Abstract
We here delve into the intricate and evolving concepts of brain death and consciousness, particularly at the end of life. We examine the historical and technological advancements that have influenced our understanding of death, such as mechanical ventilation and resuscitation techniques. These developments have challenged traditional definitions of death, leading to the concept of brain death, defined as the irreversible loss of all brain functions, including the brainstem. We emphasize that consciousness exists on a continuum, ranging from full alertness to deep coma and complete cessation of brain activity. It explores various disorders of consciousness, including coma, vegetative state, minimally conscious state, and locked-in syndrome, each with distinct characteristics and levels of awareness. Neuroimaging techniques, such as EEG, fMRI, and DTI, are highlighted for their crucial role in diagnosing and understanding disorders of consciousness. These techniques help to detect covert consciousness, assess brain activity, and predict recovery potential. The phenomenon of the “wave of death,” which includes a paradoxical surge in brain activity at the point of death, is also discussed. We address the challenges in defining and understanding both death and consciousness, calling for biologically grounded, ethically defensible, and culturally sensitive definitions. We advocate for standardized neuroimaging protocols, longitudinal studies, and the integration of artificial intelligence to improve diagnosis and treatment. In conclusion, the document underscores the importance of an integrated, evidence-based approach to understanding the gray zones between life and death, recognizing that consciousness and death are dynamic processes with both biological and experiential dimensions.
1. Introduction
Lack of a Scientific Conceptualization of Death and Cessation of Consciousness
The concept of brain death/death by neurological criteria (BD/DNC) has slowly developed a consensus, although it possesses numerous problems in understanding the physiology of end-of-life [1,2]. Moreover, there has been an incongruity between the definition of consciousness and the characterization of its pathology [3], leading to the study of different disorders of consciousness [4] (DoCs). Equivocal brain death cases have lately raised new disagreements about understanding BD/DNC and the classification of DoCs [5,6].
In the past, most agreed that death occurred when heartbeat and breathing ceased and the soul abandoned the body. However, the concept of death has evolved significantly with advancements in medical technology, particularly with the development of reanimation (resuscitation) and mechanical ventilation. These technologies made it possible to restore and maintain heart and lung function, even in cases where these functions had ceased temporarily. This led to the realization that the cessation of cardiopulmonary function could be reversible, challenging the traditional concept of death [2].
Although the interplay of anatomical and environmental conditions allows us to produce rules, exceptions to these norms complicate the process of developing universals and, thus, a definition of death. Lack of oxygenated blood flow, which is frequently the direct result of cardiac arrest (asystole), significant brain swelling, drug abuse, and strokes, is highly associated with anoxia [7,8]. Brain regions die at varying rates with ischemia or anoxia. In as little as two to four minutes, the cerebellum and brain may become permanently damaged. The brainstem, however, is significantly more robust, and it can function after as much as 15–20 min of anoxia [9,10,11]. Since the brain has completely died at this time, the body—if mechanical ventilation is provided for an individual who has lost all brain function—and the heart may still be revived, and circulation and other body functions, including brain function, may be restored. Clinicians have determined that an individual who is dependent on a ventilator and displays complete and permanent loss of all brain functions is “brain dead” [12].
When a patient is deemed dead according to accepted medical procedures because their entire brain is non-functional, the term brain death/death by neurological criteria (BD/DNC) is typically used by clinicians to describe this state [12,13,14,15]. This usage has drawn criticism, as it appears to blur the line between a “dead organ,” which is the brain itself, and a “dead organism,” which is a person who has been declared dead as a result of brain damage [16].
As medical technology advanced, the concept of BD/DNC emerged, defined as the irreversible loss of all functions of the brain, including the brainstem. This concept was introduced to address situations where mechanical ventilation could maintain cardiopulmonary function in a patient who had lost all brain activity. The Harvard Medical School’s 1968 report was pivotal in establishing brain death as the criterion of death [17].
2. Life, Death, and Consciousness Are Not Binary
Consciousness throughout the lifespan, including at the end of life, does not function as a simple on/off state; it is not switched on or off, but it is rather part of a continuum with states ranging from full alertness to deep coma, minimally conscious states, and ultimately to complete cessation of brain activity [18] represented in Figure 1.
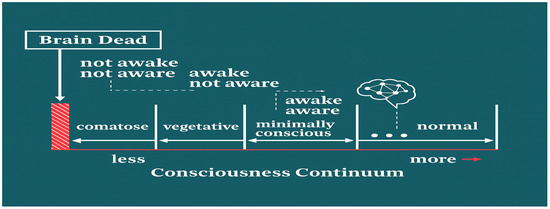
Figure 1.
Conceptual diagram illustrating the overlap and distinctions between disorders of consciousness and death by neurological criteria, integrating recent neuroimaging and pathophysiological findings. Here, we represent gradations from coma and vegetative state to a minimally conscious state and full consciousness [adapted from Laureys et al. (2004) and updated to reflect current classifications of altered states of consciousness [Leisman & Machado [2]].
Objective measurement of consciousness has advanced significantly in recent decades. Electroencephalography (EEG) remains one of the most practical and widely used tools for assessing brain states, offering a dynamic, real-time window into cortical and subcortical activity. In general terms, higher states of awareness and wakefulness tend to be associated with lower voltage, higher frequency activity—notably in the beta and gamma ranges—while states of diminished consciousness are characterized by higher voltage, slower waves in the theta and delta ranges [19]. An example of this relationship between EEG activity and behavioral arousal levels is shown in Figure 2.
