

Deep Learning for Leukemia Classification: Performance Analysis and Challenges Across Multiple Architectures

 ,
,  , , , and
, , , and
Abstract
1. Introduction
2. Literature Review
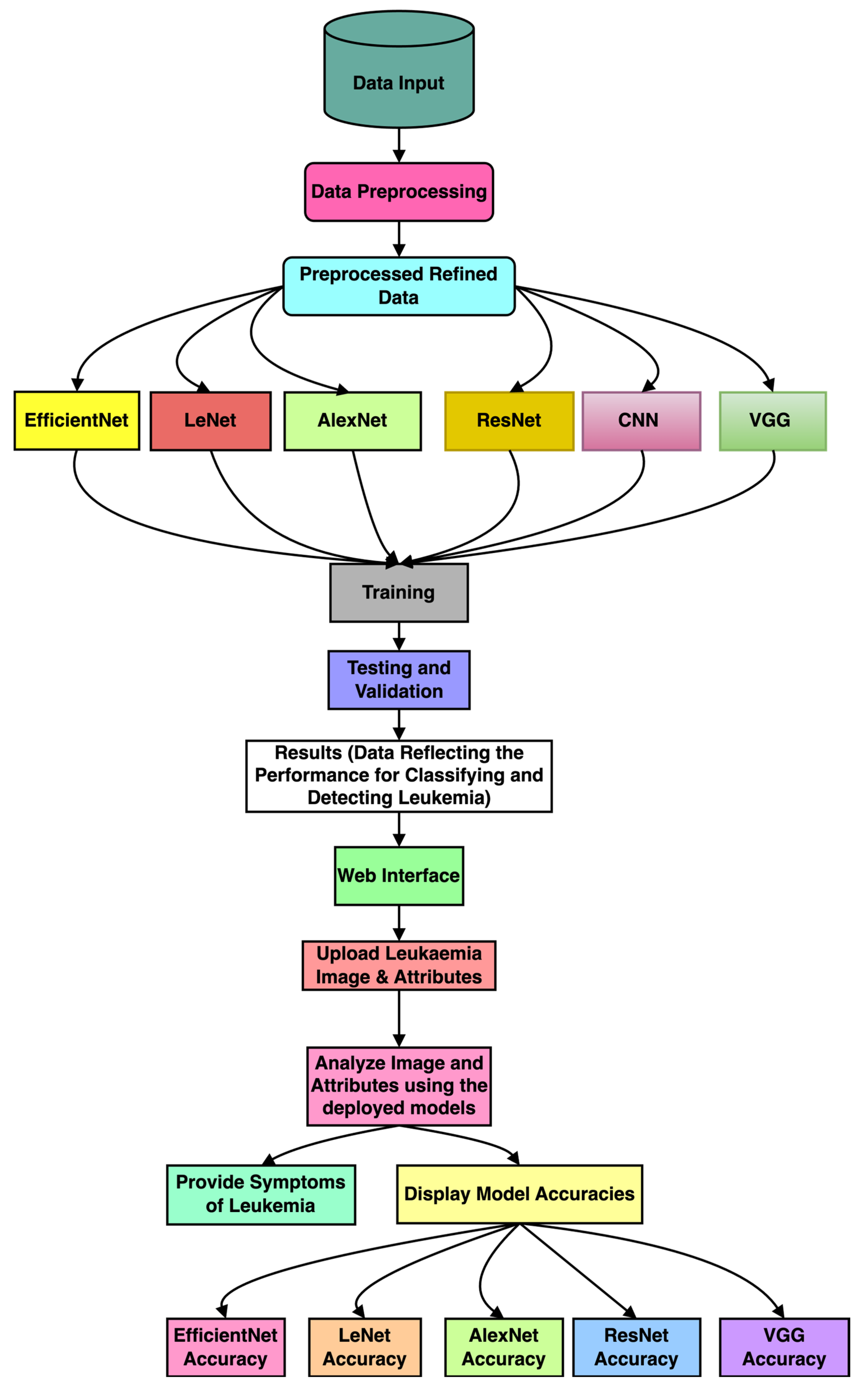
3. Methodology
3.1. Preprocessing
3.2. Selection of Optimal Deep Learning Architectures for Leukemia Detection
3.2.1. VGG (Visual Geometry Group)
3.2.2. EfficientNet
3.2.3. LeNet
3.2.4. AlexNet
3.2.5. Convolutional Neural Networks (CNNs)
3.2.6. ResNet (Residual Network)
3.3. Feature Extraction and Representation
3.4. Model Training, Validation, and Evaluation
3.5. Interpretability and Visualization
4. Experimental Results
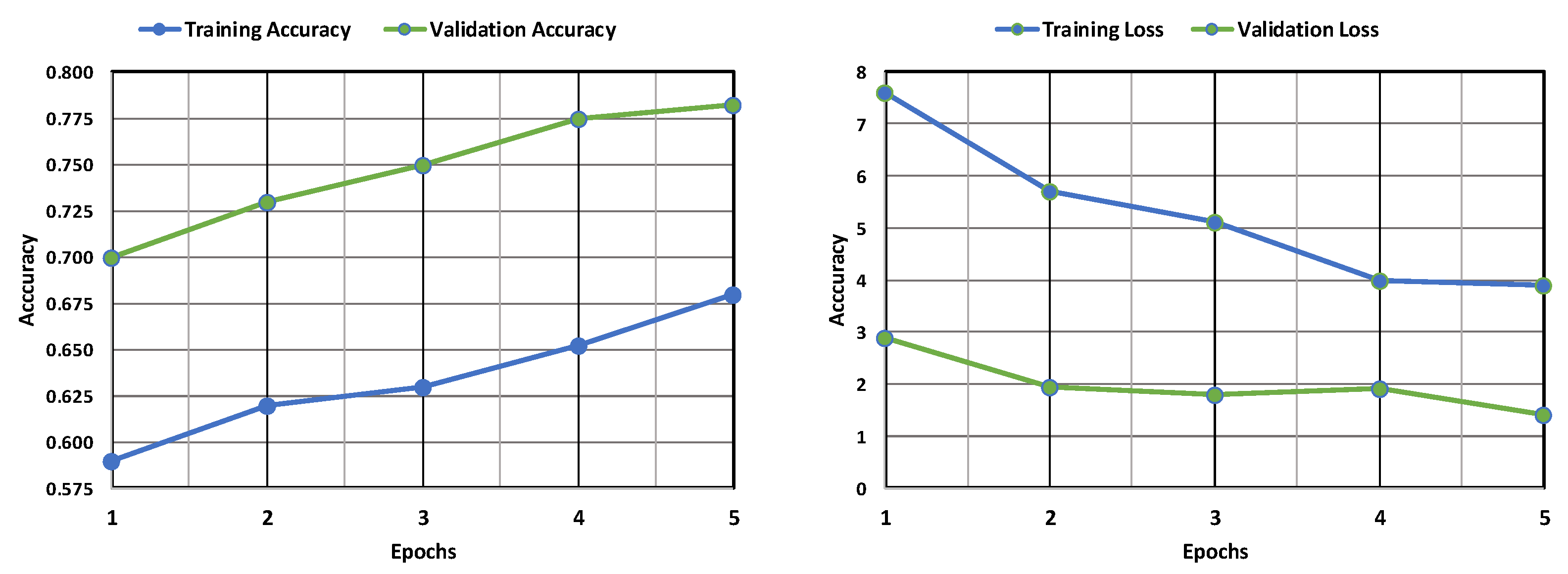
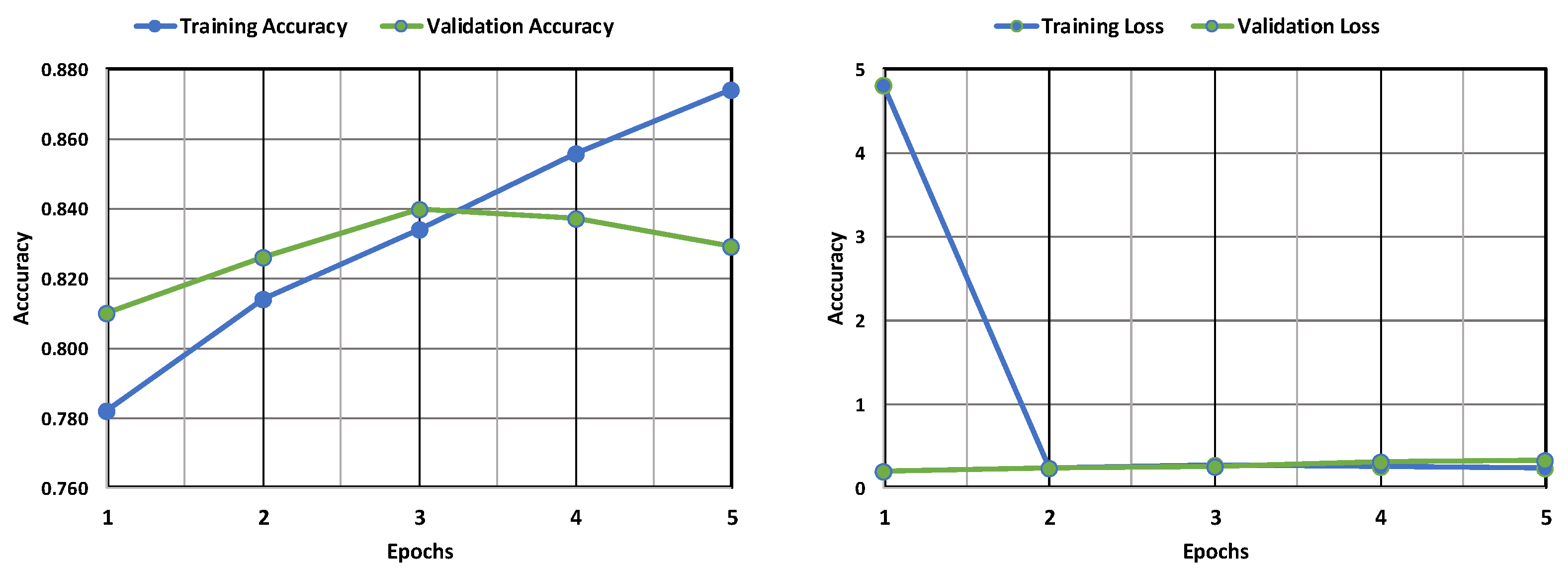
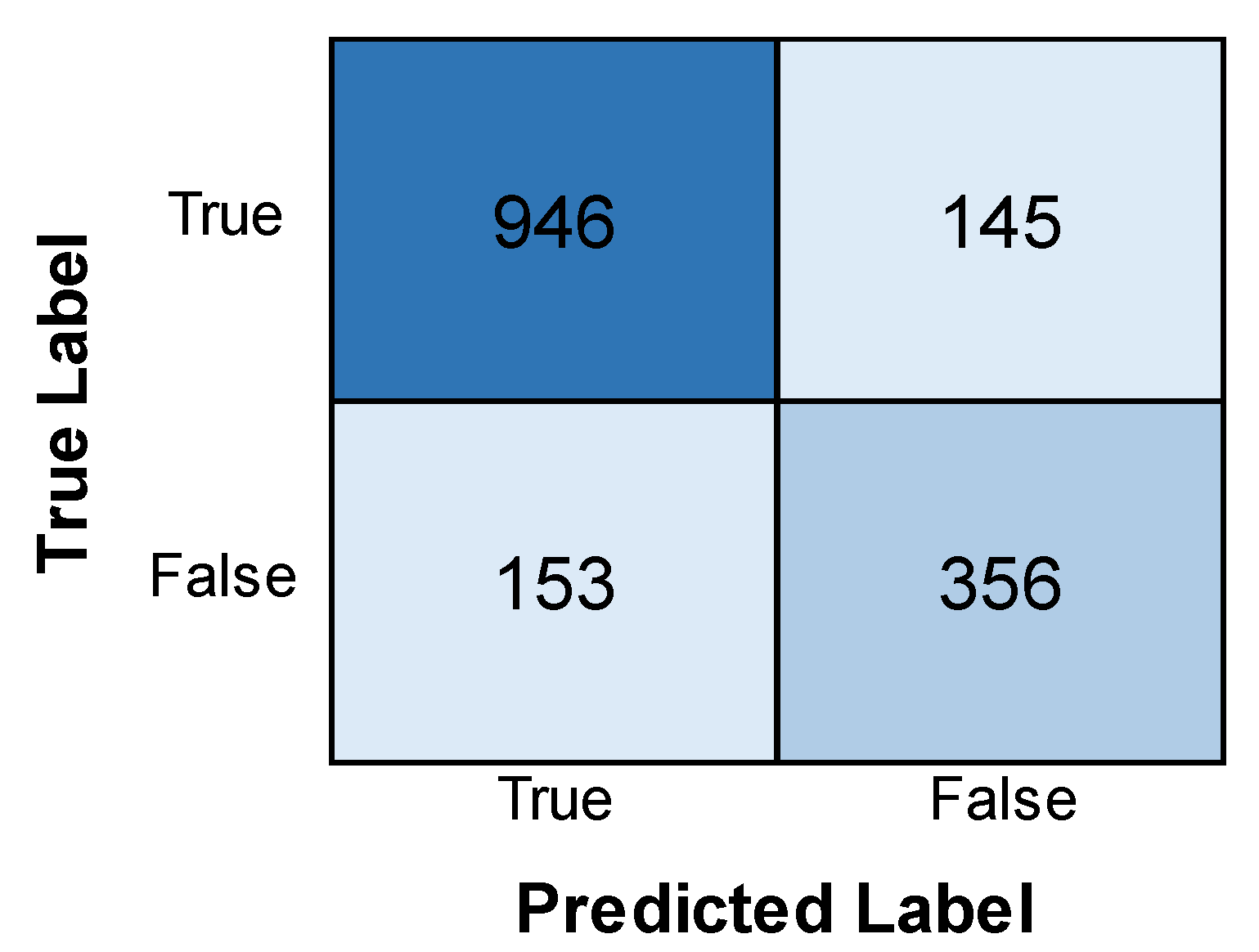
4.1. VGG Model Performance
4.2. EfficientNet Model Performance
4.3. LeNet Model Performance
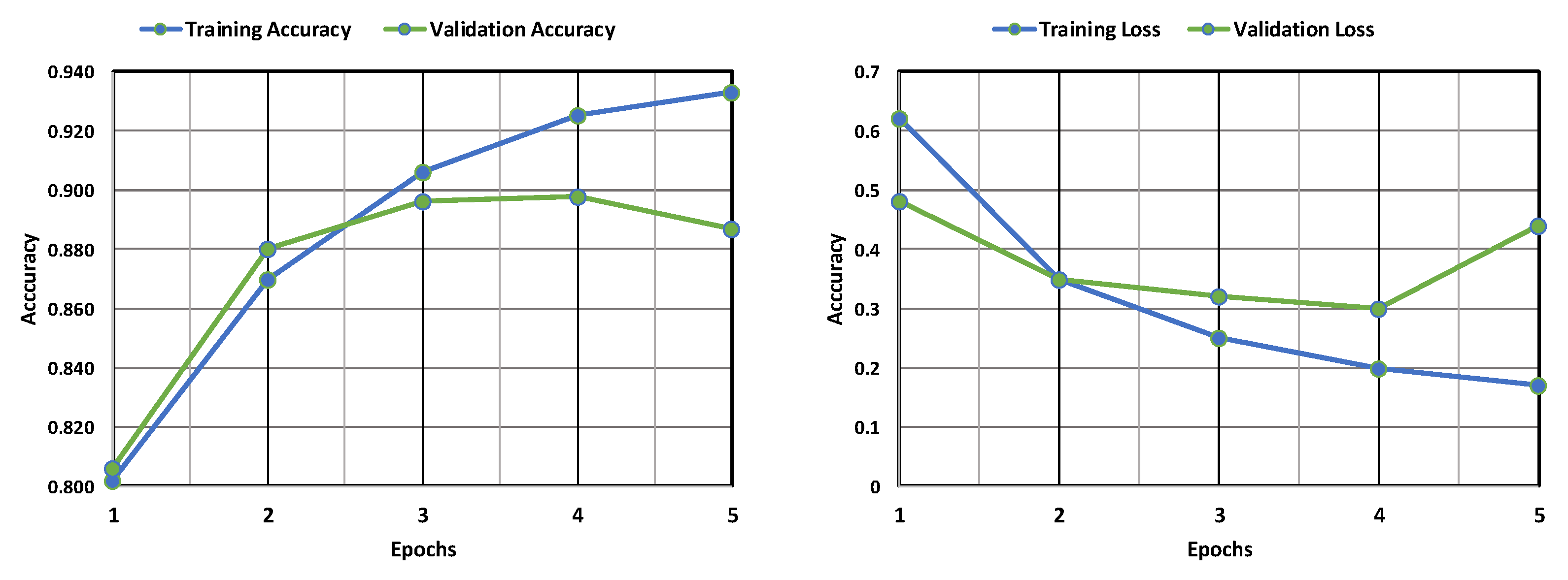
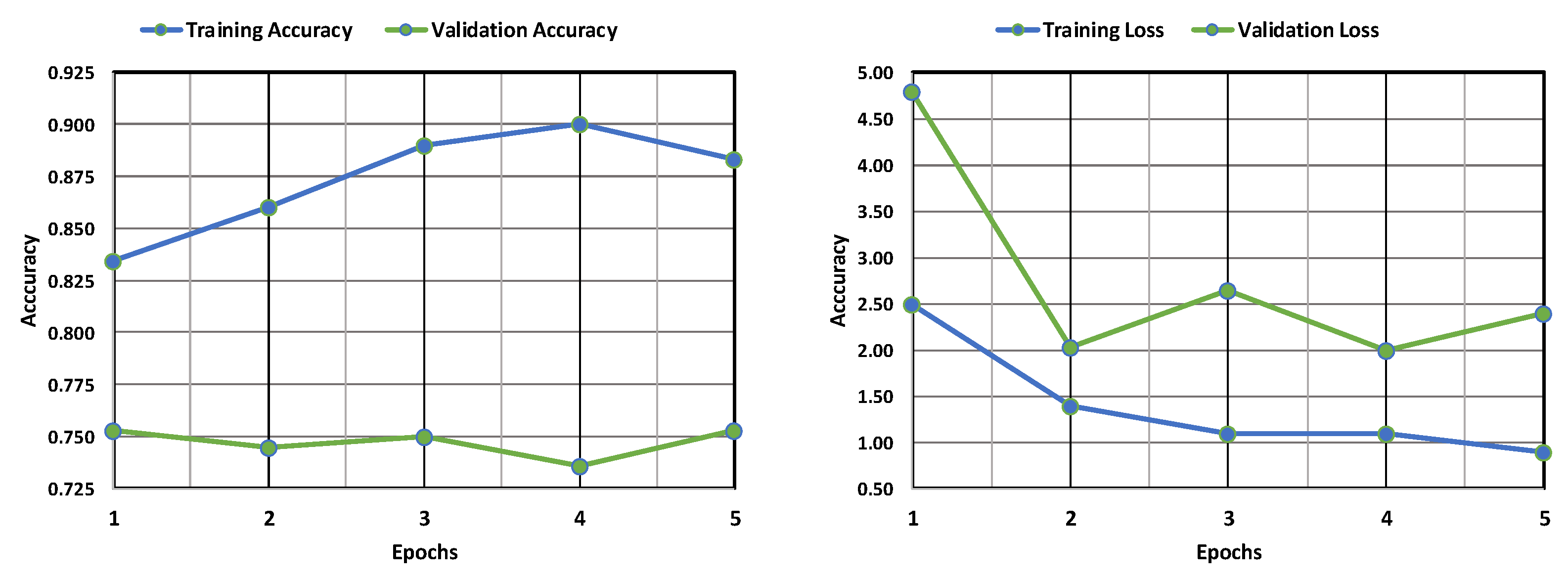
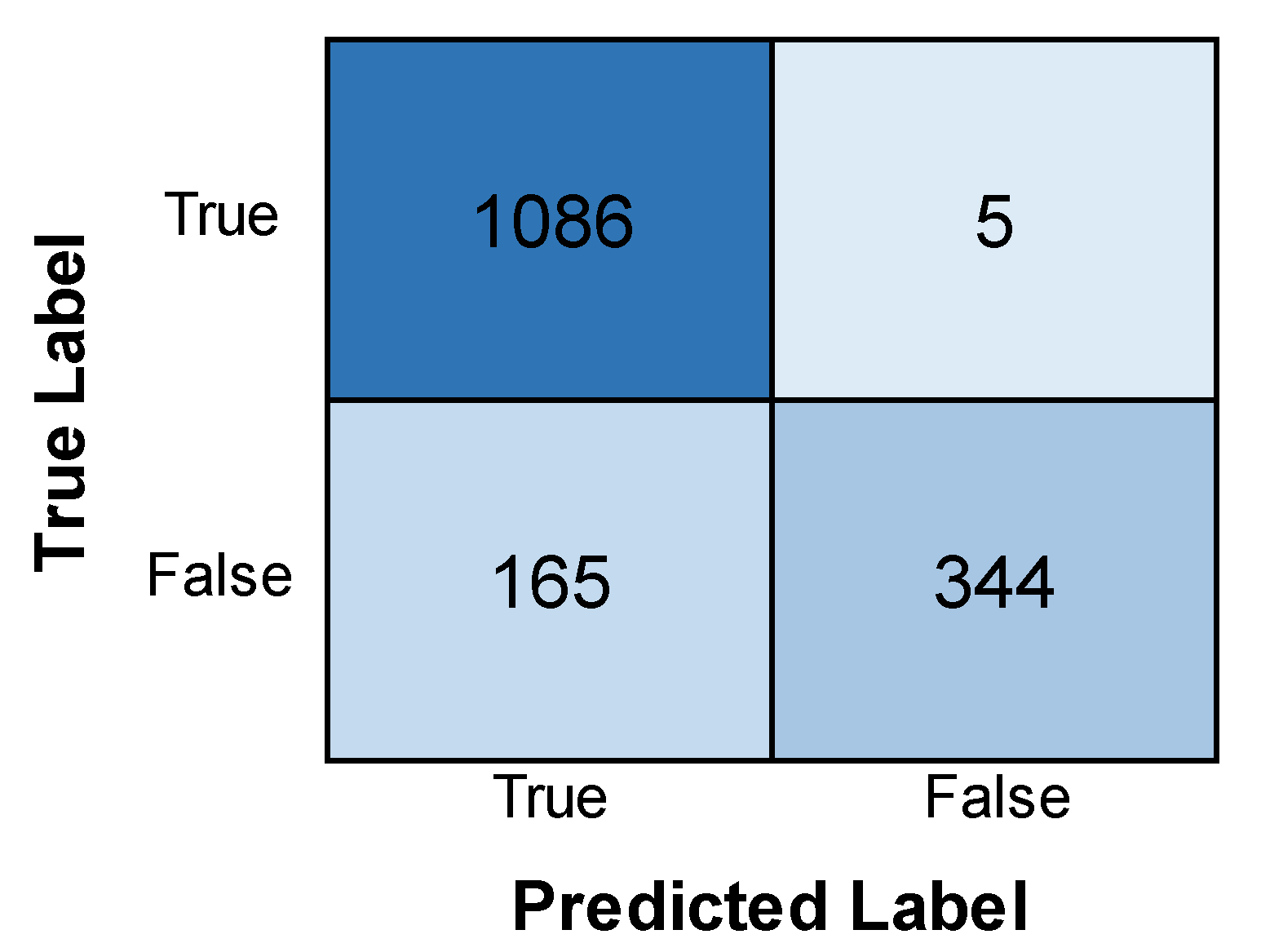
4.4. AlexNet Model Performance
4.5. CNN Model Performance
4.6. ResNet Model Performance
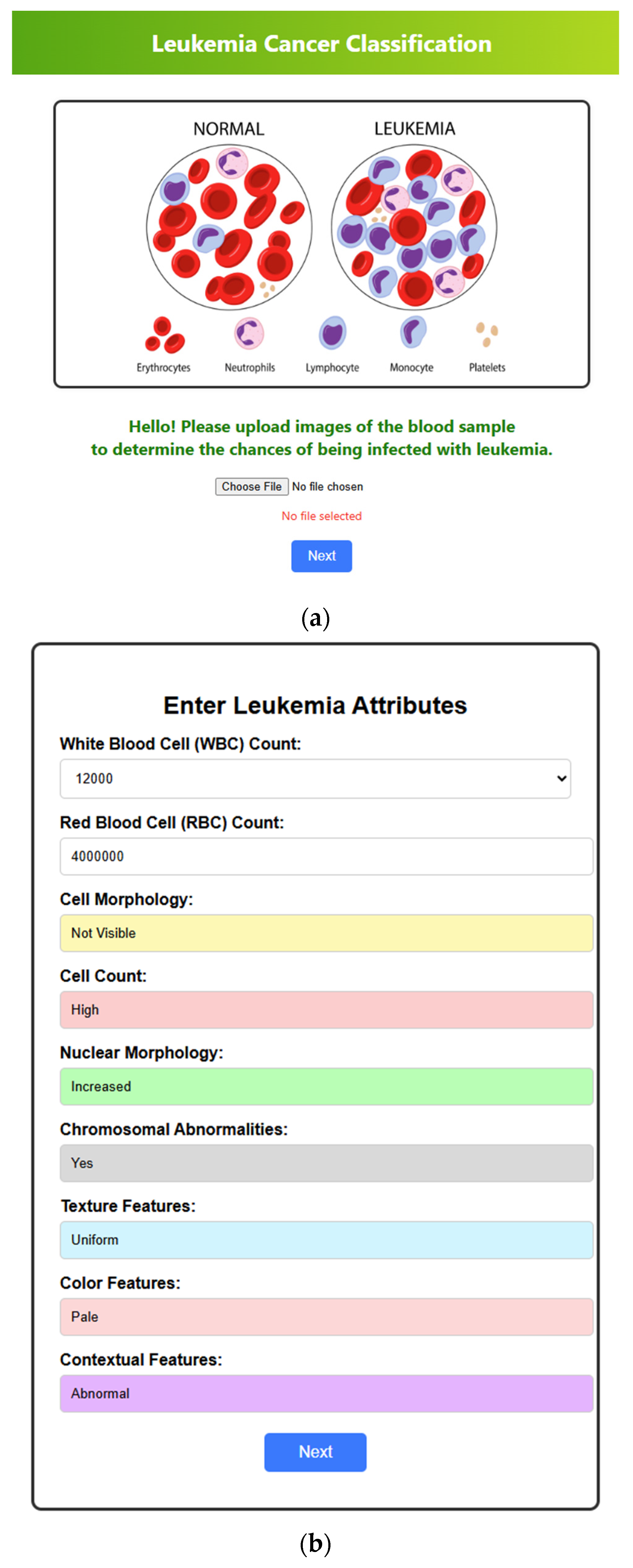
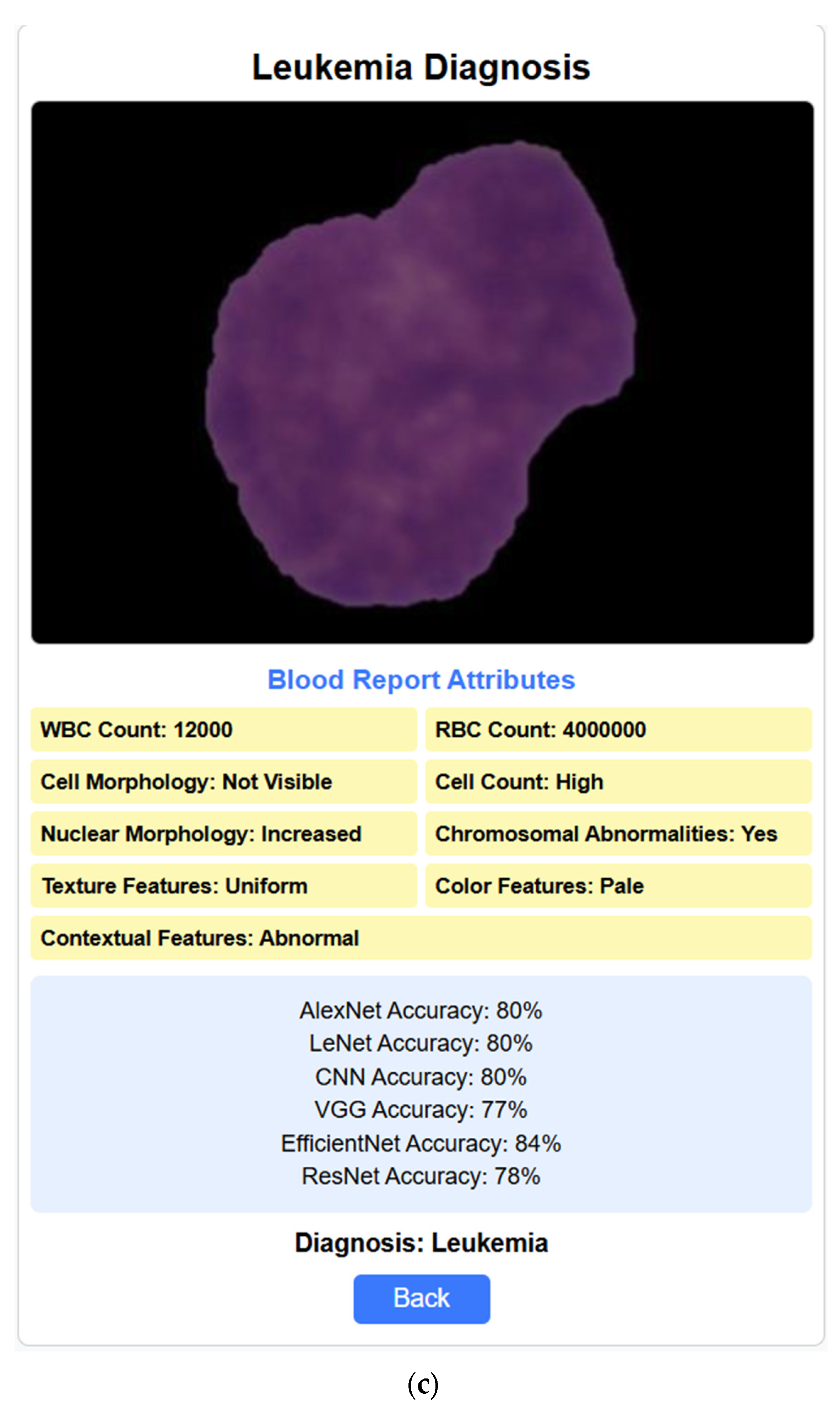
4.7. Web Interface
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Oybek Kizi, R.F.; Theodore Armand, T.P.; Kim, H.-C. A Review of Deep Learning Techniques for Leukemia Cancer Classification Based on Blood Smear Images. Appl. Biosci. 2025, 4, 9. [Google Scholar] [CrossRef]
- Garg, R.; Garg, H.; Patel, H.; Ananthakrishnan, G.; Sharma, S. Role of Machine Learning in Detection and Classification of Leukemia: A Comparative Analysis. In GANs for Data Augmentation in Healthcare; Springer International Publishing: Cham, Switzerland, 2023; pp. 1–20. [Google Scholar] [CrossRef]
- Rai, H.M.; Yoo, J.; Razaque, A. Comparative analysis of machine learning and deep learning models for improved cancer detection: A comprehensive review of recent advancements in diagnostic techniques. Expert Syst. Appl. 2024, 255, 124838. [Google Scholar] [CrossRef]
- Mallick, P.K.; Mohapatra, S.K.; Chae, G.-S.; Mohanty, M.N. Convergent learning–based model for leukemia classification from gene expression. Pers. Ubiquitous Comput. 2023, 27, 1103–1110. [Google Scholar] [CrossRef]
- Tan, M.; Le, Q.V. EfficientNet: Rethinking model scaling for convolutional neural networks. In Proceedings of the 36th International Conference on Machine Learning, ICML 2019, Long Beach, CA, USA, 9–15 June 2019; pp. 10691–10700. [Google Scholar]
- Krizhevsky, A.; Sutskever, I.; Hinton, G.E. ImageNet classification with deep convolutional neural networks. Commun. ACM 2017, 60, 84–90. [Google Scholar] [CrossRef]
- Rai, H.M.; Yoo, J.; Razaque, A. A depth analysis of recent innovations in non-invasive techniques using artificial intelligence approach for cancer prediction. Med. Biol. Eng. Comput. 2024, 62, 3555–3580. [Google Scholar] [CrossRef]
