
Quality of Electronic TB Register Data Compared with Paper-Based Records in the Kyrgyz Republic

 ,
, 
Abstract
1. Introduction
- To assess the completeness and concordance of data in both the paper-based and electronic records in individuals with drug-sensitive pulmonary TB in two regions of the Kyrgyz Republic who were registered between June 2021 and May 2022.
- To compare the time from diagnosis to initiation of TB treatment and programmatic TB treatment outcomes in persons with drug-sensitive pulmonary TB in two regions of the Kyrgyz Republic who were registered in the paper-based system between January and December 2019 and in the electronic register system between June 2021 and May 2022, respectively.
2. Materials and Methods
2.1. Study Design
2.2. Setting: General and Specific
Specific Setting
2.3. Study Population
2.4. Definitions
- Paper-based records—the TB01 form used for all outpatients with TB.
- Electronic TB register—National database using the TB01 form for all persons diagnosed with TB since June 2021.
- Completeness of the records was measured as the proportion of data fields that were completed out of the total number of data fields for each data variable, and the percentage of data fields completed was also calculated for each variable.
- Concordance of records was assessed by comparing the number and percentage of fields with the same value, such as “male”, in the two data sources (the paper-based and the electronic records) for specified variables.
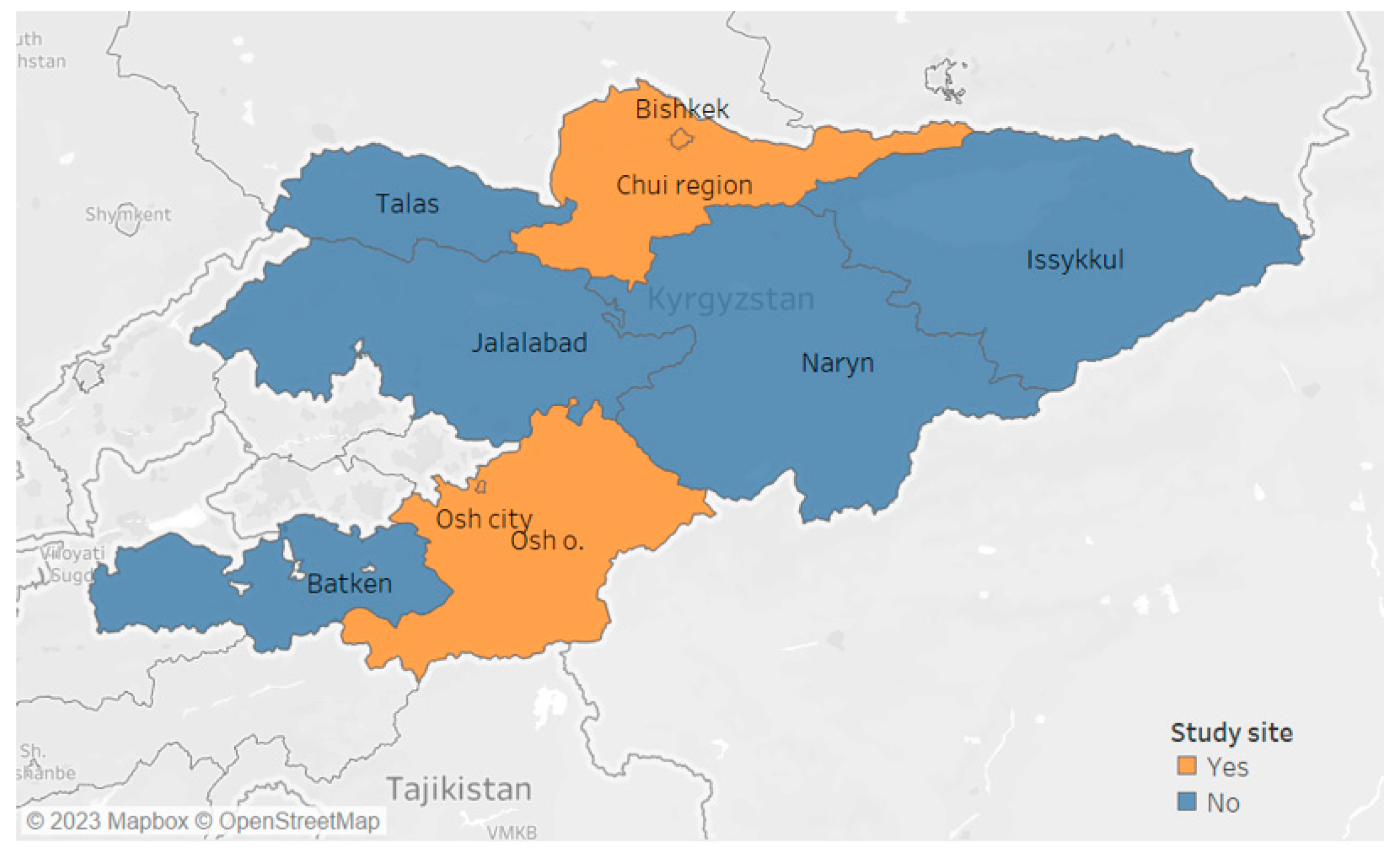
2.5. Study Sites
2.6. Data Variables Collected for Each Objective
2.6.1. Data Variables Shown in Relation to Study Objectives
2.6.2. Data Collection and Validation
2.7. Analysis and Statistics
2.7.1. Data Analysis
2.7.2. Sample Size Calculation
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Open Access Statement and Disclaimer
References
- Global Tuberculosis Report 2022 World Health Organization. 2022. Available online: https://www.who.int/teams/global-tuberculosis-programme/tb-reports/global-tuberculosis-report-2022 (accessed on 20 June 2023).
