
Effectiveness of a Multidisciplinary Headache Management Program: An Open-Label Pilot Study

 , , , and
, , , and
Abstract
1. Introduction
2. Materials and Methods
Statistical Analyses
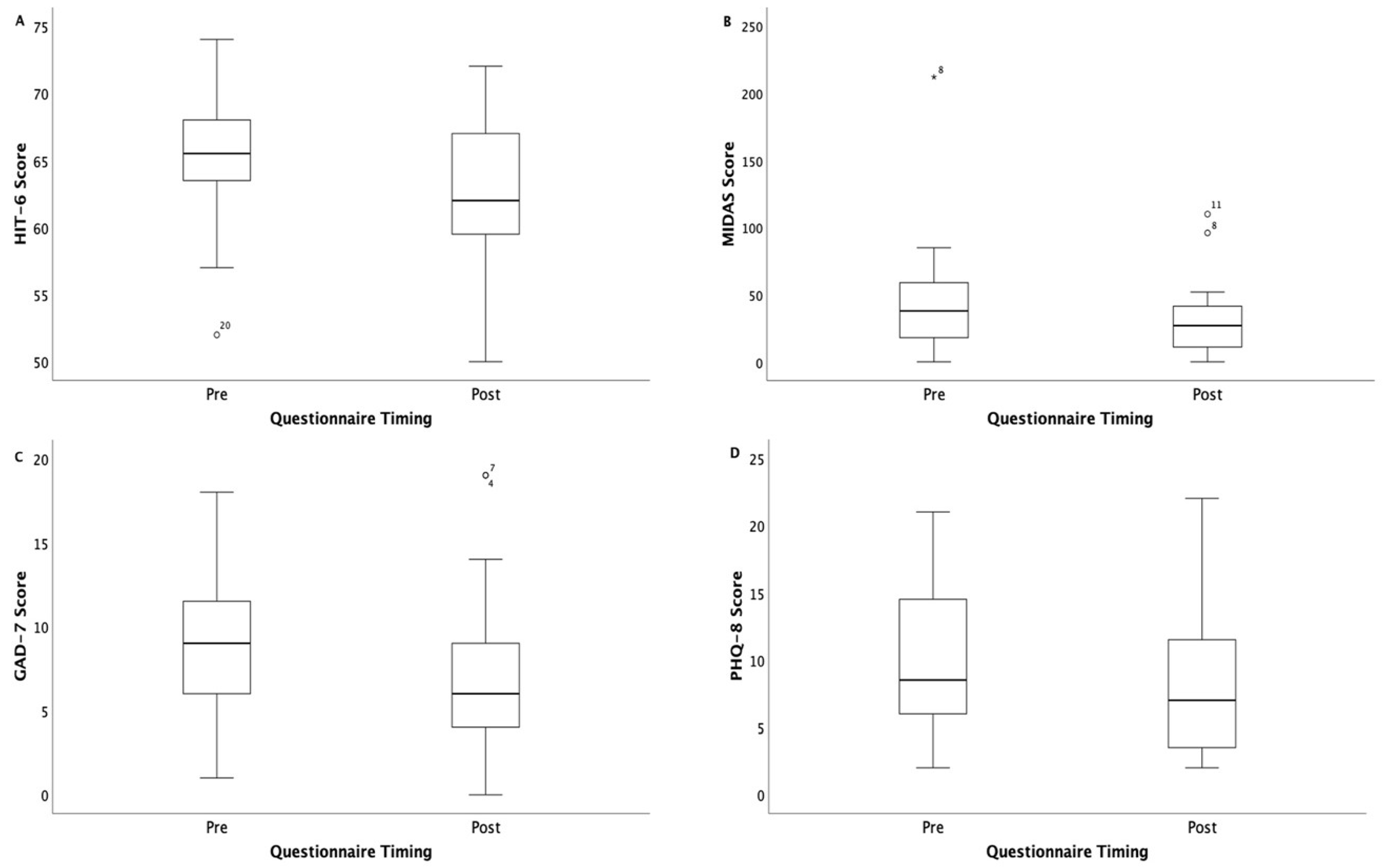
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| HIT-6 | Headache Impact Test 6 |
| MIDAS | Migraine Disability Assessment |
| GAD-7 | Generalized Anxiety Disorder 7-item scale |
| PHQ-8 | Eight-item Patient Health Questionnaire Depression Scale |
References
- Vos, T.; Lim, S.S.; Abbafati, C.; Abbas, K.M.; Abbasi, M.; Abbasifard, M.; Abbasi-Kangevari, M.; Abbastabar, H.; Abd-Allah, F.; Abdelalim, A.; et al. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1204–1222. [Google Scholar] [CrossRef] [PubMed]
- Barbanti, P.; Egeo, G.; Proietti, S.; d’Onofrio, F.; Aurilia, C.; Finocchi, C.; Di Clemente, L.; Zucco, M.; Doretti, A.; Messina, S.; et al. Assessing the Long-Term (48-Week) Effectiveness, Safety, and Tolerability of Fremanezumab in Migraine in Real Life: Insights from the Multicenter, Prospective, FRIEND3 Study. Neurol. Ther. 2024, 13, 611–624. [Google Scholar] [CrossRef] [PubMed]
- Bae, J.-Y.; Sung, H.-K.; Kwon, N.-Y.; Go, H.-Y.; Kim, T.-J.; Shin, S.-M.; Lee, S. Cognitive Behavioral Therapy for Migraine Headache: A Systematic Review and Meta-Analysis. Medicina 2022, 58, 44. [Google Scholar] [CrossRef]
- Ailani, J.; Burch, R.C.; Robbins, M.S. Board of Directors of the American Headache S. The American Headache Society Consensus Statement: Update on integrating new migraine treatments into clinical practice. Headache 2021, 61, 1021–1039. [Google Scholar] [CrossRef] [PubMed]
- Kropp, P.; Meyer, B.; Dresler, T.; Fritsche, G.; Gaul, C.; Niederberger, U.; Förderreuther, S.; Malzacher, V.; Jürgens, P.T.; Marziniak, M.; et al. Relaxation techniques and behavioural therapy for the treatment of migraine: Guidelines from the German Migraine and Headache Society. Schmerz 2017, 31, 433–447. [Google Scholar] [CrossRef]
- Stanos, S. Focused review of interdisciplinary pain rehabilitation programs for chronic pain management. Curr. Pain Headache Rep. 2012, 16, 147–152. [Google Scholar] [CrossRef]
- Gewirtz, A.; Minen, M. Adherence to Behavioral Therapy for Migraine: Knowledge to Date, Mechanisms for Assessing Adherence, and Methods for Improving Adherence. Curr. Pain Headache Rep. 2019, 23, 3. [Google Scholar] [CrossRef]
- Headache Classification Committee of the International Headache Society (IHS). The International Classification of Headache Disorders, 3rd edition. Cephalalgia 2018, 38, 1–211. [Google Scholar] [CrossRef]
- Rendas-Baum, R.; Yang, M.; Varon, S.F.; Bloudek, L.M.; DeGryse, R.E.; Kosinski, M. Validation of the Headache Impact Test (HIT6) in patients with chronic migraine. Health Qual. Life Outcomes 2014, 12, 1–10. [Google Scholar] [CrossRef]