- Raina, R.; Gondhi, N.K.; Chaahat Singh, D.; Kaur, M.; Lee, H.-N. A Systematic Review on Acute Leukemia Detection Using Deep Learning Techniques. Arch. Comput. Methods Eng. 2023, 30, 251–270. [Google Scholar] [CrossRef]
- Khan, S.; Sajjad, M.; Hussain, T.; Ullah, A.; Imran, A.S. A review on traditional machine learning and deep learning models for WBCs classification in blood smear images. IEEE Access 2020, 9, 10657–10673. [Google Scholar] [CrossRef]
- Kanimozhi, N.; Nayak, S.; Kumar K, K.; Manjramkar, V.; Kumar, R.; Suganthi, D. Blood Cancer Detection and Classification using Auto Encoder and Regularized Extreme Learning Machine. In Proceedings of the 2023 8th International Conference on Communication and Electronics Systems (ICCES), Coimbatore, India, 1–3 June 2023; pp. 1122–1127. [Google Scholar] [CrossRef]
- Anilkumar, K.K.; Manoj, V.J.; Sagi, T.M. A review on computer aided detection and classification of leukemia. Multimed. Tools Appl. 2023, 83, 17961–17981. [Google Scholar] [CrossRef]
- Nautiyal, U.; Bhatt, A.; Chauhan, R.; Rawat, R.; Gupta, R. A Modified Conventional Neural Network for Detecting and Classifying Leukemia. In Proceedings of the 2024 International Conference on Intelligent and Innovative Technologies in Computing, Electrical and Electronics (IITCEE), Bangalore, India, 24–25 January 2024; pp. 1–7. [Google Scholar]
- Abirami, M.; Revathy, S.; Swathika, R.; Rajheshwari, K.C.; Mohanaprakash, T.A. An Extensive Study of Different Types of Leukemia using Image Processing Techniques. Int. J. Intell. Syst. Appl. Eng. 2024, 12, 586–596. [Google Scholar]
- Singh, R.; Sharma, N.; Aggarwal, P.; Singh, M.; Chythanya, K.R. Revolutionary Changes in Acute Lymphoblastic Leukaemia Classification: The Impact of Deep Learning Convolutional Neural Networks. In Proceedings of the 2024 2nd International Conference on Computer, Communication and Control (IC4), Indore, India, 8–10 February 2024; pp. 1–6. [Google Scholar]
- Al-Hussaini, I.; White, B.; Varmeziar, A.; Mehra, N.; Sanchez, M.; Lee, J.; DeGroote, N.P.; Miller, T.P.; Mitchell, C.S. An Interpretable Machine Learning Framework for Rare Disease: A Case Study to Stratify Infection Risk in Pediatric Leukemia. J. Clin. Med. 2024, 13, 1788. [Google Scholar] [CrossRef]
- Huérfano-Maldonado, Y.; Mora, M.; Vilches, K.; Hernández-García, R.; Gutiérrez, R.; Vera, M. A comprehensive review of extreme learning machine on medical imaging. Neurocomputing 2023, 556, 126618. [Google Scholar] [CrossRef]
- Bodzas, A.; Kodytek, P.; Zidek, J. Automated Detection of Acute Lymphoblastic Leukemia From Microscopic Images Based on Human Visual Perception. Front. Bioeng. Biotechnol. 2020, 8, 1005. [Google Scholar] [CrossRef]
- Mirmohammadi, P.; Ameri, M.; Shalbaf, A. Recognition of acute lymphoblastic leukemia and lymphocytes cell subtypes in microscopic images using random forest classifier. Phys. Eng. Sci. Med. 2021, 44, 433–441. [Google Scholar] [CrossRef]
