
A Case Series of 39 United States Veterans with Mild Traumatic Brain Injury Treated with Hyperbaric Oxygen Therapy

 ,
,
Abstract
1. Introduction
2. Methods
2.1. Study Population
2.2. Overall Approach
2.3. Statistical and Data Analysis
3. Results
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Role of the Funder/Sponsor
References
- Department of Defense Numbers for Traumatic Brain Injury Worldwide Totals—2000–2022 Source: Defense Medical Surveillance System, Theater Medical Data Store, provided by the Armed Forces Health Surveillance Division. Provided by the Traumatic Brain Injury Center of Excellence. Available online: https://www.health.mil/Reference-Center/Reports/2022/08/24/2000-Q1-2022-DOD-Worldwide-Numbers-for-TBI (accessed on 2 February 2022).
- Koleda, E.W.; Beckman, R.L. The National Brain-Wounded Veteran Brain Drain: Cost-Benefit Analysis of Changing the DoD and VA Standard of Care for TBI and Suicide Prevention. TreatNOW Webs Site. Available online: https://treatnow.org/the-national-brain-wounded-veteran-brain-drain (accessed on 1 November 2021).
- Elsayed, N.M. Toxicology of blast overpressure. Toxicology 1997, 12, 1–15. [Google Scholar] [CrossRef]
- Lindquist, L.K.; Love, H.C.; Elbogen, E.B. Traumatic Brain Injury in Iraq and Afghanistan Veterans: New Results from a National Random Sample Study. J. Neuropsych. Clin. Neurosci. 2017, 29, 254–259. [Google Scholar] [CrossRef] [PubMed]
- Simpson, G.; Tate, R. Suicidality in people surviving a traumatic brain injury: Prevalence, risk factors, and implications for clinical management. Brain Inj. 2007, 21, 1335–1351. [Google Scholar] [CrossRef] [PubMed]
- Memorandum Assistant Secretary of Defense: Traumatic Brain Injury: Updated Definition and Reporting 4/6/2015. Available online: https://www.health.mil/Reference-Center/Policies/2015/04/06/Traumatic-Brain-Injury-Updated-Definition-and-Reporting (accessed on 2 February 2022).
- 2000–2020 Q4, as of Feb 16, 2021. DoD Numbers for Traumatic Brain Injury Worldwide Totals. Defense Medical Surveillance System (DMSS), Theater Medical Data Store (TMDS) Provided by the Armed Forces Health Surveillance Division (AFHSD). Prepared by the Traumatic Brain Injury Center of Excellence (TBICoE). Available online: https://health.mil/Reference-Center/Publications/2021/01/28/2000-Q3-2020-DoD-Worldwide-Numbers-for-TBI (accessed on 2 February 2022).
- Schweitzer, A.D.; Niogi, S.N.; Whitlow, C.J.; Tsiouris, A.J. Traumatic Brain Injury: Imaging Patterns and Complications. RadioGraphics 2019, 39, 1571–1595. [Google Scholar] [CrossRef]
- Douglas, D.B.; Ro, T.; Toffoli, T.; Krawchuk, B.; Muldermans, J.; Gullo, J.; Dulberger, A.; Anderson, A.E.; Douglas, P.K.; Wintermark, M. Neuroimaging of Traumatic Brain Injury. Med. Sci. 2018, 7, 2. [Google Scholar] [CrossRef]
- Douglas, D.B.; Chaudhari, R.; Zhao, J.M.; Gullo, J.; Kirkland, J.; Douglas, P.K.; Wolin, E.; Walroth, J.; Wintermark, M. Perfusion Imaging in Acute Traumatic Brain Injury. Neuroimaging Clin. North Am. 2017, 28, 55–65. [Google Scholar] [CrossRef]
- Masdeu, J.C.; Van Heertum, R.L.; Kleiman, A.; Anselmi, G.; Kissane, K.; Horng, J.; Yudd, A.; Luck, D.; Grundman, M. Early Single-Photon Emission Computed Tomography in Mild Head Trauma. J. Neuroimaging 1994, 4, 177–181. [Google Scholar] [CrossRef]
