
Google Street View Images as Predictors of Patient Health Outcomes, 2017–2019

 ,
,  , ,
, ,  , ,
, ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Setting and Population
2.2. Study Measurement
Individual-Level Characteristics
2.3. Google Street View Image Data
2.3.1. Google Street View Image Data Collection
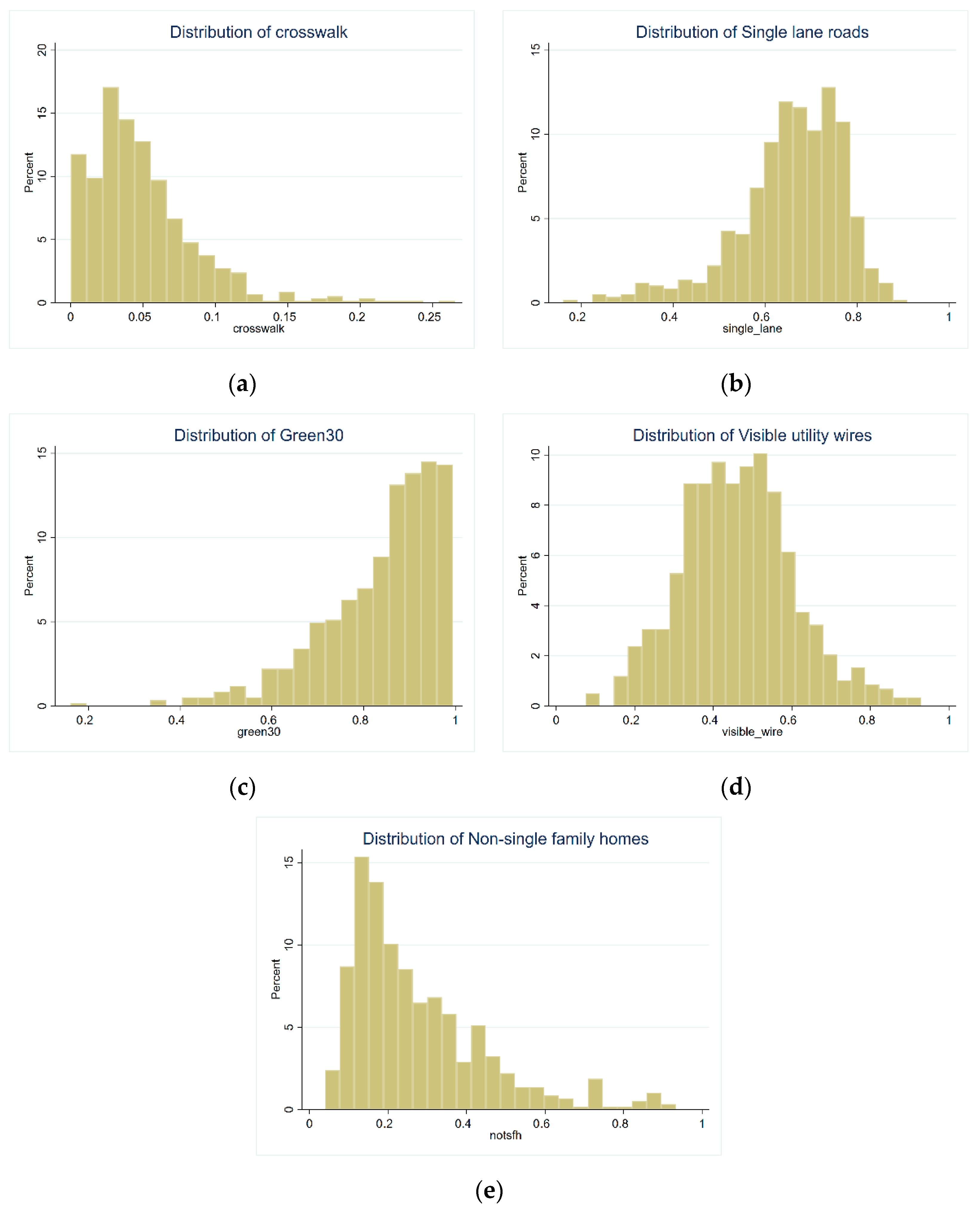
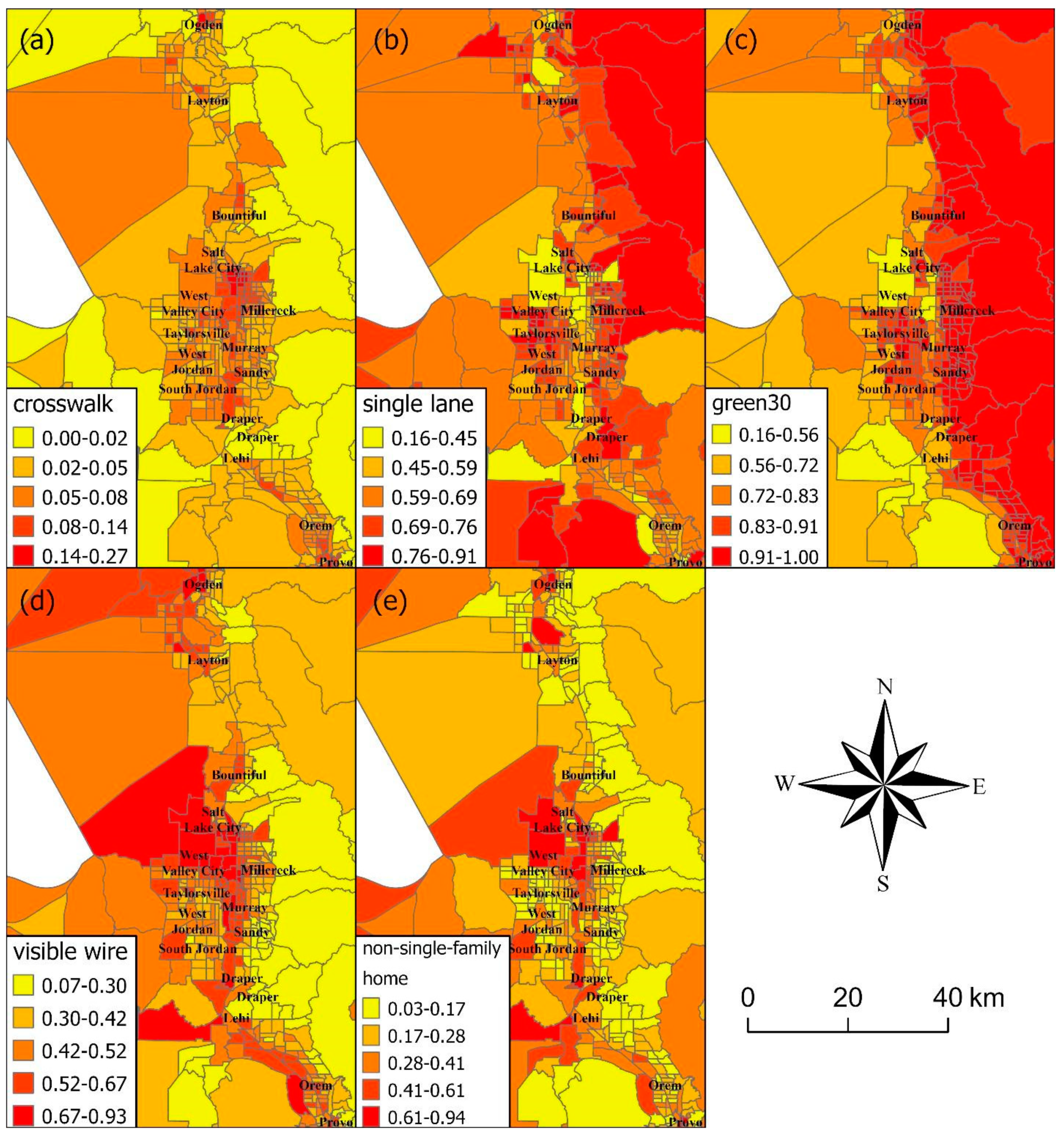
2.3.2. Built Environment Indicators
2.3.3. Image Data Processing
2.3.4. Neighborhood Definitions
2.4. Statistical Analyses
3. Results
4. Discussion
Study Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
Appendix B

{kind=link}
{kind=link}
{kind=link}
| Diabetes | Uncontrolled Diabetes | Hypertension | Obesity | Substance Use Disorder | |
|---|---|---|---|---|---|
| Prevalence Ratio (95% CI) | Prevalence Ratio (95% CI) | Prevalence Ratio (95% CI) | Prevalence Ratio (95% CI) | Prevalence Ratio (95% CI) | |
| Google Street View indicators | |||||
| Green streets, 3rd tertile | 1.19 (0.96, 1.48) | 1.03 (0.92, 1.15) | 1.03 (0.54, 1.99) | 0.90 (0.83, 0.98) * | 0.98 (0.70, 1.38) |
| Green streets, 2nd tertile | 1.03 (0.95, 1.12) | 1.32 (0.96, 1.80) | 0.78 (0.59, 1.04) | 0.97 (0.94, 1.00) * | 0.98 (0.86, 1.11) |
| Crosswalks, 3rd tertile | 1.06 (0.47, 2.38) | 1.06 (0.90, 1.24) | 1.26 (0.17, 9.17) | 0.99 (0.73, 1.33) | 1.41 (0.58, 3.44) |
| Crosswalks, 2nd tertile | 1.05 (0.93, 1.18) | 1.15 (0.43, 3.10) | 1.35 (0.96, 1.90) | 1.01 (0.97, 1.06) | 1.18 (1.00, 1.39) * |
| Non-single-family home, 3rd tertile | 0.87 (0.70, 1.08) | 0.99 (0.72, 1.36) | 1.04 (0.54, 2.00) | 0.93 (0.85, 1.01) | 0.88 (0.63, 1.22) |
| Non-single-family home, 2nd tertile | 1.02 (0.84, 1.24) | 1.04 (0.78, 1.39) | 1.12 (0.62, 2.02) | 0.98 (0.90, 1.06) | 0.85 (0.63, 1.16) |
| Single-lane roads, 3rd tertile | 1.06 (0.94, 1.19) | 0.96 (0.82, 1.12) | 1.07 (0.76, 1.52) | 1.02 (0.98, 1.07) | 1.08 (0.91, 1.27) |
| Single-lane roads, 2nd tertile | 1.08 (0.95, 1.22) | 1.02 (0.87, 1.20) | 1.03 (0.71, 1.49) | 1.02 (0.97, 1.07) | 1.13 (0.95, 1.34) |
| Visible wires, 3rd tertile | 1.26 (1.12, 1.43) * | 1.19 (1.01, 1.40) * | 1.01 (0.69, 1.49) | 1.10 (1.04, 1.15) * | 1.14 (0.95, 1.37) |
| Visible wires, 2nd tertile | 1.17 (1.04, 1.32) * | 1.19 (1.00, 1.41) * | 0.81 (0.55, 1.17) | 1.05 (1.01, 1.10) * | 1.01 (0.84, 1.20) |
| Covariates | |||||
| Age (years) | 1.01 (1.01, 1.01) * | 1.03 (1.02, 1.03) * | 1.00 (1.00, 1.01) * | 1.01 (1.01, 1.01) * | 1.00 (1.00, 1.01) * |
| White race | 0.60 (0.58, 0.62) * | 0.57 (0.43, 0.76) * | 0.84 (0.39, 1.78) | 0.83 (0.76, 0.92) * | 0.77 (0.57, 1.04) |