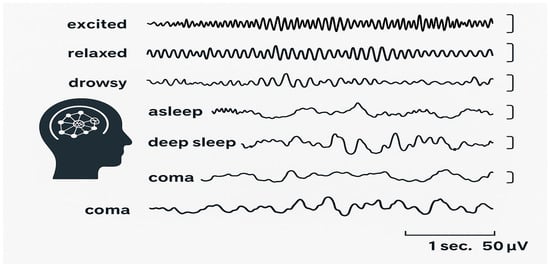
Figure 2.
EEG activity and corresponding behavioral states across varying arousal levels, adapted from Leisman & Koch [16], illustrating the shift from low-voltage fast activity in wakefulness to high-voltage slow activity in deep unconsciousness.
Attempting to Objectify the Complete Cessation of Consciousness at the Point of Death
The recently reported “wave of death” in brain cells that denotes the end of awareness provides new insights into the dying process and the brain alterations that follow, which impact consciousness. The moment of death has been portrayed as a discrete event in which all brain processes abruptly cease. Many think that, clinically and legally, death can be considered a well-defined state characterized at least by a complete and irreversible cessation of brain activities and functions [20,21]. However, death is hard to describe neurobiologically and to correlate with consciousness states [18]. Much support has been found showing that the end of life is not characterized by a sudden transformation from life to death, but rather by a process extended over time associated with a complex array of changes in brain activity [18,22]. In certain situations, the process can even be reversed [23].
Prior studies have demonstrated that over an extended period of oxygen deprivation, or anoxia, the brain’s activity changes sequentially. The brain’s reserves of ATP, which power all cellular functions, are quickly depleted when oxygen flow to the area is interrupted or restricted. This results in damage to brain neurons and is associated with a large-scale release of glutamate, a neurotransmitter vital for transmitting messages between the brain and the rest of the nervous system [24].
Shramm and colleagues [21] have found that neural circuits seem to shut down at first, followed by a surge in brain activity with a consequential increase in gamma and beta waves. These waves are highly associated with conscious experience. After that, neuronal activity progressively decreases until the brain reaches a state of complete electrical quiet [21]. An electroencephalogram (EEG) shows flat lines in this state. However, a wave of death soon breaks through this quiet, appearing on the flat EEG and reflecting abrupt phenomena known as “anoxic depolarization.” In the cortex, this event seems to trigger cell death. The wave of death does not always indicate the complete loss of brain function. Anoxic depolarization can be reversed if the brain is quickly reoxygenated [25]. A “wave of resuscitation,” which signals a gradual recovery of brain functioning, is indicative of this mechanism, which Shramm and associates [21] had previously observed. Until recently, we were unsure of whether the wave of death propagated uniformly across the brain’s layers or where it began in the cortex [26].
Similarly, Borjigin et al. [27] assessed rats undergoing experimental cardiac arrest by continuous EEG and estimated power density, coherence, directed connectivity, and cross-frequency coupling changes. These authors identified a transient surge of synchronous gamma oscillations within the first 30 s after cardiac arrest, which preceded the isoelectric EEG. During cardiac arrest, gamma oscillations were global and exceedingly coherent. Furthermore, this frequency band showed a conspicuous increment in anterior–posterior-directed connectivity and close-fitting phase-coupling with theta and alpha oscillations. These authors affirmed that the high-frequency neurophysiological activity in the near-death state surpassed levels found during the conscious waking state. They concluded that the mammalian brain could generate neural correlates of heightened conscious processing at near-death, albeit paradoxically [27,28].
Such findings have spurred renewed interest in the neurophenomenology of dying, raising fundamental questions: Could these transient high-frequency bursts represent the neural basis of so-called “near-death experiences”? Do they reflect a final integrative act of consciousness, or are they epiphenomenal discharges of a failing network? While these remain open questions, it is clear that life, death, and consciousness are not binary—but dynamically interwoven processes with phases of activity that challenge traditional definitions.
3. Objectively Classifying Disorders of Consciousness
A disorder of consciousness is a state where consciousness has been affected by damage to the brain, trauma, or shock to an individual, or pharmacologically induced [29]. The two components of consciousness—wakefulness and awareness—are intricately connected and involve extensive brain networks [30,31]. Wakefulness refers to being awake and alert, while awareness encompasses our perception, cognition, and self-awareness. It involves basic physiological functions, such as opening the eyes and exhibiting reflexes like coughing, swallowing, and sucking. It is mainly related to the ascending reticular activating system (ARAS), which regulates wakefulness and sleep–wake transitions. Awareness refers to the quality or state of understanding that something is happening or exists. It encompasses both cognizance and perception of one’s surroundings or inner experience. It is necessary to assess whether wakefulness and awareness are affected to classify the disorders of consciousness [32,33]. Unlike the primordial consciousness that is seen in the fetus, consciousness is best described as awake plus content [34,35]. Evidence that one can be awake without consciousness suggests that wakefulness is a condition of the brain in which it can take input from the external environment as well as the self (internal environment) and appropriately respond [36].
