Using Agent-Based Modeling to Understand the Emergence and Reproduction of Social Inequalities in Health †



Abstract
:1. Introduction
2. Material and Methods
2.1. Data
2.2. ABM Scenarios
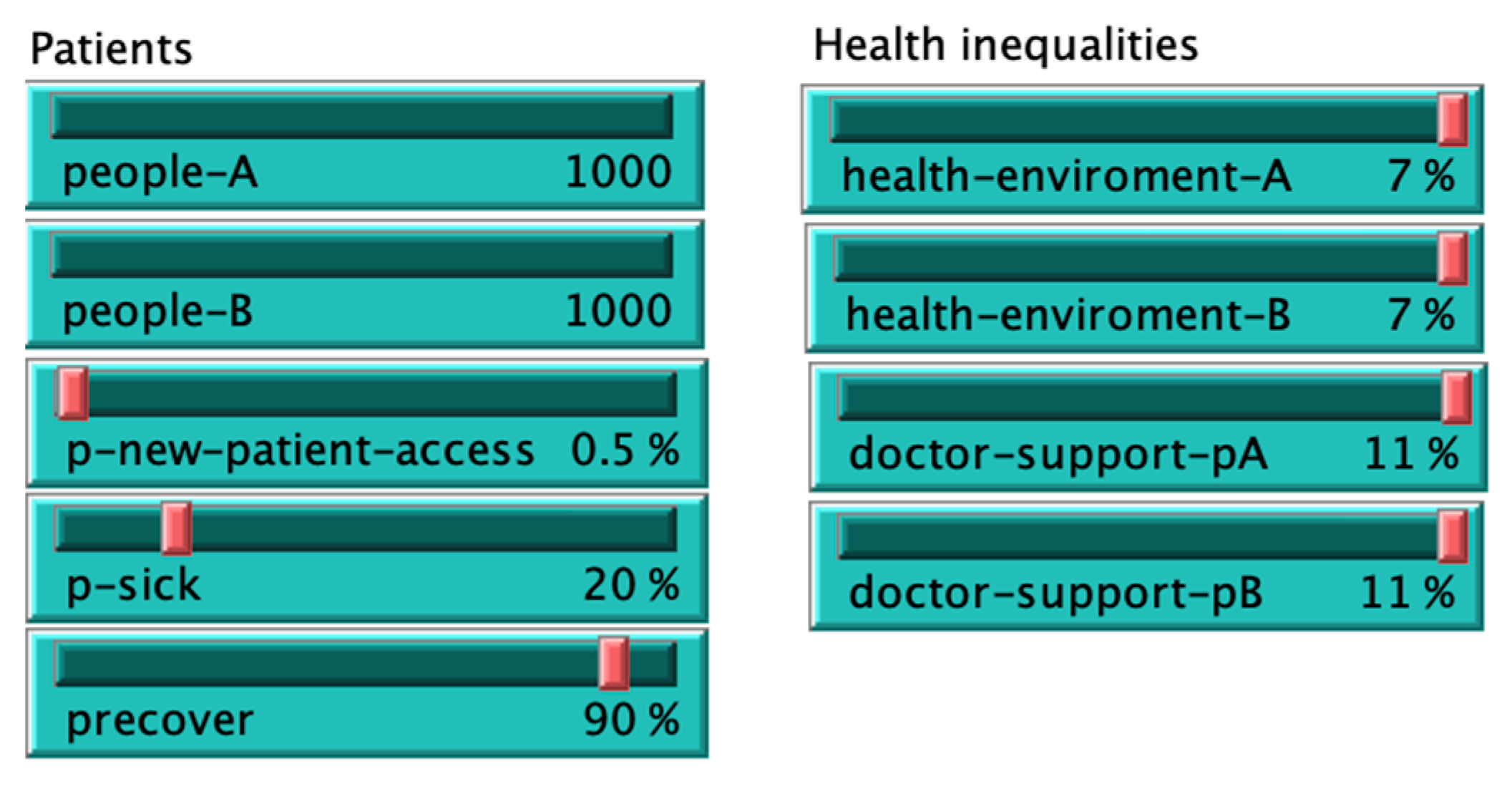
2.3. Model Specification
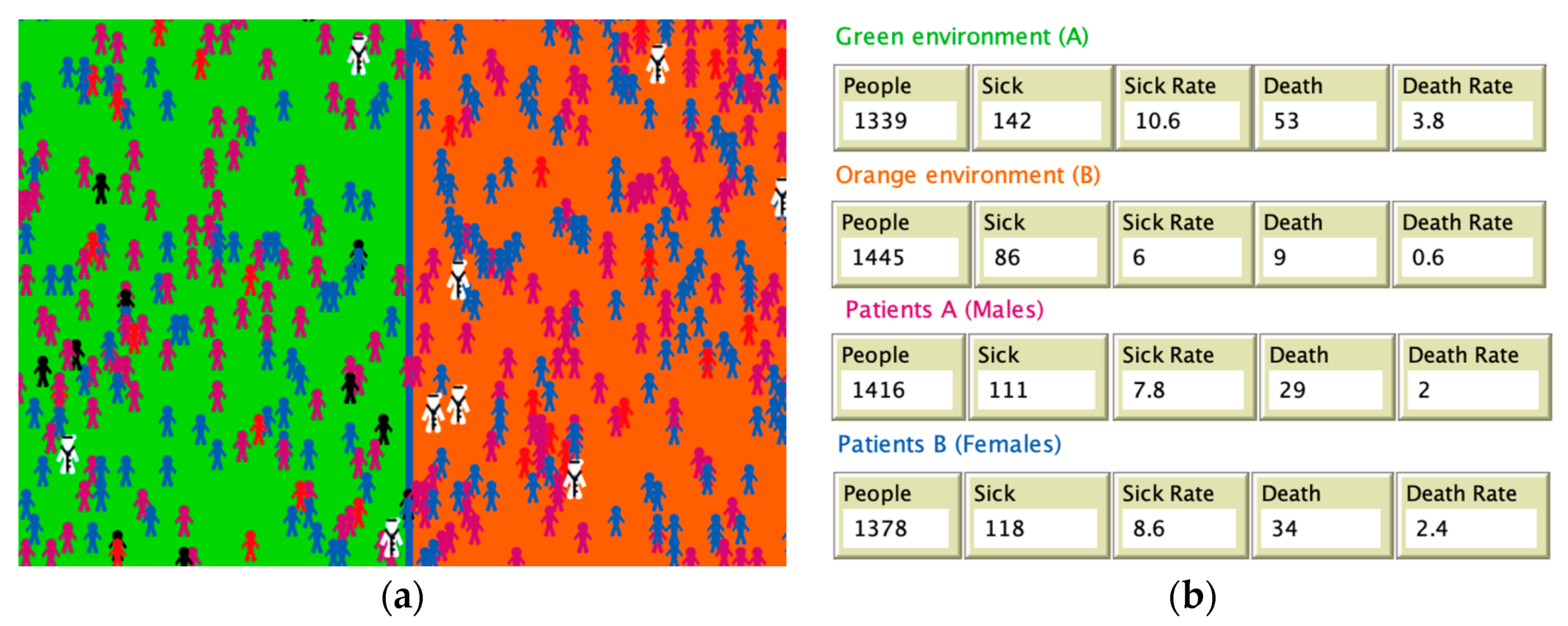
3. Results
3.1. Sick and Death Rates
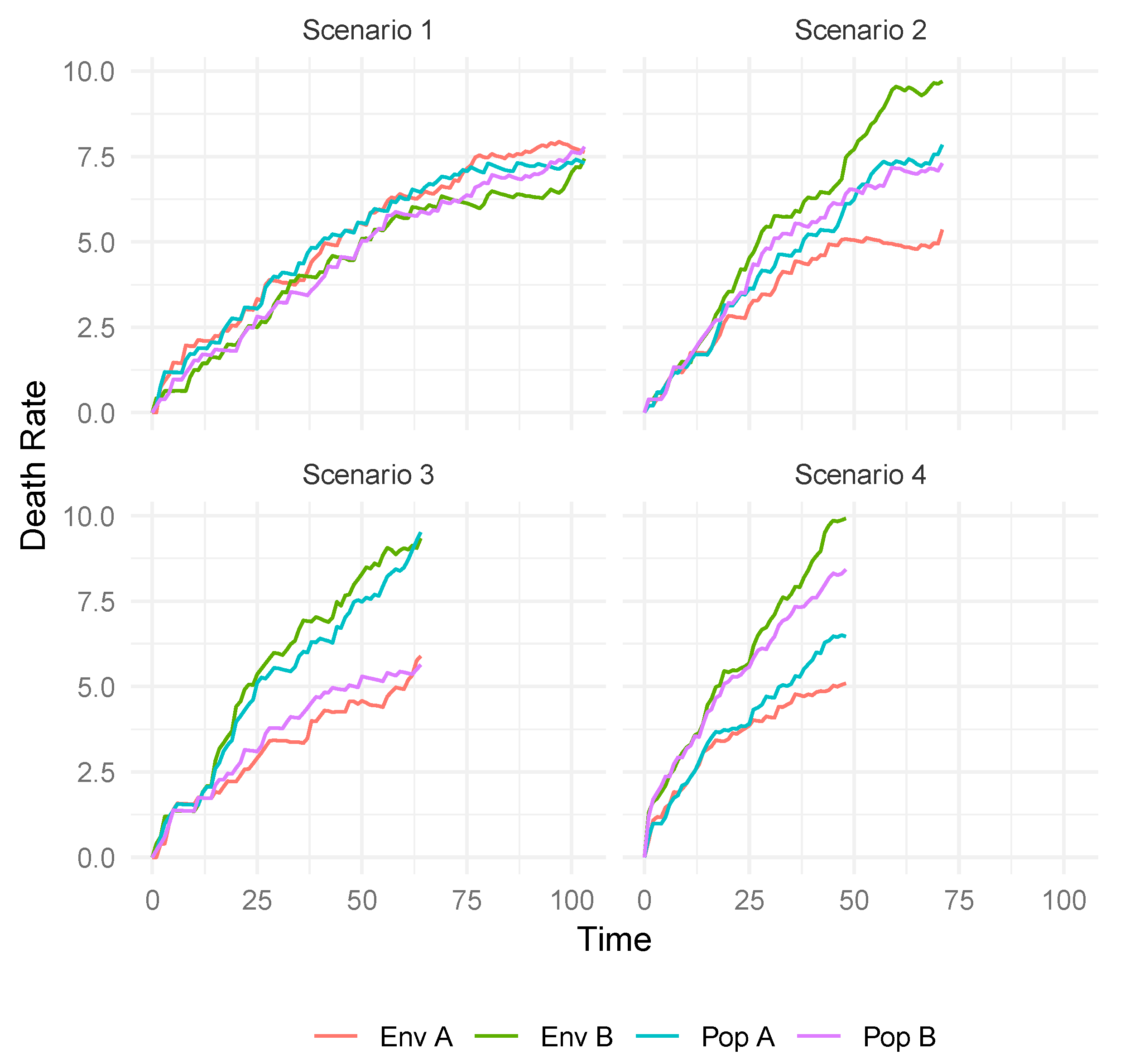
3.2. Mortality Patterns in Four Simulated Scenarios
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Rutter, H.; Savona, N.; Glonti, K.; Bibby, J.; Cummins, S.; Finegood, D.T.; Greaves, F.; Harper, L.; Hawe, P.; Moore, L.; et al. The need for a complex systems model of evidence for public health. Lancet 2017, 390, 2602–2604. [Google Scholar] [CrossRef]
- Wilkinson, R.G.; Marmot, M. (Eds.) Social Determinants of Health: The Solid Facts; WHO Regional Office for Europe: Copenhagen, Denmark, 2003. [Google Scholar]
- Alvarez-Galvez, J.; Suarez-Lledo, V.; Martinez-Cousinou, G.; Muniategui-Azkona, E.; Gonzalez-Portillo, A. The impact of financial crisis and austerity policies in Andalusia, Spain: Disentangling the mechanisms of social inequalities in health through the perceptions and experiences of experts and the general population. Int. J. Equity Health 2019, 18, 108. [Google Scholar] [CrossRef] [PubMed]
