Administering Nitric Oxide (NO) with High Flow Nasal Cannulas: A Simple Method


{kind=link}
{kind=link}
Abstract
Highlights
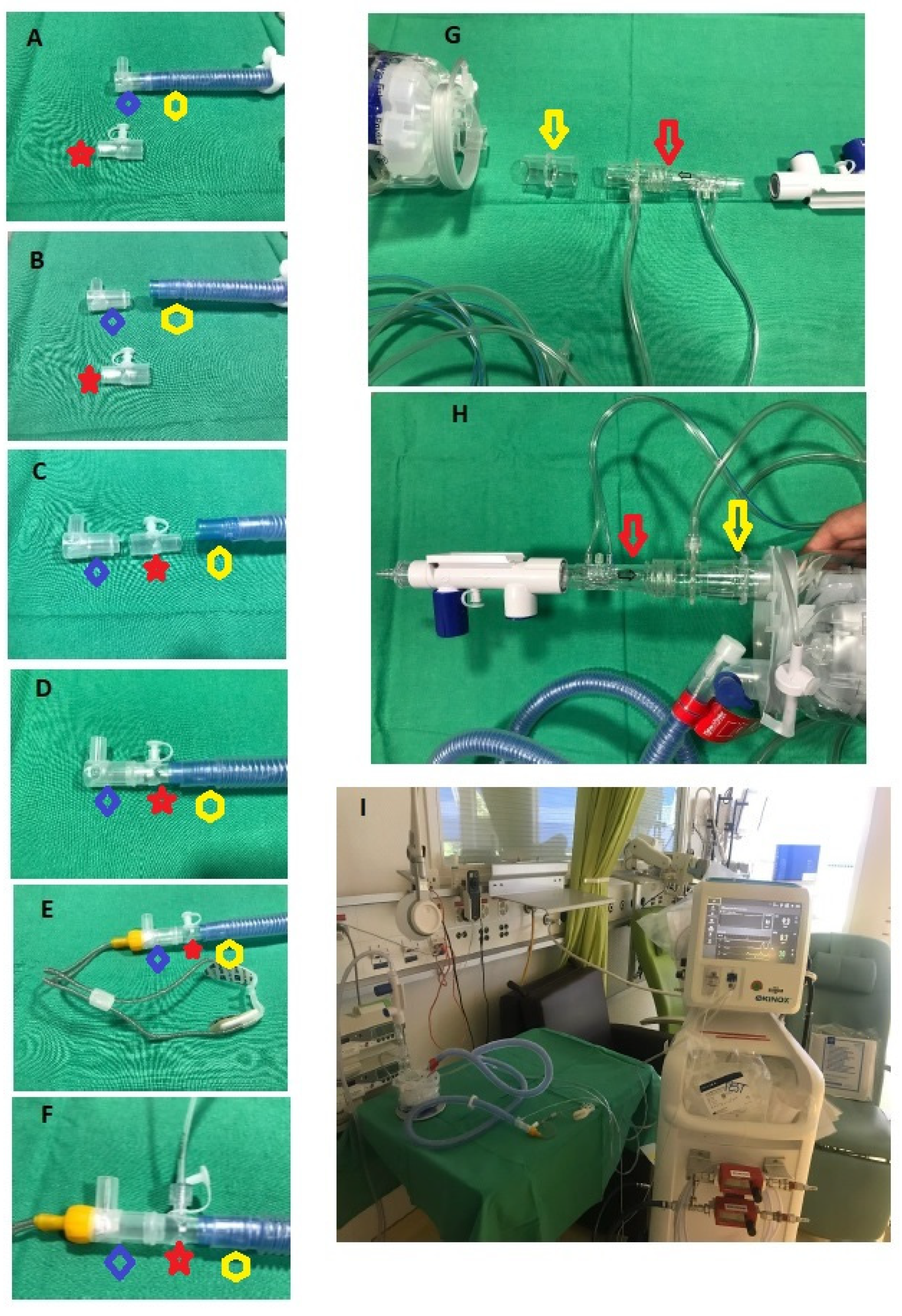
- A simple method to administer Nitric Oxide using the SoKINOX® (Air Liquide, Paris, France) Nitric Oxide delivery device with HFNC devices.
- It is suitable for both adult and pediatric circuits (Optiflow®, Fisher & Paykel Healthcare, Auckland, New Zealand).