Assuming that clinically important altered consciousness states can be viewed from the vantage point of a given position on the bounded continuum reflected in Figure 1, then the main disorders of consciousness can be placed on the spectrum.
3.1. Coma
This is the most profound and prolonged state of impaired consciousness. Individuals in a coma are unresponsive and lack awareness or wakefulness associated with a variety of causes that can include traumatic head injuries, stroke, brain tumor, drug or alcohol intoxication, or underlying illnesses, such as diabetes or sepsis. The associated behaviors can include closed eyes and depressed brainstem reflexes, including pupils not responsive to light. No responses of limbs or to painful stimuli except for reflex movements and irregular breathing. Some individuals in a coma have reported hearing or remembering events during the coma period [32].
It is sometimes possible to hear and remember events that occurred during the time an individual was in a comatose state, depending on the type and depth of the coma. There is evidence that individuals in a coma can hear what occurs around them. Some comatose individuals can remember what they heard happening nearby. However, this can vary widely, and it is difficult to predict how and when a person might experience this [37].
3.2. Vegetative State/Unresponsive Wakefulness Syndrome (VS/UWS)
In this state, individuals remain unresponsive and unaware but exhibit wakefulness. Despite spontaneous eye opening and independent vital functions, VS/UWS patients cannot functionally communicate their thoughts or feelings and appear completely unaware of their surroundings and themselves [38]. Uncertainty about the natural course of VS/UWS plays a major part in many of these cases. With a prevalence of 0.2 to 6.1 patients per 100,000 inhabitants [39], it is classified as a rare to ultra-rare medical condition [40]. The evidence about the expected outcome in patients in VS/UWS was characterized as “limited” in a 2018 review by the American Academy of Neurology (AAN) [41].
3.3. Minimally Conscious State (MCS)
MCS represents a less profound impairment. Individuals in this state exhibit wakefulness, some awareness, and limited responsivity. Unlike a VS/UWS state, individuals with MCS can show signs of self or environmental awareness, though these are often inconsistent. MCS patients may follow simple commands, gesture yes or no, have intelligible speech, or show purposeful behavior [42,43].
MCS Plus is a term used to describe patients who are in a minimally conscious state but show additional, more complex behaviors. These may include sustained visual pursuit, reproducible movement to command, or intelligible verbalization. The “Plus” signifies that these patients have surpassed the basic criteria for MCS and are demonstrating higher cognitive functions [42]. Both conditions are part of a spectrum of disorders of consciousness, and the distinction between them is important for diagnosis, prognosis, and treatment planning. While MCS is often a transitional state, it can become a permanent condition for some individuals [31,44].
3.4. Locked-In Syndrome (LIS)
LIS is a neurological condition in which a person cannot move, speak, or exhibit voluntary muscle control. Despite their paralysis, people with LIS are conscious and can hear and understand things around them. This state is characterized by complete paralysis of nearly all voluntary muscles in the body except for vertical eye movements and blinking. LIS patients can communicate using vertical eye movements and blinking to “YES” and “NO” codes [45].
4. Neuroimaging to Study DoCs
Neuroimaging plays a pivotal role in the diagnosis and classification of disorders of consciousness (DoC), such as coma, vegetative state, and minimally conscious state [46]. Advanced neuroimaging techniques, including structural and functional MRI, EEG, and functional near-infrared spectroscopy, have significantly enhanced our understanding of these conditions. Bedside examinations remain crucial for assessing patients with DoC. However, they can be supplemented with neuroimaging findings to improve accuracy [46].
Recent advances in structural and functional imaging modalities, including high-resolution structural MRI, functional MRI (fMRI), diffusion tensor imaging (DTI), electroencephalography (EEG), magnetoencephalography (MEG), and functional near-infrared spectroscopy (fNIRS), have allowed a deeper understanding of both overt and covert aspects of consciousness. These techniques reveal not only the presence or absence of residual brain activity but also the degree to which large-scale networks, such as the default mode network (DMN), salience network, and frontoparietal executive network, remain functionally connected in patients with DoCs [46,47]. For example, functional MRI can detect covert consciousness in patients who appear unresponsive. This has led to the identification of cognitive motor dissociation, where patients exhibit brain activity in response to commands despite no physical movement. Current guidelines recommend multimodal imaging protocols that combine different neuroimaging techniques to reduce misdiagnosis rates. Each technique provides complementary data, offering a more comprehensive assessment of the patient’s condition [46,47]. Neuroimaging also aids in prognostication. Studies have shown that approximately 20% of patients with DoC may be covertly aware, which has significant implications for their prognosis and treatment [46].
In summary, neuroimaging has become an essential tool in the diagnosis and classification of DoC, providing valuable information beyond traditional bedside examinations. It helps in understanding the underlying brain function, improving diagnostic accuracy, and informing treatment decisions [46,48,49].
4.1. Detecting Covert Consciousness
One of the most transformative applications of neuroimaging is the identification of cognitive motor dissociation (CMD)—a condition in which patients who appear behaviorally unresponsive nonetheless demonstrate willful modulation of brain activity in response to commands. Paradigms using mental imagery tasks in fMRI (e.g., imagining playing tennis vs. navigating a familiar home) have shown distinct and reproducible activation patterns in supplementary motor areas or parahippocampal gyrus in such patients [31].
