
Correlation between Cardiovascular Autonomic and Pulmonary Ventilation Functions in Myasthenia Gravis Patients

 , , ,
, , ,
Abstract
:Highlights
- A lower baroreflex sensitivity in the MG group was associated with worse clinical disease outcomes and reduced pulmonary function.
- Age, forced vital capacity, and total lung capacity could predict the heart rate response during deep breathing.
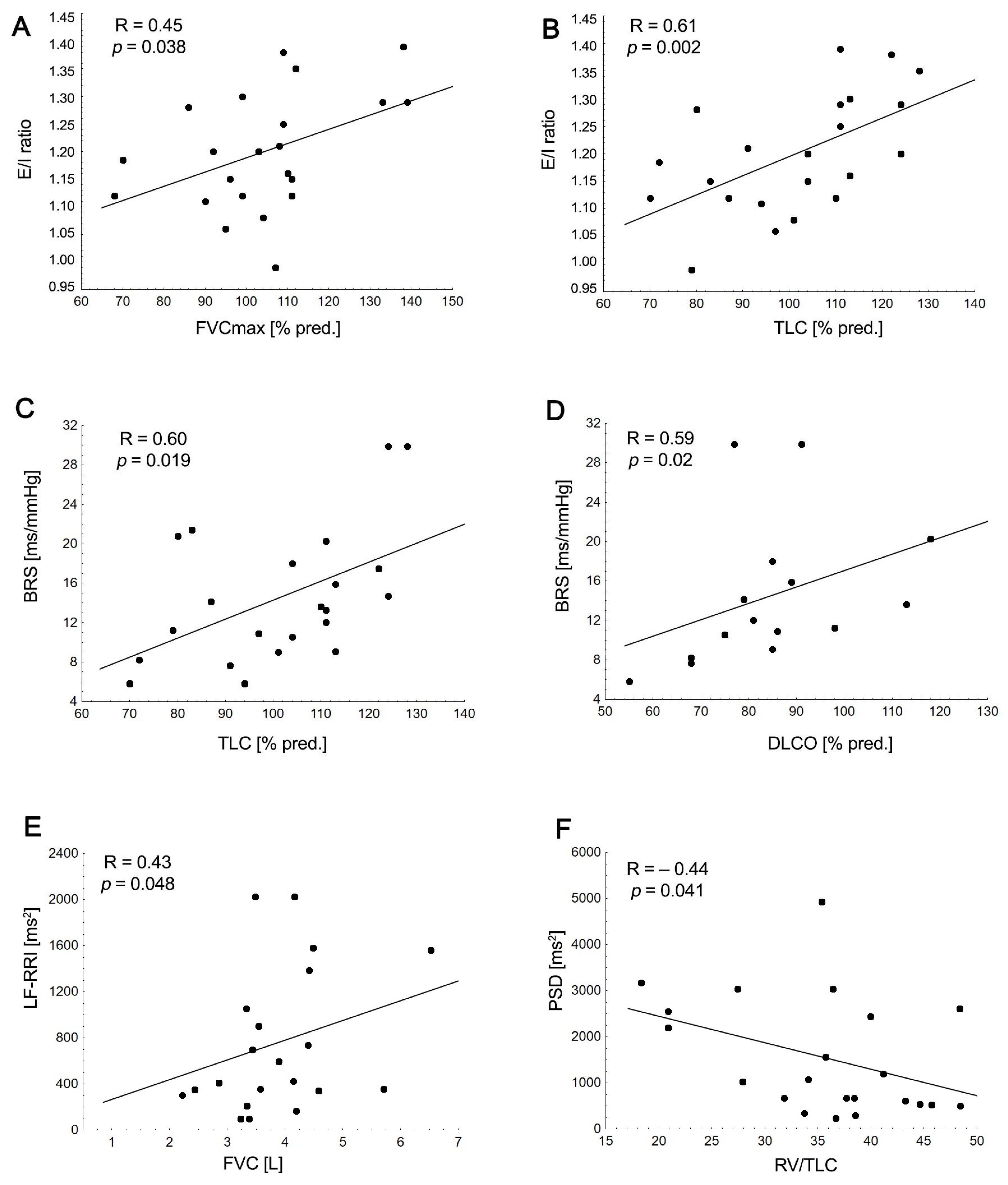
- There is a significant relationship between reduced pulmonary ventilation function or respiratory mechanics and cardiovascular autonomic parameters in MG patients.
