
Testing Alpha-1 Antitrypsin Deficiency in Black Populations




Abstract
:Highlights
- Alpha-1 antitrypsin deficiency is extensively studied in populations of European ancestry but other ethnic populations also carry SERPINA1 mutations that may be harmful to these populations.
- The majority of studies undertaken in non-European populations screen for SERPINA1 mutations in small subject numbers and not from the general population.
- Insufficient alpha-1 antitrypsin deficiency testing is performed in Black populations that already experience poor health outcomes.
- Diagnosis of severe SERPINA1 mutations and counseling assists patients in their health education and a diagnosis of alpha-1 antitrypsin deficiency is a stronger motivator to quit smoking, improves the frequency of regular health checks, and lung and liver scans in patients.
Abstract
1. Introduction
2. AATD: A Historical and Biological Perspective
3. AATD Mutations
Regulation of the SERPINA1 Gene
4. Health Outcomes in Black Populations
AATD Prevalence in Black Populations
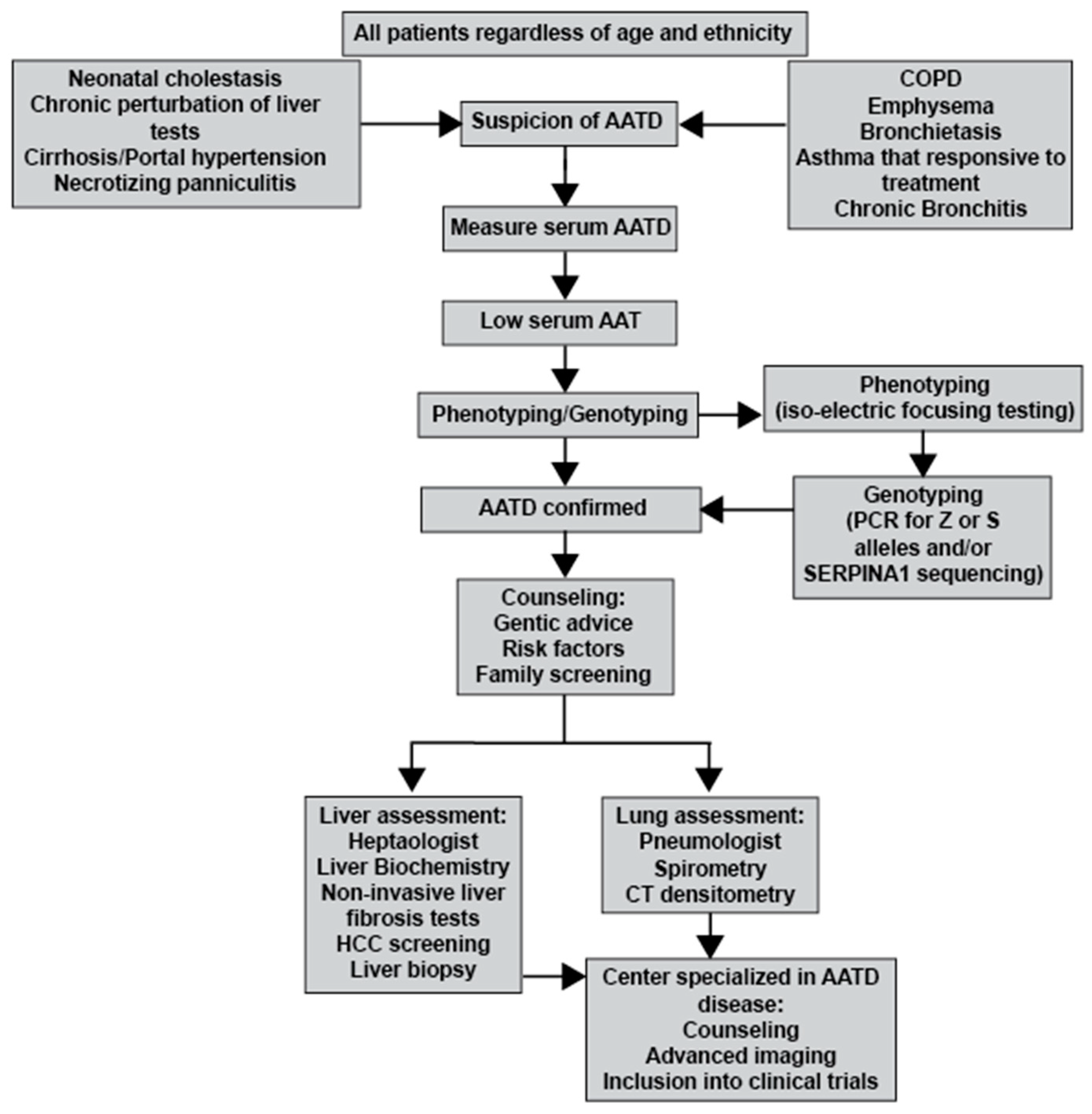
5. Screening and Diagnosis of AATD
Clinical Implications of Low Screening Rates
6. Benefits of Diagnosing AATD
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Cunningham, T.J.; Croft, J.B.; Liu, Y.; Lu, H.; Eke, P.I.; Giles, W.H. Vital Signs: Racial Disparities in Age-Specific Mortality Among Blacks or African Americans—United States, 1999–2015. MMWR Morb. Mortal. Wkly. Rep. 2017, 66, 444–456. [Google Scholar] [CrossRef] [PubMed]
- Williams, D.R. Miles to go before we sleep: Racial inequities in health. J. Health Soc. Behav. 2012, 53, 279–295. [Google Scholar] [CrossRef] [PubMed]
- Azar, K.M.J.; Shen, Z.; Romanelli, R.J.; Lockhart, S.H.; Smits, K.; Robinson, S.; Brown, S.; Pressman, A.R. Disparities in Outcomes Among COVID-19 Patients in A Large Health Care System in California. Health Aff. 2020, 39, 1253–1262. [Google Scholar] [CrossRef] [PubMed]
- Ghosh, A.J.; Hobbs, B.D.; Moll, M.; Saferali, A.; Boueiz, A.; Yun, J.H.; Sciurba, F.; Barwick, L.; Limper, A.H.; Flaherty, K.; et al. Alpha-1 Antitrypsin MZ Heterozygosity Is an Endotype of Chronic Obstructive Pulmonary Disease. Am. J. Respir. Crit. Care Med. 2022, 205, 313–323. [Google Scholar] [CrossRef] [PubMed]
- Palomino, L.; Gaffo, A.; Sun, D.; Sattui, S.E. Clinical Features of ANCA-Associated Vasculitis in African American Patients in the United States: A Single-Center Medical Records Review Study. J. Clin. Rheumatol. 2022, 28, 212–216. [Google Scholar] [CrossRef] [PubMed]
- Mamary, A.J.; Stewart, J.I.; Kinney, G.L.; Hokanson, J.E.; Shenoy, K.; Dransfield, M.T.; Foreman, M.G.; Vance, G.B.; Criner, G.J.; Investigators, C.O. Race and Gender Disparities are Evident in COPD Underdiagnoses Across all Severities of Measured Airflow Obstruction. Chronic Obstr. Pulm. Dis. 2018, 5, 177–184. [Google Scholar] [CrossRef] [PubMed]
