
Have Hand Hygiene Practices in Two Tertiary Care Hospitals, Freetown, Sierra Leone, Improved in 2023 following Operational Research in 2021?

 , , , , ,
, , , , ,  ,
,  , , and
, , and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Setting
2.2.1. General Setting
2.2.2. Site-Specific Setting
2.3. Study Population
2.4. Study Procedures
2.4.1. Dissemination Activities, Recommendations and Interventions
2.4.2. Hand Hygiene Compliance
2.5. Data Variables and Sources of Data
2.6. Analysis and Statistics
3. Results
3.1. Dissemination, Trainings, Recommendations and Actions following the 2021 Study
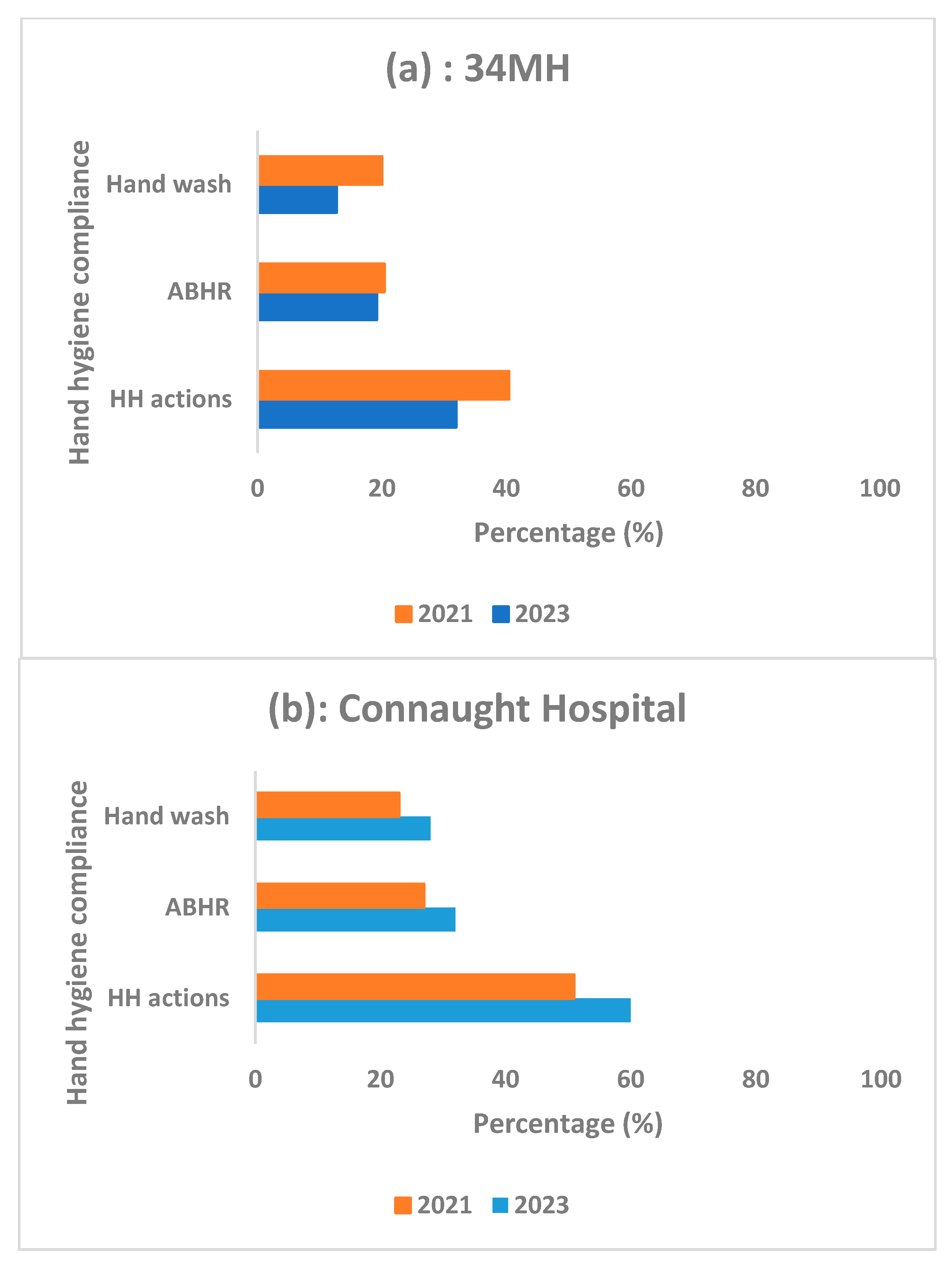
3.2. Comparison of Hand Hygiene Actions between the Two Hospitals
3.3. Hand Hygiene Actions in Relation to Five Opportunities
3.4. Hand Hygiene Actions in Relation to Hospital Departments/Wards
3.5. Hand Hygiene Actions in Relation to Type of Healthcare Worker
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Open Access Statement
References
- World Health Organizaton (WHO). Report on the Burden of Endemic Health Care-Associated Infection Worldwide; WHO: Geneva, Switzerland, 2011. [Google Scholar]
- Allegranzi, B.; Nejad, S.B.; Combescure, C.; Graafmans, W.; Attar, H.; Donaldson, L.; Pittet, D. Burden of Endemic Health-Care-Associated Infection in Developing Countries: Systematic Review and Meta-Analysis. Lancet 2011, 377, 228–241. [Google Scholar] [CrossRef]
- Allegranzi, B.; Pittet, D. Role of Hand Hygiene in Healthcare-Associated Infection Prevention. J. Hosp. Infect. 2009, 73, 305–315. [Google Scholar] [CrossRef]
- Kingston, L.; O’Connell, N.H.; Dunne, C.P. Hand Hygiene-Related Clinical Trials Reported since 2010: A Systematic Review. J. Hosp. Infect. 2016, 92, 309–320. [Google Scholar] [CrossRef]
- World Health Organization (WHO). WHO Guidelines on Hand Hygiene in Health Care; WHO: Geneva, Switzerland, 2009. [Google Scholar]