EEG-based paradigms, including motor imagery and P300-based paradigms, allow for similar assessments at the bedside without the need for high-cost MRI [32]. Current guidelines recommend that the detection of CMD be attempted through multimodal protocols that combine behavioral assessment, fMRI or fNIRS, and electrophysiological methods, as each captures complementary aspects of brain function [31,48].
4.2. Prognostic Value of Neuroimaging
Neuroimaging biomarkers also play a growing role in predicting outcomes. For example, preservation of structural integrity in the thalamus, corpus callosum, and frontoparietal white matter on DTI correlates strongly with the potential for recovery [49]. Functional measures such as metabolic activity in the precuneus/posterior cingulate cortex on PET or fMRI connectivity strength in the DMN are also predictive of emergence from MCS [50]. Critically, ~20% of patients diagnosed as VS/UWS may have covert consciousness detectable by neuroimaging, which can substantially change prognosis and influence treatment planning [49,51].
4.3. Clinical Integration and Challenges
Despite the promise of advanced neuroimaging, routine clinical adoption faces challenges, including cost, limited scanner access, motion artifacts in severely impaired patients, and the need for standardized interpretation guidelines. Additionally, false negatives are possible if patients cannot sustain attention or if network dysfunction precludes task-related activation despite retained awareness [34]. Therefore, neuroimaging results must always be interpreted in conjunction with repeated bedside and electrophysiological assessments.
4.4. Future Directions
Emerging tools, such as ultra-high-field 7T MRI, resting-state network mapping, machine learning-based EEG classifiers, and multimodal hybrid imaging (e.g., simultaneous EEG-fMRI), promise improved sensitivity for detecting residual cognition. In parallel, portable imaging technologies like wearable fNIRS systems and high-density EEG headsets may expand bedside applications in ICU and rehabilitation settings [33]. Integration of these data streams into AI-driven prognostic models could further personalize patient management and optimize rehabilitation strategies.
In summary, neuroimaging has evolved into an indispensable adjunct for diagnosing, classifying, and prognosticating DoCs as reflected in Figure 3. By enabling the detection of covert consciousness, elucidating network-level dysfunction, and predicting recovery potential, multimodal imaging substantially augments traditional behavioral assessment. Its future lies in bedside-adapted, high-sensitivity protocols that integrate seamlessly with clinical workflows, ensuring that no patient with residual awareness is overlooked [49].
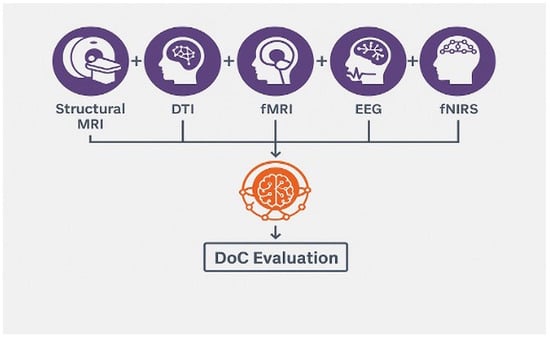
Figure 3.
Schematic showing multimodal neuroimaging workflow for DoC evaluation, integrating structural MRI, DTI, fMRI, EEG, and fNIRS.
5. Discussion
The present work has examined the multifaceted challenges in defining and understanding both the physiological and neurological dimensions of end-of-life and the discrepancies between the definition of consciousness and its pathological characterization. Despite decades of conceptual refinement, the criteria for brain death/death by neurological criteria (BD/DNC) remain an area of ongoing debate. While a growing international consensus exists, inconsistencies in diagnostic protocols, cultural interpretations, and legal definitions still complicate the uniform application of BD/DNC across jurisdictions [3,4]. This ambiguity is further magnified by the absence of a universally agreed-upon definition of consciousness itself, which hampers the precision with which we can identify its disorders [5].
Historically, death was understood as the irreversible cessation of cardiopulmonary function, an endpoint marked by the simultaneous stillness of heart and lungs. However, technological advances in resuscitation, mechanical ventilation, extracorporeal membrane oxygenation (ECMO), and targeted temperature management have fundamentally altered this definition. The possibility of restoring cardiopulmonary function long after spontaneous activity has ceased underscores the limitations of purely cardio-respiratory criteria and shifts the focus toward brain-based standards [12]. This shift, while scientifically justified, is not without its own complexities, as neurophysiological evidence shows that different brain regions succumb to injury at variable rates. The cerebral cortex and cerebellum may sustain irreversible injury within two to four minutes of complete ischemia, while the brainstem can remain viable for up to 15–20 min, especially under hypothermic or pharmacologically protective conditions [36]. This staggered vulnerability complicates the establishment of a singular biological threshold for death.
A recurring theme throughout this discussion is the rejection of a binary model of consciousness in favor of a continuum of wakefulness and awareness, extending from full cognitive engagement to states of minimal responsiveness and ultimately to complete unresponsiveness [2]. This continuum-based view aligns with emerging neuroimaging and electrophysiological data showing that patients traditionally diagnosed as vegetative/unresponsive wakefulness syndrome (VS/UWS) may retain covert consciousness detectable only through advanced functional imaging or EEG paradigms [49,51].