- American Thoracic, S.; European Respiratory, S. American Thoracic Society/European Respiratory Society statement: Standards for the diagnosis and management of individuals with alpha-1 antitrypsin deficiency. Am. J. Respir. Crit. Care Med. 2003, 168, 818–900. [Google Scholar] [CrossRef]
- Laurell, C.B.; Eriksson, S. Hypo-Alpha-1-Antitrypsinemia. Verh. Dtsch. Ges. Inn. Med. 1964, 70, 537–539. [Google Scholar]
- McElvaney, N.G.; Stoller, J.K.; Buist, A.S.; Prakash, U.B.; Brantly, M.L.; Schluchter, M.D.; Crystal, R.D. Baseline characteristics of enrollees in the National Heart, Lung and Blood Institute Registry of alpha 1-antitrypsin deficiency. Alpha 1-Antitrypsin Deficiency Registry Study Group. Chest 1997, 111, 394–403. [Google Scholar] [CrossRef]
- Strange, C. Alpha-1 Antitrypsin Deficiency Associated COPD. Clin. Chest Med. 2020, 41, 339–345. [Google Scholar] [CrossRef]
- Bernspang, E.; Sveger, T.; Piitulainen, E. Respiratory symptoms and lung function in 30-year-old individuals with alpha-1-antitrypsin deficiency. Respir. Med. 2007, 101, 1971–1976. [Google Scholar] [CrossRef]
- Parr, D.G.; Guest, P.G.; Reynolds, J.H.; Dowson, L.J.; Stockley, R.A. Prevalence and impact of bronchiectasis in alpha1-antitrypsin deficiency. Am. J. Respir. Crit. Care Med. 2007, 176, 1215–1221. [Google Scholar] [CrossRef]
- Adair-Kirk, T.L.; Senior, R.M. Fragments of extracellular matrix as mediators of inflammation. Int. J. Biochem. Cell Biol. 2008, 40, 1101–1110. [Google Scholar] [CrossRef]
- Lascano, J.E.; Campos, M.A. The important role of primary care providers in the detection of alpha-1 antitrypsin deficiency. Postgrad. Med. 2017, 129, 889–895. [Google Scholar] [CrossRef]
- Molloy, K.; Hersh, C.P.; Morris, V.B.; Carroll, T.P.; O’Connor, C.A.; Lasky-Su, J.A.; Greene, C.M.; O’Neill, S.J.; Silverman, E.K.; McElvaney, N.G. Clarification of the risk of chronic obstructive pulmonary disease in alpha1-antitrypsin deficiency PiMZ heterozygotes. Am. J. Respir. Crit. Care Med. 2014, 189, 419–427. [Google Scholar] [CrossRef] [PubMed]
- Foreman, M.G.; Wilson, C.; DeMeo, D.L.; Hersh, C.P.; Beaty, T.H.; Cho, M.H.; Ziniti, J.; Curran-Everett, D.; Criner, G.; Hokanson, J.E.; et al. Alpha-1 Antitrypsin PiMZ Genotype Is Associated with Chronic Obstructive Pulmonary Disease in Two Racial Groups. Ann. Am. Thorac. Soc. 2017, 14, 1280–1287. [Google Scholar] [CrossRef] [PubMed]
- Ortega, V.E.; Li, X.; O’Neal, W.K.; Lackey, L.; Ampleford, E.; Hawkins, G.A.; Grayeski, P.J.; Laederach, A.; Barjaktarevic, I.; Barr, R.G.; et al. The Effects of Rare SERPINA1 Variants on Lung Function and Emphysema in SPIROMICS. Am. J. Respir. Crit. Care Med. 2020, 201, 540–554. [Google Scholar] [CrossRef] [PubMed]