- Shahin, A.I.; Guo, Y.; Amin, K.M.; Sharawi, A.A. White blood cells identification system based on convolutional deep neural learning networks. Comput Methods Programs Biomed. 2019, 168, 69–80. [Google Scholar] [CrossRef]
- Emam Atteia, G. Latent Space Representational Learning of Deep Features for Acute Lymphoblastic Leukemia Diagnosis. Comput. Syst. Sci. Eng. 2023, 45, 361–376. [Google Scholar] [CrossRef]
- Elhassan, T.A.M.; Rahim, M.S.M.; Swee, T.T.; Hashim, S.Z.M.; Aljurf, M. Feature Extraction of White Blood Cells Using CMYK-Moment Localization and Deep Learning in Acute Myeloid Leukemia Blood Smear Microscopic Images. IEEE Access 2022, 10, 16577–16591. [Google Scholar] [CrossRef]
- Deshpande, N.M.; Gite, S.; Pradhan, B.; Alamri, A.; Lee, C.-W. A New Method for Diagnosis of Leukemia Utilizing a Hybrid DL-ML Approach for Binary and Multi-Class Classification on a Limited-Sized Database. Comput. Model. Eng. Sci. 2024, 139, 593–631. [Google Scholar] [CrossRef]
- Claro, M.; Vogado, L.; Veras, R.; Santana, A.; Tavares, J.; Santos, J.; Machado, V. Convolution Neural Network Models for Acute Leukemia Diagnosis. In Proceedings of the 2020 International Conference on Systems, Signals and Image Processing (IWSSIP), Niteroi, Brazil, 1–3 July 2020; pp. 63–68. [Google Scholar] [CrossRef]
- Jusman, Y.; Riyadi, S.; Faisal, A.; Kanafiah, S.N.A.M.; Mohamed, Z.; Hassan, R. Classification System for Leukemia Cell Images based on Hu Moment Invariants and Support Vector Machines. In Proceedings of the Proceedings—2021 11th IEEE International Conference on Control System, Computing and Engineering, ICCSCE 2021, Penang, Malaysia, 27–28 August 2021; pp. 137–141. [Google Scholar]
- Anil, B.C.; Nikitha, B.A.; Supriya, N.H.; Koushal, B.; Suhas, S.; Dayananda, P. Detection of WBC Cancer Using Image Processing. J. Inst. Eng. (India) Ser. B 2023, 104, 141–152. [Google Scholar] [CrossRef]
- More, P.; Sugandhi, R. Automated and Enhanced Leucocyte Detection and Classification for Leukemia Detection Using Multi-Class SVM Classifier. Eng. Proc. 2023, 37, 36. [Google Scholar]
- Hasanaath, A.A.; Mohammed, A.S.; Latif, G.; Abdelhamid, S.E.; Alghazo, J.; Hussain, A.A. Acute lymphoblastic leukemia detection using ensemble features from multiple deep CNN models. Electron. Res. Arch. 2024, 32, 2407–2423. [Google Scholar] [CrossRef]
- Hameed, S.M.; Ahmed, W.A.; Othman, M.A. Leukemia Diagnosis using Machine Learning Classifiers based on MRMR Feature Selection. Eng. Technol. Appl. Sci. Res. 2024, 14, 15614–15619. [Google Scholar] [CrossRef]
- Talaat, F.M.; Gamel, S.A. Machine learning in detection and classification of leukemia using C-NMC_Leukemia. Multimed. Tools Appl. 2023, 83, 8063–8076. [Google Scholar] [CrossRef]
- Jawahar, M.; Anbarasi, L.J.; Narayanan, S.; Gandomi, A.H. An attention-based deep learning for acute lymphoblastic leukemia classification. Sci. Rep. 2024, 14, 17447. [Google Scholar] [CrossRef]