- Allegranzi, B.; Gayet-Ageron, A.; Damani, N.; Bengaly, L.; McLaws, M.L.; Moro, M.L.; Memish, Z.; Urroz, O.; Richet, H.; Storr, J.; et al. Global Implementation of WHO’s Multimodal Strategy for Improvement of Hand Hygiene: A Quasi-Experimental Study. Lancet Infect. Dis. 2013, 13, 843–851. [Google Scholar] [CrossRef]
- World Health Organizaton (WHO). Hand Hygiene Technical Reference Manual; WHO: Geneva, Switzerland, 2009. [Google Scholar]
- Holmen, I.C.; Seneza, C.; Nyiranzayisaba, B.; Nyiringabo, V.; Bienfait, M.; Safdar, N. Improving Hand Hygiene Practices in a Rural Hospital in Sub-Saharan Africa. Infect. Control Hosp. Epidemiol. 2016, 37, 834–839. [Google Scholar] [CrossRef]
- Labi, A.K.; Obeng-Nkrumah, N.; Nuertey, B.D.; Issahaku, S.; Ndiaye, N.F.; Baffoe, P.; Dancun, D.; Wobil, P.; Enweronu-Laryea, C. Hand Hygiene Practices and Perceptions among Healthcare Workers in Ghana: A WASH Intervention Study. J. Infect. Dev. Ctries 2019, 13, 1076–1085. [Google Scholar] [CrossRef]
- Uneke, C.J.; Ndukwe, C.D.; Oyibo, P.G.; Nwakpu, K.O.; Nnabu, R.C.; Prasopa-Plaizier, N. Promotion of Hand Hygiene Strengthening Initiative in a Nigerian Teaching Hospital: Implication for Improved Patient Safety in Low-Income Health Facilities. Braz. J. Infect. Dis. 2014, 18, 21–27. [Google Scholar] [CrossRef]
- Müller, S.A.; Diallo, A.O.K.; Wood, R.; Bayo, M.; Eckmanns, T.; Tounkara, O.; Arvand, M.; Diallo, M.; Borchert, M. Implementation of the WHO Hand Hygiene Strategy in Faranah Regional Hospital, Guinea. Antimicrob. Resist. Infect. Control 2020, 9, 65. [Google Scholar] [CrossRef]
- Wiedenmayer, K.; Msamba, V.-S.; Chilunda, F.; Kiologwe, J.C.; Seni, J. Impact of Hand Hygiene Intervention: A Comparative Study in Health Care Facilities in Dodoma Region, Tanzania Using WHO Methodology. Antimicrob. Resist. Infect. Control 2020, 9, 80. [Google Scholar] [CrossRef]
- Government of Sierra Leone. National Strategic Plan for Combating Antimicrobial Resistance 2018–2022; World Health Organization: Freetown, Sierra Leone, 2018.