| Hispanic ethnicity | 1.15 (1.12, 1.18) * | 1.46 (1.19, 1.78) * | 0.64 (0.34, 1.21) | 1.07 (1.01, 1.14) * | 0.61 (0.47, 0.80) * |
| Any religion | 1.21 (1.19, 1.23) * | 1.39 (1.24, 1.55) * | 1.02 (0.81, 1.30) | 1.10 (1.07, 1.14) * | 0.59 (0.54, 0.66) * |
| Married | 1.09 (1.07, 1.11) * | 0.94 (0.85, 1.03) | 1.50 (1.16, 1.93) * | 1.16 (1.12, 1.19) * | 0.45 (0.41, 0.50) * |
| Uninsured | 1.60 (1.57, 1.63) * | 1.98 (1.79, 2.18) * | 1.28 (1.00, 1.62) * | 1.12 (1.08, 1.15) * | 2.60 (2.35, 2.87) * |
| Area deprivation index | 1.01 (1.01, 1.01) * | 1.02 (1.01, 1.02) * | 1.00 (0.99, 1.01) | 1.01 (1.01, 1.01) * | 1.00 (1.00, 1.01) * |
References
- Macintyre, S.; Ellaway, A. Ecological approaches: Rediscovering the role of the physical and social environment. Soc. Epidemiol. 2000, 9, 332–348. [Google Scholar]
- Nguyen, Q.C.; Khanna, S.; Dwivedi, P.; Huang, D.; Huang, Y.; Tasdizen, T.; Brunisholz, K.D.; Li, F.; Gorman, W.; Nguyen, T.T.; et al. Using Google Street View to examine associations between built environment characteristics and US health outcomes. Prev. Med. Rep. 2019, 14, 100859. [Google Scholar] [CrossRef] [PubMed]
- Keralis, J.M.; Javanmardi, M.; Khanna, S.; Dwivedi, P.; Huang, D.; Tasdizen, T.; Nguyen, Q.C. Health and the built environment in United States cities: Measuring associations using Google Street View-derived indicators of the built environment. BMC Public Health 2020, 20, 215. [Google Scholar] [CrossRef]
- Chaiyachati, K.H.; Hom, J.K.; Hubbard, R.A.; Wong, C.; Grande, D. Evaluating the association between the built environment and primary care access for new Medicaid enrollees in an urban environment using walk and transit scores. Prev. Med. Rep. 2018, 9, 24–28. [Google Scholar] [CrossRef] [PubMed]
- Morland, K.; Wing, S.; Diez Roux, A. The Contextual Effect of the Local Food Environment on Residents’ Diets: The Atherosclerosis Risk in Communities Study. Am. J. Public Health 2002, 92, 1761–1768. [Google Scholar] [CrossRef] [PubMed]
- Laraia, B.A.; Siega-Riz, A.M.; Kaufman, J.S.; Jones, S.J. Proximity of supermarkets is positively associated with diet quality index for pregnancy. Prev. Med. 2004, 39, 869–875. [Google Scholar] [CrossRef] [PubMed]
- Fein, A.J.; Plotnikoff, R.C.; Wild, T.C.; Spence, J.C. Perceived environment and physical activity in youth. Int. J. Behav. Med. 2004, 11, 135–142. [Google Scholar] [CrossRef]
- Giles-Corti, B.; Donovan, R.J. The relative influence of individual, social and physical environment determinants of physical activity. Soc. Sci. Med. 2002, 54, 1793–1812. [Google Scholar] [CrossRef]