- Blanco, I.; Bueno, P.; Diego, I.; Perez-Holanda, S.; Casas-Maldonado, F.; Esquinas, C.; Miravitlles, M. Alpha-1 antitrypsin Pi*Z gene frequency and Pi*ZZ genotype numbers worldwide: An update. Int. J. Chron. Obstruct Pulmon Dis. 2017, 12, 561–569. [Google Scholar] [CrossRef] [PubMed]
- Association, A.L. COPD Prevalence. Available online: https://www.lung.org/research/trends-in-lung-disease/copd-trends-brief/copd-prevalence (accessed on 9 September 2023).
- World Health Organization. Chronic Obstructive Pulmonary Disease (COPD). Available online: https://www.who.int/data/global-health-estimates (accessed on 9 September 2023).
- Ejike, C.O.; Dransfield, M.T.; Hansel, N.N.; Putcha, N.; Raju, S.; Martinez, C.H.; Han, M.K. Chronic Obstructive Pulmonary Disease in America’s Black Population. Am. J. Respir. Crit. Care Med. 2019, 200, 423–430. [Google Scholar] [CrossRef] [PubMed]
- Tan, W.C.; Sin, D.D.; Bourbeau, J.; Hernandez, P.; Chapman, K.R.; Cowie, R.; FitzGerald, J.M.; Marciniuk, D.D.; Maltais, F.; Buist, A.S.; et al. Characteristics of COPD in never-smokers and ever-smokers in the general population: Results from the CanCOLD study. Thorax 2015, 70, 822–829. [Google Scholar] [CrossRef]
- Riley, L.; Sriram, A.; Brantly, M.; Lascano, J. Testing Patterns and Disparities for Alpha-1 Antitrypsin Deficiency. Am. J. Med. 2023, 136, 1011–1017. [Google Scholar] [CrossRef] [PubMed]
- Franciosi, A.N.; Hobbs, B.D.; McElvaney, O.J.; Molloy, K.; Hersh, C.; Clarke, L.; Gunaratnam, C.; Silverman, E.K.; Carroll, T.P.; McElvaney, N.G. Clarifying the Risk of Lung Disease in SZ Alpha-1 Antitrypsin Deficiency. Am. J. Respir. Crit. Care Med. 2020, 202, 73–82. [Google Scholar] [CrossRef] [PubMed]
- Hernandez-Perez, J.M.; Ramos-Diaz, R.; Vaquerizo-Pollino, C.; Perez, J.A. Frequency of alleles and genotypes associated with alpha-1 antitrypsin deficiency in clinical and general populations: Revelations about underdiagnosis. Pulmonology 2022, 29, 214–220. [Google Scholar] [CrossRef] [PubMed]
- Carroll, T.P.; O’Connor, C.A.; Floyd, O.; McPartlin, J.; Kelleher, D.P.; O’Brien, G.; Dimitrov, B.D.; Morris, V.B.; Taggart, C.C.; McElvaney, N.G. The prevalence of alpha-1 antitrypsin deficiency in Ireland. Respir. Res. 2011, 12, 91. [Google Scholar] [CrossRef] [PubMed]
- Ashenhurst, J.R.; Nhan, H.; Shelton, J.F.; Wu, S.; Tung, J.Y.; Elson, S.L.; Stoller, J.K.; 23andMe Research Team. Prevalence of Alpha-1 Antitrypsin Deficiency, Self-Reported Behavior Change, and Health Care Engagement Among Direct-to-Consumer Recipients of a Personalized Genetic Risk Report. Chest 2022, 161, 373–381. [Google Scholar] [CrossRef] [PubMed]
- The Genome Aggregation Database (gnomAD). Available online: https://gnomad.broadinstitute.org/ (accessed on 12 August 2023).
