
Increased Prevalence of Symptomatic Human Intestinal Spirochetosis in MSM with High-Risk Sexual Behavior in a Cohort of 165 Individuals

 , ,
, ,  ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population and Sample Collection
2.2. Scanning Electron Microscopy
2.3. Microbiological Studies
2.3.1. Sexually Transmitted Diseases
2.3.2. Gastrointestinal Infections
- Bacterial culture
- Direct microscopy
- Molecular detection
2.4. Statistical Analysis
3. Results
3.1. Age and Sex
3.2. Lifestyle and Risk Factors
3.3. Sexual Orientation, HIV Status, and Sexually Transmitted Diseases
3.4. Symptomatology
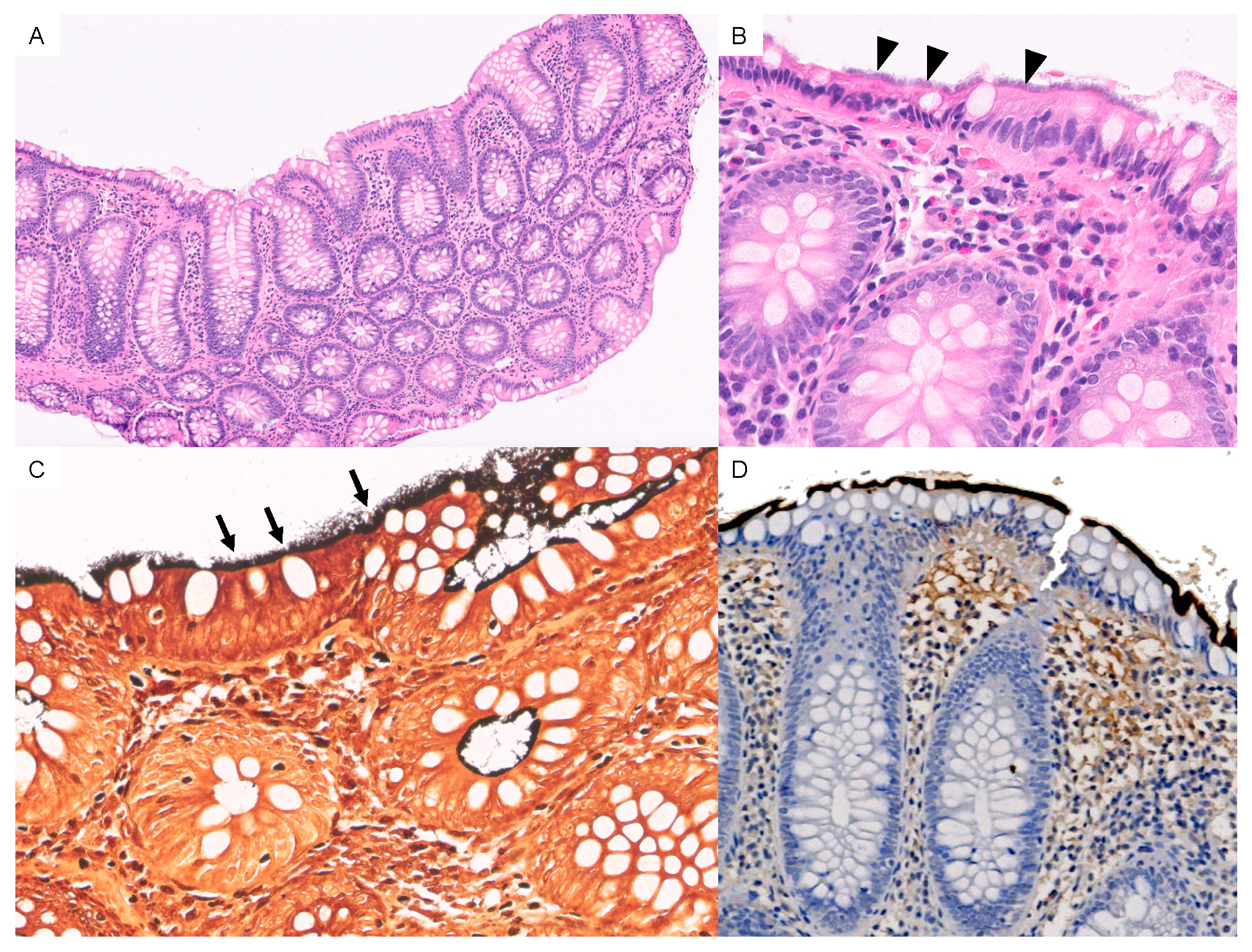
3.5. Localization and Histologic Findings
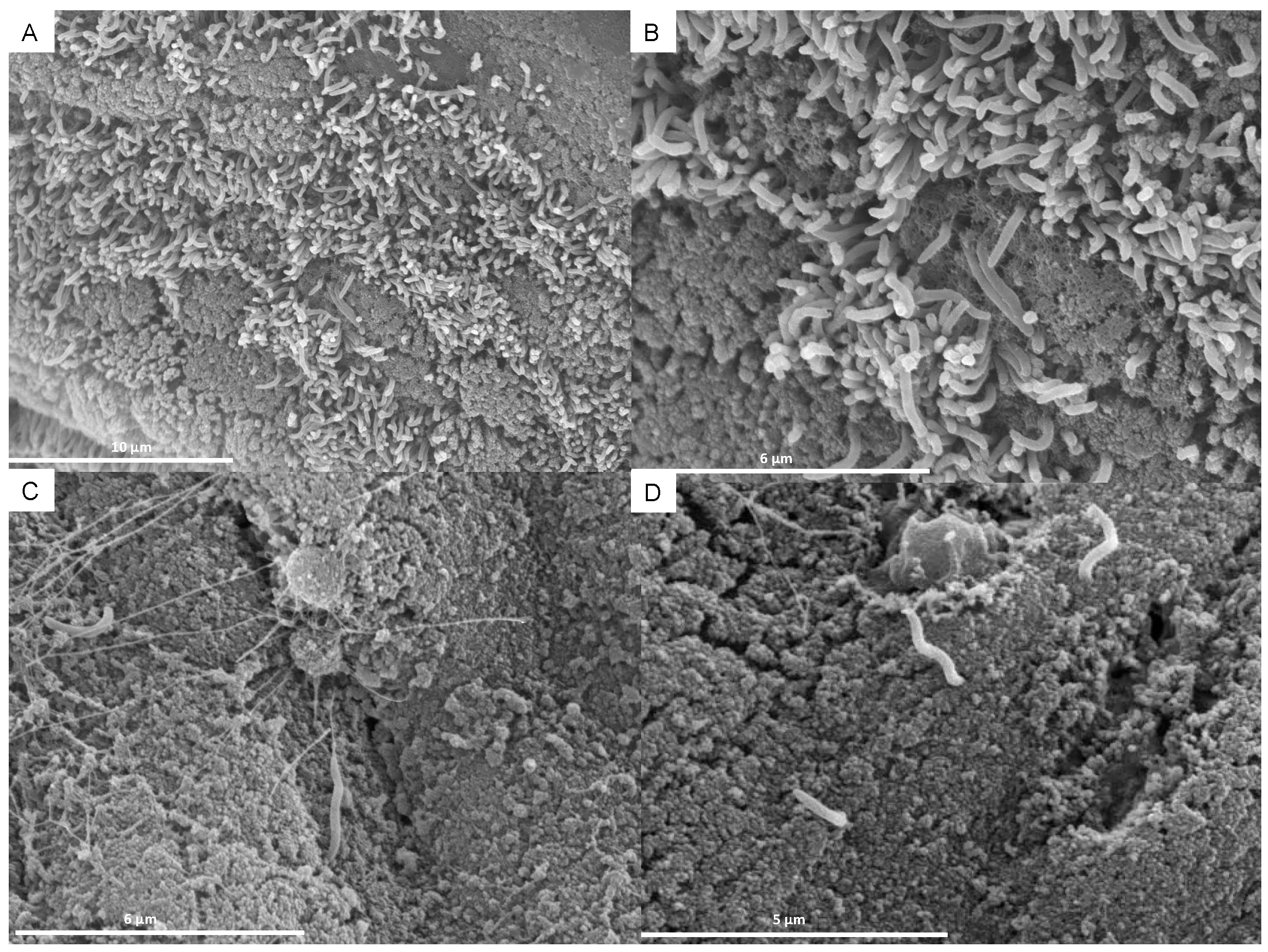
Scanning Electron Microscopy (SEM)
3.6. Additional Microbiological Studies
3.7. Blood Tests
3.8. Treatment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Harland, W.A.; Lee, F.D. Intestinal Spirochaetosis. Br. Med. J. 1967, 3, 718–719. [Google Scholar] [CrossRef] [PubMed]
- Lee, F.D.; Kraszewski, A.; Gordon, J.; Howie, J.G.R.; Mcseveney, D.; Harland, W.A. Intestinal Spirochaetosis. Gut 1971, 12, 126–133. [Google Scholar] [CrossRef] [PubMed]
- Erickson, L.A.; Torbenson, M.S. Intestinal Spirochetosis. Mayo Clin. Proc. 2020, 95, 427–428. [Google Scholar] [CrossRef]
- Weisheit, B.; Bethke, B.; Stolte, M. Human Intestinal Spirochetosis: Analysis of the Symptoms of 209 Patients. Scand. J. Gastroenterol. 2007, 42, 1422–1427. [Google Scholar] [CrossRef] [PubMed]
- Norris, S.J. Hiding in Plain Sight: Colonic Spirochetosis in Humans. J. Bacteriol. 2019, 201, e00465-19. [Google Scholar] [CrossRef]
- Anthony, N.E.; Blackwell, J.; Ahrens, W.; Lovell, R.; Scobey, M.W. Intestinal Spirochetosis: An Enigmatic Disease. Dig. Dis. Sci. 2013, 58, 202–208. [Google Scholar] [CrossRef]
- Fan, K.; Eslick, G.D.; Nair, P.M.; Burns, G.L.; Walker, M.M.; Hoedt, E.C.; Keely, S.; Talley, N.J. Human Intestinal Spirochetosis, Irritable Bowel Syndrome, and Colonic Polyps: A Systematic Review and Meta-Analysis. J. Gastroenterol. Hepatol. 2022, 37, 1222–1234. [Google Scholar] [CrossRef]
- Escherich, T. Beiträge Zur Kenntniss Der Darmbakterien. München Med. Wochenschr. 1886, 33, 815–817. [Google Scholar]