- Haywood, K.L.; Mars, T.S.; Potter, R.; Patel, S.; Matharu, M.; Underwood, M. Assessing the impact of headaches and the outcomes of treatment: A systematic review of patient-reported outcome measures (PROMs). Cephalalgia 2018, 38, 1374–1386. [Google Scholar] [CrossRef]
- Martin, M.; Blaisdell, B.; Kwong, J.W.; Bjorner, J.B. The Short-Form Headache Impact Test (HIT-6) was psychometrically equivalent in nine languages. J. Clin. Epidemiol. 2004, 57, 1271–1278. [Google Scholar] [CrossRef]
- Kosinski, M. A six item short form survey for measuring headache impact the HIT6. Qual. Life Res. 2003, 12, 963–974. [Google Scholar] [CrossRef] [PubMed]
- Yang, M.; Rendas-Baum, R.; Varon, S.F.; Kosinski, M. Validation of the Headache Impact Test (HIT-6) across episodic and chronic migraine. Cephalalgia 2011, 31, 357–367. [Google Scholar] [CrossRef] [PubMed]
- Stewart, W.F. Validity of the Migraine Disability Assessment MIDAS score in comparison to a diary based measure in a population sample of migraine sufferers. Pain 2000, 88, 41–52. [Google Scholar] [CrossRef] [PubMed]
- Benz, T.; Lehmann, S.; Gantenbein, A.R.; Sandor, P.S.; Stewart, W.F.; Elfering, A.; Aeschlimann, A.G.; Angst, F. Translation, cross-cultural adaptation and reliability of the German version of the migraine disability assessment (MIDAS) questionnaire. Health Qual. Life Outcomes 2018, 16, 42. [Google Scholar] [CrossRef]
- Plummer, F.; Manea, L.; Trepel, D.; McMillan, D. Screening for anxiety disorders with the GAD-7 and GAD-2: A systematic review and diagnostic metaanalysis. Gen. Hosp. Psychiatry 2016, 39, 24–31. [Google Scholar] [CrossRef]
- Seo, J.G.; Park, S.P. Validation of the Generalized Anxiety Disorder-7 (GAD-7) and GAD-2 in patients with migraine. J. Headache Pain 2015, 16, 97. [Google Scholar] [CrossRef]
- Martin, A.; Rief, W.; Klaiberg, A.; Braehler, E. Validity of the Brief Patient Health Questionnaire Mood Scale (PHQ-9) in the general population. Gen. Hosp. Psychiatry 2006, 28, 71–77. [Google Scholar] [CrossRef]
- Seo, J.G.; Park, S.P. Validation of the Patient Health Questionnaire-9 (PHQ-9) and PHQ-2 in patients with migraine. J. Headache Pain 2015, 16, 65. [Google Scholar] [CrossRef]
- Shin, C.; Lee, S.H.; Han, K.M.; Yoon, H.K.; Han, C. Comparison of the Usefulness of the PHQ-8 and PHQ-9 for Screening for Major Depressive Disorder: Analysis of Psychiatric Outpatient Data. Psychiatry Investig. 2019, 16, 300–305. [Google Scholar] [CrossRef]
- Coeytaux, R.R.; Kaufman, J.S.; Chao, R.; Mann, J.D.; Devellis, R.F. Four methods of estimating the minimal important difference score were compared to establish a clinically significant change in Headache Impact Test. J. Clin. Epidemiol. 2006, 59, 374–380. [Google Scholar] [CrossRef] [PubMed]