- Kamara, G.N.; Sevalie, S.; Molleh, B.; Koroma, Z.; Kallon, C.; Maruta, A.; Kamara, I.F.; Kanu, J.S.; Campbell, J.S.O.; Shewade, H.D.; et al. Hand Hygiene Compliance at Two Tertiary Hospitals in Freetown, Sierra Leone, in 2021: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2022, 19, 2978. [Google Scholar] [CrossRef]
- Special Programme for Research & Training in Tropical Diseases (TDR). AMR-SORT IT Evidence Summaries: Communicating Research Findings. Available online: https://tdr.who.int/activities/sort-it-operational-research-and-training/communicating-research-findings (accessed on 5 June 2023).
- Statistics Sierra Leone. 2021 Mid Term Population and Housing Census. Provisional Results; Statistics Sierra Leone: Freetown, Sierra Leone, 2021. [Google Scholar]
- 34th Military Hospital Statistics. Annual Patient Admissions; 34th Military Hospital Statistics: Freetown, Sierra Leone, 2019. [Google Scholar]
- Lakoh, S.; Jiba, D.F.; Kanu, J.E.; Poveda, E.; Salgado-Barreira, A.; Sahr, F.; Sesay, M.; Deen, G.F.; Sesay, T.; Gashau, W.; et al. Causes of Hospitalization and Predictors of HIV-Associated Mortality at the Main Referral Hospital in Sierra Leone: A Prospective Study. BMC Public Health 2019, 19, 1320. [Google Scholar] [CrossRef]
- Special Programme for Research & Training in Tropical Diseases (TDR). SORT IT—Operational Research and Training. Available online: https://tdr.who.int/activities/sort-it-operational-research-and-training# (accessed on 5 June 2023).
- Chen, L.F.; Vander Weg, M.W.; Hofmann, D.A.; Reisinger, H.S. The Hawthorne Effect in Infection Prevention and Epidemiology. Infect. Control Hosp. Epidemiol. 2015, 36, 1444–1450. [Google Scholar] [CrossRef]
- Luangasanatip, N.; Hongsuwan, M.; Limmathurotsakul, D.; Lubell, Y.; Lee, A.S.; Harbarth, S.; Day, N.P.J.; Graves, N.; Cooper, B.S. Comparative Efficacy of Interventions to Promote Hand Hygiene in Hospital: Systematic Review and Network Meta-Analysis. BMJ 2015, 351, h3728. [Google Scholar] [CrossRef]
- Huis, A.; van Achterberg, T.; de Bruin, M.; Grol, R.; Schoonhoven, L.; Hulscher, M. A Systematic Review of Hand Hygiene Improvement Strategies: A Behavioural Approach. Implement. Sci. 2012, 7, 92. [Google Scholar] [CrossRef]
- Omuemu, V.; Ogboghodo, E.; Opene, R.; Oriarewo, P.; Onibere, O. Hand Hygiene Practices among Doctors in a Tertiary Health Facility in Southern Nigeria. J. Med. Trop. 2013, 15, 96. [Google Scholar] [CrossRef]
- Engdaw, G.T.; Gebrehiwot, M.; Andualem, Z. Hand Hygiene Compliance and Associated Factors among Health Care Providers in Central Gondar Zone Public Primary Hospitals, Northwest Ethiopia. Antimicrob. Resist. Infect. Control 2019, 8, 190. [Google Scholar] [CrossRef]
- Alene, M.; Tamiru, D.; Bazie, G.W.; Mebratu, W.; Kebede, N. Hand Hygiene Compliance and Its Associated Factors among Health Care Providers in Primary Hospitals of Waghimira Zone, Northeast Ethiopia: A Mixed Study Design. Antimicrob. Resist. Infect. Control 2022, 11, 75. [Google Scholar] [CrossRef]