- Escherich, T. Klinisch-therapeutische Beobachtungen aus der Cholera-Epidemiein Neapel. Aerztliches Intell. 1984, 31, 561–564. [Google Scholar]
- Stephens, C.P.; Hampson, D.J. Intestinal Spirochete Infections of Chickens: A Review of Disease Associations, Epidemiology and Control. Anim. Health Res. Rev. 2001, 2, 83–91. [Google Scholar] [CrossRef]
- Mikosza, A.S.J.; Hampson, D.J. Human Intestinal Spirochetosis: Brachyspira Aalborgi and/or Brachyspira Pilosicoli? Anim. Health Res. Rev. 2001, 2, 101–110. [Google Scholar] [CrossRef] [PubMed]
- Trott, D.J.; Huxtable, C.R.; Hampson, D.J. Experimental Infection of Newly Weaned Pigs with Human and Porcine Strains of Serpulina Pilosicoli. Infect. Immun. 1996, 64, 4648–4654. [Google Scholar] [CrossRef] [PubMed]
- Trott, D.J.; Mclaren, A.J.; Hampson, D.J. Pathogenicity of Human and Porcine Intestinal Spirochetes in One-Day-Old Specific-Pathogen-Free Chicks: An animal model of intestinal spirochetosis. Infect. Immun. 1995, 63, 3705–3710. [Google Scholar] [CrossRef] [PubMed]
- Munshi, M.A.; Traub, R.J.; Robertson, I.D.; Mikosza, A.S.J.; Hampson, D.J. Colonization and Risk Factors for Brachyspiraa Alborgi and Brachyspira Pilosicoli in Humans and Dogs on Tea Estates in Assam, India. Epidemiol. Infect. 2004, 132, 137–144. [Google Scholar] [CrossRef] [PubMed]
- Jones, M.J.; Miller, J.N.; Lance Georgel’, A.W. Microbiological and Biochemical Characterization of Spirochetes Isolated from the Feces of Homosexual Males. J. Clin. Microbiol. 1986, 24, 1071–1074. [Google Scholar] [CrossRef] [PubMed]
- Tompkins, D.S.; Waugh, M.A.; Cooke, E.M. Isolation of Intestinal Spirochaetes from Homosexuals. J. Clin. Pathol. 1981, 34, 1385–1387. [Google Scholar] [CrossRef] [PubMed]
- Law, C.L.H.; Grierson, J.M.; Stevens, S.M.B.; Law, C. Rectal Spirochaetosis in Homosexual Men: The Association with Sexual Practices, HIV Infection and Enteric Flora. Genitourin. Med. 1994, 70, 26–29. [Google Scholar] [CrossRef]
- Cooper, C.; Cotton, D.W.K.; Hudson, M.J.; Kirkham, N.; Wilmott, F.E.W. Rectal Spirochaetosis in Homosexual Men: Characterisation of the Organism and Pathophysiology. Genitourin. Med. 1986, 62, 47–52. [Google Scholar] [CrossRef]
- Surawicz, C.M.; Roberts, P.L.; Ann Rompalo, M.; Quinn, T.C.; Holmes, K.K.; Stamm, W.E. Intestinal Spirochetosis in Homosexual Men. Am. J. Med. 1987, 82, 587–592. [Google Scholar] [CrossRef]