- Newton, M.R.; Greenwood, R.J.; Britton, K.E.; Charlesworth, M.; Nimmon, C.C.; Carroll, M.J.; Dolke, G. A study comparing SPECT with CT and MRI after closed head injury. J. Neurol. Neurosurg. Psychiatry 1992, 55, 92–94. [Google Scholar] [CrossRef]
- Stamatakis, E.A.; Wilson, J.T.L.; Hadley, N.M.; Wyper, D.J. SPECT imaging in head injury interpreted with statistical parametric mapping. J. Nucl. Med. 2002, 43, 476–483. [Google Scholar]
- Smith, L.G.F.; Milliron, E.; Ho, M.-L.; Hu, H.H.; Rusin, J.; Leonard, J.; Sribnick, E.A. Advanced neuroimaging in traumatic brain injury: An overview. Neurosurg. Focus 2019, 47, E17. [Google Scholar] [CrossRef]
- Bryan, C.J.; Clemans, T.A.; Hernandez, A.M.; Rudd, M.D. Loss of Consciousness, Depression, Posttraumatic Stress Disorder, and Suicide Risk Among Deployed Military Personnel with Mild Traumatic Brain Injury. J. Head Trauma Rehabil. 2013, 28, 13–20. [Google Scholar] [CrossRef] [PubMed]
- Hostetter, T.A.; Hoffmire, C.A.; Forster, J.E.; Adams, R.S.; Stearns-Yoder, K.A.; Brenner, L.A. Suicide and Traumatic Brain Injury Among Individuals Seeking Veterans Health Administration Services Between Fiscal Years 2006 and 2015. J. Head Trauma Rehabil. 2019, 34, E1–E9. [Google Scholar] [CrossRef] [PubMed]
- Greer, N.; Sayer, N.A.; Spoont, M.; Taylor, B.; Ackland, P.E.; Macdonald, R.; McKenzie, L.; Rosebush, C.; Wilt, T.J. Prevalence and Severity of Psychiatric Disorders and Suicidal Behavior in Service Members and Veterans with and Without Traumatic Brain Injury: Systematic Review. J. Head Trauma Rehabil. 2020, 35, 1–13. [Google Scholar] [CrossRef]
- Bryan, C.J.; Clemans, T.A. Repetitive Traumatic Brain Injury, Psychological Symptoms, and Suicide Risk in a Clinical Sample of Deployed Military Personnel. JAMA Psychiatry 2013, 70, 686–691. [Google Scholar] [CrossRef]
- Kemp, J.; Bossarte, R. Suicide Data Report, 2012. Department of Veterans Affairs, Mental Health Services, Suicide Prevention Program. Available online: https://www.va.gov/opa/docs/suicide-data-report-2012-final.pdf (accessed on 2 February 2022).
- Al-Waili, N.S.; Butler, G.J.; Beale, J.; Abdullah, M.S.; Hamilton, R.W.B.; Lee, B.Y.; Lucus, P.; Allen, M.W.W.; Petrillo, R.L.; Carrey, Z.; et al. Hyperbaric oxygen in the treatment of patients with cerebral stroke, brain trauma, and neurologic disease. Adv. Ther. 2005, 22, 659–678. [Google Scholar] [CrossRef] [PubMed]
- Raji, C.A.; Tarzwell, R.; Pavel, D.; Schneider, H.; Uszler, M.; Thornton, J.; Van Lierop, M.; Cohen, P.; Amen, D.G.; Henderson, T. Clinical Utility of SPECT Neuroimaging in the Diagnosis and Treatment of Traumatic Brain Injury: A Systematic Review. PLoS ONE 2014, 9, e91088. [Google Scholar] [CrossRef]
- Boussi-Gross, R.; Golan, H.; Fishlev, G.; Bechor, Y.; Volkov, O.; Bergan, J.; Friedman, M.; Hoofien, D.; Shlamkovitch, N.; Ben-Jacob, E.; et al. Hyperbaric Oxygen Therapy Can Improve Post Concussion Syndrome Years after Mild Traumatic Brain Injury—Randomized Prospective Trial. PLoS ONE 2013, 8, e79995. [Google Scholar] [CrossRef]
- Wang, F.; Wang, Y.; Sun, T.; Yu, H.-L. Hyperbaric oxygen therapy for the treatment of traumatic brain injury: A meta-analysis. Neurol. Sci. 2016, 37, 693–701. [Google Scholar] [CrossRef]
- Mozayeni, B.; Duncan, W.; Zant, E.; Love, T.; Beckman, R.; Stoller, K. The National Brain Injury Rescue and Rehabilitation Study—A multicenter observational study of hyperbaric oxygen for mild traumatic brain injury with post-concussive symptoms. Med. Gas Res. 2019, 9, 1–12. [Google Scholar] [CrossRef]