- Daba, C.; Atamo, A.; Debela, S.A.; Gebrehiwot, M. Observational Assessment of Hand Hygiene Compliance among Healthcare Workers in Public Hospitals of Northeastern Ethiopia. Int. J. Environ. Health Res. 2023; online ahead of print. [Google Scholar]
- Soboksa, N.E.; Negassa, B.; Kanno, G.; Ashuro, Z.; Gudeta, D. Hand Hygiene Compliance and Associated Factors among Healthcare Workers in Ethiopia: A Systematic Review and Meta-Analysis. Adv. Prev. Med. 2021, 2021, 7235248. [Google Scholar] [CrossRef]
- Ogbonnaya, G.U.; Ogbonnaya, U.L.; Nwamoh, U.N.; Nwokeukwu, H.I.; Odeyemi, K.A. Five Moments for Hand Hygiene: A Study of Compliance among Healthcare Workers in a Tertiary Hospital in South East Nigeria. Community Med. Public Health Care 2015, 2, 1–4. [Google Scholar] [CrossRef][Green Version]
- Onyedibe, K.I.; Shehu, N.Y.; Pires, D.; Isa, S.E.; Okolo, M.O.; Gomerep, S.S.; Ibrahim, C.; Igbanugo, S.J.; Odesanya, R.U.; Olayinka, A.; et al. Assessment of Hand Hygiene Facilities and Staff Compliance in a Large Tertiary Health Care Facility in Northern Nigeria: A Cross Sectional Study. Antimicrob. Resist. Infect. Control 2020, 9, 30. [Google Scholar] [CrossRef]
- Tesfaye, G.; Gebrehiwot, M.; Girma, H.; Malede, A.; Bayu, K.; Adane, M. Application of the Gold Standard Direct Observation Tool to Estimate Hand Hygiene Compliance among Healthcare Providers in Dessie Referral Hospital, Northeast Ethiopia. Int. J. Environ. Health Res. 2022, 32, 2533–2546. [Google Scholar] [CrossRef]
- Abuosi, A.A.; Akoriyea, S.K.; Ntow-Kummi, G.; Akanuwe, J.; Abor, P.A.; Daniels, A.A.; Alhassan, R.K. Hand Hygiene Compliance among Healthcare Workers in Ghana’s Health Care Institutions: An Observational Study. J. Patient Saf. Risk Manag. 2020, 25, 177–186. [Google Scholar] [CrossRef]
- Lakoh, S.; Firima, E.; Williams, C.E.E.; Conteh, S.K.; Jalloh, M.B.; Sheku, M.G.; Adekanmbi, O.; Sevalie, S.; Kamara, S.A.; Kamara, M.A.S.; et al. An Intra-COVID-19 Assessment of Hand Hygiene Facility, Policy and Staff Compliance in Two Hospitals in Sierra Leone: Is There a Difference between Regional and Capital City Hospitals? Trop. Med. Infect. Dis. 2021, 6, 204. [Google Scholar] [CrossRef]
- Chang, N.C.N.; Schweizer, M.L.; Reisinger, H.S.; Jones, M.; Chrischilles, E.; Chorazy, M.; Huskins, W.C.; Herwaldt, L. The Impact of Workload on Hand Hygiene Compliance: Is 100% Compliance Achievable? Infect. Control Hosp. Epidemiol. 2022, 43, 1259–1261. [Google Scholar] [CrossRef]
- Umar, H.; Geremew, A.; Worku Kassie, T.; Dirirsa, G.; Bayu, K.; Mengistu, D.A.; Berhanu, A.; Mulat, S. Hand Hygiene Compliance and Associated Factor among Nurses Working in Public Hospitals of Hararghe Zones, Oromia Region, Eastern Ethiopia. Front. Public Health 2022, 10, 1032167. [Google Scholar] [CrossRef]
- Lambe, K.A.; Lydon, S.; Madden, C.; Vellinga, A.; Hehir, A.; Walsh, M.; O’Connor, P. Hand Hygiene Compliance in the ICU: A Systematic Review. Crit. Care Med. 2019, 47, 1251–1257. [Google Scholar] [CrossRef]