- Nielsen, R.H.; Orholm, M.; Pedersen, J.O.; Hovind-Hougen, K.; StubbeTeglbjærg, P.; Hess Thaysen, E. Colorectal Spirochetosis: Clinical Significance of the Infestation. Gastroenterology 1983, 85, 62–67. [Google Scholar] [CrossRef]
- van Mook, W.N.K.A.; Koek, G.H.; van der Ven, A.J.A.M.; Ceelen, T.L.; Bos, R.P. Human Intestinal Spirochaetosis: Any Clinical Significance? Eur. J. Gastroenterol. Hepatol. 2004, 16, 83–87. [Google Scholar] [CrossRef] [PubMed]
- Tsinganou, E.; Gebbers, J.-O. Human Intestinal Spirochetosis—A Review. GER Med. Sci. 2010, 8, Doc01. [Google Scholar]
- Kanavaki, S.; Mantadakis, E.; Thomakos, N.; Pefanis, A.; Matsiota-Bernard, P.; Karabela, S.; Samonis, G. Brachyspira (Serpulina) Pilosicoli Spirochetemia in an Immunocompromised Patient. Infection 2002, 30, 175–177. [Google Scholar] [CrossRef] [PubMed]
- Takezawa, T.; Hayashi, S.; Adachi, Y.; Sunada, K.; Hayashi, Y.; Nishimura, N.; Yano, T.; Miyata, T.; Yamamoto, H.; Hirai, Y.; et al. Human Intestinal Spirochetosis in an Immunocompromised Host: Evaluation of Eradication Therapy by Endoscopy, Histopathology and Bacteriology. Clin. J. Gastroenterol. 2012, 5, 69–73. [Google Scholar] [CrossRef] [PubMed]
- Tateishi, Y.; Takahashi, M.; Horiguchi, S.I.; Funata, N.; Koizumi, K.; Okudela, K.; Hishima, T.; Ohashi, K. Clinicopathologic Study of Intestinal Spirochetosis in Japan with Special Reference to Human Immunodeficiency Virus Infection Status and Species Types: Analysis of 5265 Consecutive Colorectal Biopsies. BMC Infect. Dis. 2015, 15, 13. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Hernandez, D.; Vall-Mayans, M.; Coll-Estrada, S.; Naranjo-Hans, L.; Armengol, P.; Iglesias, M.A.; Barberá, M.J.; Arando, M. Human Intestinal Spirochetosis, a Sexually Transmissible Infection? Review of Six Cases from Two Sexually Transmitted Infection Centres in Barcelona. Int. J. STD AIDS 2021, 32, 52–58. [Google Scholar] [CrossRef]
- Edmundson, C.; Heinsbroek, E.; Glass, R.; Hope, V.; Mohammed, H.; White, M.; Desai, M. Sexualised Drug Use in the United Kingdom (UK): A Review of the Literature. Int. J. Drug Policy 2018, 55, 131–148. [Google Scholar] [CrossRef]