- Zhang, C.; Wu, S.; Lu, Z.; Shen, Y.; Wang, J.; Huang, P.; Lou, J.; Liu, C.; Xing, L.; Zhang, J.; et al. Hybrid adversarial-discriminative network for leukocyte classification in leukemia. Med. Phys. 2020, 47, 3732–3744. [Google Scholar] [CrossRef]
- Zare, L.; Rahmani, M.; Khaleghi, N.; Sheykhivand, S.; Danishvar, S. Automatic Detection of Acute Leukemia (ALL and AML) Utilizing Customized Deep Graph Convolutional Neural Networks. Bioengineering 2024, 11, 644. [Google Scholar] [CrossRef]
- Ul Ain, Q.; Akbar, S.; Hassan, S.A.; Naaqvi, Z. Diagnosis of Leukemia Disease through Deep Learning using Microscopic Images. In Proceedings of the 2022 2nd International Conference on Digital Futures and Transformative Technologies, ICoDT2. Rawalpindi, Pakistan, 24–26 May 2022; Institute of Electrical and Electronics Engineers Inc.: New York, NY, USA, 2022. [Google Scholar]
- Jha, K.K.; Dutta, H.S. Mutual Information based hybrid model and deep learning for Acute Lymphocytic Leukemia detection in single cell blood smear images. Comput. Methods Programs Biomed. 2019, 179, 104987. [Google Scholar] [CrossRef] [PubMed]
- Jiang, Z.; Dong, Z.; Wang, L.; Jiang, W. Method for Diagnosis of Acute Lymphoblastic Leukemia Based on ViT-CNN Ensemble Model. Comput. Intell. Neurosci. 2021, 2021, 7529893. [Google Scholar] [CrossRef]
- Rahman, W.; Faruque, M.G.G.; Roksana, K.; Sadi, A.H.M.S.; Rahman, M.M.; Azad, M.M. Multiclass blood cancer classification using deep CNN with optimized features. Array 2023, 18, 100292. [Google Scholar] [CrossRef]
- Sampathila, N.; Chadaga, K.; Goswami, N.; Chadaga, R.P.; Pandya, M.; Prabhu, S.; Bairy, M.G.; Katta, S.S.; Bhat, D.; Upadya, S.P. Customized Deep Learning Classifier for Detection of Acute Lymphoblastic Leukemia Using Blood Smear Images. Healthcare 2022, 10, 1812. [Google Scholar] [CrossRef]
- Islam, M.M.; Rifat, H.R.; Shahid MdSBin Akhter, A.; Uddin, M.A. Utilizing Deep Feature Fusion for Automatic Leukemia Classification: An Internet of Medical Things-Enabled Deep Learning Framework. Sensors 2024, 24, 4420. [Google Scholar] [CrossRef]
- Asar, T.O.; Ragab, M. Leukemia detection and classification using computer-aided diagnosis system with falcon optimization algorithm and deep learning. Sci. Rep. 2024, 14, 21755. [Google Scholar] [CrossRef] [PubMed]
- Lecun, Y.; Bottou, L.; Bengio, Y.; Haffner, P. Gradient-based learning applied to document recognition. Proc. IEEE 1998, 86, 2278–2324. [Google Scholar] [CrossRef]
- Rai, H.M.; Yoo, J.; Atif Moqurrab, S.; Dashkevych, S. Advancements in traditional machine learning techniques for detection and diagnosis of fatal cancer types: Comprehensive review of biomedical imaging datasets. Measurement 2024, 225, 114059. [Google Scholar] [CrossRef]
- Simonyan, K.; Zisserman, A. Very deep convolutional networks for large-scale image recognition. In Proceedings of the 3rd International Conference on Learning Representations, ICLR 2015—Conference Track Proceedings, San Diego, CA, USA, 7–9 May 2015. [Google Scholar]