- Future studies should prioritize investigating how respiratory and autonomic function testing interact, alongside exploring the impact of pulmonary rehabilitation.
Abstract
1. Introduction
2. Material and Methods
2.1. Pulmonary Function Tests (PFTs)
2.2. Cardiovascular Autonomic Testing
2.3. Statistical Analysis
3. Results
3.1. Demographic and Clinical Data
3.2. Pulmonary Function Tests: MG Patients vs. HCs
3.3. Autonomic Function
3.4. Relationship between Cardiovascular Autonomic, Pulmonary Function Parameters, and Clinical Disease Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gilhus, N.E.; Tzartos, S.; Evoli, A.; Palace, J.; Burns, T.M.; Verschuuren, J.J.G.M. Myasthenia gravis. Nat. Rev. Dis. Prim. 2019, 5, 30. [Google Scholar] [CrossRef] [PubMed]
- Di Stefano, V.; Tubiolo, C.; Gagliardo, A.; Presti, R.L.; Montana, M.; Todisco, M.; Lupica, A.; Caimi, G.; Tassorelli, C.; Fierro, B.; et al. Metalloproteinases and Tissue Inhibitors in Generalized Myasthenia Gravis. A Preliminary Study. Brain Sci. 2022, 12, 1439. [Google Scholar] [CrossRef] [PubMed]
- Gilhus, N.E. Myasthenia gravis, respiratory function, and respiratory tract disease. J. Neurol. 2023, 270, 3329–3340. [Google Scholar] [CrossRef] [PubMed]
- Lupica, A.; Di Stefano, V.; Iacono, S.; Pignolo, A.; Quartana, M.; Gagliardo, A.; Fierro, B.; Brighina, F. Impact of COVID-19 in AChR Myasthenia Gravis and the Safety of Vaccines: Data from an Italian Cohort. Neurol. Int. 2022, 14, 406–416. [Google Scholar] [CrossRef] [PubMed]
- Keenan, S.P.; Alexander, D.; Road, J.; Ryan, C.; Oger, J.; Wilcox, P. Ventilatory muscle strength and endurance in myasthenia gravis. Eur. Respir. J. 1995, 8, 1130–1135. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, E.F.; Nacif, S.R.; Urbano, J.J.; Silva, A.S.; Oliveira, C.S.; Perez, E.A.; Polaro, M.N.; Valerio, B.C.O.; Stirbulov, R.; Insalaco, G.; et al. Sleep, lung function, and quality of life in patients with myasthenia gravis: A cross-sectional study. Neuromuscul. Disord. 2017, 27, 120–127. [Google Scholar] [CrossRef] [PubMed]
- Jiao, P.; Wu, F.; Liu, Y.; Wu, J.; Sun, Y.; Tian, W.; Yu, H.; Huang, C.; Li, D.; Wu, Q.; et al. Analysis of influencing factors of postoperative myasthenic crisis in 564 patients with myasthenia gravis in a single center. Thorac. Cancer 2023, 14, 517–523. [Google Scholar] [CrossRef]
- Elsais, A.; Johansen, B.; Kerty, E. Airway limitation and exercise intolerance in well-regulated myasthenia gravis patients. Acta Neurol. Scand. 2010, 122, 12–17. [Google Scholar] [CrossRef]
- Calik-Kutukcu, E.; Salci, Y.; Karanfil, E.; Fil-Balkan, A.; Bekircan-Kurt, C.E.; Armutlu, K. Expiratory muscle strength as a pre-dictor of functional exercise capacity in generalized myasthenia gravis. Neurosciences 2019, 24, 95–100. [Google Scholar] [CrossRef]