- Marshall, S.; Bayley, M.; Mccullagh, S.; Velikonja, D.; Berrigan, L.; Ouchterlony, D.; Weegar, K. Updated clinical practice guidelines for concussion/mild traumatic brain injury and persistent symptoms. Brain Inj. 2015, 29, 688–700. [Google Scholar] [CrossRef]
- Bramley, H.; Hong, J.; Zacko, C.; Royer, C.; Silvis, M. Mild Traumatic Brain Injury and Post-concussion Syndrome: Treatment and Related Sequela for Persistent Symptomatic Disease. Sports Med. Arthrosc. Rev. 2016, 24, 123–129. [Google Scholar] [CrossRef] [PubMed]
- Tal, S.; Hadanny, A.; Sasson, E.; Suzin, G.; Efrati, S. Hyperbaric Oxygen Therapy Can Induce Angiogenesis and Regeneration of Nerve Fibers in Traumatic Brain Injury Patients. Front. Hum. Neurosci. 2017, 11, 508. [Google Scholar] [CrossRef] [PubMed]
- Badr, A.E.; Yin, W.; Mychaskiw, G.; Zhang, J.H. Effect of hyperbaric oxygen on striatal metabolites: A microdialysis study in awake freely moving rats after MCA occlusion. Brain Res. 2001, 916, 85–90. [Google Scholar] [CrossRef]
- Calvert, J.W.; Yin, W.; Patel, M.; Badr, A.; Mychaskiw, G.; Parent, A.D.; Zhang, J.H. Hyperbaric oxygenation prevented brain injury induced by hypoxia–ischemia in a neonatal rat model. Brain Res. 2002, 951, 1–8. [Google Scholar] [CrossRef]
- Chirumamilla, S.; Sun, D.; Bullock, M.R.; Colello, R.J. Traumatic Brain Injury Induced Cell Proliferation in the Adult Mammalian Central Nervous System. J. Neurotrauma 2002, 19, 693–703. [Google Scholar] [CrossRef]
- Benson, R.M.; Minter, L.M.; Osborne, B.A.; Granowitz, E.V. Hyperbaric oxygen inhibits stimulus-induced proinflammatory cytokine synthesis by human blood-derived monocyte-macrophages. Clin. Exp. Immunol. 2003, 134, 57–62. [Google Scholar] [CrossRef]
- Dave, K.; Prado, R.; Busto, R.; Raval, A.; Bradley, W.; Torbati, D.; Pérez-Pinzón, M. Hyperbaric oxygen therapy protects against mitochondrial dysfunction and delays onset of motor neuron disease in wobbler mice. Neuroscience 2003, 120, 113–120. [Google Scholar] [CrossRef]
- Van Hulst, R.A.; Haitsma, J.J.; Klein, J.; Lachmann, B. Oxygen tension under hyperbaric conditions in healthy pig brain. Clin. Physiol. Funct. Imaging 2003, 23, 143–148. [Google Scholar] [CrossRef]
- Vlodavsky, E.; Palzur, E.; Soustiel, J.F. Hyperbaric oxygen therapy reduces neuroinflammation and expression of matrix metalloproteinase-9 in the rat model of traumatic brain injury. Neuropathol. Appl. Neurobiol. 2006, 32, 40–50. [Google Scholar] [CrossRef]
- Lin, K.-C.; Niu, K.-C.; Tsai, K.-J.; Kuo, J.-R.; Wang, L.-C.; Chio, C.-C.; Chang, C.-P. Attenuating inflammation but stimulating both angiogenesis and neurogenesis using hyperbaric oxygen in rats with traumatic brain injury. J. Trauma Inj. Infect. Crit. Care 2012, 72, 650–659. [Google Scholar] [CrossRef]
- Efrati, S.; Ben-Jacob, E. Reflections on the neurotherapeutic effects of hyperbaric oxygen. Expert Rev. Neurother. 2014, 14, 233–236. [Google Scholar] [CrossRef]
- Camporesi, E.M.; Bosco, G. Mechanisms of action of hyperbaric oxygen therapy. Undersea Hyperb. Med. J. Undersea Hyperb. Med. Soc. Inc. 2014, 41, 247–252. [Google Scholar]
- Zhang, J.H.; Lo, T.; Mychaskiw, G.; Colohan, A. Mechanisms of hyperbaric oxygen and neuroprotection in stroke. Pathophysiology 2005, 12, 63–77. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Chen, D.; Chen, G. Hyperbaric oxygen therapy applied research in traumatic brain injury: From mechanisms to clinical investigation. Med. Gas. Res. 2014, 4, 18. [Google Scholar] [CrossRef] [PubMed][Green Version]