- Esteva, A.; Kuprel, B.; Novoa, R.A.; Ko, J.; Swetter, S.M.; Blau, H.M.; Thrun, S. Dermatologist-level classification of skin cancer with deep neural networks. Nature 2017, 542, 115–118. [Google Scholar] [CrossRef]
- Russakovsky, O.; Deng, J.; Su, H.; Krause, J.; Satheesh, S.; Ma, S.; Huang, Z.; Karpathy, A.; Khosla, A.; Bernstein, M.; et al. ImageNet Large Scale Visual Recognition Challenge. Int. J. Comput. Vis. 2015, 115, 211–252. [Google Scholar] [CrossRef]
- Szegedy, C.; Wei Liu Yangqing Jia Sermanet, P.; Reed, S.; Anguelov, D.; Erhan, D.; Vanhoucke, V.; Rabinovich, A. Going deeper with convolutions. In Proceedings of the 2015 IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Boston, MA, USA, 7–12 June 2015; pp. 1–9. [Google Scholar] [CrossRef]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Deep Residual Learning for Image Recognition. In Proceedings of the 2016 IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Las Vegas, NV, USA, 27–30 June 2016; pp. 770–778. [Google Scholar] [CrossRef]
- Sandler, M.; Howard, A.; Zhu, M.; Zhmoginov, A.; Chen, L.-C. MobileNetV2: Inverted Residuals and Linear Bottlenecks. In Proceedings of the 2018 IEEE/CVF Conference on Computer Vision and Pattern Recognition, Salt Lake City, UT, USA, 18–23 June 2018; pp. 4510–4520. [Google Scholar] [CrossRef]
- Duggal, R.; Gupta, A.; Gupta, R.; Mallick, P. SD-Layer: Stain Deconvolutional Layer for CNNs in Medical Microscopic Imaging. In Medical Image Computing and Computer Assisted Intervention—MICCAI 2017; Springer: Berlin/Heidelberg, Germany, 2017; pp. 435–443. [Google Scholar]
- Gupta, A.; Gupta, R. (Eds.) ISBI 2019 C-NMC Challenge: Classification in Cancer Cell Imaging; Singapore: Springer, 2019. [Google Scholar] [CrossRef]
- Gupta, A.; Duggal, R.; Gehlot, S.; Gupta, R.; Mangal, A.; Kumar, L.; Thakkar, N.; Satpathy, D. GCTI-SN: Geometry-inspired chemical and tissue invariant stain normalization of microscopic medical images. Med. Image Anal. 2020, 65, 101788. [Google Scholar] [CrossRef]
- Gupta, R.; Mallick, P.; Duggal, R.; Gupta, A.; Sharma, O. Stain Color Normalization and Segmentation of Plasma Cells in Microscopic Images as a Prelude to Development of Computer Assisted Automated Disease Diagnostic Tool in Multiple Myeloma. Clin. Lymphoma Myeloma Leuk. 2017, 17, e99. [Google Scholar] [CrossRef]
- Duggal, R.; Gupta, A.; Gupta, R.; Wadhwa, M.; Ahuja, C. Overlapping cell nuclei segmentation in microscopic images using deep belief networks. In Proceedings of the Tenth Indian Conference on Computer Vision, Graphics and Image Processing, Guwahati, India, 18–22 December 2016; ACM: New York, NY, USA, 2016; pp. 1–8. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| S.N. | Year | Techniques Used | Findings | Challenges | Ref. No. |
|---|---|---|---|---|---|