- Smelt, A.F.; Assendelft, W.J.; Terwee, C.B.; Ferrari, M.D.; Blom, J.W. What is a clinically relevant change on the HIT-6 questionnaire? An estimation in a primary-care population of migraine patients. Cephalalgia 2014, 34, 29–36. [Google Scholar] [CrossRef] [PubMed]
- Carvalho, G.F.; Luedtke, K.; Braun, T. Minimal important change and responsiveness of the Migraine Disability Assessment Score (MIDAS) questionnaire. J. Headache Pain 2021, 22, 126. [Google Scholar] [CrossRef] [PubMed]
- Hussein, M.; Hassan, A.; Nada, M.A.F.; Mohammed, Z.; Abdel Ghaffar, N.F.; Kedah, H.; Fathy, W.; Magdy, R. Reliability, validity, and responsiveness of the Arabic version of HIT-6 questionnaire in patients with migraine indicated for preventive therapy: A multi-center study. Headache 2024, 64, 500–508. [Google Scholar] [CrossRef]
- Houts, C.R.; Wirth, R.J.; McGinley, J.S.; Cady, R.; Lipton, R.B. Determining Thresholds for Meaningful Change for the Headache Impact Test (HIT-6) Total and Item-Specific Scores in Chronic Migraine. Headache 2020, 60, 2003–2013. [Google Scholar] [CrossRef]
- Bromberg, J.; Wood, M.E.; Black, R.A.; Surette, D.A.; Zacharoff, K.L.; Chiauzzi, E.J. A randomized trial of a web-based intervention to improve migraine self-management and coping. Headache 2012, 52, 244–261. [Google Scholar] [CrossRef]
- Perlini, C.; Donisi, V.; Del Piccolo, L. From research to clinical practice: A systematic review of the implementation of psychological interventions for chronic headache in adults. BMC Health Serv. Res. 2020, 20, 459. [Google Scholar] [CrossRef]
- Kindelan-Calvo, P.; Gil-Martínez, A.; Paris-Alemany, A.; Pardo-Montero, J.; Muñoz-García, D.; Angulo-Díaz-Parreño, S.; Touche, R.L. Effectiveness of therapeutic patient education for adults with migraine. A systematic review and meta-analysis of randomized controlled trials. Pain Med. 2014, 15, 1619–1636. [Google Scholar] [CrossRef]
- Vetvik, K.G.; MacGregor, E.A. Sex differences in the epidemiology, clinical features, and pathophysiology of migraine. Lancet Neurol. 2017, 16, 76–87. [Google Scholar] [CrossRef]
- Steiner, T.J.; Stovner, L.J.; Jensen, R.; Uluduz, D.; Katsarava, Z. Lifting The Burden: The Global Campaign against H. Migraine remains second among the world’s causes of disability, and first among young women: Findings from GBD2019. J. Headache Pain 2020, 21, 137. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Lectures | Aims | Theoretical Foundation | |
|---|---|---|---|
| Week 1 | Understanding headaches | To increase the knowledge of what headaches are and the different type of headaches. | Information and education to increase knowledge and awareness. |
| Week 2 | Headache treatments | To understand the predisposition for headaches and to increase the knowledge about acute and prophylactic medications. | Knowledge about predisposition for headache and how acute and prophylactic treatment can streamline the therapeutic process. |