- Huang, X.; Xu, M.; Wang, Y.; Zhang, Z.; Li, F.; Chen, X.; Zhang, Y. The systemic inflammation markers as possible indices for predicting respiratory failure and outcome in patients with myasthenia gravis. Ann. Clin. Transl. Neurol. 2023, 10, 98–110. [Google Scholar] [CrossRef]
- Pongratz, G.; Straub, R.H. The sympathetic nervous response in inflammation. Arthritis Res. Ther. 2014, 16, 504. [Google Scholar] [CrossRef]
- Shivamurthy, P.; Parker, M.W. Cardiac manifestations of myasthenia gravis: A systematic review. IJC Metab. Endocr. 2014, 5, 3–6. [Google Scholar] [CrossRef]
- Singh, N.; Moneghetti, K.J.; Christle, J.; Hadley, D.; Plews, D.; Froelicher, V. Heart Rate Variability: An Old Metric with New Meaning in the Era of using mHealth Technologies for Health and Exercise Training Guidance. Part One: Physiology and Methods. Arrhythm. Electrophysiol. Rev. 2018, 7, 193–198. [Google Scholar] [CrossRef] [PubMed]
- Narkiewicz, K.; van de Borne, P.; Montano, N.; Hering, D.; Kara, T.; Somers, V.K. Sympathetic neural outflow and chemoreflex sensitivity are related to spontaneous breathing rate in normal men. Hypertension 2006, 47, 51–55. [Google Scholar] [CrossRef] [PubMed]
- Narkiewicz, K.; Pesek, C.A.; van de Borne, P.J.H.; Kato, M.; Somers, V.K. Enhanced sympathetic and ventilatory responses to central chemoreflex activation in heart failure. Circulation 1999, 100, 262–267. [Google Scholar] [CrossRef] [PubMed]
- Nikolić, A.; Perić, S.; Nišić, T.; Popović, S.; Ilić, M.; Stojanović, V.R.; Lavrnić, D. The presence of dysautonomia in different subgroups of myasthenia gravis patients. J. Neurol. 2014, 261, 2119–2127. [Google Scholar] [CrossRef] [PubMed]
- Zawadka-Kunikowska, M.; Rzepiński, Ł.; Tafil-Klawe, M.; Klawe, J.J.; Zalewski, P.; Słomko, J. Association of Cardiac Autonomic Responses with Clinical Outcomes of Myasthenia Gravis: Short-Term Analysis of the Heart-Rate and Blood Pressure Variability. J. Clin. Med. 2022, 11, 3697. [Google Scholar] [CrossRef] [PubMed]
- Owe, J.F.; Davidsen, E.S.; Eide, G.E.; Gerdts, E.; Gilhus, N.E. Left ventricular long-axis function in myasthenia gravis. J. Neurol. 2008, 255, 1777–1784. [Google Scholar] [CrossRef]
- Cheng, C.-Y.; Cheng, G.-Y.; Shan, Z.-G.; Baritussio, A.; Lorenzoni, G.; Tyminska, A.; Ozieranski, K.; Iliceto, S.; Marcolongo, R.; Gregori, D.; et al. Efficacy of immunosuppressive therapy in myocarditis: A 30-year systematic review and meta analysis. Autoimmun. Rev. 2021, 20, 102710. [Google Scholar] [CrossRef]
- Zawadka-Kunikowska, M.; Rzepiński, Ł.; Tafil-Klawe, M.; Veronese, N.; Barbagallo, M.; Habek, M.; Gilhus, N.E. Altered Cardiac Autonomic Regulation in Individuals with Myasthenia Gravis—A Systematic Review and Meta-Analysis. Neurol. Int. 2023, 15, 1140–1154. [Google Scholar] [CrossRef]