- Peghini, P.L.; Guccion, J.G.; Sharma, A. Improvement of Chronic Diarrhea After Treatment for Intestinal Spirochetosis. Dig. Dis. Sci. 2000, 45, 1006–1010. [Google Scholar] [CrossRef]
- Esteve, M.; Salas, A.; Fernández-Bañares, F.; Lloreta, J.; Mariné, M.; Gonzalez, C.I.; Forné, M.; Casalots, J.; Santaolalla, R.; Espinós, J.C.; et al. Intestinal Spirochetosis and Chronic Watery Diarrhea: Clinical and Histological Response to Treatment and Long-Term Follow Up. J. Gastroenterol. Hepatol. 2006, 21, 1326–1333. [Google Scholar] [CrossRef]
- de Vries, H.J.C.; Nori, A.v.; Kiellberg Larsen, H.; Kreuter, A.; Padovese, V.; Pallawela, S.; Vall-Mayans, M.; Ross, J. 2021 European Guideline on the Management of Proctitis, Proctocolitis and Enteritis Caused by Sexually Transmissible Pathogens. J. Eur. Acad. Dermatol. Venereol. 2021, 35, 1434–1443. [Google Scholar] [CrossRef]
- de Vries, H.J.C.; de Barbeyrac, B.; de Vrieze, N.H.N.; Viset, J.D.; White, J.A.; Vall-Mayans, M.; Unemo, M. 2019 European Guideline on the Management of Lymphogranuloma Venereum. J. Eur. Acad. Dermatol. Venereol. 2019, 33, 1821–1828. [Google Scholar] [CrossRef] [PubMed]
- Zboromyrska, Y.; Hurtado, J.C.; Salvador, P.; Alvarez-Martínez, M.J.; Valls, M.E.; Mas, J.; Marcos, M.A.; Gascón, J.; Vila, J. Aetiology of traveller’s diarrhoea: Evaluation of a multiplex PCR tool to detect different enteropathogens. Clin. Microbiol. Infect. 2014, 20, O753–O759. [Google Scholar] [CrossRef][Green Version]
- Stanley, S.L., Jr. Amoebiasis. Lancet 2003, 361, 1025–1034. [Google Scholar] [CrossRef] [PubMed]
- Gutiérrez-Cisneros, M.J.; Cogollos, R.; López-Vélez, R.; Martín-Rabadá, P.; Martínez-Ruiz, R.; Subirats, M.; Merino, F.J.; Fuentes, I. Application of Real-Time PCR for the Differentiation of Entamoeba Histolytica and E. Dispar in Cyst-Positive Faecal Samples from 130 Immigrants Living in Spain. Ann. Trop. Med. Parasitol. 2010, 104, 145–149. [Google Scholar] [CrossRef] [PubMed]
- Carr, N.J.; Mahajan, H.; Tan, K.L.; Sharma, R. The Histological Features of Intestinal Spirochetosis in a Series of 113 Patients. Int. J. Surg. Pathol. 2010, 18, 144–148. [Google Scholar] [CrossRef]
- Mcmillan, A.; Lee, F.D. Sigmoidoscopic and Microscopic Appearance of the Rectal Mucosa in Homosexual Men. Gut 1981, 22, 1035–1041. [Google Scholar] [CrossRef]