- Seixas, S.; Marques, P.I. Known Mutations at the Cause of Alpha-1 Antitrypsin Deficiency an Updated Overview of SERPINA1 Variation Spectrum. Appl. Clin. Genet. 2021, 14, 173–194. [Google Scholar] [CrossRef]
- Silva, D.; Oliveira, M.J.; Guimaraes, M.; Lima, R.; Gomes, S.; Seixas, S. Alpha-1-antitrypsin (SERPINA1) mutation spectrum: Three novel variants and haplotype characterization of rare deficiency alleles identified in Portugal. Respir. Med. 2016, 116, 8–18. [Google Scholar] [CrossRef]
- Giacopuzzi, E.; Laffranchi, M.; Berardelli, R.; Ravasio, V.; Ferrarotti, I.; Gooptu, B.; Borsani, G.; Fra, A. Real-world clinical applicability of pathogenicity predictors assessed on SERPINA1 mutations in alpha-1-antitrypsin deficiency. Hum. Mutat. 2018, 39, 1203–1213. [Google Scholar] [CrossRef]
- Gaillard, M.C.; Mahadeva, R.; Lomas, D.A. Identification of DNA polymorphisms associated with the V type alpha1-antitrypsin gene. Biochim. Biophys. Acta 1999, 1444, 166–170. [Google Scholar] [CrossRef]
- Laurell, C.B.; Eriksson, S. The electrophoretic alpha1-globulin pattern of serum in alpha1-antitrypsin deficiency. 1963. COPD: J. Chronic Obstr. Pulm. Dis. 2013, 10, 3–8. [Google Scholar] [CrossRef]
- Fagerhol, M.K.; Tenfjord, O.W. Serum Pi types in some European, American, Asian and African populations. Acta Pathol. Microbiol. Scand. 1968, 72, 601–608. [Google Scholar] [CrossRef] [PubMed]
- Curiel, D.T.; Holmes, M.D.; Okayama, H.; Brantly, M.L.; Vogelmeier, C.; Travis, W.D.; Stier, L.E.; Perks, W.H.; Crystal, R.G. Molecular basis of the liver and lung disease associated with the alpha 1-antitrypsin deficiency allele Mmalton. J. Biol. Chem. 1989, 264, 13938–13945. [Google Scholar] [CrossRef] [PubMed]
- Poller, W.; Merklein, F.; Schneider-Rasp, S.; Haack, A.; Fechner, H.; Wang, H.; Anagnostopoulos, I.; Weidinger, S. Molecular characterisation of the defective alpha 1-antitrypsin alleles PI Mwurzburg (Pro369Ser), Mheerlen (Pro369Leu), and Q0lisbon (Thr68Ile). Eur. J. Hum. Genet. 1999, 7, 321–331. [Google Scholar] [CrossRef] [PubMed]
- Lomas, D.A.; Finch, J.T.; Seyama, K.; Nukiwa, T.; Carrell, R.W. Alpha 1-antitrypsin Siiyama (Ser53-->Phe). Further evidence for intracellular loop-sheet polymerization. J. Biol. Chem. 1993, 268, 15333–15335. [Google Scholar] [CrossRef] [PubMed]
- Talamo, R.C.; Langley, C.E.; Reed, C.E.; Makino, S. α1-Antitrypsin deficiency: A variant with no detecTable α1-antitrypsin. Science 1973, 181, 70–71. [Google Scholar] [CrossRef] [PubMed]
- de Serres, F.J.; Blanco, I. Prevalence of alpha1-antitrypsin deficiency alleles PI*S and PI*Z worldwide and effective screening for each of the five phenotypic classes PI*MS, PI*MZ, PI*SS, PI*SZ, and PI*ZZ: A comprehensive review. Ther. Adv. Respir. Dis. 2012, 6, 277–295. [Google Scholar] [CrossRef] [PubMed]
- Qiu, W.; Baccarelli, A.; Carey, V.J.; Boutaoui, N.; Bacherman, H.; Klanderman, B.; Rennard, S.; Agusti, A.; Anderson, W.; Lomas, D.A.; et al. Variable DNA methylation is associated with chronic obstructive pulmonary disease and lung function. Am. J. Respir. Crit. Care Med. 2012, 185, 373–381. [Google Scholar] [CrossRef] [PubMed]
- Beckmeyer-Borowko, A.; Imboden, M.; Rezwan, F.I.; Wielscher, M.; Amaral, A.F.S.; Jeong, A.; Schaffner, E.; Auvinen, J.; Sebert, S.; Karhunen, V.; et al. SERPINA1 methylation and lung function in tobacco-smoke exposed European children and adults: A meta-analysis of ALEC population-based cohorts. Respir. Res. 2018, 19, 156. [Google Scholar] [CrossRef]