| 1 | 2019 | SVM with shape, texture, and complex features | Achieved 0.9610 accuracy, 0.9890 specificity, and 0.9120 precision on ALL_DB1 and ALL_DB2. | Limited sensitivity may impact rare class detection; dataset skew is not addressed. | [19] |
| 2 | 2020 | ANN with morphological and statistical features | Achieved 0.9752 accuracy, 1.000 sensitivity, and 0.9531 specificity. | A limited dataset (private hospital data) reduces generalizability and lacks the interpretability of ANN. | [17] |
| 3 | 2020 | AlexNet with deep features | Achieved 0.9718 accuracy and 0.9723 sensitivity across 16 public datasets. | Lack of clarity on dataset harmonization; computation-heavy model (AlexNet). | [23] |
| 4 | 2021 | Random Forest (RF) with geometric and statistical features | Reported 0.9800 accuracy. | No additional metrics (like specificity or precision) were provided; dataset diversity was not verified. | [18] |
| 5 | 2021 | SVM using Hu invariant moments | Accuracy of 0.9500. | The dataset source is unknown; it lacks robustness verification and deep feature comparison. | [24] |
| 6 | 2022 | RF with CNN-based features from the AML-C-LMU dataset | Achieved 0.9757 accuracy, 0.9782 F1-score, and 0.9848 precision. | Dataset imbalance might influence findings; RF’s scalability to larger datasets is unclear. | [21] |
| 7 | 2023 | SVM with deep features | Perfect scores: 1.0000 accuracy, sensitivity, precision, and specificity on ALL-IDB dataset. | Exceptional results suggest potential overfitting or insufficient dataset variability. | [20] |
| 8 | 2023 | MLP with cell-based features | Reported 0.9840 accuracy on the ALL-IDB dataset. | The model’s overfitting risk was not discussed, and feature scalability was not evaluated. | [25] |
| 9 | 2023 | SVM with intensity variation features | Achieved 0.9885 accuracy, 0.9900 precision, and 0.9880 sensitivity on the ALL-IDB1 dataset. | Dataset reliance on intensity variations may not generalize to other imaging modalities. | [26] |
| 10 | 2024 | Linear SVM with deep features | Accuracy of 0.9163 and F1-score of 0.9014 on the C-NMC-2019 dataset. | Limited performance on larger datasets indicates the need for improved feature engineering. | [27] |
| 11 | 2024 | KNN, SVM, and ANN on microarray attributes | Achieved 1.000 accuracy using attribute data. | Microarray data may limit the application to an image-based leukemia diagnosis. | [28] |
| 12 | 2024 | RF with DenseNet-based deep features | Achieved 0.9600 accuracy, 0.9700 precision, and 0.9700 sensitivity on ALL-IDB1 and ALL-IDB2 datasets. | Limited dataset size for DenseNet features may restrict findings; interpretability challenges of deep learning remain. | [22] |
| S.N. | Year | Techniques Used | Findings | Challenges | Ref. No. |
|---|---|---|---|---|---|
| 1 | 2019 | SCA-CNN with statistical and local directional pattern (LDP) features | Achieved 0.9870 accuracy, 0.9800 sensitivity, and 0.9800 specificity. | The small dataset size (260 samples) limits generalizability. | [34] |