- Penedo, F.J.; Dahn, J.R. Exercise and well-being: A review of mental and physical health benefits associated with physical activity. Curr. Opin. Psychiatry 2005, 18, 189–193. [Google Scholar] [CrossRef]
- Sallis, J.F.; Saelens, B.E.; Frank, L.D.; Conway, T.L.; Slymen, D.J.; Cain, K.L.; Chapman, J.E.; Kerr, J. Neighborhood built environment and income: Examining multiple health outcomes. Soc. Sci. Med. 2009, 68, 1285–1293. [Google Scholar] [CrossRef] [Green Version]
- Burls, A. People and green spaces: Promoting public health and mental well-being through ecotherapy. J. Public Ment. Health 2007, 6, 24. [Google Scholar] [CrossRef] [Green Version]
- Nutsford, D.; Pearson, A.; Kingham, S. An ecological study investigating the association between access to urban green space and mental health. Public Health 2013, 127, 1005–1011. [Google Scholar] [CrossRef] [PubMed]
- Browning, M.H.; Lee, K.; Wolf, K.L. Tree cover shows an inverse relationship with depressive symptoms in elderly residents living in US nursing homes. Urban For. Urban Green. 2019, 41, 23–32. [Google Scholar] [CrossRef]
- Frank, L.D.; Schmid, T.L.; Sallis, J.F.; Chapman, J.; Saelens, B.E. Linking objectively measured physical activity with objectively measured urban form: Findings from SMARTRAQ. Am. J. Prev. Med. 2005, 28, 117–125. [Google Scholar] [CrossRef]
- Nguyen, Q.C.; Sajjadi, M.; McCullough, M.; Pham, M.; Nguyen, T.T.; Yu, W.; Meng, H.-W.; Wen, M.; Li, F.; Smith, K.R.; et al. Neighbourhood looking glass: 360° automated characterisation of the built environment for neighborhood effects research. J. Epidemiol. Community Health 2018, 72, 260–266. [Google Scholar] [CrossRef]
- Chum, A.; O’Campo, P.; Lachaud, J.; Fink, N.; Kirst, M.; Nisenbaum, R. Evaluating same-source bias in the association between neighbourhood characteristics and depression in a community sample from Toronto, Canada. Soc. Psychiatry Psychiatr. Epidemiol. 2019, 54, 1177–1187. [Google Scholar] [CrossRef]
- Krumpal, I. Determinants of social desirability bias in sensitive surveys: A literature review. Qual. Quant. 2013, 47, 2025–2047. [Google Scholar] [CrossRef]
- Rundle, A.G.; Bader, M.D.M.; Richards, C.A.; Neckerman, K.M.; Teitler, J.O. Using Google Street View to Audit Neighborhood Environments. Am. J. Prev. Med. 2011, 40, 94–100. [Google Scholar] [CrossRef] [Green Version]
- Kelly, C.M.; Wilson, J.S.; Baker, E.A.; Miller, D.K.; Schootman, M. Using Google Street View to audit the built environment: Inter-rater reliability results. Ann. Behav. Med. 2013, 45, S108–S112. [Google Scholar] [CrossRef] [Green Version]
