
Epidemiological Survey of Human Alphaherpesvirus 2 (HSV-2) Infection in Indigenous People of Dourados Municipality, Central Brazil

 , , , , , and
, , , , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Ethical Statement
2.2. Serological Analysis
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Brazilian Geographic and Statistics Institute. IBGE. Indigenous in the 2010 Population Census. Available online: https://indigenas.ibge.gov.br/images/indigenas/estudos/indigena_censo2010.pdf (accessed on 26 October 2022).
- Coelho, R. A Composição da População Segundo a Cor no Brasil e Nas Diversas Regiões Fisiográficas e Unidades da Federação, em 1950. In ONTRIBUIÇÕES Para o Estudo da Demografia do Brasil. (Estudos de Estatística Teórica e Aplicada), 2nd ed.; IBGE: Rio de Janeiro, Brazil, 1970; pp. 68–197. [Google Scholar]
- SECID/MS. Subsecretaria Especial de Cidadania. Governo do Estado de Mato Grosso do Sul. Available online: http://www.ms.gov.br/em-quatro-ano-governo-promove-acoes-e-executa-programas-que-garantem-cidadania-aos-indios-de-ms/ (accessed on 26 October 2022).
- de Alcantara, M.L.B.; Moure, W.; Trajber, Z.; Machado, I.R. Equipe de Jovens da Ação dos Jovens Indígenas de Dourados-MS. A percepção do suicídio como inseparável das outras formas de violência segundo os/as jovens indígenas: Um estudo de caso da Reserva Indígena de Dourados. Rev. Med. 2020, 99, 305–318. [Google Scholar]
- Mota, J.G.B.; Cavalcante, T.L.V. Reserva Indígena de Dourados: Histórias e Desafios Contemporâneos, 285. Ebook; Karywa: São Leopoldo, Brazil, 2019; 285p, ISBN 978-85-68730-38-6. [Google Scholar]
- Kotronias, D.; Kapranos, N. Detection of herpes simplex virus DNA in maternal breast milk by in situ hybridization with tyramide signal amplification. Vivo 1999, 13, 463–466. [Google Scholar]
- Braço, I.L.J.; De Sá, K.S.G.; Waqasi, M.; Queiroz, M.A.F.; Da Silva, A.N.R.; Cayres-Vallinoto, I.M.V.; Lima, S.S.; Ishak, M.D.O.G.; Ishak, R.; Guerreiro, J.F.; et al. High prevalence of human T-lymphotropic virus 2 (HTLV-2) infection in villages of the Xikrin tribe (Kayapo), Brazilian Amazon region. BMC Infect Dis. 2019, 19, 459. [Google Scholar] [CrossRef] [PubMed]
- Graeff, S.V.; Pícolli, R.P.; Arantes, R.; Castro, V.O.L.; Cunha, R.V.D. Epidemiological aspects of HIV infection and AIDS among indigenous populations. Rev. Saude Publica 2019, 53, 71. [Google Scholar] [CrossRef] [PubMed]
- Vallinoto, A.C.R.; Ishak, M.O.G.; Azevedo, V.N.; Vicente, A.C.P.; Otsuki, K.; Hall, W.W.; Ishak, R. Molecular epidemiology of human T-lymphotropic virus type II infection in Amerindian and urban populations of the Amazon region of Brazil. Hum. Biol. 2002, 74, 633–644. [Google Scholar] [CrossRef]
- Santos, V.L. Analyzing STD and Aids control policies among Brazilian indigenous population. Tempus Actas De Saúde Coletiva 2010, 4, 89–100. [Google Scholar] [CrossRef][Green Version]
- Romero-Sandoval, N.; Cifuentes, L.; León, G.; Lecaro, P.; Ortiz-Rico, C.; Cooper, P.; Martín, M. High Rates of Exposures to Waterborne Pathogens in Indigenous Communities in the Amazon Region of Ecuador. Am. J. Trop. Med. Hyg. 2019, 101, 45–50. [Google Scholar] [CrossRef]
- Gabster, A.; Pascale, J.M.; Cislaghi, B.; Francis, S.C.; Weiss, H.A.; Martinez, A.; Ortiz, A.; Herrera, M.; Herrera, G.; Gantes, C.; et al. High Prevalence of Sexually Transmitted Infections, and High-Risk Sexual Behaviors Among Indigenous Adolescents of the Comarca Ngäbe-Buglé, Panama. Sex Transm. Dis. 2019, 46, 780–787. [Google Scholar] [CrossRef]
- Sauerbrei, Herpes Genitalis: Diagnosis, Treatment and Prevention. Geburtshilfe Frauenheilkd 2016, 76, 1310–1317. [CrossRef]