- World Health Organization. Kyrgyzstan. 2021. Available online: https://www.who.int/countries/kgz/en/ (accessed on 3 November 2022).
- World Health Organization & Society. Digital Health Technologies for TB Control: A Rapid Scan of Experience and Lessons Learned. 2015. Available online: https://www.who.int/tb/publications/digital-health-technologies-tb-control/en/ (accessed on 5 November 2022).
- Lee, Y.; Raviglione, M.C.; Flahault, A. Use of Digital Technology to Enhance Tuberculosis Control: Scoping Review. J. Med. Internet Res. 2020, 22, e15727. [Google Scholar] [CrossRef] [PubMed]
- Soltobekova, N.; Kozukeev, T.; Yiehdego, G.; Labib, F.; Hovhannesyan, A.; Rossi, R. Time to start of tuberculosis treatment in penitentiary system of Kyrgyz Republic: A retrospective cohort study. PLoS ONE 2022, 17, e0264252. [Google Scholar] [CrossRef] [PubMed]
- Williams, F.; Boren, S.A. The role of the electronic medical record (EMR) in care delivery development in developing countries: A systematic review. Inform. Prim. Care 2008, 16, 139–145. [Google Scholar] [CrossRef] [PubMed]
- Fritz, F.; Tilahun, B.; Dugas, M. Success criteria for electronic medical record implementations in low-resource settings: A systematic review. J. Am. Med. Inform. Assoc. JAMIA 2015, 22, 479–488. [Google Scholar] [CrossRef] [PubMed]
- Abiy, R.; Gashu, K.; Asemaw, T.; Mitiku, M.; Fekadie, B.; Abebaw, Z.; Mamuye, A.; Tazebew, A.; Teklu, A.; Nurhussien, F.; et al. A Comparison of Electronic Medical Record Data to Paper Records in Antiretroviral Therapy Clinic in Ethiopia: What is affecting the Quality of the Data? Online J. Public Health Inform. 2018, 10, e212. [Google Scholar] [CrossRef] [PubMed]
- Oluoch, T.; Katana, A.; Ssempijja, V.; Kwaro, D.; Langat, P.; Kimanga, D.; Okeyo, N.; Abu-Hanna, A.; de Keizer, N. Electronic medical record systems are associated with appropriate placement of HIV patients on antiretroviral therapy in rural health facilities in Kenya: A retrospective pre-post study. J. Am. Med. Inform. Assoc. 2014, 21, 1009–1014. [Google Scholar] [CrossRef] [PubMed]
- Gadabu, O.J.; Munthali, C.V.; Zachariah, R.; Gudmund-Hinderaker, S.; Jahn, A.; Twea, H.; Gondwe, A.; Mumba, S.; Pulmonaryu, M.; Malisita, K.; et al. Is transcription of data on antiretroviral treatment from electronic to paper-based registers reliable in Malawi? Public Health Action 2011, 1, 10–12. [Google Scholar] [CrossRef] [PubMed][Green Version]
- National Statistical Committee of the Kyrgyz Republic. Available online: http://www.stat.kg/en/ (accessed on 4 May 2023).
- The World Bank. Kyrgyz Republic Overview. 2022. Available online: https://www.worldbank.org/en/country/kyrgyzrepublic/overview (accessed on 13 August 2023).