- Silva, V.; Grande, A.J.; Rech, C.R.; Peccin, M.S. Geoprocessing via google maps for assessing obesogenic built environments related to physical activity and chronic noncommunicable diseases: Validity and reliability. J. Healthc. Eng. 2015, 6, 41–54. [Google Scholar] [CrossRef] [Green Version]
- Krizhevsky, A.; Sutskever, I.; Hinton, G.E. ImageNet classification with deep convolutional neural networks. In Proceedings of the 25th International Conference on Neural Information Processing Systems, Lake Tahoe, NV, USA, 3–6 December 2012; Curran Associates Inc.: Red Hook, NY, USA, 2012; Volume 1, pp. 1097–1105. [Google Scholar]
- Simonyan, K.; Zisserman, A. Very Deep Convolutional Networks for Large-Scale Image Recognition. arXiv 2014, arXiv:1409.1556. [Google Scholar]
- Perronnin, F.; Sánchez, J.; Mensink, T. Improving the fisher kernel for large-scale image classification. In Proceedings of the European Conference on Computer Vision, Crete, Greece, 5–11 September 2010; Springer: Berlin/Heidelberg, Germany, 2010; pp. 143–156. [Google Scholar]
- Dosovitskiy, A.; Beyer, L.; Kolesnikov, A.; Weissenborn, D.; Zhai, X.; Unterthiner, T.; Dehghani, M.; Minderer, M.; Heigold, G.; Gelly, S. An image is worth 16 × 16 words: Transformers for image recognition at scale. arXiv 2020, arXiv:2010.11929. [Google Scholar]
- Huang, G.; Liu, Z.; Van Der Maaten, L.; Weinberger, K.Q. Densely connected convolutional networks. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Honolulu, HI, USA, 21–26 July 2017; pp. 4700–4708. [Google Scholar]
- Brock, A.; De, S.; Smith, S.L.; Simonyan, K. High-performance large-scale image recognition without normalization. arXiv 2021, arXiv:2102.06171. [Google Scholar]
- Szegedy, C.; Liu, W.; Jia, Y.; Sermanet, P.; Reed, S.; Anguelov, D.; Erhan, D.; Vanhoucke, V.; Rabinovich, A. Going deeper with convolutions. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Boston, MA, USA, 7–12 June 2015; pp. 1–9. [Google Scholar]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Deep residual learning for image recognition. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Las Vegas, NV, USA, 27–30 June 2016; pp. 770–778. [Google Scholar]
- Loffe, S.; Szegedy, C. Batch Normalization: Accelerating Deep Network Training by Reducing Internal Covariate Shift. In Proceedings of the International Conference on Machine Learning, Lille, France, 6–11 July 2015; pp. 448–456. [Google Scholar]
- Cohen, T.; Welling, M. Group equivariant convolutional networks. In Proceedings of the International Conference on Machine Learning, New York, NY, USA, 19–24 June 2016; pp. 2990–2999. [Google Scholar]