- De Wolde, S.D.; Hulskes, R.H.; Weenink, R.P.; Hollmann, M.W.; Van Hulst, R.A. The Effects of Hyperbaric Oxygenation on Oxidative Stress, Inflammation and Angiogenesis. Biomolecules 2021, 11, 1210. [Google Scholar] [CrossRef]
- Hadanny, A.; Efrati, S. Treatment of persistent post-concussion syndrome due to mild traumatic brain injury: Current status and future directions. Expert Rev. Neurother. 2016, 16, 875–887. [Google Scholar] [CrossRef]
- Khalatbary, A.; Ahmadi, F. A review on the neuroprotective effects of hyperbaric oxygen therapy. Med. Gas. Res. 2021, 11, 72–82. [Google Scholar] [CrossRef]
- Eve, D.J.; Steele, M.R.; Sanberg, P.R.; Borlongan, C.V. Hyperbaric oxygen therapy as a potential treatment for post-traumatic stress disorder associated with traumatic brain injury. Neuropsychiatr. Dis. Treat. 2016, 12, 2689–2705. [Google Scholar] [CrossRef]
- Harch, P.G.; Andrews, S.R.; Fogarty, E.F.; Lucarini, J.; Van Meter, K.W. Case control study: Hyperbaric oxygen treatment of mild traumatic brain injury persistent post-concussion syndrome and post-traumatic stress disorder. Med. Gas. Res. 2017, 7, 156–174. [Google Scholar] [CrossRef]
- Hadanny, A.; Abbott, S.; Suzin, G.; Bechor, Y.; Efrati, S. Effect of hyperbaric oxygen therapy on chronic neurocognitive deficits of post-traumatic brain injury patients: Retrospective analysis. BMJ Open 2018, 8, e023387. [Google Scholar] [CrossRef]
- Wang, Y.-Z.; Li, T.-T.; Cao, H.-L.; Yang, W.-C. Recent advances in the neuroprotective effects of medical gases. Med. Gas. Res. 2019, 9, 80–87. [Google Scholar] [CrossRef] [PubMed]
- Shi, X.-Y.; Tang, Z.-Q.; Sun, D.; He, X.-J. Evaluation of hyperbaric oxygen treatment of neuropsychiatric disorders following traumatic brain injury. Chin. Med. J. 2006, 119, 1978–1982. [Google Scholar] [CrossRef] [PubMed]
- Mathieu, D.; Marroni, A.; Kot, J. Tenth European Consensus Conference on Hyperbaric Medicine: Recommendations for accepted and non-accepted clinical indications and practice of hyperbaric oxygen treatment. Diving Hyperb. Med. J. 2017, 47, 24–32. [Google Scholar] [CrossRef] [PubMed]
- Moon, R.E. (Ed.) Undersea and Hyperbaric Medical Society, Hyperbaric Oxygen Therapy Indications, 14th ed.; Best Publishing Company: North Palm Beach, FL, USA, 2019. [Google Scholar]
- Choudhury, R. Hypoxia and hyperbaric oxygen therapy: A review. Int. J. Gen. Med. 2018, 11, 431–442. [Google Scholar] [CrossRef]
- Efrati, S.; Fishlev, G.; Bechor, Y.; Volkov, O.; Bergan, J.; Kliakhandler, K.; Kamiager, I.; Gal, N.; Friedman, M.; Ben-Jacob, E.; et al. Hyperbaric Oxygen Induces Late Neuroplasticity in Post Stroke Patients—Randomized, Prospective Trial. PLoS ONE 2013, 8, e53716. [Google Scholar] [CrossRef]
- Boussi-Gross, R.; Golan, H.; Volkov, O.; Bechor, Y.; Hoofien, D.; Beeri, M.S.; Ben-Jacob, E.; Efrati, S. Improvement of memory impairments in poststroke patients by hyperbaric oxygen therapy. Neuropsychology 2015, 29, 610–621. [Google Scholar] [CrossRef]
- Daly, S.; Thorpe, M.; Rockswold, S.; Hubbard, M.; Bergman, T.; Samadani, U.; Rockswold, G. Hyperbaric Oxygen Therapy in the Treatment of Acute Severe Traumatic Brain Injury: A Systematic Review. J. Neurotrauma 2018, 35, 623–629. [Google Scholar] [CrossRef]