- Manesen, R.; Mekler, K.A.; Molobi, T.R.; Tyiki, A.A.; Madlavu, M.J.; Velen, K.; Charalambous, S.; van der Heijden, Y.F. Data quality assessment of a South African electronic registry for drug-resistant TB, 2015–2016. Public Health Action 2021, 11, 33–39. [Google Scholar] [CrossRef] [PubMed]
- Thai, L.H.; Nhat, L.M.; Shah, N.; Lyss, S.; Ackers, M. Sensitivity, completeness and agreement of the tuberculosis electronic system in Ho Chi Minh City, Viet Nam. Public Health Action 2017, 7, 294–298. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Records Compared for Time from Diagnosis to Treatment Initiation and Outcomes | ||
| Paper records: January to December 2019 | ||
| Records compared for completeness and concordance | Electronic records: June 2021 to May 2022 | Paper records: June 2021 to May 2022 |
| Variable | Completeness + | Concordance * | |||||
|---|---|---|---|---|---|---|---|
| Electronic | Paper-Based | ||||||
| n | (%) | n | (%) | Total | n | (%) | |
| Total people with TB | 302 | 302 | |||||
| Auto-calculated fields | |||||||
| Sex | 302 | (100) | 257 | (85.1) | 257 | 254 | (98.8) |
| Age | 302 | (100) | 237 | (78.5) | 237 | 225 | (95.0) |
| Date of birth | 302 | (100) | 281 | (93.0) | 281 | 272 | (96.8) |
| Mandatory fields | |||||||
| Date of symptom onset | 302 | (100) | 257 | (85.1) | 257 | 234 | (91.1) |
| Date of diagnosis | 302 | (100) | 259 | (85.8) | 259 | 217 | (83.8) |
| Date of TB treatment initiation | 302 | (100) | 281 | (93.0) | 281 | 242 | (86.1) |
| Date of the first visit to a TB clinic | 302 | (100) | 270 | (89.4) | 270 | 239 | (88.5) |
| Case definition | 292 | (96.7) | 261 | (86.4) | 261 | 260 | (99.9) |
| Date of treatment outcome | 302 | (100) | 209 | (69.2) | 209 | 174 | (83.2) |
| Treatment outcome | 302 | (100) | 229 | (75.8) | 229 | 224 | (97.8) |
| Nonmandatory fields | |||||||
| Height | 284 | (94.0) | 263 | (87.0) | 259 | 253 | (97.6) |
| Weight | 289 | (95.7) | 261 | (86.4) | 259 | 255 | (98.4) |
| Location of the disease | 290 | (96.0) | 247 | (81.8) | 247 | 247 | (100) |
| Number of medication side effects reported | 81 | (26.8) | 41 | (13.6) | 41 | 35 | (85.4) |
| Characteristics | Paper-Based | Electronic | p Value $ | ||
|---|---|---|---|---|---|
| Median | (IQR) | Median | (IQR) | ||
| Total | 350 | 350 | |||
| Symptom onset to diagnosis in days | 25 | (5–49) | 27 | (13–45) | 0.210 |
| Diagnosis to treatment initiation in days | 0 | (0–1) | 0 | (0–0) | <0.001 |
| Symptom onset to treatment initiation in days | 29 | (13–48) | 30 | (16–32) | 0.056 |
| Number (percentage) initiated on treatment * | |||||
| On the day of diagnosis | 200 | (57.1) | 281 | (80.3) | <0.001 |
| Second day of diagnosis | 33 | (9.4) | 14 | (4.0) | 0.004 |
| Third day of diagnosis | 17 | (4.9) | 8 | (2.3) | 0.070 |
| Fourth day or later of diagnosis | 100 | (28.6) | 47 | (13.4) | <0.001 |
| Treatment Outcomes * | Paper-Based | Electronic | p Value $ | ||
|---|---|---|---|---|---|
| n | (%) * | n | (%) * | ||
| Total | 350 | 350 | |||
| Successful Outcomes | 285 | (81.4) | 279 | (79.7) | 0.284 |
| Cured | 105 | (30.0) | 88 | (25.1) | 0.076 |
| Treatment completed | 180 | (51.4) | 191 | (54.6) | 0.203 |
| Unsuccessful Outcomes | |||||
| Lost to follow-up | 7 | (2.0) | 20 | (5.7) | <0.001 |
| Death # | 6 | (1.7) | 18 | (5.1) | <0.001 |
| Failure | 2 | (0.6) | 16 | (4.6) | <0.001 |
| Not evaluated/recorded | 50 | (14.3) | 17 | (4.8) | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shauer, D.; Petrosyan, O.; Gemilyan, M.; Kamau, E.M.; Thekkur, P.; Goncharova, O.; Gulmira, K.; Kyrbashov, B.; Istamov, K.; Kadyrov, M.; et al. Quality of Electronic TB Register Data Compared with Paper-Based Records in the Kyrgyz Republic. Trop. Med. Infect. Dis. 2023, 8, 416. https://doi.org/10.3390/tropicalmed8080416
Shauer D, Petrosyan O, Gemilyan M, Kamau EM, Thekkur P, Goncharova O, Gulmira K, Kyrbashov B, Istamov K, Kadyrov M, et al. Quality of Electronic TB Register Data Compared with Paper-Based Records in the Kyrgyz Republic. Tropical Medicine and Infectious Disease. 2023; 8(8):416. https://doi.org/10.3390/tropicalmed8080416
Chicago/Turabian StyleShauer, Daniil, Ofelya Petrosyan, Manik Gemilyan, Edward M. Kamau, Pruthu Thekkur, Olga Goncharova, Kalmambetova Gulmira, Bolot Kyrbashov, Kylychbek Istamov, Meder Kadyrov, and et al. 2023. "Quality of Electronic TB Register Data Compared with Paper-Based Records in the Kyrgyz Republic" Tropical Medicine and Infectious Disease 8, no. 8: 416. https://doi.org/10.3390/tropicalmed8080416
APA StyleShauer, D., Petrosyan, O., Gemilyan, M., Kamau, E. M., Thekkur, P., Goncharova, O., Gulmira, K., Kyrbashov, B., Istamov, K., Kadyrov, M., & Wilkinson, E. (2023). Quality of Electronic TB Register Data Compared with Paper-Based Records in the Kyrgyz Republic. Tropical Medicine and Infectious Disease, 8(8), 416. https://doi.org/10.3390/tropicalmed8080416