- Rotondo, J.C.; Oton-Gonzalez, L.; Selvatici, R.; Rizzo, P.; Pavasini, R.; Campo, G.C.; Lanzillotti, C.; Mazziotta, C.; De Mattei, M.; Tognon, M.; et al. SERPINA1 Gene Promoter Is Differentially Methylated in Peripheral Blood Mononuclear Cells of Pregnant Women. Front. Cell Dev. Biol. 2020, 8, 550543. [Google Scholar] [CrossRef]
- Corley, M.; Solem, A.; Phillips, G.; Lackey, L.; Ziehr, B.; Vincent, H.A.; Mustoe, A.M.; Ramos, S.B.V.; Weeks, K.M.; Moorman, N.J.; et al. An RNA structure-mediated, posttranscriptional model of human alpha-1-antitrypsin expression. Proc. Natl. Acad. Sci. USA 2017, 114, E10244–E10253. [Google Scholar] [CrossRef]
- Lackey, L.; McArthur, E.; Laederach, A. Increased Transcript Complexity in Genes Associated with Chronic Obstructive Pulmonary Disease. PLoS ONE 2015, 10, e0140885. [Google Scholar] [CrossRef] [PubMed]
- Grayeski, P.J.; Weidmann, C.A.; Kumar, J.; Lackey, L.; Mustoe, A.M.; Busan, S.; Laederach, A.; Weeks, K.M. Global 5’-UTR RNA structure regulates translation of a SERPINA1 mRNA. Nucleic Acids Res. 2022, 50, 9689–9704. [Google Scholar] [CrossRef] [PubMed]
- Stoller, J.K. Alpha-1 antitrypsin deficiency: An underrecognized, treatable cause of COPD. Cleve Clin. J. Med. 2016, 83, 507–514. [Google Scholar] [CrossRef] [PubMed]
- Zhao, X.; Qiao, D.; Yang, C.; Kasela, S.; Kim, W.; Ma, Y.; Shrine, N.; Batini, C.; Sofer, T.; Taliun, S.A.G.; et al. Whole genome sequence analysis of pulmonary function and COPD in 19,996 multi-ethnic participants. Nat. Commun. 2020, 11, 5182. [Google Scholar] [CrossRef] [PubMed]
- de Serres, F.J. Worldwide racial and ethnic distribution of alpha1-antitrypsin deficiency: Summary of an analysis of published genetic epidemiologic surveys. Chest 2002, 122, 1818–1829. [Google Scholar] [CrossRef] [PubMed]
- Stoller, J.K.; Aboussouan, L.S. A review of alpha1-antitrypsin deficiency. Am. J. Respir. Crit. Care Med. 2012, 185, 246–259. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Gonzalez, C.; Blanco, I.; Diego, I.; Bueno, P.; Miravitlles, M. Estimated Prevalence and Number of PiMZ Genotypes of Alpha-1 Antitrypsin in Seventy-Four Countries Worldwide. Int. J. Chron. Obstruct Pulmon Dis. 2021, 16, 2617–2630. [Google Scholar] [CrossRef]
- Chatila, W.M.; Hoffman, E.A.; Gaughan, J.; Robinswood, G.B.; Criner, G.J.; National Emphysema Treatment Trial Research, G. Advanced emphysema in African-American and white patients: Do differences exist? Chest 2006, 130, 108–118. [Google Scholar] [CrossRef]
- Silverman, E.K.; Miletich, J.P.; Pierce, J.A.; Sherman, L.A.; Endicott, S.K.; Broze, G.J., Jr.; Campbell, E.J. Alpha-1-antitrypsin deficiency. High prevalence in the St. Louis area determined by direct population screening. Am. Rev. Respir. Dis. 1989, 140, 961–966. [Google Scholar] [CrossRef]
- Banauch, G.I.; Brantly, M.; Izbicki, G.; Hall, C.; Shanske, A.; Chavko, R.; Santhyadka, G.; Christodoulou, V.; Weiden, M.D.; Prezant, D.J. Accelerated spirometric decline in New York City firefighters with alpha(1)-antitrypsin deficiency. Chest 2010, 138, 1116–1124. [Google Scholar] [CrossRef]
- Spinola, C.; Brehm, A.; Spinola, H. Alpha-1-antitrypsin deficiency in the Cape Verde islands (Northwest Africa): High prevalence in a sub-Saharan population. Respir. Med. 2010, 104, 1069–1072. [Google Scholar] [CrossRef] [PubMed]
- Miskoff, J.A.; Khan, B.; Chaudhri, M.; Phan, H.; Carson, M.P. Identifying Alpha-1 Antitrypsin Deficiency Based on Computed Tomography Evidence of Emphysema. Cureus 2019, 11, e3971. [Google Scholar] [CrossRef] [PubMed]