- Roizman, B.; Knipe, D.M.; Whitley, R.J. Herpes Simplex Viruses. Fields Virology, 5th ed.; Lippincott William & Wilkins: Philadelphia, PA, USA, 2007; pp. 2502–2600. [Google Scholar]
- Davison, A.J.; Eberle, R.; Ehlers, B.; Hayward, G.S.; McGeoch, D.J.; Minson, A.C.; Pellett, P.E.; Roizman, B.; Studdert, M.J.; Thiry, E. The order Herpesvirales. Arch. Virol. 2009, 154, 171–177. [Google Scholar] [CrossRef]
- Smith, J.S.; Robinson, N.J. Age-specific prevalence of infection with herpes simplex virus types 2 and 1: A global review. J. Infect Dis. 2002, 186 (Suppl. S1), S3–S28. [Google Scholar] [CrossRef] [PubMed]
- Livorsi, D.; Anderson, E.; Qureshi, S.; Howard, M.; Wang, Y.F.; Franco-Paredes, C. Brainstem encephalitis: An unusual presentation of herpes simplex virus infection. J. Neurol. 2010, 257, 1432–1437. [Google Scholar] [CrossRef] [PubMed]
- Zajkowska, J.M.; Ustymowicz, A.; Hermanowska-Szpakowicz, T. Difficulties in early diagnosis of Herpes simplex encephalitis. Pol Merkur Lekarski 2005, 19, 719–722. [Google Scholar] [PubMed]
- MRL, P. Nosso compromisso e sua participação, 2 editorial. J. Bras Doencas Sex Transm. 2002, 14, 3. [Google Scholar]
- Clemens, S.A.; Farhat, C.K. Seroprevalence of herpes simplex 1–2 antibodies in Brazil. Rev Saude Publica 2010, 44, 726–734. [Google Scholar] [CrossRef]
- Pieknik, J.R.; Bertke, A.S.; Krause, P.R. Herpes Simplex Virus 2 in Autonomic Ganglia: Evidence for Spontaneous Reactivation. J. Virol. 2019, 93, e00227-19. [Google Scholar] [CrossRef]
- Davenport, D.S.; Johnson, D.R.; Holmes, G.P.; Jewett, D.A.; Ross, S.C.; Hilliard, J.K. Diagnosis and management of human B virus (Herpesvirus simiae) infections in Michigan. Clin. Infect Dis. 1994, 19, 33–41. [Google Scholar] [CrossRef]
- Fierer, J.; Bazely, P.; Braude, A.I. Herpes B virus encephalomyelitis presenting as ophthalmic zoster. A possible latent infection reactivated. Ann. Intern. Med. 1973, 79, 225–228. [Google Scholar] [CrossRef]
- Holmes, A.W.; Caldwell, R.G.; Dedmon, R.E.; Deinhardt, F. Isolation and Characterization of A New Herpes Virus. J. Immunol. 1964, 92, 602–610. [Google Scholar] [CrossRef]
- Whitley, R. Herpes simplex virus. In Infections of the Central Nervous System, 4th ed.; Scheld, W.M., Whitley, R.J., Marra, C.M., Eds.; Lippincott William & Wilkins: Philadelphia, PA, USA, 2014; pp. 137–156. [Google Scholar]
- Freeman, E.E.; Weiss, H.A.; Glynn, J.R.; Cross, P.L.; Whitworth, J.A.; Hayes, R.J. Herpes simplex virus 2 infection increases HIV acquisition in men and women: Systematic review and meta-analysis of longitudinal studies. AIDS 2006, 20, 73–83. [Google Scholar] [CrossRef]
- Corey, L.; Wald, A.; Celum, C.L.; Quinn, T.C. The effects of herpes simplex virus-2 on HIV-1 acquisition and transmission: A review of two overlapping epidemics. J. Acquir. Immune. Defic. Syndr. 2004, 35, 435–445. [Google Scholar] [CrossRef]
- Anzivino, E.; Fioriti, D.; Mischitelli, M.; Bellizzi, A.; Barucca, V.; Chiarini, F.; Pietropaolo, V. Herpes simplex virus infection in pregnancy and in neonate: Status of art of epidemiology, diagnosis, therapy and prevention. Virol. J. 2009, 6, 40. [Google Scholar] [CrossRef] [PubMed]
- Brown, Z.A.; Selke, S.; Zeh, J.; Kopelman, J.; Maslow, A.; Ashley, R.L.; Watts, D.H.; Berry, S.; Herd, M.; Corey, L. The acquisition of herpes simplex virus during pregnancy. N. Engl. J. Med. 1997, 337, 509–515. [Google Scholar] [CrossRef]
- Fleming, D.T.; Leone, P.; Esposito, D.; Heitman, C.K.; Justus, S.; Chin, S.; Fife, K.H. Herpes virus type 2 infection and genital symptoms in primary care patients. Sex Transm. Dis. 2006, 33, 416–421. [Google Scholar] [CrossRef] [PubMed]