- Calderaro, A.; Bommezzadri, S.; Gorrini, C.; Piccolo, G.; Peruzzi, S.; Villanacci, V.; Zambelli, C.; Dettori, G.; Chezzi, C. Infective Colitis Associated with Human Intestinal Spirochetosis. J. Gastroenterol. Hepatol. 2007, 22, 1772–1779. [Google Scholar] [CrossRef] [PubMed]
- Heiligenberg, M.; Wermeling, P.R.; van Rooijen, M.S.; Urbanus, A.T.; Speksnijder, A.G.C.L.; Heijman, T.; Prins, M.; Coutinho, R.A.; van der Loeff, M.F.S. Recreational Drug Use during Sex and Sexually Transmitted Infections among Clients of a City Sexually Transmitted Infections Clinic in Amsterdam, the Netherlands. Sex. Transm. Dis. 2012, 39, 518–527. [Google Scholar] [CrossRef] [PubMed]
- Weatherburn, P.; Hickson, F.; Reid, D.; Torres-Rueda, S.; Bourne, A. Motivations and Values Associated with Combining Sex and Illicit Drugs (Chemsex) among Gay Men in South London: Findings from a Qualitative Study. Sex. Transm. Infect. 2017, 93, 203–206. [Google Scholar] [CrossRef] [PubMed]
- Körner, M.; Gebbers, J.O. Clinical Significance of Human Intestinal Spirochetosis—A Morphologic Approach. Infection 2003, 31, 341–349. [Google Scholar] [CrossRef]
- Tong, Y.T.; Younes, M. Intestinal Spirochetosis: Case Series and Review of Literature. Ann. Clin. Lab. Sci. 2020, 50, 386–390. [Google Scholar] [PubMed]
- Edwards, D.L.; Fink, P.C.; Van-Dyke, P.O. Disulfiram-like reaction associated with intravenous trimethoprim-sulfamethoxazole and metronidazole. Clin. Pharm. 1986, 5, 999–1000. [Google Scholar] [PubMed]
- Ristow, P.; Bourhy, P.; Kerneis, S.; Schmitt, C.; Prevost, M.C.; Lilenbaum, W.; Picardeau, M. Biofilm Formation by Saprophytic and Pathogenic Leptospires. Microbiology 2008, 154, 1309–1317. [Google Scholar] [CrossRef] [PubMed]
- Santos, A.A.N.; dos Santos Ribeiro, P.; da França, G.V.; Souza, F.N.; Ramos, E.A.G.; Figueira, C.P.; Reis, M.G.; Costa, F.; Ristow, P. Leptospira Interrogans Biofilm Formation in Rattus Norvegicus (Norway Rats) Natural Reservoirs. PLoS Negl. Trop. Dis. 2021, 15, e0009736. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Total | Symptomatic n = 133 | Asymptomatic n = 31 | p-Value | |
|---|---|---|---|---|
| Age (median) | 41.0 (IQR:34.0–50.0) | 39 (IQR:33.0–48.0) | 50 (IQR:43.0–57.0) | <0.001 |
| Male (n = 165) | 156 (94.5%) | 127 (95.5%) | 28 (90.3%) | 0.255 |
