.; Bisca, G.W.; Nellessen, A.G.; Pitta, F.; A Hernandes, N. Fat-free mass depletion in patients with COPD in Brazil: Development of a new cutoff point and its relation with mortality and extrapulmonary manifestations. Eur. J. Clin. Nutr. 2017, 71, 1285–1290. [Google Scholar] [CrossRef]
- Leong, D.P.; Teo, K.K.; Rangarajan, S.; Kutty, V.R.; Lanas, F.; Hui, C.; Quanyong, X.; Zhenzhen, Q.; Jinhua, T.; Noorhassim, I.; et al. Reference ranges of handgrip strength from 125,462 healthy adults in 21 countries: A prospective urban rural epidemiologic (PURE) study. J. Cachex Sarcopenia Muscle 2016, 7, 535–546. [Google Scholar] [CrossRef]
- da Silva, R.A.; Bilodeau, M.; Parreira, R.B.; Teixeira, D.C.; Amorim, C.F. Age-related differences in time-limit performance and force platform-based balance measures during one-leg stance. J. Electromyogr. Kinesiol. 2013, 23, 634–639. [Google Scholar] [CrossRef]
- Michikawa, T.; Nishiwaki, Y.; Takebayashi, T.; Toyama, Y. One-leg standing test for elderly populations. J. Orthop. Sci. 2009, 14, 675–685. [Google Scholar] [CrossRef] [PubMed]
- Hermens, H.J.; Freriks, B.; Disselhorst-Klug, C.; Rau, G. Development of recommendations for SEMG sensors and sensor placement procedures. J. Electromyogr. Kinesiol. 2000, 10, 361–374. [Google Scholar] [CrossRef] [PubMed]
- Jácome, C.; Cruz, J.; Oliveira, A.; Marques, A. Validity, reliability, and ability to identify fall status of the berg balance scale, BESTest, mini-BESTest, and brief-BESTest in patients with COPD. Phys. Ther. 2016, 96, 1807–1815. [Google Scholar] [CrossRef]
- Albarrati, A.M.; Gale, N.S.; Munnery, M.M.; Reid, N.; Cockcroft, J.R.; Shale, D.J. The Timed Up and Go test predicts frailty in patients with COPD. npj Prim. Care Respir. Med. 2022, 32, 24. [Google Scholar] [CrossRef]
- Alberto, C.; Pereira, D.C.; Sato, T. New reference values for forced spirometry in white adults in Brazil. J. Bras. Pneumol. 2007, 33, 397–406. [Google Scholar]
- Charlson, M.; Szatrowski, T.P.; Peterson, J.; Gold, J. Validation of a combined comorbidity index. J. Clin. Epidemiol. 1994, 47, 1245–1251. [Google Scholar] [CrossRef]
- Schober, P.; Boer, C.; Schwarte, L.A. Correlation Coefficients: Appropriate Use and Interpretation. Anesth. Analg. 2018, 126, 1763–1768. [Google Scholar] [CrossRef]
- Park, J.K.; Deutz, N.E.P.; Cruthirds, C.L.; Kirschner, S.K.; Park, H.; Madigan, M.L.; Engelen, M.P.K.J. Risk Factors for Postural and Functional Balance Impairment in Patients with Chronic Obstructive Pulmonary Disease. J. Clin. Med. 2020, 9, 609. [Google Scholar] [CrossRef]
- Yohannes, A.M.; Raue, P.J.; Kanellopoulos, D.; McGovern, A.; Sirey, J.A.; Kiosses, D.N.; Banerjee, S.; Seirup, J.K.; Novitch, R.S.; Alexopoulos, G.S. Predictors of All-Cause Mortality in Patients With Severe COPD and Major Depression Admitted to a Rehabilitation Hospital. Chest 2016, 149, 467–473. [Google Scholar] [CrossRef]