- Lansdorp, N.C.; Van Hulst, R.A. Double-blind trials in hyperbaric medicine: A narrative review on past experiences and considerations in designing sham hyperbaric treatment. Clin. Trials 2018, 15, 462–476. [Google Scholar] [CrossRef]
- Weaver, L.K.; Churchill, S.K.; Bell, J.; Deru, K.; Snow, G.L. A blinded trial to investigate whether ‘pressure-familiar’ individuals can determine chamber pressure. Undersea Hyperb. Med. 2012, 39, 801–805. [Google Scholar]
- Ren, H.; Wang, W.; Ge, Z.; Zhang, J. Clinical, brain electric earth map, endothelin and transcranial ultrasonic Doppler findings after hyperbaric oxygen treatment for severe brain injury. Chin. Med. J. 2001, 114, 387–390. [Google Scholar]
- Sunami, K.; Takeda, Y.; Hashimoto, M.; Hirakawa, M. Hyperbaric oxygen reduces infarct volume in rats by increasing oxygen supply to the ischemic periphery. Crit. Care Med. 2000, 28, 2831–2836. [Google Scholar] [CrossRef] [PubMed]
- Harch, P.G. Hyperbaric Oxygen Therapy for Post-Concussion Syndrome: Contradictory Conclusions from a Study Mischaracterized as Sham-Controlled. J. Neurotrauma 2013, 30, 1995–1999. [Google Scholar] [CrossRef] [PubMed]
- Efrati, S.; Golan, H.; Bechor, Y.; Faran, Y.; Daphna-Tekoah, S.; Sekler, G.; Fishlev, G.; Ablin, J.N.; Bergan, J.; Volkov, O.; et al. Hyperbaric Oxygen Therapy Can Diminish Fibromyalgia Syndrome—Prospective Clinical Trial. PLoS ONE 2015, 10, e0127012. [Google Scholar] [CrossRef] [PubMed]
- Hadanny, A.; Golan, H.; Fishlev, G.; Bechor, Y.; Volkov, O.; Suzin, G.; Ben-Jacob, E.; Efrati, S. Hyperbaric oxygen can induce neuroplasticity and improve cognitive functions of patients suffering from anoxic brain damage. Restor. Neurol. Neurosci. 2015, 33, 471–486. [Google Scholar] [CrossRef] [PubMed]
- Kahle, A.C.; Cooper, J.S. Hyperbaric, physiological, and pharmacological effects gases. In StatPearls; StatPearls Publishing LLC: Tampa, FL, USA, 2021. Available online: https://www.ncbi.nlm.nih.gov/books/NBK470481/ (accessed on 2 February 2022).
- Başar, E.; Düzgün, A. The CLAIR model: Extension of Brodmann areas based on brain oscillations and connectivity. Int. J. Psychophysiol. 2016, 103, 185–198. [Google Scholar] [CrossRef]
- Joint ACR–SPR (American College of Radiology-Society of Pediatric Radiology) Practice Guidelines for the Performance of Single Photon Emission Computed Tomography (SPECT) Brain Perfusion Imaging, including Brain Death Examinations. Available online: https://www.acr.org/-/media/ACR/Files/Practice-Parameters/BrainPerf-SPECT.pdf?la=en (accessed on 2 February 2022).
- Baker, S.M.; Bennett, P.; Bland, J.; Vasquez, A.; Galland, L.; Hedaya, R.J.; Houstion, M.; Hyman, M.; Lombard, J.; Rountree, R. Multiple Symptom Questionnaire. Textbook of Functional Medicine; Institute for Functional Medicine: Federal Way, WA, USA, 2010; pp. 838–839. ISBN 0977371379/9780977371372. [Google Scholar]
- Shabalin, A.A.; Hattab, M.W.; Clark, S.L.; Chan, R.F.; Kumar, G.; Aberg, K.A.; van den Oord, E.J.C.G. RaMWAS: Fast methylome-wide association study pipeline for enrichment platforms. Bioinformatics 2018, 34, 2283–2285. [Google Scholar] [CrossRef]
- Papademetris, X.; Scheinost, D. Talariach Converter with Broadmann Areas. BioImage Suite Web. NIH Brain Initiative under grant R24 MH114805. Available online: https://bioimagesuiteweb.github.io/webapp/mni2tal.html (accessed on 2 February 2022).