- National Committee for Quality Assurance (NCQA). HEDIS 2014: Healthcare Effectiveness Data and Information. 2013. Available online: https://www.ncqa.org/hedis/ (accessed on 1 December 2021).
- Phillips, R.L.; Liaw, W.; Crampton, P.; Exeter, D.J.; Bazemore, A.; Vickery, K.D.; Petterson, S.; Carrozza, M. How other countries use deprivation indices—And why the United States desperately needs one. Health Aff. 2016, 35, 1991–1998. [Google Scholar] [CrossRef] [PubMed]
- Singh, G.K. Area deprivation and widening inequalities in US mortality, 1969–1998. Am. J. Public Health 2003, 93, 1137–1143. [Google Scholar] [CrossRef]
- Rundle, A.; Neckerman, K.M.; Freeman, L.; Lovasi, G.S.; Purciel, M.; Quinn, J.; Richards, C.; Sircar, N.; Weiss, C. Neighborhood food environment and walkability predict obesity in New York City. Environ. Health Perspect. 2008, 117, 442–447. [Google Scholar] [CrossRef]
- Van Cauwenberg, J.; Van Holle, V.; De Bourdeaudhuij, I.; Van Dyck, D.; Deforche, B. Neighborhood walkability and health outcomes among older adults: The mediating role of physical activity. Health Place 2016, 37, 16–25. [Google Scholar] [CrossRef]
- Li, F.; Harmer, P.; Cardinal, B.J.; Bosworth, M.; Johnson-Shelton, D.; Moore, J.M.; Acock, A.; Vongjaturapat, N. Built environment and 1-year change in weight and waist circumference in middle-aged and older adults: Portland Neighborhood Environment and Health Study. Am. J. Epidemiol. 2009, 169, 401–408. [Google Scholar] [CrossRef]
- Ross, C.E.; Mirowsky, J. Neighborhood Disadvantage, Disorder, and Health. J. Health Soc. Behav. 2001, 42, 258–276. [Google Scholar] [CrossRef] [Green Version]
- Molnar, B.E.; Gortmaker, S.L.; Bull, F.C.; Buka, S.L. Unsafe to play? Neighborhood disorder and lack of safety predict reduced physical activity among urban children and adolescents. Am. J. Health Promot. 2004, 18, 378–386. [Google Scholar] [CrossRef]
- Burdette, A.M.; Hill, T.D. An examination of processes linking perceived neighborhood disorder and obesity. Soc. Sci. Med. 2008, 67, 38–46. [Google Scholar] [CrossRef] [PubMed]
- Rundle, A.; Roux, A.V.D.; Freeman, L.M.; Miller, D.; Neckerman, K.M.; Weiss, C.C. The Urban Built Environment and Obesity in New York City: A Multilevel Analysis. Am. J. Health Promot. 2007, 21, 326–334. [Google Scholar] [CrossRef] [PubMed]
- Renalds, A.; Smith, T.H.; Hale, P.J. A systematic review of built environment and health. Fam. Community Health 2010, 33, 68–78. [Google Scholar] [CrossRef] [PubMed]
- Stevenson, M.; Thompson, J.; de Sá, T.H.; Ewing, R.; Mohan, D.; McClure, R.; Roberts, I.; Tiwari, G.; Giles-Corti, B.; Sun, X. Land use, transport, and population health: Estimating the health benefits of compact cities. Lancet 2016, 388, 2925–2935. [Google Scholar] [CrossRef] [Green Version]