- Hoffmann, M.; Sendlhofer, G.; Gombotz, V.; Pregartner, G.; Zierler, R.; Schwarz, C.; Tax, C.; Brunner, G. Hand Hygiene Compliance in Intensive Care Units: An Observational Study. Int. J. Nurs. Pract. 2020, 26, e12789. [Google Scholar] [CrossRef]
- Bangura, I.A. The Impact of Multimodal Strategy Intervention Program on Hand Hygiene Compliance at a University Teaching Hospital in Sierra Leone (Ola During Children’s Hospital). Infect. Control Hosp. Epidemiol. 2020, 41, s498–s499. [Google Scholar] [CrossRef]
- Irek, E.O.; Aliyu, A.A.; Dahiru, T.; Obadare, T.O.; Aboderin, A.O. Healthcare-Associated Infections and Compliance of Hand Hygiene among Healthcare Workers in a Tertiary Health Facility, Southwest Nigeria. J. Infect. Prev. 2019, 20, 289–296. [Google Scholar] [CrossRef]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for Reporting Observational Studies. Lancet 2007, 370, 1453–1457. [Google Scholar] [CrossRef]
- Purssell, E.; Drey, N.; Chudleigh, J.; Creedon, S.; Gould, D.J. The Hawthorne Effect on Adherence to Hand Hygiene in Patient Care. J. Hosp. Infect. 2020, 106, 311–317. [Google Scholar] [CrossRef]
- Ibrahim, U.M.; Gajida, A.U.; Garba, R.M.; Gadanya, M.A.; Umar, A.A.; Jalo, R.I.; Adamu, A.L.; Ismai, F.; Tsiga-Ahmed; Gwarzo, D.H.; et al. Effect of Voice Reminder on Compliance with Recommended Hand Hygiene Practise among Health-Care Workers in Kano Metropolis. Niger. Postgrad. Med. J. 2021, 28, 94–101. [Google Scholar] [CrossRef] [PubMed]
- Ojanperä, H.; Ohtonen, P.; Kanste, O.; Syrjälä, H. Impact of Direct Hand Hygiene Observations and Feedback on Hand Hygiene Compliance among Nurses and Doctors in Medical and Surgical Wards: An Eight-Year Observational Study. J. Hosp. Infect. 2022, 127, 83–90. [Google Scholar] [CrossRef]


{kind=link}
| Recommendation | Action | Medicine | Surgery | Paediatrics | Accident and Emergency | Intensive Care | Obstetrics/ Gynaecology |
|---|---|---|---|---|---|---|---|
| 34MH | |||||||
| Place HH reminders/job aids in hospital departments | No. HH reminders and job aids placed on walls or tables | 3 | 2 | 1 | 2 | - | 2 |
| Improve hand wash infrastructure at hand wash stations | No. Hand wash stations | 3 | 2 | 1 | 2 | - | 2 |
| No. Running taps | 0 | 0 | 0 | 0 | - | 2 | |
| No. Veronica buckets | 3 | 2 | 1 | 2 | - | 2 | |
| No. Receiving bowls | 3 | 2 | 1 | 2 | - | 2 | |
| No. Soap items | 2 | 2 | 0 | 2 | - | 2 | |
| No. Paper towels | 0 | 0 | 0 | 0 | - | 0 | |
| No. ABHR | 1 | 1 | 0 | 1 | - | 1 | |
| Improve ABHR Supplies | ABHR supplied monthly | Yes | Yes | No | Yes | - | Yes |
| ABHR missing monthly | No | No | No | No | - | No | |
| Connaught Hospital | |||||||
| Place HH reminders/job aids in hospital departments | No. HH reminders and job aids placed on walls or Tables | 18 | 16 | 6 | 8 | 8 | - |
| Improve hand wash infrastructure at hand wash stations | No. Hand wash stations | 16 | 16 | 6 | 8 | 6 | - |
| No. Running taps | 8 | 8 | 4 | 4 | 4 | - | |