The phenomenon of the “wave of death,” as described in Section 2, further refines our understanding of the dying brain. Rather than an abrupt cessation of function, the terminal phase often involves a sequence of events: suppression of synaptic activity, a paradoxical surge in gamma-band oscillations (associated with heightened conscious processing), followed by anoxic depolarization, and a spreading loss of electrochemical gradients in neurons [17,19,20]. Importantly, the reversibility of anoxic depolarization in certain contexts—manifested as a “wave of resuscitation”, demonstrates that the final loss of consciousness is not necessarily an instantaneous event but may be modifiable within a narrow therapeutic window.
The classification of disorders of consciousness (DoCs), detailed in Section 3, benefits from this continuum-based perspective. Coma, VS/UWS, minimally conscious state (MCS), and locked-in syndrome (LIS) can be situated along a graded axis of preserved awareness and wakefulness, each with distinct neurophysiological signatures. The integration of multimodal neuroimaging (Section 4) into diagnostic workflows not only reduces the risk of misdiagnosis but also provides prognostic indicators by revealing patterns of residual network connectivity. Such approaches have already demonstrated that up to 20% of patients previously thought to be entirely unaware may retain some level of conscious processing [46].
The difference between clinical definitions of DoCs and theories of consciousness comes down to purpose, scope, and method—they are trying to answer different questions, using different tools, for different audiences. Any clinical definition and description of death endeavors to describe and classify observable and measurable states of consciousness for diagnosis, prognosis, and treatment so as to guide medical decisions, including prognosis, rehabilitation, and sometimes end-of-life care. Clinical definitions are grounded in behavioral observation, neuroimaging, and neurophysiology. The criteria, as we have indicated earlier, are defined by wakefulness (level of arousal) and awareness (content of consciousness). These states are evaluated by standardized clinical exams (e.g., Glasgow Coma Scale, Coma Recovery Scale–Revised) and supplementary tests (EEG, fMRI, etc.). The definitions must be practical, operational, and universally applicable to patients in diverse medical settings. They avoid speculation about what consciousness “is” and focus on what can be measured and acted upon in a clinical environment.
On the other hand, consciousness endeavors to explain what consciousness is, how it arises, and what mechanisms support it. Also, to address fundamental questions like: Why does subjective experience exist? How is it related to brain activity? These theories are built from neuroscience, psychology, philosophy, and computational modeling [1,2].
Clinical and theoretical definitions of death and consciousness as represented in Table 1, obviously fulfill different functions. Clinical definitions guide diagnosis and care decisions, often in urgent settings. Theories aim to explain the nature and mechanisms of consciousness, often without immediate clinical application. There also exist different evidence sources, with clinical definitions being based on observable behavior, bedside examination, neuroimaging results, and theories involving empirical neuroscience data, computational models, and philosophical analysis. Different constraints exist and must be operationalizable and replicable across hospitals, legal systems, and cultures, whereas theories are free to be conceptually bold or speculative, so long as they remain logically consistent and testable.

Table 1.
Comparison of clinical v. theoretical understanding of DoC addresses these point in comparative terms.
There are, in addition, different “units of analysis” with clinical views based on patients as cases, often with impaired communication, whereas with theories, the mind-brain relationship is in healthy as well as impaired systems. In short, clinical definitions are pragmatic, observable, and decision-oriented. Theories of consciousness are explanatory, mechanistic, and often abstract. They differ because medicine needs actionable categories to treat patients, while science and philosophy seek to understand the essence and mechanisms behind those categories.
6. Conclusions
The borders between life and death are neither sharp nor uniform across brains, patients, or contexts. Evidence reviewed here supports a continuum model of consciousness—spanning wakefulness, minimally conscious and covertly conscious states, through deep unresponsiveness—alongside a brain-based criterion of death (BD/DNC) whose clinical application is complicated by differential regional vulnerability, technological supports, and jurisdictional heterogeneity. Taken together, these insights argue for an integrated framework that couples meticulous bedside examination with multimodal neurophysiology and imaging, embedded within clear legal and ethical guardrails.
Advanced electrophysiological and neuroimaging tools can detect residual network function and covert command-following in a meaningful minority of patients historically labeled unresponsive. Their value, however, is maximized only when protocols are standardized, results are interpreted longitudinally and in context, and negative tests are not taken as definitive in isolation. Convergent, repeated assessments across methods should therefore be the rule rather than the exception.
For clinical practice and policy, we recommend the following priorities:
- Harmonize BD/DNC determination across institutions via consensus operational criteria, explicit documentation standards, and mandatory training/competency maintenance.
- Implement tiered, multimodal diagnostic pathways for disorders of consciousness (DoC) that integrate standardized behavioral scales with EEG/ERP and, when feasible, fMRI or fNIRS for covert responsiveness.
- Establish routine re-assessment schedules in prolonged DoC, with predefined triggers for escalating diagnostic depth (e.g., from EEG to fMRI).
- Create ethical decision frameworks for cases with covert consciousness, including communication aids, rehabilitation access, and transparent guidance for life-sustaining therapy deliberations.
- Build secure, prospective registries linking clinical phenotypes, imaging/electrophysiology, treatments, and outcomes to accelerate learning health–system cycles.
Future work should converge on portable, bedside-deployable modalities; robust cross-site standardization; and AI models that fuse structural, functional, and electrophysiological data to individualize prognosis. Particular attention is needed in pediatrics, in the early post-injury window when reversibility is most plausible, and in neuroethical scholarship that respects cultural variation while upholding patient dignity.