| 2 | 2020 | CNN + HOG with SVM | Reported 0.9593 accuracy, 0.9611 sensitivity, and 0.9457 specificity on MIC modality. | Dependency on handcrafted HOG features; limited validation on other modalities. | [31] |
| 3 | 2021 | ViT-CNN | Achieved 0.9903 accuracy and 0.9914 precision on MIC. | Lack of clarity on utilized features; training complexity due to ViT. | [35] |
| 4 | 2022 | ResNet-34 with DCNN | Reported 0.9840 accuracy for BSI modality. | Limited metric diversity (no specificity or precision reported); lacks interpretability. | [33] |
| 5 | 2023 | AlexNet with OCNN | Achieved nearly perfect metrics: 0.9999 accuracy, 1.0000 sensitivity, and 0.9998 specificity for LYI. | Dataset diversity (C-NMC 2019) might not cover other blood conditions, possibly overfitting due to high results. | [29] |
| 6 | 2023 | ResNet-50 pre-trained | Achieved 0.9984 accuracy, 0.9981 F1, 0.9975 precision, and 0.9987 sensitivity on MIC modality. | Performance depends on pre-trained weights; it may not generalize well to new datasets. | [36] |
| 7 | 2023 | CNN | Reported 0.9554 accuracy, 0.9600 precision, and 0.9591 sensitivity on BSI modality. | Performance is lower compared to other approaches; it lacks deep feature representation. | [37] |
| 8 | 2024 | DG-CNN | Achieved 0.9940 accuracy, 0.9920 sensitivity, and 0.9730 specificity for BSI. | The dataset was sourced from a private hospital; it was not tested on public datasets. | [32] |
| 9 | 2024 | VGG16 and DenseNet-121 with DFFM | Reported 0.9989 accuracy, 0.9980 precision, and 0.9972 sensitivity on BSI modality. | With the high computational cost of DenseNet-121, performance validation on larger datasets is required. | [38] |
| 10 | 2024 | DDRNet | Achieved perfect results: 0.9999 accuracy, 1.0000 F1, MCC, precision, and sensitivity for BSI modality. | The unrealistically high performance suggests possible overfitting; it requires extensive cross-validation. | [30] |
| 11 | 2024 | ShuffleNetv2 with FOADCNN-LDC | Reported 0.9962 accuracy, 0.9978 specificity, and 0.9714 sensitivity for BSI. | The sample size is limited (518 samples); it may not be generalized well to other modalities. | [39] |
| Model | Architecture Description | Advantages | Disadvantages |
|---|---|---|---|
| VGG | Deep CNN with 16 convolutional layers and 3 × 3 filters, followed by max-pooling and fully connected layers. ReLU activation and dropout regularization mitigate overfitting. | Captures intricate spatial patterns and textures. | It is computationally intensive due to its deep architecture. |
| EfficientNet | Scalable CNN architecture prioritizing efficiency and performance through compound scaling of depth, width, and resolution. EfficientNet-B0 balances efficiency and accuracy. | Efficient utilization of computational resources. | It may sacrifice some model expressiveness for efficiency. |