- Manaugh, K.; Kreider, T. What is mixed use? Presenting an interaction method for measuring land use mix. J. Transp. Land Use 2013, 6, 63–72. [Google Scholar] [CrossRef]
- Remigio, R.V.; Zulaika, G.; Rabello, R.S.; Bryan, J.; Sheehan, D.M.; Galea, S.; Carvalho, M.S.; Rundle, A.; Lovasi, G.S. A Local View of Informal Urban Environments: A Mobile Phone-Based Neighborhood Audit of Street-Level Factors in a Brazilian Informal Community. J. Urban Health 2019, 96, 537–548. [Google Scholar] [CrossRef]
- Russakovsky, O.; Deng, J.; Su, H.; Krause, J.; Satheesh, S.; Ma, S.; Huang, Z.; Karpathy, A.; Khosla, A.; Bernstein, M. Imagenet large scale visual recognition challenge. Int. J. Comput. Vis. 2015, 115, 211–252. [Google Scholar] [CrossRef] [Green Version]
- Abadi, M.; Barham, P.; Chen, J.; Chen, Z.; Davis, A.; Dean, J.; Devin, M.; Ghemawat, S.; Irving, G.; Isard, M. Tensorflow: A System for Large-Scale Machine Learning. In Proceedings of the 12th {USENIX} Symposium on Operating Systems Design and Implementation ({OSDI} 16), Savannah, GA, USA, 2–4 November 2016; pp. 265–283. [Google Scholar]
- Census Bureau. Census Tracts and Block Numbering Areas. Available online: https://www2.census.gov/geo/pdfs/reference/GARM/Ch10GARM.pdf (accessed on 19 November 2020).
- Phan, L.; Yu, W.; Keralis, J.M.; Mukhija, K.; Dwivedi, P.; Brunisholz, K.D.; Javanmardi, M.; Tasdizen, T.; Nguyen, Q.C. Google Street View Derived Built Environment Indicators and Associations with State-Level Obesity, Physical Activity, and Chronic Disease Mortality in the United States. Int. J. Environ. Res. Public Health 2020, 17, 3659. [Google Scholar] [CrossRef]
- Nguyen, Q.C.; Keralis, J.M.; Dwivedi, P.; Ng, A.E.; Javanmardi, M.; Khanna, S.; Huang, Y.; Brunisholz, K.D.; Kumar, A.; Tasdizen, T. Leveraging 31 Million Google Street View Images to Characterize Built Environments and Examine County Health Outcomes. Public Health Rep. 2020, 136, 201–211. [Google Scholar] [CrossRef]
- Casciano, R.; Massey, D.S. Neighborhood disorder and anxiety symptoms: New evidence from a quasi-experimental study. Health Place 2012, 18, 180–190. [Google Scholar] [CrossRef] [Green Version]
- Bjornstrom, E.E.S.; Ralston, M.L.; Kuhl, D.C. Social Cohesion and Self-Rated Health: The Moderating Effect of Neighborhood Physical Disorder. Am. J. Community Psychol. 2013, 52, 302–312. [Google Scholar] [CrossRef] [PubMed]
- U.S. Census Bureau. QuickFacts: Utah. Available online: https://www.census.gov/quickfacts/UT (accessed on 15 June 2021).