- Yeung, S.S.Y.; Reijnierse, E.M.; Pham, V.K.; Trappenburg, M.C.; Lim, W.K.; Meskers, C.G.M.; Maier, A.B. Sarcopenia and its association with falls and fractures in older adults: A systematic review and meta-analysis. J. Cachexia Sarcopenia Muscle 2019, 10, 485–500. [Google Scholar] [CrossRef]
- Zhang, T.; Huo, Y.; Yin, W.; Xiang, J. Postural balance disorders in sarcopenia based on surface electromyography. Heliyon 2024, 10, e24116. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, A.L.; Killian, K.J.; Summers, E.; Jones, N.L. Muscle strength, symptom intensity, and exercise capacity in patients with cardiorespiratory disorders. Am. J. Respir. Crit. Care Med. 1995, 152, 2021–2031. [Google Scholar] [CrossRef] [PubMed]
- McCormick, R.; Vasilaki, A. Age-related changes in skeletal muscle: Changes to life-style as a therapy. Biogerontology 2018, 19, 519–536. [Google Scholar] [CrossRef] [PubMed]
- Sousa-Victor, P.; Gutarra, S.; García-Prat, L.; Rodriguez-Ubreva, J.; Ortet, L.; Ruiz-Bonilla, V.; Jardí, M.; Ballestar, E.; González, S.; Serrano, A.L.; et al. Geriatric muscle stem cells switch reversible quiescence into senescence. Nature 2014, 506, 316–321. [Google Scholar] [CrossRef]
- Heymsfield, S.B.; Gonzalez, M.C.; Lu, J.; Jia, G.; Zheng, J. Skeletal muscle mass and quality: Evolution of modern measurement concepts in the context of sarcopenia. Proc. Nutr. Soc. 2015, 74, 355–366. [Google Scholar] [CrossRef]
- McGregor, R.A.; Cameron-Smith, D.; Poppitt, S.D. It is not just muscle mass: A review of muscle quality, composition and metabolism during ageing as determinants of muscle function and mobility in later life. Longev. Health 2014, 3, 9. [Google Scholar] [CrossRef]
- Kiriya, Y.; Toshiaki, N.; Shibasaki, I.; Ogata, K.; Ogawa, H.; Takei, Y.; Tezuka, M.; Seki, M.; Kato, T.; Lefor, A.K.; et al. Sarcopenia assessed by the quantity and quality of skeletal muscle is a prognostic factor for patients undergoing cardiac surgery. Surg. Today 2020, 50, 895–904. [Google Scholar] [CrossRef]
- Zhang, Y.; Zou, L.; Chen, S.-T.; Bae, J.H.; Kim, D.Y.; Liu, X.; Song, W. Effects and Moderators of Exercise on Sarcopenic Components in Sarcopenic Elderly: A Systematic Review and Meta-Analysis. Front. Med. 2021, 8, 649748. [Google Scholar] [CrossRef]
- Nascimento, C.; Ingles, M.; Salvador-Pascual, A.; Cominetti, M.; Gomez-Cabrera, M.; Viña, J. Sarcopenia, frailty and their prevention by exercise. Free. Radic. Biol. Med. 2018, 132, 42–49. [Google Scholar] [CrossRef]
- Laidlaw, D.H.; Kornatz, K.W.; Keen, D.A.; Suzuki, S.; Enoka, R.M. Strength training improves the steadiness of slow lengthening contractions performed by old adults. J. Appl. Physiol. 1999, 87, 1786–1795. [Google Scholar] [CrossRef]
- Loughran, K.J.; Atkinson, G.; Beauchamp, M.K.; Dixon, J.; Martin, D.; Rahim, S.; Harrison, S.L. Balance impairment in individuals with COPD: A systematic review with meta-analysis. Thorax 2020, 75, 539–546. [Google Scholar] [CrossRef] [PubMed]