- Alvarez-Galvez, J.; Jaime-Castillo, A.M. The impact of social expenditure on health inequalities in Europe. Soc. Sci. Med. 2018, 200, 9–18. [Google Scholar] [CrossRef] [PubMed]
- MacKenbach, J.P. The persistence of health inequalities in modern welfare states: The explanation of a paradox. Soc. Sci. Med. 2012, 75, 761–769. [Google Scholar] [CrossRef] [PubMed]
- Speybroeck, N.; Van Malderen, C.; Harper, S.; Müller, B.; Devleesschauwer, B. Simulation Models for Socioeconomic Inequalities in Health: A Systematic Review. Int. J. Environ. Res. Public Health 2013, 10, 5750–5780. [Google Scholar] [CrossRef] [PubMed]
- Alvarez-Galvez, J. Discovering complex interrelationships between socioeconomic status and health in Europe: A case study applying Bayesian Networks. Soc. Sci. Res. 2016, 56, 133–143. [Google Scholar] [CrossRef] [PubMed]
- Galea, S.; Riddle, M.; Kaplan, G.A. Causal thinking and complex system approaches in epidemiology. Int. J. Epidemiol. 2010, 39, 97–106. [Google Scholar] [CrossRef] [PubMed]
- ESS Round 7: European Social Survey Round 7 Data; Data File Edition 2.2; NSD—Norwegian Centre for Research Data: Bergen, Norway, 2014. [CrossRef]