- Li, F.; Fisher, K.J.; Brownson, R.C.; Bosworth, M. Multilevel modelling of built environment characteristics related to neighbourhood walking activity in older adults. J. Epidemiol. Community Health 2005, 59, 558–564. [Google Scholar] [CrossRef] [PubMed] [Green Version]
| N a | Mean (Standard Deviation)/% (95% CI) | |
|---|---|---|
| Individual-level covariates | ||
| Age (years) | 1,433,316 | 46.53 (19.03) |
| % Female | 1,433,316 | 54.36% (54.28–54.45) |
| % Married | 1,069,207 | 58.06% (57.98–58.14) |
| % White | 1,346,584 | 95.39% (95.35–95.42) |
| % Hispanic ethnicity | 1,357,627 | 10.83% (10.78–10.88) |
| % Uninsured | 1,433,316 | 28.39% (28.31–28.46) |
| % Religious affiliation | 1,069,207 | 68.17% (68.08–68.25) |
| Area deprivation index | 1,433,298 | 97.51 (18.61) |
| Health outcomes | ||
| % Obesity | 1,374,731 | 47.28% (47.19–47.36) |
| % Diabetes | 1,433,316 | 5.88% (5.84–5.92) |
| Hemoglobin A1c (%) | 1,433,316 | 9.23% (9.18–9.28) |
| % Hypertension | 1,433,316 | 0.69% (0.68–0.71) |
| Google Street View (Census tract) | ||
| Green street | 1,394,442 | 83.76 (12.68) |
| Crosswalk | 1,394,442 | 4.95 (3.82) |
| Non-single-family home b | 1,394,442 | 27.53 (17.24) |
| Single-lane road | 1,394,442 | 65.56 (11.65) |
| Visible utility wires | 1,394,442 | 46.19 (14.36) |
| Diabetes | Uncontrolled Diabetes | Hypertension | Obesity | Substance Use Disorder | |
|---|---|---|---|---|---|
| Prevalence Ratio (95% CI) b | Prevalence Ratio (95% CI) b | Prevalence Ratio (95% CI) b | Prevalence Ratio (95% CI) b | Prevalence Ratio (95% CI) b | |
| GSV indicators | |||||
| Green streets, 3rd tertile | 0.90 (0.88, 0.92) * | 0.89 (0.86, 0.92) * | 0.84 (0.78, 0.90) * | 0.90 (0.89, 0.91) * | 1.17 (1.13, 1.21) * |
| Green streets, 2nd tertile | 0.99 (0.97, 1.01) | 0.98 (0.95, 1.01) | 0.98 (0.93, 1.05) | 0.98 (0.97, 0.98) * | 1.06 (1.03, 1.09) * |
| Crosswalks, 3rd tertile | 1.02 (1.00, 1.05) * | 1.01 (0.98, 1.04) | 1.07 (1.00, 1.14) * | 1.01 (1.00, 1.02) * | 1.00 (0.97, 1.03) |
| Crosswalks, 2nd tertile | 1.01 (0.99, 1.03) | 1.00 (0.98, 1.03) | 1.09 (1.02, 1.16) * | 1.02 (1.01, 1.02) * | 0.99 (0.96, 1.02) |
| Non-single-family home, 3rd tertile | 0.83 (0.81, 0.85) * | 0.86 (0.82, 0.89) * | 0.73 (0.67, 0.80) * | 0.89 (0.88, 0.90) * | 1.12 (1.08, 1.17) * |
| Non-single-family home, 2nd tertile | 0.91 (0.89, 0.93) * | 0.91 (0.88, 0.94) * | 0.89 (0.83, 0.96) * | 0.95 (0.95, 0.96) * | 1.03 (0.99, 1.06) |
| Single-lane roads, 3rd tertile | 1.02 (0.99, 1.04) | 1.00 (0.97, 1.04) | 0.94 (0.87, 1.01) | 1.00 (0.99, 1.01) | 0.98 (0.95, 1.02) |
| Single-lane roads, 2nd tertile | 1.03 (1.01, 1.05) * | 1.01 (0.99, 1.04) | 0.98 (0.92, 1.04) | 1.00 (1.00, 1.01) | 0.97 (0.94, 1.00) |
| Visible wires, 3rd tertile | 1.09 (1.06, 1.11) * | 1.10 (1.06, 1.14) * | 1.05 (0.97, 1.14) | 1.04 (1.03, 1.06) * | 1.05 (1.01, 1.09) * |
| Visible wires, 2nd tertile | 1.09 (1.07, 1.12) * | 1.10 (1.07, 1.13) * | 1.08 (1.01, 1.16) * | 1.05 (1.04, 1.05) * | 0.99 (0.96, 1.02) |
| Covariates | |||||
| Age (years) | 1.04 (1.04, 1.04) * | 1.03 (1.03, 1.03) * | 1.01 (1.01, 1.01) * | 1.01 (1.01, 1.01) * | 1.00 (1.00, 1.00) |
| White race | 0.60 (0.58, 0.62) * | 0.53 (0.51, 0.55) * | 0.80 (0.72, 0.90) * | 0.93 (0.91, 0.94) * | 1.16 (1.10, 1.22) * |
| Hispanic ethnicity | 1.15 (1.12, 1.18) * | 1.34 (1.30, 1.39) * | 0.96 (0.88, 1.05) | 1.08 (1.07, 1.09) * | 0.68 (0.65, 0.70) * |
| Any religion | 1.21 (1.19, 1.23) * | 1.18 (1.15, 1.21) * | 0.86 (0.82, 0.91) * | 1.07 (1.06, 1.07) * | 0.65 (0.64, 0.67) * |
| Married | 1.09 (1.07, 1.11) * | 1.03 (1.01, 1.05) * | 1.40 (1.33, 1.48) * | 1.12 (1.11, 1.13) * | 0.40 (0.39, 0.41) * |