| Week 3 | Pain management, relaxation methods | To increase the knowledge of non-pharmacological interventions. | PMR, autogenic training, mindfulness-based stress reduction, biofeedback. |
| Week 4 | Stress | To understand the link between stress and migraine. | The physiological stress response can be a trigger for migraine attacks. |
| Week 5 | Sleep | To understand the relationship between sleep and migraine. | Prolonged or shortened sleep or a shift in the sleep–wake cycle can be a trigger for migraine attacks. |
| Week 6 | Physical activity | To understand the effects regular exercise can have on migraine attacks. | Moderate exercise can reduce the frequency and severity of migraine attacks. Regular exercise can be effective in preventing migraine. |
| Week 7 | Summary, including review and feedback | Summary of all lectures and to provide the opportunity for questions and feedback on the program. | Capture key points and facilitate efficient understanding and provide opportunities to share experiences and feedback. |
| Outcome Measures | Pre (M ± SD) | Post (M ± SD) | Mean Difference (95% CI) | p-Value |
|---|---|---|---|---|
| HIT-6 | 65.2 ± 4.8 | 61.9 ± 6.0 | 3.3 (0.14, 1.10) | 0.012 |
| PHQ-8 | 10.4 ± 5.8 | 8.3 ± 5.6 | 2.1 (0.18, 1.16) | 0.007 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Published by MDPI on behalf of the Swiss Federation of Clinical Neuro-Societies. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Souren, R.; Winteler, B.R.; Bischoff, N.; Fluri, O.; Grolimund, J.; Scutelnic, A.; Streitberger, K.; Beckwée, D.; Schankin, C.J. Effectiveness of a Multidisciplinary Headache Management Program: An Open-Label Pilot Study. Clin. Transl. Neurosci. 2025, 9, 27. https://doi.org/10.3390/ctn9020027
Souren R, Winteler BR, Bischoff N, Fluri O, Grolimund J, Scutelnic A, Streitberger K, Beckwée D, Schankin CJ. Effectiveness of a Multidisciplinary Headache Management Program: An Open-Label Pilot Study. Clinical and Translational Neuroscience. 2025; 9(2):27. https://doi.org/10.3390/ctn9020027
Chicago/Turabian StyleSouren, Rini, Balz Ronald Winteler, Nina Bischoff, Oliver Fluri, Johannes Grolimund, Adrian Scutelnic, Konrad Streitberger, David Beckwée, and Christoph J. Schankin. 2025. "Effectiveness of a Multidisciplinary Headache Management Program: An Open-Label Pilot Study" Clinical and Translational Neuroscience 9, no. 2: 27. https://doi.org/10.3390/ctn9020027
APA StyleSouren, R., Winteler, B. R., Bischoff, N., Fluri, O., Grolimund, J., Scutelnic, A., Streitberger, K., Beckwée, D., & Schankin, C. J. (2025). Effectiveness of a Multidisciplinary Headache Management Program: An Open-Label Pilot Study. Clinical and Translational Neuroscience, 9(2), 27. https://doi.org/10.3390/ctn9020027