- Denden, S.; Zorzetto, M.; Amri, F.; Knani, J.; Ottaviani, S.; Scabini, R.; Gorrini, M.; Ferrarotti, I.; Campo, I.; Chibani, J.B.; et al. Screening for Alpha 1 antitrypsin deficiency in Tunisian subjects with obstructive lung disease: A feasibility report. Orphanet J. Rare Dis. 2009, 4, 12. [Google Scholar] [CrossRef] [PubMed]
- Webb, D.R.; Hyde, R.W.; Schwartz, R.H.; Hall, W.J.; Condemi, J.J.; Townes, P.L. Serum alpha 1-antitrypsin variants. Prevalence and clinical spirometry. Am. Rev. Respir. Dis. 1973, 108, 918–925. [Google Scholar] [CrossRef] [PubMed]
- Young, R.C., Jr.; Headings, V.E.; Henderson, A.L.; Bose, S.; Hackney, R.L., Jr. Protease inhibitor profile of black Americans with and without chronic cardiopulmonary disease. J. Natl. Med. Assoc. 1978, 70, 849–856. [Google Scholar] [PubMed]
- Pierce, J.A.; Eradio, B.; Dew, T.A. Antitrypsin phenotypes in St. Louis. J. Am. Med. Assoc. 1975, 231, 609–612. [Google Scholar] [CrossRef]
- Massi, G.; Vecchio, F.M. Alpha-1-antitrypsin phenotypes in a group of newborn infants in Somalia. Hum. Genet. 1977, 38, 265–269. [Google Scholar] [CrossRef]
- Vandeville, D.; Martin, J.P.; Ropartz, C. Alpha 1-antitrypsin polymorphism of a Bantu population: Description of a new allele PiL. Humangenetik 1974, 21, 33–38. [Google Scholar] [CrossRef]
- Welch, S.G.; McGregor, I.A.; Williams, K. Alpha 1-antitrypsin (pi) phenotypes in a village population from The Gambia, West Africa. Evidence of a new variant occurring at a polymorphic frequency. Hum. Genet. 1980, 53, 233–235. [Google Scholar] [CrossRef]
- Pascali, V.L.; Ranalletta, D.; Spedini, G. Antitrypsin and Gc polymorphisms in some populations of Congo: An unusual, highly frequent mutant, PIS, in Bateke and Babenga. Ann. Hum. Biol. 1986, 13, 267–271. [Google Scholar] [CrossRef]
- Chaabani, H.; Martin, J.P.; Frants, R.R.; Lefranc, G. Genetic study of Tunisian Berbers. II. Alpha 1-antitrypsin (Pi) polymorphism: Report of a new allele (Pi S Berber). Exp. Clin. Immunogenet. 1984, 1, 19–24. [Google Scholar] [PubMed]
- Lieberman, J.; Gaidulis, L.; Roberts, L. Racial distribution of alpha1-antitrypsin variants among junior high school students. Am. Rev. Respir. Dis. 1976, 114, 1194–1198. [Google Scholar] [CrossRef]
- Brems, J.H.; Balasubramanian, A.; Psoter, K.J.; Shah, P.D.; Bush, E.; Merlo, C.A.; McCormack, M.C. Race-specific Interpretation of Spirometry: Impact on the Lung Allocation Score. Ann. Am. Thorac. Soc. 2023, 20, 1408–1415. [Google Scholar] [CrossRef] [PubMed]
- Ekstrom, M.; Mannino, D. Research race-specific reference values and lung function impairment, breathlessness and prognosis: Analysis of NHANES 2007–2012. Respir. Res. 2022, 23, 271. [Google Scholar] [CrossRef] [PubMed]
- Seaman, E.L.; Corcy, N.; Chang, J.T.; Chomenko, D.; Hartman, A.M.; Kittner, D.L.; Reyes-Guzman, C.M. Menthol Cigarette Smoking Trends among United States Adults, 2003–2019. Cancer Epidemiol. Biomark. Prev. 2022, 31, 1959–1965. [Google Scholar] [CrossRef] [PubMed]
- Foulds, J.; Hooper, M.W.; Pletcher, M.J.; Okuyemi, K.S. Do smokers of menthol cigarettes find it harder to quit smoking? Nicotine Tob. Res. 2010, 12, S102–S109. [Google Scholar] [CrossRef] [PubMed]
- Patrucco, F.; Venezia, L.; Gavelli, F.; Pellicano, R.; Solidoro, P. Alpha1-antitrypsin deficiency: What’s new after European Respiratory Society Statement. Panminerva Med. 2018, 60, 101–108. [Google Scholar] [CrossRef] [PubMed]