| LeNet | Shallow CNN has two convolutional layers, max-pooling layers, and fully connected layers. It is the baseline model for comparison with deeper architectures. | Lightweight design suitable for low-resolution images. | Limited capacity to capture complex features due to shallow architecture. |
| AlexNet | Deep CNN architecture introduces ReLU activation functions and dropout regularization. Facilitates the extraction of complex features from leukemia images. | Pioneering the use of innovative activation functions. | Requires substantial computational resources for training. |
| CNN | Flexible and scalable architecture for image classification tasks, featuring convolutional and pooling layers followed by fully connected layers. | Adaptable to a wide range of image classification tasks. | It may require extensive hyperparameter tuning for optimal performance. |
| ResNet | Deep CNN architecture featuring residual connections to address vanishing gradients. Enables the extraction of highly abstract features, improving classification performance. | Mitigates challenges associated with training deep networks. | Increased model complexity may lead to overfitting on smaller datasets. |
| Model/Metric | Accuracy | Precision | Recall | F1-Score |
|---|---|---|---|---|
| VGG | 0.77125 | 0.87534 | 0.80591 | 0.83919 |
| EfficientNet | 0.85187 | 0.99450 | 0.82446 | 0.90153 |
| LeNet | 0.87375 | 0.98900 | 0.85027 | 0.91440 |
| AlexNet | 0.89375 | 0.99541 | 0.86811 | 0.92741 |
| CNN | 0.81375 | 0.86709 | 0.86078 | 0.86392 |
| ResNet | 0.82625 | 0.94775 | 0.82390 | 0.88149 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rai, H.M.; Omkar Lakshmi Jagan, B.; Rao, N.T.; Mohammed, T.K.; Agarwal, N.; Abdallah, H.A.; Agarwal, S. Deep Learning for Leukemia Classification: Performance Analysis and Challenges Across Multiple Architectures. Fractal Fract. 2025, 9, 337. https://doi.org/10.3390/fractalfract9060337
Rai HM, Omkar Lakshmi Jagan B, Rao NT, Mohammed TK, Agarwal N, Abdallah HA, Agarwal S. Deep Learning for Leukemia Classification: Performance Analysis and Challenges Across Multiple Architectures. Fractal and Fractional. 2025; 9(6):337. https://doi.org/10.3390/fractalfract9060337
Chicago/Turabian StyleRai, Hari Mohan, B. Omkar Lakshmi Jagan, N. Thiruapthi Rao, Thayyaba Khatoon Mohammed, Neha Agarwal, Hanaa A. Abdallah, and Saurabh Agarwal. 2025. "Deep Learning for Leukemia Classification: Performance Analysis and Challenges Across Multiple Architectures" Fractal and Fractional 9, no. 6: 337. https://doi.org/10.3390/fractalfract9060337
APA StyleRai, H. M., Omkar Lakshmi Jagan, B., Rao, N. T., Mohammed, T. K., Agarwal, N., Abdallah, H. A., & Agarwal, S. (2025). Deep Learning for Leukemia Classification: Performance Analysis and Challenges Across Multiple Architectures. Fractal and Fractional, 9(6), 337. https://doi.org/10.3390/fractalfract9060337