| Spanish nationality * (n = 164) | 135 (82.3%) | 109 (82.6%) | 25 (80.6%) | 0.800 |
| MSM (n = 143) | 124 (86.7%) | 102 (87.9%) | 21 (80.8%) | 0.332 |
| No steady partner (n = 125) | 85 (68.0%) | 70 (69.3%) | 15 (62.5%) | 0.627 |
| HIV+ (n = 153) | 65 (42.5%) | 55 (44.4%) | 10 (34.5%) | 0.333 |
| Alcohol (n = 142) | 83 (58.5%) | 70 (60.3%) | 13(50.0%) | 0.333 |
| Drug use (n = 119) | 36 (30.2%) | 33 (34.7%) | 3 (12.5%) | 0.034 |
| Sexualized drug use (chemsex) (n = 115) | 27 (23.5%) | 25 (27.8%) | 2 (8.0%) | 0.039 |
| Prior travel to developing countries (n = 106) | 67 (63.2%) | 52 (61.9%) | 15 (68.2%) | 0.587 |
| Animal ownership (n = 101) | 61 (60.4%) | 44 (56.4%) | 17 (73.9%) | 0.131 |
| n (%) | |
|---|---|
| Urethritis n = 103 | 43 (41.7%) |
| Neisseria gonorrhoeae | 36 (35.0%) |
| Chlamydia trachomatis | 11 (10.7%) |
| Treponema pallidum | 3 (2.9%) |
| Herpes simplex 1–2 | 1 (1.0%) |
| Ureaplasma urealyticum/ Mycoplasma genitalum | 5 (4.9%) |
| Proctitis n = 99 | 33(33.3%) |
| Neisseria gonorrhoeae | 9 (9.1%) |
| Chlamydia trachomatis | 24 (24.2%) |
| Treponema pallidum | 2 (2.0%) |
| Herpes simplex 1–2 | 5 (5.1%) |
| Ureaplasma urealyticum/ Mycoplasma genitalum | 8 (8.1%) |
| Univariate OR (95% CI) | p-Value | Multivariate OR (95% CI) | p-Value | |
|---|---|---|---|---|
| Age < 41 years | 5.39 (2.07–14.00) | ≤0.001 | 5.44 (1.87–15.88) | 0.002 |
| Male (n = 165) | 2.27 (0.54–9.62) | 0.267 | ||
| Spanish nationality * (n = 164) | 1.14 (0.42–3.09) | 0.800 | ||
| MSM (n = 143) | 1.74 (0.56–5.34) | 0.337 | ||
|
No steady partner (n = 125) | 1.36 (0.535–3.43) | 0.521 | ||
| HIV+ (n = 153) | 1.51 (0.65–3.52) | 0.335 | ||
| Alcohol (n = 142) | 1.52 (0.65–3.58) | 0.335 | ||
| Drug use (n = 119) | 3.73 (1.04–13.42) | 0.044 | Not included p > 0.05 | n.s. |
| Sexualized drug use (chemsex) (n = 115) | 4.42 (0.97–20.16) | 0.055 | Not included p > 0.05 | n.s. |
| Prior travel to developing countries (n = 106) | 0.76 (0.28–2.06) | 0.587 | ||
| Animal ownership (n = 101) | 0.46 (0.16–1.28) | 0.137 | ||
| STD (n = 147) | 0.87 (0.35–2.16) | 0.760 | ||
| DPS (n = 102) | 0.79 (0.20–3.11) | 0.731 |
| Microorganism | n |
|---|---|
| Giardia duodenalis | 5 |
| EAEC | 2 |
| Campylobacter sp. | 2 |
| Blastocystis hominis | 2 |
| EPEC | 1 |
| STEC | 1 |