- Arama, V.; Cercel, A.S.; Vladareanu, R.; Mihai, C.; Mihailescu, R.; Rankin, J.; Goschin, S.; Filipescu, A.; Rafila, A.; Arama, S.; et al. Type-specific herpes simplex virus-1 and herpes simplex virus-2 seroprevalence in Romania: Comparison of prevalence and risk factors in women and men. Int. J. Infect Dis. 2010, 14 (Suppl. S3), e25–e31. [Google Scholar] [CrossRef] [PubMed]
- Langan, S.M.; Clair, J.; Lyons, J.F. Renal failure with herpes simplex. J. Eur. Acad. Dermatol. Venereol. 2006, 20, 347–349. [Google Scholar] [CrossRef] [PubMed]
- Sizemore, J.M.; Lakeman, F.; Whitley, R.; Hughes, A.; Hook, E.W. The spectrum of genital herpes simplex virus infection in men attending a sexually transmitted disease clinic. J. Infect Dis. 2006, 193, 905–911. [Google Scholar] [CrossRef]
- Mahalakshmi, B.; Therese, K.L.; Devipriya, U.; Pushpalatha, V.; Margarita, S.; Madhavan, H.N. Infectious aetiology of congenital cataract based on TORCHES screening in a tertiary eye hospital in Chennai, Tamil Nadu, India. Indian J. Med. Res. 2010, 131, 559–564. [Google Scholar]
- MINISTÉRIO DE SAÚDE. Povos Indígenas e A Prevenção as DST, HIV e Aids: Manual de Diretrizes Técnicas; Ministério da Saúde: Brasília, Brasil, 2000; 24p, ISBN 85-334-0232-5. Available online: https://bvsms.saude.gov.br/bvs/publicacoes/indigena_hiv.pdf (accessed on 23 October 2022).
- Carvalho, M.; de Carvalho, S.; Pannuti, C.S.; Sumita, L.M.; de Souza, V.A. Prevalence of herpes simplex type 2 antibodies and a clinical history of herpes in three different populations in Campinas City, Brazil. Int. J. Infect Dis. 1998, 3, 94–98. [Google Scholar] [CrossRef]
- Amudha, V.P.; Rashetha; Sucilathangam, G.; Cinthujah, B.; Revathy, C. Serological Profile of HSV-2 in STD Patients: Evaluation of Diagnostic Utility of HSV-2 IgM and IgG Detection. J. Clin. Diagn. Res. 2014, 8, DC16-9. [Google Scholar]
- Naveca, F.G.; Sabidó, M.; de Almeida, T.A.P.; Veras, E.A.; Mejía, M.D.C.C.; Galban, E.; Benzaken, A.S. Etiology of genital ulcer disease in a sexually transmitted infection reference center in Manaus, Brazilian Amazon. PLoS ONE 2013, 8, e63953. [Google Scholar]
- Looker, K.J.; Magaret, A.S.; Turner, K.M.; Vickerman, P.; Gottlieb, S.L.; Newman, L.M. Correction: Global estimates of prevalent and incident herpes simplex virus type 2 infections in 2012. PLoS ONE 2015, 10, e0128615. [Google Scholar] [CrossRef] [PubMed]
- Agabi, Y.A.; Banwat, E.B.; Mawak, J.D.; Lar, P.M.; Dashe, N.; Dashen, M.M.; Adoga, M.P.; Agabi, F.Y.; Zakari, H. Seroprevalence of herpes simplex virus type-2 among patients attending the Sexually Transmitted Infections Clinic in Jos, Nigeria. J. Infect. Dev. Ctries. 2010, 4, 572–575. [Google Scholar] [CrossRef]
- Xu, F.; Sternberg, M.R.; Kottiri, B.J.; McQuillan, G.M.; Lee, F.K.; Nahmias, A.J.; Berman, S.M.; Markowitz, L.E. Trends in herpes simplex virus type 1 and type 2 seroprevalence in the United States. JAMA 2006, 296, 964–973. [Google Scholar] [CrossRef] [PubMed]
- Langenberg, A.G.; Corey, L.; Ashley, R.L.; Leong, W.P.; Straus, S.E. A prospective study of new infections with herpes simplex virus type 1 and type 2. Chiron HSV Vaccine Study Group. N. Engl. J. Med. 1999, 341, 1432–1438. [Google Scholar] [CrossRef] [PubMed]
- Clemens, S.A.C.; Farhat, C.K. Soroprevalência de anticorpos contra vírus herpes simples 1–2 no Brasil. Rev. Saúde Pública 2010, 44, 726–734. [Google Scholar] [CrossRef]
- Suligoi, B.; Calistri, A.; Cusini, M.; Palù, G.; Forum, I.H.M. Seroprevalence and determinants of herpes simplex type 2 infection in an STD clinic in Milan, Italy. J. Med. Virol. 2002, 67, 345–348. [Google Scholar] [CrossRef]
- Ministério da Cidadania/Conselho Nacional de Assistência Social. RESOLUÇÃO Nº 20, DE 20 DE NOVEMBRO DE 2020. Available online: https://www.suas.sedhast.ms.gov.br/resolucao-no-20-de-20-de-novembro-de-2020/ (accessed on 26 December 2022).