Recognizing consciousness and death as dynamic, graded phenomena reshapes how we diagnose, prognosticate, and care for patients at the threshold of life. By operationalizing this recognition—clinically, scientifically, and ethically—we can reduce misdiagnosis, personalize trajectories of care and rehabilitation, and make better-informed, more humane decisions for patients and families. The intertwined challenges of defining brain death, understanding the neurobiology of dying, and accurately classifying disorders of consciousness underscore the need for an integrated, evidence-based, and technologically informed approach. Advances in neuroimaging, electrophysiology, and neurocritical care are beginning to illuminate the gray zones between life and death, but their translation into clinical consensus will require sustained collaboration across neurology, critical care, bioethics, and law. The recognition that consciousness and death are not binary phenomena but dynamic processes with both biological and experiential dimensions represents a paradigm shift—one that promises to reshape both our scientific frameworks and our ethical responsibilities in end-of-life care.
Author Contributions
C.M. and G.L. contributed equally to this work. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| BD | Brain Death |
| CMD | Cognitive Motor Dissociation |
| DNC | Death by Neurological Criteria |
| DTI | Diffusion Tensor Imaging |
| DMN | Default Mode Network |
| ECMO | Extracorporeal Membrane Oxygenation |
| EEG | Electroencephalography |
| fMRI | Functional Magnetic Resonance Imaging |
| fNIRS | Functional Near-Infrared Spectroscopy |
| DoC | Disorders of Consciousness |
| LIS | Locked-In Syndrome |
| MCS | Minimally Conscious State |
| MEG | Magnetoencephalography |
| UWS | Unresponsive Wakeful State |
| VS | Vegetative State |
References
- Leisman, G.; Koch, P. Networks of conscious experience: Computational neuroscience in understanding life, death, and consciousness. Rev. Neurosci. 2009, 20, 151–176. [Google Scholar] [CrossRef]
- Leisman, G.; Machado, C. Many paths to consciousness or just one? Life in a bounded continuum. J. Conscious. Stud. 2021, 28, 83–96. [Google Scholar]
- Greer, D.M.; Lewis, A.; Kirschen, M.P. New developments in guidelines for brain death/death by neurological criteria. Nat. Rev. Neurol. 2024, 20, 151–161. [Google Scholar] [CrossRef] [PubMed]
- Bernat, J.L. The brainstem criterion of death and accurate syndromic diagnosis. Am. J. Bioeth. 2024, 1, 103–106. [Google Scholar] [CrossRef]
- Bayne, T.; Seth, A.K.; Massimini, M.; Shepherd, J.; Cleeremans, A.; Fleming, S.M.; Malach, R.; Mattingley, J.B.; Menon, D.K.; Owen, A.M.; et al. Tests for consciousness in humans and beyond. Trends Cogn. Sci. 2024, 28, 454–466. [Google Scholar] [CrossRef]
- Golden, K.; Bodien, Y.G.; Giacino, J.T. Disorders of consciousness: Classification and taxonomy. Phys. Med. Rehabil. Clin. N. Am. 2024, 35, 15–33. [Google Scholar] [CrossRef]
- Machado, C. Comment on: Canadian clinical practice guideline on brain death. Can. J. Anaesth. 2023, 70, 2013–2014. [Google Scholar] [CrossRef]
- Lewis, A. The Uniform Determination of Death Act is being revised. Neurocrit. Care 2022, 36, 335–338. [Google Scholar] [CrossRef]
- Lewis, A. How can international consistency in determination of brain death/death by neurological criteria be improved? The World Brain Death Project. J. Neurosurg. Anesthesiol. 2023, 35, 169–171. [Google Scholar] [CrossRef]
- Johnson, L.S.M. Philosophical, Medical, and Legal Controversies About Brain Death; Cambridge University Press: Cambridge, UK, 2024. [Google Scholar]
- Lewis, A. Response to Machado RE: Revisions to the Uniform Determination of Death Act and other controversial aspects of the determination of death by neurologic criteria. Neurocrit. Care 2023, 38, 214–216. [Google Scholar] [CrossRef]
- Wijdicks, E.F.M. The historical trajectory of the apnea test in brain death determination. Neurocrit. Care 2024, 40, 364–366. [Google Scholar] [CrossRef]
- Laureys, S.; Celesia, G.G.; Cohadon, F.; Lavrijsen, J.; Leon-Carrion, J.; Sannita, W.G.; Sazbon, L.; Schmutzhard, E.; von Wild, K.R.; Zeman, A.; et al. Unresponsive wakefulness syndrome: A new name for the vegetative state or apallic syndrome. BMC Med. 2010, 8, 68. [Google Scholar] [CrossRef]