- Haillot, A.; Pelland, A.A.; Bosse, Y.; Carroll, T.P.; Maltais, F.; Dandurand, R.J. IntraIndividual Variability in Serum Alpha-1 Antitrypsin Levels. Chronic Obstr. Pulm. Dis. 2021, 8, 464–473. [Google Scholar] [CrossRef]
- Franciosi, A.N.; Carroll, T.P.; McElvaney, N.G. Pitfalls and caveats in alpha1-antitrypsin deficiency testing: A guide for clinicians. Lancet Respir. Med. 2019, 7, 1059–1067. [Google Scholar] [CrossRef]
- Belmonte, I.; Barrecheguren, M.; Lopez-Martinez, R.M.; Esquinas, C.; Rodriguez, E.; Miravitlles, M.; Rodriguez-Frias, F. Application of a diagnostic algorithm for the rare deficient variant Mmalton of alpha-1-antitrypsin deficiency: A new approach. Int. J. Chron. Obs. Pulmon Dis. 2016, 11, 2535–2541. [Google Scholar] [CrossRef]
- Papiris, S.A.; Veith, M.; Papaioannou, A.I.; Apollonatou, V.; Ferrarotti, I.; Ottaviani, S.; Tzouvelekis, A.; Tzilas, V.; Rovina, N.; Stratakos, G.; et al. Alpha1-antitrypsin deficiency in Greece: Focus on rare variants. Pulmonology, 2023; Epub ahead of print. [Google Scholar] [CrossRef]
- Kueppers, F.; Sanders, C. State-of-the-art testing for alpha-1 antitrypsin deficiency. Allergy Asthma Proc. 2017, 38, 108–114. [Google Scholar] [CrossRef] [PubMed]
- McShane, P.J.; Choate, R.; Johnson, M.; Maselli, D.J.; Winthrop, K.L.; Metersky, M.L.; Bronchiectasis and NTM Research Registry Investigators. Racial and ethnic differences in patients enrolled in the national bronchiectasis and nontuberculous mycobacteria research registry. Respir. Med. 2023, 209, 107167. [Google Scholar] [CrossRef] [PubMed]
- Tejwani, V.; Nowacki, A.S.; Fye, E.; Sanders, C.; Stoller, J.K. The Impact of Delayed Diagnosis of Alpha-1 Antitrypsin Deficiency: The Association Between Diagnostic Delay and Worsened Clinical Status. Respir. Care 2019, 64, 915–922. [Google Scholar] [CrossRef] [PubMed]
- Franciosi, A.N.; Alkhunaizi, M.A.; Woodsmith, A.; Aldaihani, L.; Alkandari, H.; Lee, S.E.; Fee, L.T.; McElvaney, N.G.; Carroll, T.P. Alpha-1 Antitrypsin Deficiency and Tobacco Smoking: Exploring Risk Factors and Smoking Cessation in a Registry Population. COPD: J. Chronic Obstr. Pulm. Dis. 2021, 18, 76–82. [Google Scholar] [CrossRef] [PubMed]
- Chapman, K.R.; Burdon, J.G.; Piitulainen, E.; Sandhaus, R.A.; Seersholm, N.; Stocks, J.M.; Stoel, B.C.; Huang, L.; Yao, Z.; Edelman, J.M.; et al. Intravenous augmentation treatment and lung density in severe alpha1 antitrypsin deficiency (RAPID): A randomised, double-blind, placebo-controlled trial. Lancet 2015, 386, 360–368. [Google Scholar] [CrossRef]
- McElvaney, O.J.; Carroll, T.P.; Franciosi, A.N.; Sweeney, J.; Hobbs, B.D.; Kowlessar, V.; Gunaratnam, C.; Reeves, E.P.; McElvaney, N.G. Consequences of Abrupt Cessation of Alpha1-Antitrypsin Replacement Therapy. N. Engl. J. Med. 2020, 382, 1478–1480. [Google Scholar] [CrossRef]
- Sieluk, J.; Levy, J.; Sandhaus, R.A.; Silverman, H.; Holm, K.E.; Mullins, C.D. Costs of Medical Care Among Augmentation Therapy Users and Non-Users with Alpha-1 Antitrypsin Deficiency in the United States. Chronic Obstr. Pulm. Dis. 2018, 6, 6–16. [Google Scholar] [CrossRef]


{kind=link}
| SERPINA1 Variant | Molecular Basis | SNP Number | Cellular Effect | Disease Association | Reference | Observed in Non-European Populations? |
|---|---|---|---|---|---|---|
| S | p.Glu264Val | rs17580 | Polymerization, impaired secretion, reduced antiprotease activity | Lung & liver if inherited with other severe AATD variant(s) (e.g., Z) | Lomas et al., 1999 [32] | Yes |
| Z | p.Glu342Lys | rs28929474 | Polymerization, impaired secretion, reduced antiprotease activity | Lung & liver | Laurell & Eriksson, 1963 [33] | Yes |