- Zhu, J.; Hladik, F.; Woodward, A.L.; Klock, A.; Peng, T.; Johnston, C.; Remington, M.; Magaret, A.; Koelle, D.; Wald, A.; et al. Persistence of HIV-1 receptor-positive cells after HSV-2 reactivation is a potential mechanism for increased HIV-1 acquisition. Nat. Med. 2009, 15, 886–892. [Google Scholar] [CrossRef]
- Gutierrez, J.P.; Bertozzi, S.M.; Conde-Glez, C.J.; Sanchez-Aleman, M.A. Risk behaviors of 15–21 year olds in Mexico lead to a high prevalence of sexually transmitted infections: Results of a survey in disadvantaged urban areas. BMC Public Health 2006, 6, 49. [Google Scholar] [CrossRef]
- Cowan, F.F.; Pascoe, S.J.; Barlow, K.L.; Langhaug, L.F.; Jaffar, S.; Hargrove, J.W.; Robinson, N.J.; Latif, A.S.; Bassett, M.T.; Wilson, D.; et al. Association of genital shedding of herpes simplex virus type 2 and HIV-1 among sex workers in rural Zimbabwe. AIDS 2006, 20, 261–267. [Google Scholar] [CrossRef]
- James, C.; Harfouche, M.; Welton, N.J.; Turner, K.M.E.; Abu-Raddad, L.J.; Gottlieb, S.L.; Looker, K.J. Herpes simplex virus: Global infection prevalence and incidence estimates, 2016. Bull. World Health Organ. 2020, 98, 315–329. [Google Scholar] [CrossRef] [PubMed]
- ACunningham, L.; Taylor, R.; Taylor, J.; Marks, C.; Shaw, J.; Mindel, A. Prevalence of infection with herpes simplex virus types 1 and 2 in Australia: A nationwide population based survey. Sex Transm. Infect. 2006, 82, 164–168. [Google Scholar] [CrossRef] [PubMed]
- Brazzale, A.G.; Russell, D.B.; Cunningham, A.L.; Taylor, J.; McBride, W.J. Seroprevalence of herpes simplex virus type 1 and type 2 among the Indigenous population of Cape York, Far North Queensland, Australia. Sex Health 2010, 7, 453–459. [Google Scholar] [CrossRef] [PubMed]
- BRASIL. Instituto Brasileiro de Geografia e Estatística (Cidades e Estados Dourados, 2022). Available online: https://www.ibge.gov.br/cidades-e-estados/ms/dourados.html (accessed on 26 October 2022).
- Obasi, A.; Mosha, F.; Quigley, M.; Sekirassa, Z.; Gibbs, T.; Munguti, K.; Todd, J.; Grosskurth, H.; Mayaud, P.; Changalucha, J.; et al. Antibody to herpes simplex virus type 2 as a marker of sexual risk behavior in rural Tanzania. J. Infect. Dis. 1999, 179, 16–24. [Google Scholar] [CrossRef] [PubMed]