- van Bakel, S.I.; Gosker, H.R.; Langen, R.C.; Schols, A.M.W.J. Towards Personalized Management of Sarcopenia in COPD. Int. J. Chronic Obstr. Pulm. Dis. 2021, 16, 25–40. [Google Scholar] [CrossRef] [PubMed]
- Lisco, G.; Disoteo, O.E.; De Tullio, A.; De Geronimo, V.; Giagulli, V.A.; Monzani, F.; Jirillo, E.; Cozzi, R.; Guastamacchia, E.; De Pergola, G.; et al. Sarcopenia and Diabetes: A Detrimental Liaison of Advancing Age. Nutrients 2023, 16, 63. [Google Scholar] [CrossRef]
- Hafner, T.; Marolt, T.P.; Šelb, J.; Grošelj, A.; Kosten, T.; Simonič, A.; Košnik, M.; Korošec, P. Predictors of Success of Inpatient Pulmonary Rehabilitation Program in COPD Patients. Int. J. Chronic Obstr. Pulm. Dis. 2023, 18, 2483–2495. [Google Scholar] [CrossRef]
- Kim, S.H.; Hong, C.H.; Shin, M.-J.; Kim, K.U.; Park, T.S.; Park, J.Y.; Shin, Y.B. Prevalence and clinical characteristics of Sarcopenia in older adult patients with stable chronic obstructive pulmonary disease: A cross-sectional and follow-up study. BMC Pulm. Med. 2024, 24, 219. [Google Scholar] [CrossRef]
- Brauwers, B.; Machado, F.V.C.; Beijers, R.J.H.C.G.; Spruit, M.A.; Franssen, F.M.E. Combined Exercise Training and Nutritional Interventions or Pharmacological Treatments to Improve Exercise Capacity and Body Composition in Chronic Obstructive Pulmonary Disease: A Narrative Review. Nutrients 2023, 15, 5136. [Google Scholar] [CrossRef]
- Chuatrakoon, B.; Uthaikhup, S.; Ngai, S.P.; Liwsrisakun, C.; Pothirat, C.; Sungkarat, S. The effectiveness of home-based balance and pulmonary rehabilitation program in individuals with chronic obstructive pulmonary disease: A randomized controlled trial. Eur. J. Phys. Rehabil. Med. 2022, 58, 478–486. [Google Scholar] [CrossRef]
- Mkacher, W.; Mekki, M.; Chaieb, F.; Tabka, Z.; Trabelsi, Y. Balance Training in Pulmonary Rehabilitation: Effects on Psychosocial Outcomes. J. Cardiopulm. Rehabil. Prev. 2015, 35, 278–285. [Google Scholar] [CrossRef]
- Beauchamp, M.K.; Janaudis-Ferreira, T.; Parreira, V.; Romano, J.M.; Woon, L.; Goldstein, R.S.; Brooks, D. A randomized controlled trial of balance training during pulmonary rehabilitation for individuals with COPD. Chest 2013, 144, 1803–1810. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Sarcopenic (n = 13) | Non-Sarcopenic (n = 22) | p | |
|---|---|---|---|
| Anthropometric data | |||
| Age (years) | 71 ± 7 | 70 ± 5 | 0.3 |
| Female, n (%) | 5 (38%) | 7 (32%) | 0.93 |
| BMI (kg/m2) | 20.3 ± 3.7 | 28.4 ± 3.6 | 0.001 * |
| FFMI (kg/m2) | 13.5 ± 5.7 | 17.6 ± 1.8 | 0.01 * |
| SMI (kg/m2) | 7.3 ± 1.4 | 10 ± 1.8 | 0.004 * |
| FMI (kg/m2) | 9.1 ± 4.5 | 11 ± 2.5 | 0.15 |
| Abdominal girth | 89 ± 9 | 102.6 ± 10.9 | 0.006 * |
| Pulmonary Function | |||
| FVC (L) | 2.7 ± 0.6 | 2.8 ± 0.8 | 0.8 |
| FVC (%pred) | 88 ± 15 | 80 ± 18 | 0.3 |
| FEV1 (L) | 1.2 ± 0.4 | 1.4 ± 0.5 | 0.4 |
| FEV1 (%pred) | 47 ± 10 | 49 ± 14.2 | 0.5 |
| FEV1/FVC (%) | 43 ± 9 | 49 ± 9 | 0.06 |
| Comorbidities | |||
| ACCI (score) | 4.9 ± 1.2 | 5 ± 1.3 | 0.89 |
| Muscle Force | |||
| HGS (kg) | 19.8 ± 5.9 | 24.5 ± 7.4 | 0.001 * |