- Ching, S.-M.; Chia, Y.-C.; Lentjes, M.A.H.; Luben, R.; Wareham, N.; Khaw, K.-T. FEV1 and total Cardiovascular mortality and morbidity over an 18 years follow-up Population-Based Prospective EPIC-NORFOLK Study. BMC Public Health 2019, 19, 501. [Google Scholar] [CrossRef] [PubMed]
- La Rovere, M.T.; Bigger, J.T., Jr.; Marcus, F.I.; Mortara, A.; Schwartz, P.J. Baroreflex sensitivity and heart-rate variability in prediction of total cardiac mortality after myocardial infarction. ATRAMI (Autonomic Tone and Reflexes After Myocardial Infarction) Investigators. Lancet 1998, 351, 478–484. [Google Scholar] [CrossRef] [PubMed]
- Tantucci, C.; Bottone, D.; Levi, G.; Uccelli, S.; Venturoli, N.; Magri, R.; Garrafa, E.; Pini, L. Respiratory function, autonomic dysfunction, and systemic inflammation are closely linked in patients with COPD and tidal flow limitation: An exploratory study. Respir. Physiol. Neurobiol. 2020, 284, 103565. [Google Scholar] [CrossRef] [PubMed]
- Reis, M.S.; Arena, R.; Deus, A.P.; Simões, R.P.; Catai, A.M.; Borghi-Silva, A. Deep breathing heart rate variability is associated with respiratory muscle weakness in patients with chronic obstructive pulmonary disease. Clinics 2010, 65, 369–375. [Google Scholar] [CrossRef] [PubMed]
- Bianchi, L.; Porta, C.; Rinaldi, A.; Gazzaruso, C.; Fratino, P.; DeCata, P.; Protti, P.; Paltro, R.; Bernardi, L. Integrated cardiovascular/respiratory control in type 1 diabetes evidences functional imbalance: Possible role of hypoxia. Int. J. Cardiol. 2017, 244, 254–259. [Google Scholar] [CrossRef] [PubMed]
- Junior, M.S.A.; Carvalhal, R.; Carneiro, J.; Lapa, M.; Zin, W.; Lugon, J.; Guimarães, F. Association between respiratory mechanics and autonomic function in morbid obesity. Rev. Port. Pneumol. 2014, 20, 31–35. [Google Scholar] [CrossRef]
- Bai, T.; Zhou, D.; Yushanjiang, F.; Wang, D.; Zhang, D.; Liu, X.; Song, J.; Zhang, J.; Hou, X.; Ma, Y. Alternation of the Autonomic Nervous System Is Associated With Pulmonary Sequelae in Patients With COVID-19 After Six Months of Discharge. Front. Physiol. 2022, 12, 805925. [Google Scholar] [CrossRef]
- Rzepiński, Ł.; Zawadka-Kunikowska, M.; Newton, J.L.; Zalewski, P. Cardiac Autonomic Dysfunction in Myasthenia Gravis and Re-lapsing-Remitting Multiple Sclerosis-A Pilot Study. J. Clin. Med. 2021, 10, 2173. [Google Scholar] [CrossRef]
- Jaretzki, A.; Barohn, R.; Ernstoff, R.; Kaminski, H.; Keesey, J.; Penn, A.; Sanders, D. Myasthenia gravis: Recommendations for clinical research standards. Task force of the medical scientific advisory board of the myasthenia gravis foundation of America. Neurology 2000, 55, 16–23. [Google Scholar] [CrossRef]
- Graham, B.L.; Steenbruggen, I.; Miller, M.R.; Barjaktarevic, I.Z.; Cooper, B.G.; Hall, G.L.; Hallstrand, T.S.; Kaminsky, D.A.; McCarthy, K.; McCormack, M.C.; et al. Standardization of spirometry 2019 update. An official American thoracic society and European respiratory society technical statement. Am. J. Respir. Crit. Care Med. 2019, 200, e70–e88. [Google Scholar] [CrossRef]