- Miskulin, M.; Miskulin, I.; Milas, J.; Antolović-Pozgain, A.; Rudan, S.; Vuksić, M. Prevalence and risk factors for herpes simplex virus type 2 infections in East Croatia. Coll. Antropol. 2011, 35, 9–14. [Google Scholar] [PubMed]
- Stanberry, L.R.; Rosenthal, S.L.; Mills, L.; Succop, P.A.; Biro, F.M.; Morrow, R.A.; Bernstein, D.I. Longitudinal risk of herpes simplex virus (HSV) type 1, HSV type 2, and cytomegalovirus infections among young adolescent girls. Clin. Infect. Dis. 2004, 39, 1433–1438. [Google Scholar] [CrossRef][Green Version]
- Engels, D.; Zhou, X.N. Neglected tropical diseases: An effective global response to local poverty-related disease priorities. Infect. Dis. Poverty 2020, 9, 10. [Google Scholar] [CrossRef]
- Van Zyl Smit, R.N.; Pai, M.; Yew, W.W.; Leung, C.C.; Zumla, A.; Bateman, E.D.; Dheda, K. Global lung health: The colliding epidemics of tuberculosis, tobacco smoking, HIV and COPD. Eur. Respir. J. 2010, 35, 27–33. [Google Scholar] [CrossRef]
- Halsey, N.A.; Coberly, J.S.; Holt, E.; Coreil, J.; Kissinger, P.; Moulton, L.H. Sexual behavior, smoking, and HIV-1 infection in Haitian Women. JAMA 1992, 267, 2062–2066. [Google Scholar] [CrossRef]
- Penkower, L.; A Dew, M.; Kingsley, L.; Becker, J.T.; Satz, P.; Schaerf, F.W.; Sheridan, K. Behavioral, health and psychosocial factors and risk for HIV infection among sexually active homosexual men: The Multicenter AIDS Cohort Study. Am. J. Public Health 1991, 81, 194–196. [Google Scholar] [CrossRef][Green Version]
- Gupta, R.; Warren, T.; Wald, A. Genital herpes. Lancet 2007, 370, 2127–2137. [Google Scholar] [CrossRef] [PubMed]
- Garland, S.M.; Steben, M. Genital herpes. Best Pract. Res. Clin. Obstet. Gynaecol. 2014, 28, 1098–1110. [Google Scholar] [CrossRef] [PubMed]
- Hollier, L.M.S.H. Genital herpes. BMJ Clin. Evid. 2011, 15, 1603. [Google Scholar]
- Shangase, N.; Kharsany, A.B.M.; Ntombela, N.P.; Pettifor, A.; McKinnon, L.R. A Systematic Review of Randomized Controlled Trials of School Based Interventions on Sexual Risk Behaviors and Sexually Transmitted Infections among Young Adolescents in Sub-Saharan Africa. AIDS Behav. 2021, 25, 3669–3686. [Google Scholar] [CrossRef]