| No. Veronica buckets | 8 | 8 | 2 | 4 | 2 | - | |
| No. Receiving bowls | 8 | 8 | 2 | 4 | 2 | - | |
| No. Soap items | 16 | 16 | 4 | 6 | 6 | - | |
| No. Paper towels | 0 | 0 | 0 | 0 | 0 | - | |
| No. ABHR | 8 | 8 | 2 | 2 | 2 | - | |
| Improve ABHR Supplies | ABHR supplied monthly | Yes | Yes | Yes | Yes | Yes | - |
| ABHR missing monthly | No | No | No | No | Yes | - | |
| Hospital and Type of HH Action | June to August 2021 | February to April 2023 | Change in HH Compliance 2023 v 2021 | p Value | ||||
|---|---|---|---|---|---|---|---|---|
| Opportunities for HH Action | HH Actions Performed | Opportunities for HH Action | HH Actions Performed | |||||
| n | n | (%) | n | n | (%) | |||
| 34MH | ||||||||
| Total opportunities: | 2072 | 838 | (40) | 4529 | 1446 | (32) |  | <0.001 |
| Bef-pat | 602 | 120 | (20) | 1189 | 140 | (12) | | <0.001 |
| Bef-aspet | 285 | 89 | (31) | 265 | 25 | (9) | | <0.001 |
| Aft-b.f. | 315 | 237 | (75) | 760 | 507 | (68) | | <0.001 |
| Aft-pat | 473 | 238 | (50) | 1537 | 593 | (39) | | <0.001 |
| Aft.p.surr. | 397 | 154 | (39) | 778 | 181 | (23) | | <0.001 |
| Not recorded | - | - | - | - | - | - | ||
| Connaught Hospital | ||||||||
| Total opportunities: | 8389 | 4248 | (51) | 2677 | 1605 | (60) |  | <0.001 |
| Bef-pat | 2642 | 672 | (25) | 630 | 151 | (24) |  | 0.45 |
| Bef-aspet | 754 | 261 | (35) | 84 | 61 | (73) | | <0.001 |
| Aft-b.f. | 685 | 543 | (79) | 297 | 288 | (97) | | <0.001 |
| Aft-pat | 2248 | 1539 | (69) | 1119 | 920 | (82) | | <0.001 |
| Aft.p.surr. | 2050 | 1228 | (60) | 547 | 185 | (34) | | <0.001 |
| Not recorded | 10 | 5 | (50) | 0 | 0 | (0) | ||
| Hospital and Department/Ward | June to August 2021 | February to April 2023 | Change in HH Compliance 2023 v 2021 | p Value | ||||
|---|---|---|---|---|---|---|---|---|
| Opportunities for HH Action | HH actions Performed | Opportunities for HH Action | HH Actions Performed | |||||
| n | n | (%) | n | n | (%) | |||
| 34MH | ||||||||
| Total opportunities | 2072 | 838 | (40) | 4529 | 1446 | (32) | | <0.001 |
| Medical ward | 401 | 161 | (40) | 911 | 304 | (33) | | 0.02 |
| Surgical ward | 555 | 214 | (39) | 960 | 317 | (33) | | 0.03 |
| Paediatric ward | 78 | 42 | (54) | 764 | 239 | (31) | | <0.001 |
| Accident and Emergency | 413 | 187 | (45) | 1118 | 331 | (30) | | <0.001 |
| Obstetrics/Gynaecology | 468 | 157 | (34) | 776 | 255 | (33) | | <0.001 |
| Not recorded | 157 | 77 | (49) | 0 | 0 | (0) | ||
| Connaught Hospital | ||||||||
| Total opportunities | 8389 | 4248 | (51) | 2677 | 1605 | (60) | | <0.001 |
| Medical ward | 3088 | 1427 | (46) | 916 | 562 | (61) | | <0.001 |
| Surgical ward | 2271 | 1195 | (53) | 1002 | 614 | (61) | | <0.001 |
| Paediatric ward | 263 | 165 | (63) | 174 | 114 | (66) | | 0.55 |
| Intensive care | 536 | 279 | (52) | 129 | 90 | (70) | | <0.001 |
| Accident and Emergency | 231 | 130 | (56) | 456 | 225 | (49) | | 0.09 |
| Obstetrics/Gynaecology | 31 | 11 | (36) | - | - | - | ||