- Pellegrino, R.; Viegi, G.; Brusasco, V.; Crapo, R.O.; Burgos, F.; Casaburi, R.; Coates, A.; Van Der Grinten, C.P.M.; Gustafsson, P.; Hankinson, J.; et al. Interpretative strategies for lung function tests. Eur. Respir. J. 2005, 26, 948–968. [Google Scholar] [CrossRef] [PubMed]
- Stanojevic, S.; Kaminsky, D.A.; Miller, M.R.; Thompson, B.; Aliverti, A.; Barjaktarevic, I.; Cooper, B.G.; Culver, B.; Derom, E.; Hall, G.L.; et al. ERS/ATS technical standard on interpretive strategies for routine lung function tests. Eur. Respir. J. 2021, 60, 2101499. [Google Scholar] [CrossRef] [PubMed]
- Cheshire, W.P.; Freeman, R.; Gibbons, C.H.; Cortelli, P.; Wenning, G.K.; Hilz, M.J.; Spies, J.M.; Lipp, A.; Sandroni, P.; Wada, N.; et al. Electrodiagnostic assessment of the autonomic nervous system: A consensus statement endorsed by the American Autonomic Society, American Academy of Neurology, and the International Federation of Clinical Neurophysiology. Clin. Neurophysiol. 2020, 132, 666–682. [Google Scholar] [CrossRef] [PubMed]
- Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology. Assessment clinical auto-nomic testing report of the therapeutics and technology subcommittee of the American Academy of Neurology. Neurology 1996, 46, 873–880. [Google Scholar]
- Bianchi, A.M.; Mainardi, L.T.; Meloni, C.; Chierchiu, S.; Cerutti, S. Continuous monitoring of the sympatho-vagal balance through spectral analysis. IEEE Eng. Med. Biol. Mag. 1997, 16, 64–73. [Google Scholar] [CrossRef]
- Fortin, J.; Klinger, T.; Wagner, C.; Sterner, H.; Madritsch, C.; Grüllenberger, R.; Hacker, A.; Habenbacher, W.; Skrabal, F. The task force monitor—A non-invasive beat-to beat monitor for hemodynamic and autonomic function of the human body. In Proceedings of the 20th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Hong Kong, China, 1 November 1998; Volume 66, pp. 63–151. [Google Scholar]
- NIST/SEMATECH e-Handbook of Statistical Methods. Available online: http://www.itl.nist.gov/div898/handbook/.2012/01/20 (accessed on 21 August 2020).
- Aguirre, F.; Fernández, R.N.; Arrejoría, R.; Manin, A.; Cores, V.; Sivori, M.; Villa, A. Peak expiratory flow and the single-breath count test as markers of respiratory function in patients with myasthenia gravis. Neurol. Engl. Ed. 2020, 38, 405–411. [Google Scholar] [CrossRef] [PubMed]
- Puri, S.; Baker, B.L.; Dutka, D.P.; Oakley, C.M.; Hughes, J.M.B.; Cleland, J.G.F. Reduced alveolar–capillary membrane diffusing capacity in chronic heart failure. Its pathophysiological relevance and relationship to exercise performance. Circulation 1995, 91, 2769–2774. [Google Scholar] [CrossRef]