| Uninsured | 1.60 (1.57, 1.63) * | 1.73 (1.69, 1.77) * | 1.11 (1.05, 1.17) * | 1.10 (1.09, 1.11) * | 2.38 (2.33, 2.44) * |
| Area deprivation index | 1.01 (1.01, 1.01) * | 1.01 (1.01, 1.01) * | 1.00 (1.00, 1.00) * | 1.01 (1.01, 1.01) * | 1.01 (1.01, 1.01) * |
| Prevalence Ratio (95% CI) | |
|---|---|
| GSV indicators | |
| Green streets, 3rd tertile | 0.89 (0.87, 0.92) * |
| Green streets, 2nd tertile | 1.01 (0.99, 1.03) |
| Crosswalks, 3rd tertile | 1.08 (1.05, 1.10) * |
| Crosswalks, 2nd tertile | 1.06 (1.04, 1.08) * |
| Non-single-family home, 3rd tertile | 0.85 (0.83, 0.87) * |
| Non-single-family home, 2nd tertile | 0.88 (0.86, 0.90) * |
| Single-lane roads, 3rd tertile | 1.06 (1.03, 1.08) * |
| Single-lane roads, 2nd tertile | 1.04 (1.01, 1.06) * |
| Visible wires, 3rd tertile | 1.32 (1.29, 1.35) * |
| Visible wires, 2nd tertile | 1.23 (1.20, 1.25) * |
| Covariates | |
| Age (years) | 1.04 (1.04, 1.04) * |
| White race | 0.57 (0.55, 0.59) * |
| Hispanic ethnicity | 1.33 (1.29, 1.36) * |
| Any religion | 1.23 (1.21, 1.25) * |
| Married | 1.03 (1.01, 1.05) * |
| Built Environment Indicators | |||||
|---|---|---|---|---|---|
| Census Tract Characteristics a | Green Space | Crosswalk | Non-Single-Family Home | Single-Lane Roads | Visible Wire |
| Prevalence (95% CI) | Prevalence (95% CI) | Prevalence (95% CI) | Prevalence (95% CI) | Prevalence (95% CI) | |
| % non-Hispanic Black | −43.68 (−60.61, −26.74) * | 13.84 (9.08, 18.61) * | 70.67 (48.88, 92.45) * | −67.12 (−84.09, −50.16) * | 51.00 (32.75, 69.24) * |
| % Hispanic | 0.16 (−2.00, 2.32) | −0.38 (−0.99, 0.23) | −3.50 (−6.28, −0.72) * | 4.01 (1.85, 6.18) * | 2.54 (0.21, 4.86) * |
| % Unemployed | 1.72 (0.07, 3.36) * | 0.34 (−0.13, 0.80) | 0.83 (−1.29, 2.95) | −0.57 (−2.22, 1.08) | −0.26 (−2.04, 1.52) |
| Median household income | 7.46 (5.75, 9.17) * | −0.70 (−1.18, −0.22) * | −11.59 (−13.79, −9.39) * | 5.68 (3.97, 7.40) * | −10.55 (−12.39, −8.70) * |
| Household size | −2.96 (−3.89, −2.04) * | −0.76 (−1.02, −0.50) * | −2.56 (−3.75, −1.36) * | −0.33 (−1.26, 0.60) | −0.09 (−1.09, 0.91) |
| Population density | 5.90 (5.00, 6.80) * | 1.57 (1.32, 1.83) * | −5.65 (−6.81, −4.50) * | 0.95 (0.05, 1.85) * | −2.69 (−3.66, −1.73) * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nguyen, Q.C.; Belnap, T.; Dwivedi, P.; Deligani, A.H.N.; Kumar, A.; Li, D.; Whitaker, R.; Keralis, J.; Mane, H.; Yue, X.; et al. Google Street View Images as Predictors of Patient Health Outcomes, 2017–2019. Big Data Cogn. Comput. 2022, 6, 15. https://doi.org/10.3390/bdcc6010015
Nguyen QC, Belnap T, Dwivedi P, Deligani AHN, Kumar A, Li D, Whitaker R, Keralis J, Mane H, Yue X, et al. Google Street View Images as Predictors of Patient Health Outcomes, 2017–2019. Big Data and Cognitive Computing. 2022; 6(1):15. https://doi.org/10.3390/bdcc6010015
Chicago/Turabian StyleNguyen, Quynh C., Tom Belnap, Pallavi Dwivedi, Amir Hossein Nazem Deligani, Abhinav Kumar, Dapeng Li, Ross Whitaker, Jessica Keralis, Heran Mane, Xiaohe Yue, and et al. 2022. "Google Street View Images as Predictors of Patient Health Outcomes, 2017–2019" Big Data and Cognitive Computing 6, no. 1: 15. https://doi.org/10.3390/bdcc6010015
APA StyleNguyen, Q. C., Belnap, T., Dwivedi, P., Deligani, A. H. N., Kumar, A., Li, D., Whitaker, R., Keralis, J., Mane, H., Yue, X., Nguyen, T. T., Tasdizen, T., & Brunisholz, K. D. (2022). Google Street View Images as Predictors of Patient Health Outcomes, 2017–2019. Big Data and Cognitive Computing, 6(1), 15. https://doi.org/10.3390/bdcc6010015