| Campylobacter sp. and Shigella/EIEC | 1 |
| Campylobacter sp., EAEC, EPEC and Shigella/EIEC | 1 |
| Giardia duodenalis, Campylobacter sp. and EPEC | 1 |
| Giardia duodenalis, Cryptosporidium spp., Entamoeba hystolica and EAEC | 1 |
| Shigella/EIECand Norovirus | 1 |
| Sapovirus and EAEC | 1 |
| STEC, Yersinia enterocolitica and Giardia duodenalis | 1 |
| Negative | 82 |
| Leucocyte (cel/mm3) | Hb (g/dL) | Platelets (cel/mm3) | Creatinine (mg/dL) | C-Reactive Protein (mg/dL) | |
|---|---|---|---|---|---|
| Median | 7050.00 | 15.1 | 232,000 | 0.90 | 0.36 |
| IQR | 6040.00–8510.0 | 14.5–15.8 | 203,000–283,000 | 0.80–1 | 0.11–1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pérez-Tanoira, R.; Tamarit, M.d.P.; Montaña, A.M.V.; Carmena, D.; Köster, P.; Górgolas, M.; Fortes Alen, J.R.; Cabello-Úbeda, A.; Prieto-Pérez, L. Increased Prevalence of Symptomatic Human Intestinal Spirochetosis in MSM with High-Risk Sexual Behavior in a Cohort of 165 Individuals. Trop. Med. Infect. Dis. 2023, 8, 250. https://doi.org/10.3390/tropicalmed8050250
Pérez-Tanoira R, Tamarit MdP, Montaña AMV, Carmena D, Köster P, Górgolas M, Fortes Alen JR, Cabello-Úbeda A, Prieto-Pérez L. Increased Prevalence of Symptomatic Human Intestinal Spirochetosis in MSM with High-Risk Sexual Behavior in a Cohort of 165 Individuals. Tropical Medicine and Infectious Disease. 2023; 8(5):250. https://doi.org/10.3390/tropicalmed8050250
Chicago/Turabian StylePérez-Tanoira, Ramón, Marta del Palacio Tamarit, Ana María Vicente Montaña, David Carmena, Pamela Köster, Miguel Górgolas, José R. Fortes Alen, Alfonso Cabello-Úbeda, and Laura Prieto-Pérez. 2023. "Increased Prevalence of Symptomatic Human Intestinal Spirochetosis in MSM with High-Risk Sexual Behavior in a Cohort of 165 Individuals" Tropical Medicine and Infectious Disease 8, no. 5: 250. https://doi.org/10.3390/tropicalmed8050250
APA StylePérez-Tanoira, R., Tamarit, M. d. P., Montaña, A. M. V., Carmena, D., Köster, P., Górgolas, M., Fortes Alen, J. R., Cabello-Úbeda, A., & Prieto-Pérez, L. (2023). Increased Prevalence of Symptomatic Human Intestinal Spirochetosis in MSM with High-Risk Sexual Behavior in a Cohort of 165 Individuals. Tropical Medicine and Infectious Disease, 8(5), 250. https://doi.org/10.3390/tropicalmed8050250