- Zhi, H.; Ji, X.; Zhao, Z.; Liang, H.; Zhong, S.; Luo, Y.; Zhong, M.; Zhan, C.; Gao, Y.; Deng, X.; et al. Risk factors for impaired pulmonary diffusion function in convalescent COVID-19 patients: A systematic review and meta-analysis. EClinicalMedicine 2022, 49, 101473. [Google Scholar] [CrossRef]
- Mayr, A.K.; Wieser, V.; Funk, G.-C.; Asadi, S.; Sperk, I.; Urban, M.H.; Valipour, A. Impaired Spontaneous Baroreceptor Reflex Sensitivity in Patients With COPD Compared to Healthy Controls: The Role of Lung Hyperinflation. Front. Med. 2022, 8, 791410. [Google Scholar] [CrossRef]
- Elstad, M.; O’Callaghan, E.L.; Smith, A.J.; Ben-Tal, A.; Ramchandra, R. Cardiorespiratory interactions in humans and animals: Rhythms for life. Am. J. Physiol. Heart Circ. Physiol. 2018, 315, H6–H17. [Google Scholar] [CrossRef]
- Sperandio, E.; Silveira, M.; Matheus, A.; Lauria, V.; Santos, D.; Pareira, R.; Almeida, F.; Almeida, V.; Romiti, M.; Gagliardi, A.; et al. Correlation between heart rate variability and pulmonary function in adults. Eur. Respir. J. 2014, 44, P2183. [Google Scholar]
- Bianchim, M.; Sperandio, E.; Martinhão, G.; Matheus, A.; Lauria, V.; da Silva, R.; Spadari, R.; Gagliardi, A.; Arantes, R.; Romiti, M.; et al. Correlation between heart rate variability and pulmonary function adjusted by confounding factors in healthy adults. Braz. J. Med. Biol. Res. 2016, 49, e4435. [Google Scholar] [CrossRef] [PubMed]
- Kleiger, R.E.; Stein, P.K.; Bigger, J.T., Jr. Heart rate variability: Measurement and clinical utility. Ann. Noninvasive Electrocardiol. 2005, 10, 88–101. [Google Scholar] [CrossRef] [PubMed]
- Rizzi, M.; Atzeni, F.; Airoldi, A.; Masala, I.F.; Frassanito, F.; Salaffi, F.; Macaluso, C.; Sarzi-Puttini, P. Impaired lung transfer factor in fibromyalgia syndrome. Clin Exp Rheumatol. 2016, 34, S114–S119. [Google Scholar]
- Van der Velden, V.H.; Hulsmann, A.R. Autonomic innervation of human airways: Structure, function, and pathophysiology in asthma. Neuroimmunomodulation 1999, 6, 145–159. [Google Scholar] [CrossRef]
- Zannin, E.; Pellegrino, R.; Di Toro, A.; Antonelli, A.; Dellacà, R.L.; Bernardi, L. Parasympathetic Stimuli on Bronchial and Cardiovascular Systems in Humans. PLoS ONE 2015, 10, e0127697. [Google Scholar] [CrossRef]
- Gardim, C.B.; Veiga, A.C.; Aguilar, B.A.; Philbois, S.V.; Souza, H.C.D. Effects of chronic cholinergic stimulation associated with aerobic physical training on cardiac morphofunctional and autonomic parameters in spontaneously hypertensive rats. Sci. Rep. 2021, 11, 17141. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| HCs | Total MG | p-Value | |
|---|---|---|---|
| Number of subjects | 22 | 22 | |
| Sex, female n (%) | 16 (77.73) | 17 (77.27) | 0.727 |
| BMI, mean (kg/m2) | 23.66 ± 3.82 | 25.42 ± 4.34 | 0.160 |
| Age, mean (years) | 37.32 ± 12.17 | 42.45 ± 7.19 | 0.096 |
| Age at first manifestation, mean (years) | 35.32 ± 9.42 | ||
| Disease duration (years), mean (range) | 6.93 ± 8.02 | ||