| I | p.Arg39Cys | rs28931570 | Polymerization, impaired secretion, reduced antiprotease activity | Lung & liver | Lomas et al., 1999 [32] | Yes |
| F | p.Arg223Cys | rs28929470 | Reduced antiprotease activity | Lung | Fagerhol & Tenfjord, 1968 [34] | Yes |
| Mmalton | p.Phe52del | rs775982338 | Polymerization, impaired secretion, reduced antiprotease activity | Lung and liver | Curiel et al., 1989 [35] | Yes |
| Mwurzburg | p.Pro369Ser | rs61761869 | Intracellular accumulation & polymerization | Lung and liver | Poller et al., 1999 [36] | Yes |
| Mheerlen | p.Pro369Leu | rs199422209 | Block in production | Lung | Poller et al., 1999 [36] | Yes |
| Siiyama | p.Ser53Phe | rs55819880 | Polymerization | Lung and liver | Lomas et al., 1993 [37] | Yes |
| Null (Q0) | Premature termination codon | N/A | Family of mutations that produce no detectable AAT | Lung | Talamo et al., 1973 [38] | Yes |
| Study | Location | Study Population Number (N) | AAT Genotype | |||||
|---|---|---|---|---|---|---|---|---|
| MM | MS | MZ | SS | SZ | ZZ | |||
| Spınola et al. [54] | Cape Verde Islands | 202 | 191 | 7 | 1 | 3 | 0 | 0 |
| Foreman et al. [16] | USA; COPDGene cohort a | 2803 | 2731 | 49 | 22 | 0 | 1 | 0 |
| Miskoff et al. [55] | Neptune Township, New Jersey, USA | 18 | 16 | 1 | 1 | 0 | 0 | 0 |
| Ashenhurst et al. [27] | 23andMe customers | 1443 | N/A | N/A | N/A | N/A | N/A | N/A |
| Ortega et al. [17] | USA; SPIROMICS cohort | 385 b | N/A | N/A | N/A | N/A | N/A | N/A |
| Denden et al. [56] | Tunisia; obstructive lung disease cohort | 120 | 119 | 0 | 1 | 0 | 0 | 0 |
| Webb et al. [57] | Rochester, Monroe County, NY, USA | 53 c | N/A | N/A | N/A | N/A | N/A | N/A |
| Young et al. [58] | Washington, DC, USA | 94 d | N/A | N/A | 2 | N/A | 1 | 1 |
| Pierce et al. [59] | St. Louis, MO, USA | 204 | 196 | 4 | 2 | N/A | N/A | N/A |
| Massi et al. [60] | Mogadishu, Somalia | 347 | 333 | 9 | 1 | 0 | 1 | 3 |
| Vandeville et al. [61] | Zaire | 132 e | 124 | 0 | 0 | 0 | 0 | 0 |
| Welch et al. [62] | Gambia, West Africa | 701 f | 700 | 0 | 0 | 0 | 0 | 0 |
| Pascali et al. [63] | Congo, West Africa | 278 | 243 | 35 | 0 | 0 | 0 | 0 |
| Chaabani et al. [64] | Tunisia | 310 | 260 | 50 | 0 | 0 | 0 | 0 |
| Giacopuzzi et al. [31] | Multiple public databases | 5203 g | N/A | 81 | 35 | N/A | 116 | N/A |
| Lieberman et al. [65] | High school students from Long Beach, CA, USA | 186 h | 182 | 3 | 0 | 0 | 0 | 0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lafortune, P.; Zahid, K.; Ploszaj, M.; Awadalla, E.; Carroll, T.P.; Geraghty, P. Testing Alpha-1 Antitrypsin Deficiency in Black Populations. Adv. Respir. Med. 2024, 92, 1-12. https://doi.org/10.3390/arm92010001
Lafortune P, Zahid K, Ploszaj M, Awadalla E, Carroll TP, Geraghty P. Testing Alpha-1 Antitrypsin Deficiency in Black Populations. Advances in Respiratory Medicine. 2024; 92(1):1-12. https://doi.org/10.3390/arm92010001
Chicago/Turabian StyleLafortune, Pascale, Kanza Zahid, Magdalena Ploszaj, Emilio Awadalla, Tomás P. Carroll, and Patrick Geraghty. 2024. "Testing Alpha-1 Antitrypsin Deficiency in Black Populations" Advances in Respiratory Medicine 92, no. 1: 1-12. https://doi.org/10.3390/arm92010001
APA StyleLafortune, P., Zahid, K., Ploszaj, M., Awadalla, E., Carroll, T. P., & Geraghty, P. (2024). Testing Alpha-1 Antitrypsin Deficiency in Black Populations. Advances in Respiratory Medicine, 92(1), 1-12. https://doi.org/10.3390/arm92010001