- Mena, F.; Mena, I.; Alamos, F.; Sole, C.; Neubauer, S. Normal data base of spect tc99m-hmpao brain perfusion AND Xe-133 rCBF in children, young adults and elderly. Clin. Nucl. Med. 1993, 18, 924. [Google Scholar] [CrossRef]
- Harch, P.G.; Fogarty, P.G.; Staab, P.K.; Van Meter, K. Low pressure hyperbaric oxygen therapy and SPECT brain imaging in the treatment of blast-induced chronic traumatic brain injury (post-concussion syndrome) and post traumatic stress disorder: A case report. Cases J. 2009, 2, 6538. [Google Scholar] [CrossRef]
- He, H.; Li, X.; He, Y. Hyperbaric oxygen therapy attenuates neuronal apoptosis induced by traumatic brain injury via Akt/GSK3β/β-catenin pathway. Neuropsychiatr. Dis. Treat. 2019, 15, 369–374. [Google Scholar] [CrossRef]
- Lindenmann, J.; Smolle, C.; Kamolz, L.-P.; Smolle-Juettner, F.M.; Graier, W.F. Survey of Molecular Mechanisms of Hyperbaric Oxygen in Tissue Repair. Int. J. Mol. Sci. 2021, 22, 11754. [Google Scholar] [CrossRef]
- Ma, J.; Hong, G.; Ha, E.; Hong, H.; Kim, J.; Joo, Y.; Yoon, S.; Lyoo, I.K.; Kim, J. Hippocampal cerebral blood flow increased following low-pressure hyperbaric oxygenation in firefighters with mild traumatic brain injury and emotional distress. Neurol. Sci. 2021, 42, 4131–4138. [Google Scholar] [CrossRef] [PubMed]
- Harch, P.G.; Andrews, S.R.; Rowe, C.J.; Lischka, J.R.; Townsend, M.H.; Yu, Q.; Mercante, D.E. Hyperbaric oxygen therapy for mild traumatic brain injury persistent postconcussion syndrome: A randomized controlled trial. Med. Gas Res. 2020, 10, 8–20. [Google Scholar] [CrossRef] [PubMed]