| Seropositivity to AChR antibodies, n (%) | 9 (40.9) | ||
| Seropositivity to MuSK antibodies, n (%) | 4 (18.2) | ||
| Seropositivity to AChR and MuSK, antibodies, n (%) | 1 (4.54) | ||
| Type of MG, n (%) | |||
| Ocular | 1 (4.5) | ||
| Generalized | 21 (95.5) | ||
| Thymectomy, n (%) | 7 (22) | ||
| Severity of disease at the moment of testing (MGFA, number, %) | |||
| Class 0 | 0 (0) | ||
| Class I (ocular) | 1 (4.5) | ||
| Class IIa | 9 (40.9) | ||
| Class IIIa | 12 (54.5) | ||
| Histology changes, n (%) | |||
| Thymic pathology | 14 (63.6) | ||
| Thymoma | 1 (4.5) | ||
| Unknown | 1 (4.5) | ||
| Type of treatment, n (%) | |||
| Use of cholinesterase inhibitors | 21 (95.5) | ||
| Use of corticosteroids | 13 (59.1) | ||
| Use of immunosuppressants | 8 (36.4) |
| MG | HCs | p | |||
|---|---|---|---|---|---|
| Pulmonary Volume | Mean | Median [Q1–Q3] | Mean | Median [Q1–Q3] | |
| VC (L) | 3.67 | 3.60 [2.91–4.22] | 4.28 | 4.22 [3.59–4.70] | 0.037 |
| VC (%pred) | 94.12 | 94.50 [83.00–110.00] | 105.95 | 107.00 [99.00–115.0] | 0.059 |
| IC (L) | 2.65 | 2.46 [2.01–3.02] | 3.01 | 2.80 [2.37–3.55] | 0.192 |
| IC (%pred) | 101.77 | 96.50 [90.00–109.00] | 106.73 | 108.50 [98.00–115.00] | 0.124 |
| RV (L) | 1.98 | 2.13 [1.57–2.41] | 1.92 | 1.82 [1.48–2.07] | 0.753 |
| RV (%pred) | 114.23 | 110.50 [99.00–132.00] | 110.50 | 107.00 [91.00–129.00] | 0.737 |
| TLC (L) | 5.59 | 4.96 [4.75–6.39] | 6.21 | 5.93 [5.50–6.80] | 0.139 |
| TLC (%pred) | 101.32 | 96.00 [91.00–103.00] | 106.73 | 105.50 [99.00–115.00] | 0.262 |
| RV/TLC | 35.70 | 36.53 [31.82–41.16] | 30.69 | 29.31 [24.90–36.49] | 0.093 |
| RV/TLC (%pred) | 109.64 | 113 [94.00–128.00] | 97.59 | 95.00 [87.00–112.00] | 0.129 |
| Pulmonary diffusing capacity | |||||
| DLCO (mmol/min/kPa) | 7.90 | 7.14 [6.01–8.87] | 8.55 | 8.44 [7.70–9.59] | 0.252 |
| DLCO (%pred) | 84.53 | 85.00 [75.00–91.00] | 88.95 | 90.00 [80.00–95.00] | 0.315 |
| KCO (mmol/min/kPa/L) | 1.53 | 1.58 [1.40–1.72] | 5.28 | 1.59 [1.40–1.75] | 0.410 |
| KCO (%pred) | 91.60 | 98.00 [84.00–100.00] | 93.05 | 92.00 [83.00–105.00] | 0.843 |
| Pulmonary ventilation | |||||
| FVC (L) | 3.70 | 3.57 [3.17–4.19] | 4.52 | 4.31 [3.97–5.29] | 0.051 |
| FVC (%pred) | 104.05 | 91.50 [80.00–99.00] | 110.86 | 113.00 [108.00–115.00] | 0.021 |
| FEV1 (L) | 2.84 | 2.74 [2.54–3.35] | 3.50 | 3.34 [3.03–3.90] | 0.011 |
| FEV1 (%pred) | 85.86 | 90.00 [80.00–96.00] | 98.23 | 99.00 [94.00–104.00] | 0.010 |
| FEV1/FVC ratio (%) | 76.58 | 79.02 [75.64–82.01] | 80.16 | 78.95 [76.43–86.50] | 0.379 |
| FEV1/FVC (%pred) | 93.64 | 97.50 [91.00–100.00] | 96.73 | 96.50 [93.00–100.00] | 0.760 |
| FEV1/VCmax | 72.93 | 75.07 [72.93–76.95] | 77.90 | 77.21 [73.14–81.65] | 0.193 |
| FEV1/VCmax% | 90.27 | 92.00 [90.00–97.00] | 95.45 | 95.50 [89.00–100.00] | 0.302 |
| Respiratory mechanics | |||||
| PEF (L/s) | 5.68 | 5.67 [4.55–6.68] | 6.53 | 6.27 [5.58–7.40] | 0.163 |