Abstract
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Yu, B.; Ichinose, F.; Bloch, D.B.; Zapol, W.M. Inhaled nitric oxide. Br. J. Pharmacol. 2019, 176, 246–255. [Google Scholar] [CrossRef] [PubMed]
- Barst, R.J.; Channick, R.; Ivy, D.; Goldstein, B. Clinical perspectives with long-term pulsed inhaled nitric oxide for the treatment of pulmonary arterial hypertension. Pulm. Circ. 2012, 2, 139–147. [Google Scholar] [CrossRef] [PubMed]
- Kamenshchikov, N.O.; Berra, L.; Carroll, R.W. Therapeutic Effects of Inhaled Nitric Oxide Therapy in COVID-19 Patients. Biomedicines 2022, 10, 369. [Google Scholar] [CrossRef] [PubMed]
- Kinsella, J.P.; Parker, T.A.; Ivy, D.D.; Abman, S.H. Noninvasive delivery of inhaled nitric oxide therapy for late pulmonary hypertension in newborn infants with congenital diaphragmatic hernia. J. Pediatr. 2003, 142, 397–401. [Google Scholar] [CrossRef] [PubMed]
- Tominaga, Y.; Iwai, S.; Yamauchi, S.; Kyogoku, M.; Kugo, Y.; Hasegawa, M.; Kayatani, F.; Takahashi, K.; Aoki, H.; Takeuchi, M.; et al. Post-Extubation Inhaled Nitric Oxide Therapy via High-Flow Nasal Cannula After Fontan Procedure. Pediatr. Cardiol. 2019, 40, 1064–1071. [Google Scholar] [CrossRef] [PubMed]
- Gupta, S.; Tang, R.; Al-Hesayen, A. Inhaled nitric oxide improves the hepatopulmonary syndrome: A physiologic analysis. Thorax 2021, 76, 1142–1145. [Google Scholar] [CrossRef] [PubMed]
- Hamada, S.; Okamoto, T.; Ogawa, E.; Sonoda, M.; Okajima, H.; Hirai, T.; Handa, T.; Uemoto, S.; Chin, K. High-flow nasal cannula oxygen therapy: Alternative respiratory therapy for severe post-transplant hypoxemia in children with hepatopulmonary syndrome. Pediatr. Transplant 2020, 24, e13813. [Google Scholar] [CrossRef] [PubMed]
- Chandel, A.; Patolia, S.; Ahmad, K.; Aryal, S.; Brown, A.W.; Sahjwani, D.; Khangoora, V.; Shlobin, O.A.; Cameron, P.C.; Singhal, A.; et al. Inhaled Nitric Oxide via High-Flow Nasal Cannula in Patients with Acute Respiratory Failure Related to COVID-19. Clin. Med. Insights Circ. Respir. Pulm.Med. 2021, 15, 11795484211047065. [Google Scholar] [CrossRef] [PubMed]
- Gianni, S.; Carroll, R.W.; Kacmarek, R.M.; Berra, L. Inhaled Nitric Oxide Delivery Systems for Mechanically Ventilated and Nonintubated Patients: A Review. Respir. Care 2021, 66, 1021–1028. [Google Scholar] [CrossRef] [PubMed]
- Oczkowski, S.; Ergan, B.; Bos, L.; Chatwin, M.; Ferrer, M.; Gregoretti, C.; Heunks, L.; Frat, J.P.; Longhini, F.; Nava, S.; et al. ERS clinical practice guidelines: High-flow nasal cannula in acute respiratory failure. Eur. Respir. J. 2022, 59, 2101574. [Google Scholar] [CrossRef] [PubMed]
- Rochwerg, B.; Einav, S.; Chaudhuri, D.; Mancebo, J.; Mauri, T.; Helviz, Y.; Goligher, E.C.; Jaber, S.; Ricard, J.D.; Rittayamai, N.; et al. The role for high flow nasal cannula as a respiratory support strategy in adults: A clinical practice guideline. Intensive Care Med. 2020, 46, 2226–2237. [Google Scholar] [CrossRef] [PubMed]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cousin, V.L.; Joye, R.; Polito, A. Administering Nitric Oxide (NO) with High Flow Nasal Cannulas: A Simple Method. Adv. Respir. Med. 2024, 92, 92-95. https://doi.org/10.3390/arm92010012
Cousin VL, Joye R, Polito A. Administering Nitric Oxide (NO) with High Flow Nasal Cannulas: A Simple Method. Advances in Respiratory Medicine. 2024; 92(1):92-95. https://doi.org/10.3390/arm92010012
Chicago/Turabian StyleCousin, Vladimir L., Raphael Joye, and Angelo Polito. 2024. "Administering Nitric Oxide (NO) with High Flow Nasal Cannulas: A Simple Method" Advances in Respiratory Medicine 92, no. 1: 92-95. https://doi.org/10.3390/arm92010012
APA StyleCousin, V. L., Joye, R., & Polito, A. (2024). Administering Nitric Oxide (NO) with High Flow Nasal Cannulas: A Simple Method. Advances in Respiratory Medicine, 92(1), 92-95. https://doi.org/10.3390/arm92010012