- Yang, Y.; Roux, A.V.D.; Auchincloss, A.H.; Rodriguez, D.; Brown, D. Exploring walking differences by socioeconomic status using a spatial agent-based model. Health Place 2012, 18, 96–99. [Google Scholar] [CrossRef] [PubMed]
- Alvarez-Galvez, J. Computational Simulation Methods. In The International Encyclopedia of Communication Research Methods; Wiley: Hoboken, NJ, USA, 2017; Volume 1–11. [Google Scholar]
- Diaz, R.; Behr, J.G.; Tulpule, M. A System Dynamics Model for Simulating Ambulatory Health Care Demands. Simul. Healthc. J. Soc. Simul. Healthc. 2012, 7, 243–250. [Google Scholar] [CrossRef] [PubMed]
- Auchincloss, A.H.; Riolo, R.L.; Brown, D.; Cook, J.; Roux, A.V.D. An Agent-Based Model of Income Inequalities in Diet in the Context of Residential Segregation. Am. J. Prev. Med. 2011, 40, 303–311. [Google Scholar] [CrossRef] [PubMed]
- Alvarez-Galvez, J. Network models of minority opinion spreading: Using agent-based modeling to study possible scenarios of social contagion. Soc. Sci. Comput. Rev. 2016, 34, 567–581. [Google Scholar] [CrossRef]
- Mahamoud, A.; Roche, B.; Homer, J. Modelling the social determinants of health and simulating short-term and long-term intervention impacts for the city of Toronto, Canada. Soc. Sci. Med. 2013, 93, 247–255. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ID | Variables | Measure | Effect Size |