| Not recorded | 1969 | 1041 | (53) | 0 | 0 | (0) | ||
| Hospital and Department/Ward | June to August 2021 | February to April 2023 | Change in HH Compliance 2023 v 2021 | p Value | ||||
|---|---|---|---|---|---|---|---|---|
| Opportunities for HH Action | HH actions Performed | Opportunities for HH Action | HH Actions Performed | |||||
| n | n | (%) | n | n | (%) | |||
| 34MH | ||||||||
| Total opportunities | 2072 | 838 | (40) | 4529 | 1446 | (32) | | <0.001 |
| Doctor | 347 | 131 | (38) | 911 | 545 | (60) | | <0.001 |
| Nurse | 1582 | 664 | (42) | 2388 | 627 | (26) | | <0.001 |
| Nursing student | 62 | 30 | (48) | 564 | 154 | (27) | | <0.001 |
| Laboratory technician | 81 | 13 | (16) | 666 | 120 | (18) | | 0.66 |
| Not recorded | - | - | - | - | - | - | ||
| Connaught Hospital | ||||||||
| Total opportunities | 8389 | 4248 | (51) | 2677 | 1605 | (60) | | <0.001 |
| Doctor | 1892 | 842 | (45) | 633 | 340 | (54) | | <0.001 |
| Nurse | 5112 | 2846 | (56) | 1413 | 856 | (61) | | <0.001 |
| Nursing student | 1032 | 486 | (47) | 389 | 279 | (72) | | <0.001 |
| Laboratory technician | 351 | 72 | (21) | 242 | 130 | (54) | | <0.001 |
| Not recorded | 2 | 2 | (100) | 0 | 0 | (0) | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moiwo, M.M.; Kamara, G.N.; Kamara, D.; Kamara, I.F.; Sevalie, S.; Koroma, Z.; Kamara, K.N.; Kamara, M.N.; Kamara, R.Z.; Kpagoi, S.S.T.K.; et al. Have Hand Hygiene Practices in Two Tertiary Care Hospitals, Freetown, Sierra Leone, Improved in 2023 following Operational Research in 2021? Trop. Med. Infect. Dis. 2023, 8, 431. https://doi.org/10.3390/tropicalmed8090431
Moiwo MM, Kamara GN, Kamara D, Kamara IF, Sevalie S, Koroma Z, Kamara KN, Kamara MN, Kamara RZ, Kpagoi SSTK, et al. Have Hand Hygiene Practices in Two Tertiary Care Hospitals, Freetown, Sierra Leone, Improved in 2023 following Operational Research in 2021? Tropical Medicine and Infectious Disease. 2023; 8(9):431. https://doi.org/10.3390/tropicalmed8090431
Chicago/Turabian StyleMoiwo, Matilda Mattu, Gladys Nanilla Kamara, Dauda Kamara, Ibrahim Franklyn Kamara, Stephen Sevalie, Zikan Koroma, Kadijatu Nabie Kamara, Matilda N. Kamara, Rugiatu Z. Kamara, Satta Sylvia Theresa Kumba Kpagoi, and et al. 2023. "Have Hand Hygiene Practices in Two Tertiary Care Hospitals, Freetown, Sierra Leone, Improved in 2023 following Operational Research in 2021?" Tropical Medicine and Infectious Disease 8, no. 9: 431. https://doi.org/10.3390/tropicalmed8090431
APA StyleMoiwo, M. M., Kamara, G. N., Kamara, D., Kamara, I. F., Sevalie, S., Koroma, Z., Kamara, K. N., Kamara, M. N., Kamara, R. Z., Kpagoi, S. S. T. K., Konteh, S. A., Margao, S., Fofanah, B. D., Thomas, F., Kanu, J. S., Tweya, H. M., Shewade, H. D., & Harries, A. D. (2023). Have Hand Hygiene Practices in Two Tertiary Care Hospitals, Freetown, Sierra Leone, Improved in 2023 following Operational Research in 2021? Tropical Medicine and Infectious Disease, 8(9), 431. https://doi.org/10.3390/tropicalmed8090431