| PEF (%pred) | 77.82 | 77.50 [67.00–88.00] | 84.86 | 82.00 [73.00–97.00] | 0.282 |
| MEF50 (L/s) | 3.47 | 3.34 [2.86–4.59] | 4.23 | 3.91 [3.43–4.55] | 0.055 |
| MEF50 (%pred) | 79.64 | 82.50 [68.00–94.00] | 91.55 | 8.50 [73.00–105.00] | 0.113 |
| MIF50(L/s) | 4.21 | 4.41 [3.36–5.07] | 4.85 | 4.62 [3.98–5.39] | 0.149 |
| PIF (L/s) | 4.40 | 4.43 [3.43–5.27] | 4.92 | 4.72 [4.32–5.32] | 0.187 |
| sRAW (kPa × s) | 0.94 | 0.88 [0.72–1.09] | 1.04 | 1.09 [0.72–1.34] | 0.336 |
| sRAW (%pred) | 93.50 | 86.50 [67.00–102.00] | 102.32 | 107.50 [75.00–124.00] | 0.296 |
| RAWtot (kPa × s/L) | 0.30 | 0.26 [0.21–0.34] | 0.31 | 0.27 [0.25–0.33] | 0.805 |
| sRAWtot (kPa × s/L) | 98.73 | 84.00 [71.00–114.00] | 103.91 | 87.50 [82.00–109.00] | 0.664 |
| MG | HCs | p | |
|---|---|---|---|
| Breathing rate (bpm) | 17.27 [14.49–19.22] | 16.21 [15.04–18.22] | 0.263 |
| HR (1/min) | 65.44 [62.35–65.44] | 62.64 [59.30–67.92] | 0.826 |
| LF-RRI (ms2) | 418.19 [306.76–1138.21] | 1014.71 [322.75–1539.50] | 0.136 |
| HF-RRI (ms2) | 235.30 [73.16–493.67] | 463.76 [191.16–884.74] | 0.038 |
| PSD-RRI (ms2) | 1047.04 [530.97–2565.85] | 2647.00 [810.82–3824.54] | 0.040 |
| LF/HF-RRI (1) | 2.14 [1.15–4.66] | 1.91 [0.99–3.35] | 0.307 |
| LF/HF (1) | 1.88 [0.95–2.84] | 1.05 [0.85–2.12] | 0.113 |
| E/I ratio | 1.19 [1.12–1.29] | 1.21 [1.17–1.36] | 0.058 |
| Valsalva ratio | 1.32 [1.11–1.47] | 1.32 [1.20–1.70] | 0.337 |
| BRS (ms/mmHg) | 13.45 [9.06–17.99] | 20.05 [12.70–27.70] | 0.037 |
| Parasympathetic dysfunction (%) | 27.27 | 4.55 | 0.047 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zawadka-Kunikowska, M.; Rzepiński, Ł.; Cieślicka, M.; Fanslau, J.; Klawe, J.J.; Tafil-Klawe, M. Correlation between Cardiovascular Autonomic and Pulmonary Ventilation Functions in Myasthenia Gravis Patients. Adv. Respir. Med. 2023, 91, 546-559. https://doi.org/10.3390/arm91060040
Zawadka-Kunikowska M, Rzepiński Ł, Cieślicka M, Fanslau J, Klawe JJ, Tafil-Klawe M. Correlation between Cardiovascular Autonomic and Pulmonary Ventilation Functions in Myasthenia Gravis Patients. Advances in Respiratory Medicine. 2023; 91(6):546-559. https://doi.org/10.3390/arm91060040
Chicago/Turabian StyleZawadka-Kunikowska, Monika, Łukasz Rzepiński, Mirosława Cieślicka, Joanna Fanslau, Jacek J. Klawe, and Małgorzata Tafil-Klawe. 2023. "Correlation between Cardiovascular Autonomic and Pulmonary Ventilation Functions in Myasthenia Gravis Patients" Advances in Respiratory Medicine 91, no. 6: 546-559. https://doi.org/10.3390/arm91060040
APA StyleZawadka-Kunikowska, M., Rzepiński, Ł., Cieślicka, M., Fanslau, J., Klawe, J. J., & Tafil-Klawe, M. (2023). Correlation between Cardiovascular Autonomic and Pulmonary Ventilation Functions in Myasthenia Gravis Patients. Advances in Respiratory Medicine, 91(6), 546-559. https://doi.org/10.3390/arm91060040