| Gait Speed | |||
| 4MGS (m/s) | 1.04 ± 0.24 | 1.2 ± 0.11 | 0.37 |
| Functional Balance | |||
| Brief-BESTest (score) | 15 ± 2 | 18 ± 3 | 0.003 * |
| Dynamic Balance | |||
| TUG (sec) | 8.3 ± 1.3 | 6.9 ± 1.3 | 0.038 * |
| Variables | Sarcopenic (n = 13) | Non-Sarcopenic (n = 22) | p |
|---|---|---|---|
| Bipedal with eyes opened | |||
| COP-a (cm2) | 2.4 ± 2 | 1.3 ± 0.5 | 0.06 |
| Vel-AP (cm/s) | 2.7 ± 0.7 | 1.9 ± 0.6 | 0.001 * |
| Vel-ML (cm/s) | 2.7 ± 0.4 | 1.9 ± 0.6 | 0.003 * |
| Amp-AP (cm) | 1.5 ± 0.4 | 1.5 ± 0.5 | 0.9 |
| Amp-ML (cm) | 2.9 ± 1.5 | 2.1 ± 0.6 | 0.02 * |
| Bipedal with eyes closed | |||
| COP-a (cm2) | 4 ± 5 | 1.5 ± 0.6 | 0.1 |
| Vel-AP (cm/s) | 2.8 ± 0.7 | 3.8 ± 4.5 | 0.6 |
| Vel-ML (cm/s) | 2.9 ± 0.6 | 2.3 ± 0.9 | 0.007 * |
| Amp-AP (cm) | 2 ± 0.9 | 1.6 ± 0.5 | 0.17 |
| Amp-ML (cm) | 3.6 ± 2 | 2.4 ± 0.7 | 0.022 * |
| One-legged stance | |||
| COP-a (cm2) | 15 [10–16.8] | 8.9 [7–12.9] † | 0.20 |
| Vel-AP (cm/s) | 6.7 ± 1.6 | 5.6 ± 1.6 † | 0.27 |
| Vel-ML (cm/s) | 6.09 ± 1.7 | 5.4 ± 1.7 † | 0.38 |
| Amp-AP (cm) | 4 ± 0.6 | 4.7 ± 1.1 † | 0.9 |
| Amp-ML (cm) | 4.9 ± 1 | 5.3 ± 1.2 † | 0.5 |
| Bipedal on unstable surface | |||
| COP-a (cm2) | 12.6 ± 2.5 | 3.9 ± 1.78 | 0.01 * |
| Vel-AP (cm/s) | 3.2 [3–3.6] | 2.2 [1.7–3] | 0.035 * |
| Vel-ML (cm/s) | 3.5 [3.1–3.5] | 2.2 [2–2.4] | 0.039 * |
| Amp-AP (cm) | 4 ± 1.4 | 2.7 ± 0.7 | 0.003 * |
| Amp-ML (cm) | 5.13 ± 2.1 | 3.2 ± 0.6 | 0.001 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Published by MDPI on behalf of the Polish Respiratory Society. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sepúlveda-Loyola, W.; Álvarez-Bustos, A.; Valenzuela-Fuenzalida, J.J.; Ordinola Ramírez, C.M.; Saldías Solis, C.; Probst, V.S. Are There Differences in Postural Control and Muscular Activity in Individuals with COPD and with and Without Sarcopenia? Adv. Respir. Med. 2025, 93, 5. https://doi.org/10.3390/arm93010005
Sepúlveda-Loyola W, Álvarez-Bustos A, Valenzuela-Fuenzalida JJ, Ordinola Ramírez CM, Saldías Solis C, Probst VS. Are There Differences in Postural Control and Muscular Activity in Individuals with COPD and with and Without Sarcopenia? Advances in Respiratory Medicine. 2025; 93(1):5. https://doi.org/10.3390/arm93010005
Chicago/Turabian StyleSepúlveda-Loyola, Walter, Alejandro Álvarez-Bustos, Juan José Valenzuela-Fuenzalida, Carla María Ordinola Ramírez, Carol Saldías Solis, and Vanessa Suziane Probst. 2025. "Are There Differences in Postural Control and Muscular Activity in Individuals with COPD and with and Without Sarcopenia?" Advances in Respiratory Medicine 93, no. 1: 5. https://doi.org/10.3390/arm93010005
APA StyleSepúlveda-Loyola, W., Álvarez-Bustos, A., Valenzuela-Fuenzalida, J. J., Ordinola Ramírez, C. M., Saldías Solis, C., & Probst, V. S. (2025). Are There Differences in Postural Control and Muscular Activity in Individuals with COPD and with and Without Sarcopenia? Advances in Respiratory Medicine, 93(1), 5. https://doi.org/10.3390/arm93010005