- van Erp, W.S.; Lavrijsen, J.C.; Vos, P.E.; Bor, H.; Laureys, S.; Koopmans, R.T. The vegetative state: Prevalence, misdiagnosis, and treatment limitations. J. Am. Med. Dir. Assoc. 2015, 16, 85.e9–85.e14. [Google Scholar] [CrossRef] [PubMed]
- Richter, T.; Nestler-Parr, S.; Babela, R.; Khan, Z.M.; Tesoro, T.; Molsen, E.; Hughes, D.A.; ISPOR Rare Disease Special Interest Group. Rare disease terminology and definitions—A systematic global review: Report of the ISPOR Rare Disease Special Interest Group. Value Health 2015, 18, 906–914. [Google Scholar] [CrossRef] [PubMed]
- Goldblatt Hyatt, E.; Wilpers, A.; Bahtiyar, M.O.; Hu, Y.; Leon-Martinez, D.; Chervenak, F.A.; McCoyd, J.L.M. “I don’t have a telephone to the fetus”: Clinicians’ conceptions of fetal patienthood in maternal-fetal surgery counseling. Soc. Sci. Med. 2024, 342, 116525. [Google Scholar] [CrossRef] [PubMed]
- Carton-Leclercq, A.; Carrion-Falgarona, S.; Baudin, P.; Lemaire, P.; Lecas, S.; Topilko, T.; Charpier, S.; Mahon, S. Laminar organization of neocortical activities during systemic anoxia. Neurobiol. Dis. 2023, 188, 106345. [Google Scholar] [CrossRef]
- Charpier, S. Between life and death: The brain twilight zones. Front. Neurosci. 2023, 17, 1156368. [Google Scholar] [CrossRef]
- Borjigin, J.; Lee, U.; Liu, T.; Pal, D.; Huff, S.; Klarr, D.; Sloboda, J.; Hernandez, J.; Wang, M.M.; Mashour, G.A. Surge of neurophysiological coherence and connectivity in the dying brain. Proc. Natl. Acad. Sci. USA 2013, 110, 14432–14437. [Google Scholar] [CrossRef]
- Borjigin, J.; Wang, M.M.; Mashour, G.A. Reply to Greyson et al.: Experimental evidence lays a foundation for a rational understanding of near-death experiences. Proc. Natl. Acad. Sci. USA 2013, 110, E4406. [Google Scholar] [CrossRef]
- Schramm, A.E.; Carton-Leclercq, A.; Diallo, S.; Navarro, V.; Chavez, M.; Mahon, S.; Charpier, S. Identifying neuronal correlates of dying and resuscitation in a model of reversible brain anoxia. Prog. Neurobiol. 2020, 185, 101733. [Google Scholar] [CrossRef]
- Sarton, B.; Tauber, C.; Fridman, E.; Peran, P.; Riu, B.; Vinour, H.; David, A.; Geeraerts, T.; Bounes, F.; Minville, V.; et al. Neuroimmune activation is associated with neurological outcome in anoxic and traumatic coma. Brain 2024, 147, 1213–1228. [Google Scholar] [CrossRef]
- Zhang, Q.; Lu, H.; Wang, J.; Yang, T.; Bi, W.; Zeng, Y.; Yu, B. Hierarchical rhythmic propagation of corticothalamic interactions for consciousness: A computational study. Comput. Biol. Med. 2024, 169, 107843. [Google Scholar] [CrossRef]
- Lawrence, M.M.; Ramirez, R.P.; Bauer, P.J. Communicating with unconscious patients: An overview. Dimens. Crit. Care Nurs. 2023, 42, 3–11. [Google Scholar] [CrossRef] [PubMed]
- Slomine, B.S.; Suskauer, S.J. Disorders of consciousness in children: Assessment, treatment, and prognosis. Phys. Med. Rehabil. Clin. N. Am. 2024, 35, 223–234. [Google Scholar] [CrossRef] [PubMed]
- Thibaut, A.; Bodien, Y.G.; Laureys, S.; Giacino, J.T. Minimally conscious state “plus”: Diagnostic criteria and relation to functional recovery. J. Neurol. 2019, 266, 936–944. [Google Scholar]
- Farisco, M.; Formisano, R.; Gosseries, O.; Kato, Y.; Koboyashi, S.; Laureys, S.; Lejeune, N.; Martial, C.; Matar, A.; Morrisey, A.M.; et al. International survey on the implementation of the European and American guidelines on disorders of consciousness. J. Neurol. 2024, 271, 395–407. [Google Scholar] [CrossRef]
- Machado, C.; Rodriguez-Rojas, R.; Leisman, G. Partial recovery of vegetative state after a massive ischaemic stroke in a child with sickle cell anaemia. BMJ Case Rep. 2020, 13, e235370. [Google Scholar] [CrossRef]
- Schnetzer, L.; McCoy, M.; Bergmann, J.; Kunz, A.; Leis, S.; Trinka, E. Locked-in syndrome revisited. Ther. Adv. Neurol. Disord. 2023, 16, 17562864231160873. [Google Scholar] [CrossRef]
- Xu, L.B.; Hampton, S.; Fischer, D. Neuroimaging in disorders of consciousness and recovery. Phys. Med. Rehabil. Clin. N. Am. 2024, 35, 51–64. [Google Scholar] [CrossRef]
- Nanni-Zepeda, M.; Degutis, J.; Wu, C.; Rothlein, D.; Fan, Y.; Grimm, S.; Walter, M.; Esterman, M.; Zuberer, A. Neural signatures of shared subjective affective engagement and disengagement during movie viewing. Hum. Brain Mapp. 2024, 45, e26622. [Google Scholar] [CrossRef]
- Wang, J.; Lai, Q.; Han, J.; Qin, P.; Wu, H. Neuroimaging biomarkers for the diagnosis and prognosis of patients with disorders of consciousness. Brain Res. 2024, 1803, 149133. [Google Scholar] [CrossRef]