- Hart, B.B.; Weaver, L.K.; Gupta, A.; Wilson, S.H.; Vijayarangan, A.; Deru, K.; Hebert, D. Hyperbaric oxygen for mTBI-associated PCS and PTSD: Pooled analysis of results from Department of Defense and other published studies. Undersea Hyperb. Med. 2019, 46, 353–383. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Veteran | Initial MSQ | 20th Tx MSQ | 40th Tx MSQ | Last Tx |
|---|---|---|---|---|
| 1 | 107 | 77 | 56 | 8/8/2017 |
| 2 | 26 | 25 | 14 | 10/12/2018 |
| 3 | 85 | 21 | 11 | 5/1/2018 |
| 4 | 126 | 57 | 41 | 11/17/2017 |
| 5 | 129 | 67 | 21 | 2/8/2017 |
| 6 | 110 | 73 | 40 | 9/21/2017 |
| 7 | 41 | 24 | 17 | 2/16/2017 |
| 8 | 65 | 34 | 10 | 11/30/2017 |
| 9 | 94 | 38 | 16 | 8/20/2018 |
| 10 | 64 | 63 | 42 | 12/27/2018 |
| 11 | 15 | 24 | 16 | 2/4/2019 |
| 12 | 33 | 21 | 19 | 2/25/2019 |
| 13 | 21 | 64 | 23 | 10/12/2018 |
| 14 | 101 | 73 | 55 | 10/15/2018 |
| 15 | 37 | 39 | 37 | 3/22/2019 |
| 16 | 160 | 154 | 154 | 3/20/2019 |
| 17 | 106 | 49 | 31 | 3/25/2019 |
| 18 | 56 | 36 | 27 | 4/23/2019 |
| 19 | 97 | 70 | 57 | 4/24/2019 |
| 20 | 29 | 22 | 17 | 5/22/2019 |
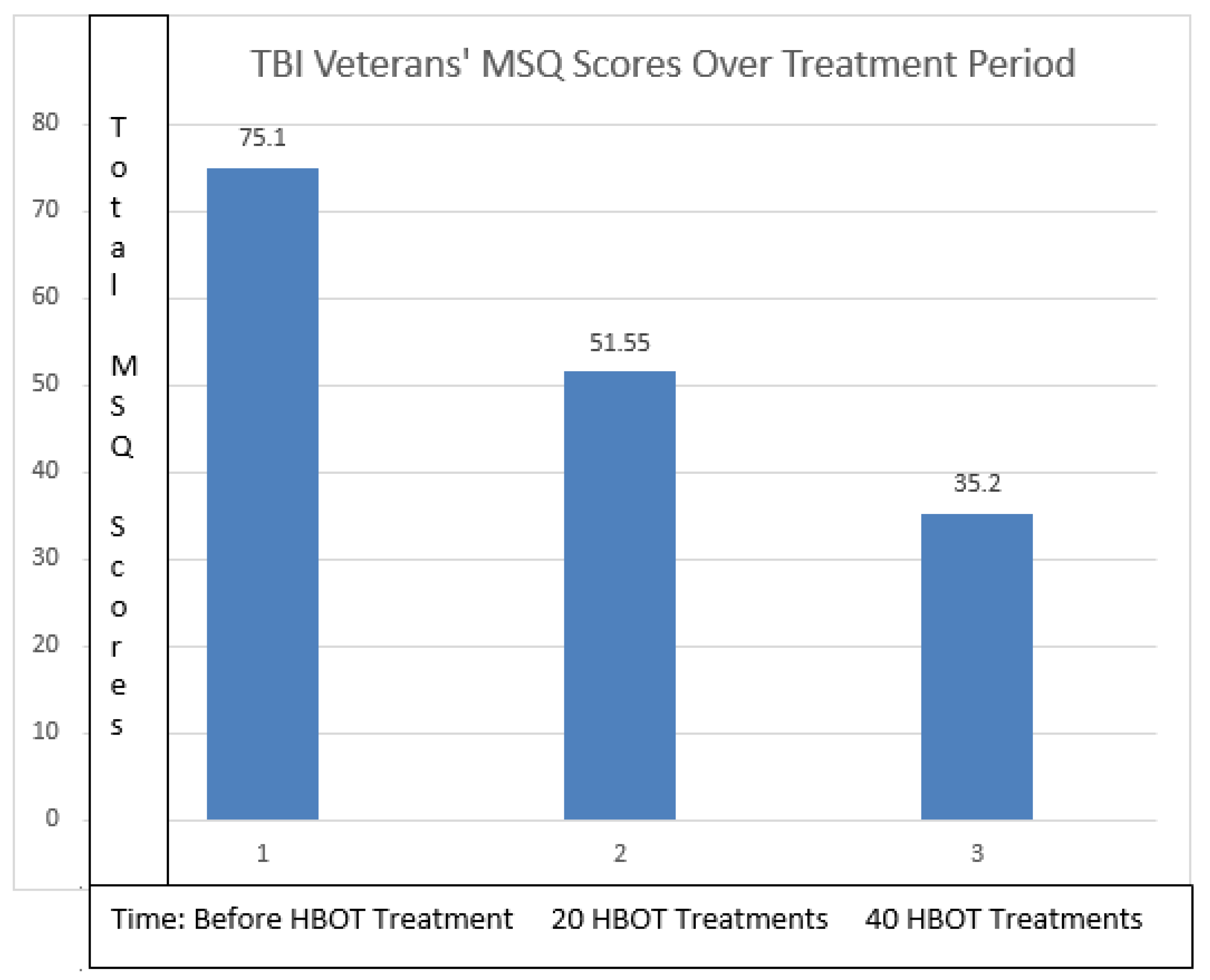
| Mean | 75.1 | 51.55 | 35.2 | |
| Std. Deviation | 42.0224251 | 31.47175 | 31.86088 |
| Paired Samples Test | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Paired Differences | t | df | Significance | |||||||
| Mean | Std. Deviation | Std. Error Mean | 95% Confidence Interval of the Difference | One-Sided p | Two-Sided p | |||||
| Lower | Upper | |||||||||
| Pair 1 | Initial MSQ—40th Tx MSQ | 39.90000 | 33.16768 | 7.41652 | 24.37705 | 55.42295 | 5.380 | 19 | 0.000 | 0.000 |
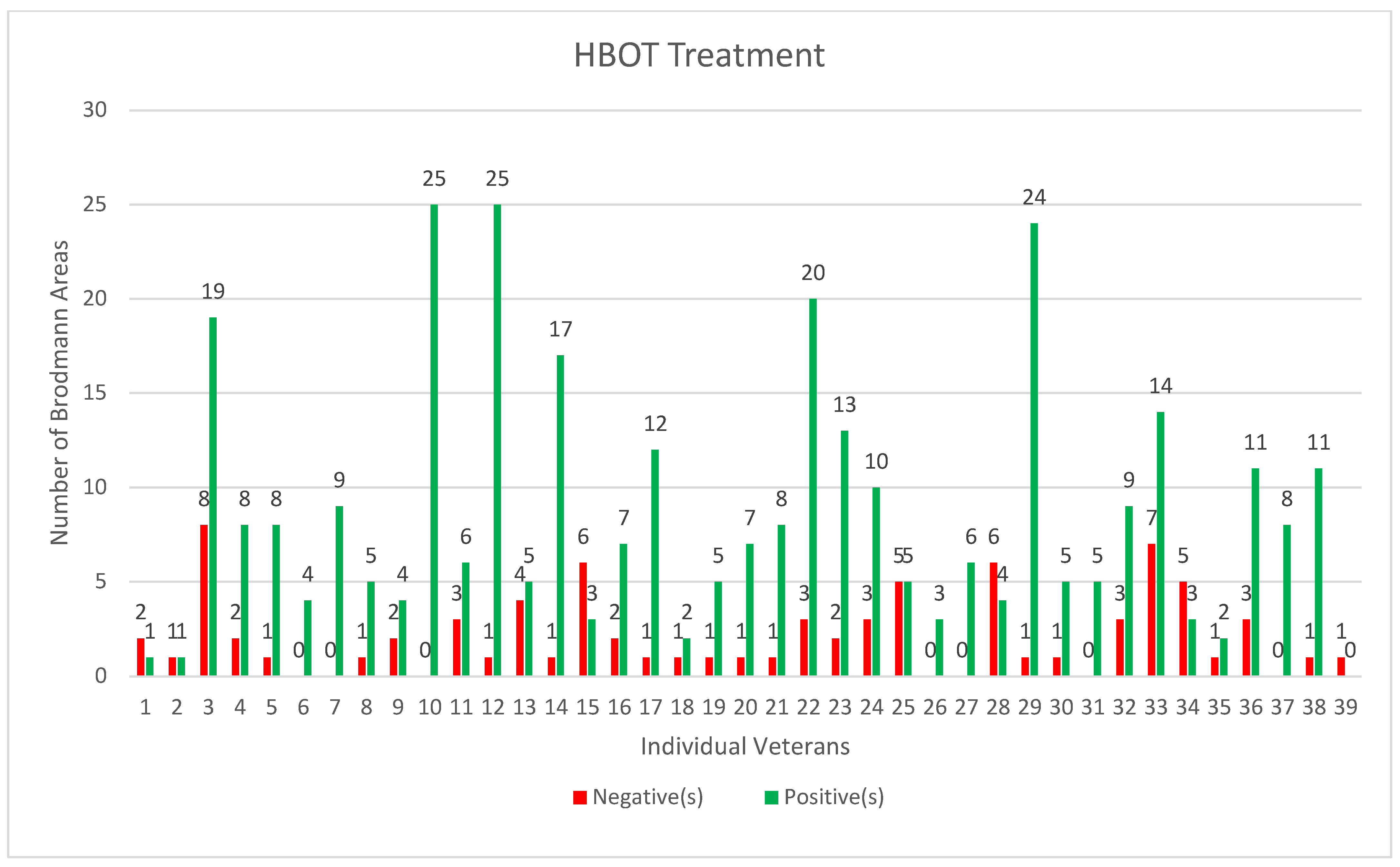