- Magaret, A.S.; Mujugira, A.; Hughes, J.P.; Lingappa, J.; Bukusi, E.A.; DeBruyn, G.; Delany-Moretlwe, S.; Fife, K.H.; Gray, G.E.; Kapiga, S.; et al. Effect of Condom Use on Per-act HSV-2 Transmission Risk in HIV-1, HSV-2-discordant Couples. Clin. Infect. Dis. 2016, 62, 456–461. [Google Scholar] [CrossRef]
- Sarmati, L.; Babudieri, S.; Longo, B.; Starnini, G.; Carbonara, S.; Monarca, R.; Buonomini, A.; Dori, L.; Rezza, G.; Andreoni, M.; et al. Human herpesvirus 8 and human herpesvirus 2 infections in prison population. J. Med. Virol. 2007, 79, 167–173. [Google Scholar] [CrossRef]
- Caballero-Hoyos, J.R.; Monárrez-Espino, J. Concurrence and selection of sexual partners as predictors of condom use among Mexican indigenous migrant workers. Rev. Salud Publica 2018, 20, 293–300. [Google Scholar] [CrossRef]
- Monsell, E.; McLuskey, J. Factors influencing STI transmission in middle-aged heterosexual individuals. Br. J. Nurs. 2016, 25, 676–680. [Google Scholar] [CrossRef]
- Carey, C.; O’Donnell, K.; Davoren, M.; Quinlan, M.; Igoe, D.; Barrett, P. Factors associated with lower knowledge of HIV and STI transmission, testing and treatment among MSM in Ireland: Findings from the MSM Internet Survey Ireland (MISI) 2015. Sex Transm. Infect. 2021, 97, 351–356. [Google Scholar] [CrossRef]
- Bozicević, I.; Stulhofer, A.; Ajduković, D.; Kufrin, K. Patterns of sexual behaviour and reported symptoms of STI/RTIs among young people in Croatia--implications for interventions’ planning. Coll. Antropol. 2006, 30 (Suppl. S2), 63–70. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Variable | N | N Positive | Prevalence (%) | p-Value * | POR ** (IC 95%) |
|---|---|---|---|---|---|
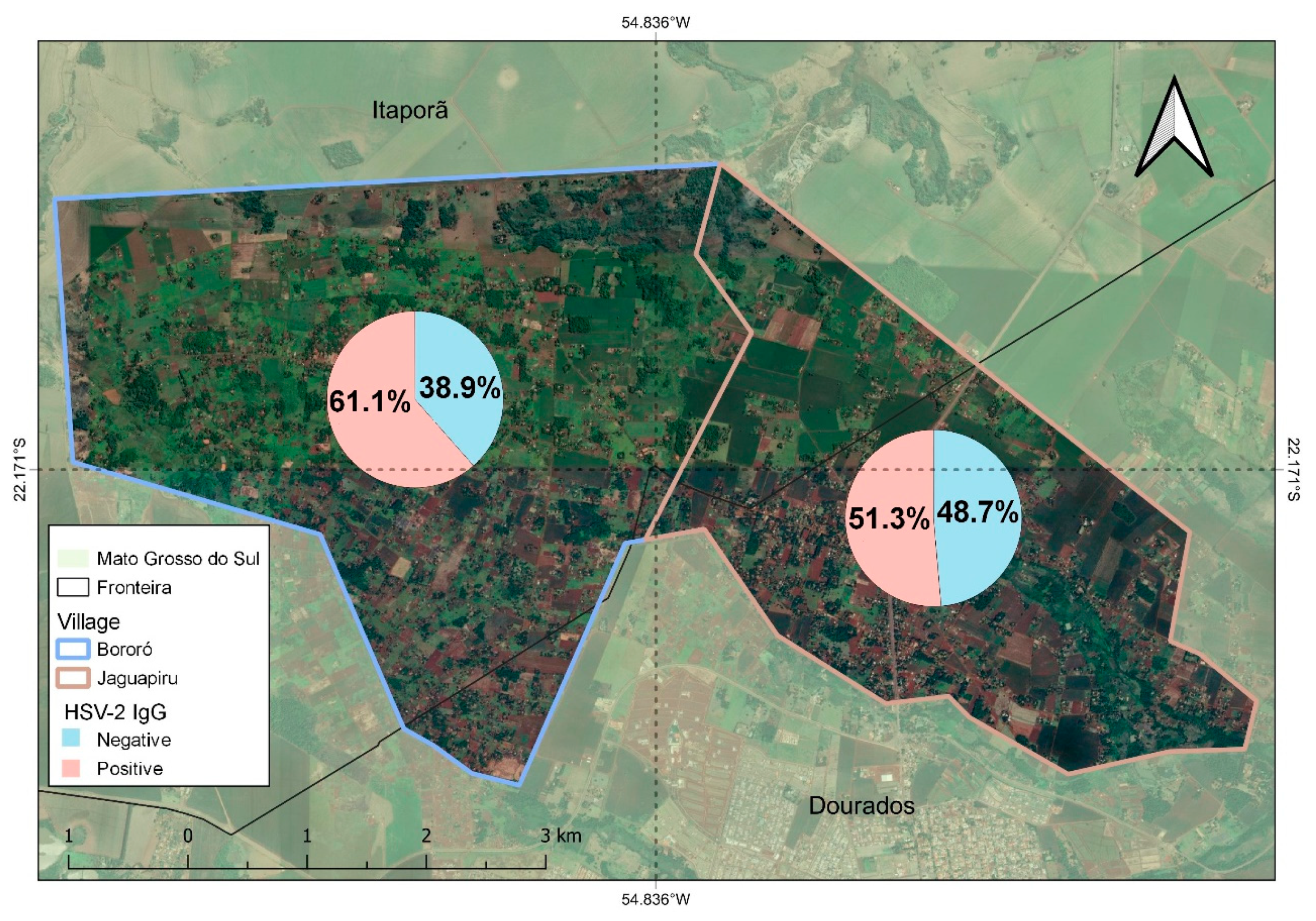
| Village | <0.001 | ||||
| Jaguapiru | 555 | 285 | 51.3% | 0.67 (0.53–0.88) | |
| Bororó | 805 | 495 | 61.1% | ||
| Gender | <0.001 | ||||
| Female | 1056 | 629 | 59.5% | ||
| Male | 304 | 149 | 49.0% | 0.64 (0.49–0.83) | |
| Lived in another village previously | 255 | 152 | 59.6% | 0.02 | 1.41 (1.06–1.87) |
| Family allowance | 667 | 403 | 60.4% | 0.01 | 1.3 (1.05–1.61) |