- Tangonan, R.; Lazaridis, C. Evaluation and management of disorders of consciousness in the acute care setting. Phys. Med. Rehabil. Clin. N. Am. 2024, 35, 79–92. [Google Scholar] [CrossRef] [PubMed]
- Christensen, R.; De Vries, L.S.; Cizmeci, M.N. Neuroimaging to guide neuroprognostication in the neonatal intensive care unit. Curr. Opin. Pediatr. 2024, 36, 190–197. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, Y.; Rameshkumar, R.; Krishnamurthy, S.; Senthilkumar, G.P. Incidence, risk factors, the role of plasma NGAL and outcome of contrast-induced acute kidney injury in critically ill children. Indian J. Pediatr. 2021, 88, 34–40. [Google Scholar] [CrossRef] [PubMed]
- Geisinger, R.; Rios, D.R.; McNamara, P.J.; Levy, P.T. Asphyxia, therapeutic hypothermia, and pulmonary hypertension. Clin. Perinatol. 2024, 51, 127–149. [Google Scholar] [CrossRef]
- Pastuszko, P.; Katz, M.G.; Ebel, T.; Bozek, V.; Kubin, L.; Kubin, J. Hypoxia-induced piglet model of cardiac arrest with assisted resuscitation by extracorporeal membrane oxygenation. Methods Mol. Biol. 2024, 2803, 227–237. [Google Scholar]
- Omairi, A.M.; Pandey, S. Targeted temperature management. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Sanches, E.F.; Carvalho, A.S.; van de Looij, Y.; Toulotte, A.; Wyse, A.T.; Netto, C.A.; Sizonenko, S.V. Experimental cerebral palsy causes microstructural brain damage in areas associated to motor deficits but no spatial memory impairments in the developing rat. Brain Res. 2021, 1761, 147389. [Google Scholar] [CrossRef]
- Theodorou, C.M.; Galganski, L.A.; Jurkovich, G.J.; Farmer, D.L.; Hirose, S.; Stephenson, J.T.; Trappey, A.F. Causes of early mortality in pediatric trauma patients. J. Trauma Acute Care Surg. 2021, 91, 523–529. [Google Scholar] [CrossRef]
- Machado, C. Jahi McMath: A new state of disorder of consciousness. J. Neurosurg. Sci. 2021, 65, 211–213. [Google Scholar] [CrossRef]
- Machado, C. Brain death diagnosis in primary posterior fossa lesions. J. Neurosurg. Sci. 2022, 70, 670–675. [Google Scholar] [CrossRef]
- Machado, C. The Jahi McMath case: First detailed study of her brain. Neurol. India 2022, 70, 2235–2236. [Google Scholar] [CrossRef] [PubMed]
- Shewmon, D.A.; Salamon, N. The MRI of Jahi McMath and its implications for the global ischemic penumbra hypothesis. J. Child Neurol. 2022, 37, 35–42. [Google Scholar] [CrossRef] [PubMed]
- Toplutas, E.; Aydin, F.; Hanoglu, L. EEG microstate analysis in patients with disorders of consciousness and its clinical significance. Brain Topogr. 2024, 37, 377–387. [Google Scholar] [CrossRef] [PubMed]
- Bernat, J.L. The Uniform Law Commission and the conceptual basis for brain death: The UDDA revision series. Neurology 2024, 102, e209157. [Google Scholar] [CrossRef]
- Giacino, J.T.; Katz, D.I.; Schiff, N.D.; Whyte, J.; Ashman, E.J.; Ashwal, S.; Barbano, R.; Hammond, F.M.; Laureys, S.; Ling, G.S.F.; et al. Practice guideline update recommendations summary: Disorders of consciousness. Neurology 2018, 91, 450–460. [Google Scholar] [CrossRef]
- Kazazian, K.; Monti, M.M.; Owen, A.M. Functional neuroimaging in disorders of consciousness: Towards clinical implementation. Brain 2025, awaf075. [Google Scholar] [CrossRef]
- Hannawi, Y.; Yanek, L.R.; Kral, B.G.; Becker, L.C.; Vaidya, D.; Nyquist, P.A. Association of the brain white matter hyperintensity with the cognitive performance in middle-aged population. Cerebrovasc. Dis. 2024, 631–638. [Google Scholar] [CrossRef]
- DeMertzi, A.; Antonopoulos, G.; Heine, L.; Voss, H.U.; Crone, J.S.; de Los Angeles, C.; Bahri, M.A.; Di Perri, C.; Vanhaudenhuyse, A.; Charland-Verville, V.; et al. Intrinsic functional connectivity differentiates minimally conscious from unresponsive patients. Brain 2015, 138, 2619–2631. [Google Scholar] [CrossRef]
- Kondziella, D.; Bender, A.; Diserens, K.; van Erp, W.; Estraneo, A.; Formisano, R.; Laureys, S.; Naccache, L.; Ozturk, S.; Rohaut, B.; et al. European Academy of Neurology guideline on the diagnosis of coma and other disorders of consciousness. Eur. J. Neurol. 2020, 27, 741–756. [Google Scholar] [CrossRef]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Published by MDPI on behalf of the Swiss Federation of Clinical Neuro-Societies. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).