|---|---|---|---|
| 1 | Genetic/biological | Initial health | 22% |
| 2 | Environmental | Exposure | 7% |
| 3 | Health care | Accessibility | 11% |
| 4 | Social/behavioral | Survey data | 60% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alvarez-Galvez, J.; Suarez-Lledo, V. Using Agent-Based Modeling to Understand the Emergence and Reproduction of Social Inequalities in Health. Proceedings 2020, 44, 2. https://doi.org/10.3390/IECEHS-2-06372
Alvarez-Galvez J, Suarez-Lledo V. Using Agent-Based Modeling to Understand the Emergence and Reproduction of Social Inequalities in Health. Proceedings. 2020; 44(1):2. https://doi.org/10.3390/IECEHS-2-06372
Chicago/Turabian StyleAlvarez-Galvez, Javier, and Victor Suarez-Lledo. 2020. "Using Agent-Based Modeling to Understand the Emergence and Reproduction of Social Inequalities in Health" Proceedings 44, no. 1: 2. https://doi.org/10.3390/IECEHS-2-06372
APA StyleAlvarez-Galvez, J., & Suarez-Lledo, V. (2020). Using Agent-Based Modeling to Understand the Emergence and Reproduction of Social Inequalities in Health. Proceedings, 44(1), 2. https://doi.org/10.3390/IECEHS-2-06372