| Retired | 97 | 71 | 73.2% | 0.001 | 2.13 (1.36–3.45) |
| Cell phone | 999 | 551 | 55.1% | 0.01 | 0.73 (0.57–0.94) |
| Television | 644 | 336 | 52.2% | 0.001 | 0.69 (0.55–0.86) |
| Internet | 281 | 87 | 30.9% | <0.001 | 0.41 (0.4–0.54) |
| Ethnicities | |||||
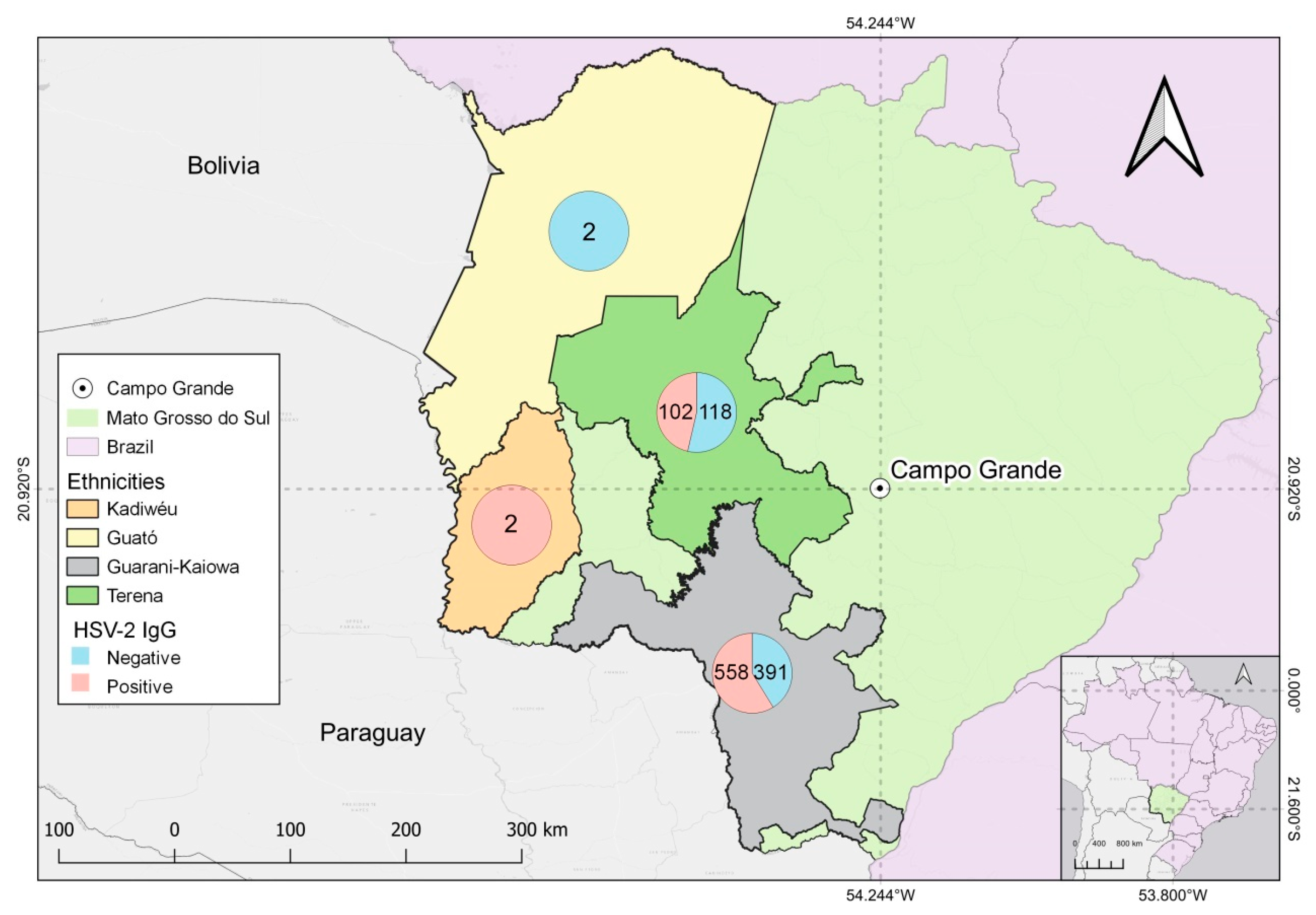
| Guarani-Kaiowá | 949 | 558 | 58.8% | 0.02 | 1.32 (1.04–1.6) |
| Terena | 220 | 102 | 46.3% | 0.001 | 0.60 (0.45–0.81) |
| Guarani-Nhandeva | 18 | 9 | 50.0% | 0.69 | |
| Kadiwéu | 2 | 2 | 100% | 0.61 | |
| Guató | 2 | - | - | 0.35 | |
| Education | <0.001 | ||||
| Elementary School | 859 | 526 | 61.2% | ||
| High School | 296 | 129 | 43.6% | 0.48 (0.56–0.63) | |
| College education | 55 | 19 | 34.5% | 0.33 (0.18–0.57) | |
| Working | 413 | 217 | 52.5% | 0.02 | 0.76 (0.6–0.96) |
| Smoking | 656 | 398 | 60.7% | 0.008 | 1.34 (1.08–1.6) |
| Use of Condoms | 504 | 266 | 52.9% | 0.01 | 0.75 (0.60–0.93) |
| Income | 0.02 | ||||
| 1 to 2 minimum wages | 494 | 263 | 53.5% | ||
| 3 to 4 minimum wages | 71 | 28 | 39.4% | 0.56 (0.33–0.93) | |
| >5 minimum wages | 11 | 3 | 27.3% | 0.32 (0.07–1.14) | |
| Former inmate | 38 | 23 | 60.5% | 0.81 | |
| Alcoholism | 348 | 189 | 54.3% | 0.21 | |
| Illicit drogs | 45 | 20 | 44.4% | 0.10 | |
| Tatoo | 339 | 188 | 56.0% | 0.60 | |
| Syringe and needle sharing | 163 | 93 | 57.4% | 0.99 | |
| Sexual intercourse with a partner who is a non-injecting illicit drug user | 110 | 65 | 79.6% | 0.68 | |
| Sexual intercourse with partner who is an injecting drug user | 12 | 5 | 41.7% | 0.42 | |
| Sex worker | 17 | 11 | 64.7% | 0.70 | |
| Homosexual relationship | 26 | 16 | 61.5% | 0.81 |
| Variable | Guarani-Kaiowá | Guarani-Nhandeva | Terena | |||
|---|---|---|---|---|---|---|
| Income | N (%) | p-value * | N (%) | p-value | N (%) | p-value |
| 0.03 | 0.22 | 0.22 | ||||
| 1 to 2 minimum wages | 319 (64.6) | 9 (1.8) | 108 (21.9) | |||
| 3 to 4 minimum wages | 35 (49.3) | 2 (2.8) | 22 (31.0) | |||
| >5 minimum wages | 6 (54.5) | 1 (9.1) | 3 (27.3) | |||
| Education | <0.01 | 0.11 | <0.01 | |||
| Elementary school | 639 (0.74) | 8 (0.9) | 121 (14.1) | |||
| High school | 172 (0.58) | 6 (2.0) | 67 (22.6) | |||