| Pre-HBOT | Post-HBOT | Change | p Value | |
|---|---|---|---|---|
| Brodmann Area Mean Value | −1.65 | −1.35 | 0.29 | <0.001 |
| Std Dev | 1.45 | 1.46 | --- | |
| Std Err Mean | 0.03 | 0.03 | 0.01 | |
| Upper 95% Mean | −1.60 | −1.30 | 0.32 | |
| Lower 95% Mean | −1.70 | −1.41 | 0.26 | |
| N | 2904 | 2904 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bested, A.C.; Rana, A.M.; Hardigan, P.; Niyirora, J.; Cheema, A.; Antony, G.; Defina, P.A.; Machado, C. A Case Series of 39 United States Veterans with Mild Traumatic Brain Injury Treated with Hyperbaric Oxygen Therapy. Clin. Transl. Neurosci. 2022, 6, 21. https://doi.org/10.3390/ctn6030021
Bested AC, Rana AM, Hardigan P, Niyirora J, Cheema A, Antony G, Defina PA, Machado C. A Case Series of 39 United States Veterans with Mild Traumatic Brain Injury Treated with Hyperbaric Oxygen Therapy. Clinical and Translational Neuroscience. 2022; 6(3):21. https://doi.org/10.3390/ctn6030021
Chicago/Turabian StyleBested, Alison C., Arif M. Rana, Patrick Hardigan, Jerome Niyirora, Amanpreet Cheema, George Antony, Philip A. Defina, and Calixto Machado. 2022. "A Case Series of 39 United States Veterans with Mild Traumatic Brain Injury Treated with Hyperbaric Oxygen Therapy" Clinical and Translational Neuroscience 6, no. 3: 21. https://doi.org/10.3390/ctn6030021
APA StyleBested, A. C., Rana, A. M., Hardigan, P., Niyirora, J., Cheema, A., Antony, G., Defina, P. A., & Machado, C. (2022). A Case Series of 39 United States Veterans with Mild Traumatic Brain Injury Treated with Hyperbaric Oxygen Therapy. Clinical and Translational Neuroscience, 6(3), 21. https://doi.org/10.3390/ctn6030021