| College education | 28 (50.9) | 2 (3.6) | 17 (30.9) | |||
| N | N Positive | Prevalence | p-Value * | |
|---|---|---|---|---|
| Urinary problems | 155 | 22 | 14.2 | 0.7 |
| Genital Wounds | 57 | 7 | 12.3 | - |
| Genital Warts | 26 | 4 | 15.4 | 0.93 |
| Urethral discharge | 138 | 20 | 14.5 | 0.65 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bonfim, F.F.d.O.; Villar, L.M.; Croda, J.; Silva, S.R.d.; Gonçalves, C.C.M.; de Castro, V.d.O.L.; de Rezende Romeira, G.R.; Cesar, G.A.; dos Santos Weis-Torres, S.M.; Horta, M.A.; et al. Epidemiological Survey of Human Alphaherpesvirus 2 (HSV-2) Infection in Indigenous People of Dourados Municipality, Central Brazil. Trop. Med. Infect. Dis. 2023, 8, 197. https://doi.org/10.3390/tropicalmed8040197
Bonfim FFdO, Villar LM, Croda J, Silva SRd, Gonçalves CCM, de Castro VdOL, de Rezende Romeira GR, Cesar GA, dos Santos Weis-Torres SM, Horta MA, et al. Epidemiological Survey of Human Alphaherpesvirus 2 (HSV-2) Infection in Indigenous People of Dourados Municipality, Central Brazil. Tropical Medicine and Infectious Disease. 2023; 8(4):197. https://doi.org/10.3390/tropicalmed8040197
Chicago/Turabian StyleBonfim, Flávia Freitas de Oliveira, Livia Melo Villar, Julio Croda, Solange Rodrigues da Silva, Crhistinne Cavalheiro Maymone Gonçalves, Vivianne de Oliveira Landgraf de Castro, Grazielli Rocha de Rezende Romeira, Gabriela Alves Cesar, Sabrina Moreira dos Santos Weis-Torres, Marco Aurélio Horta, and et al. 2023. "Epidemiological Survey of Human Alphaherpesvirus 2 (HSV-2) Infection in Indigenous People of Dourados Municipality, Central Brazil" Tropical Medicine and Infectious Disease 8, no. 4: 197. https://doi.org/10.3390/tropicalmed8040197
APA StyleBonfim, F. F. d. O., Villar, L. M., Croda, J., Silva, S. R. d., Gonçalves, C. C. M., de Castro, V. d. O. L., de Rezende Romeira, G. R., Cesar, G. A., dos Santos Weis-Torres, S. M., Horta, M. A., Simionatto, S., Motta-Castro, A. R. C., & de Paula, V. S. (2023). Epidemiological Survey of Human Alphaherpesvirus 2 (HSV-2) Infection in Indigenous People of Dourados Municipality, Central Brazil. Tropical Medicine and Infectious Disease, 8(4), 197. https://doi.org/10.3390/tropicalmed8040197