Abstract
Central nervous system (CNS) infections constitute a life-threatening condition, especially in children. Treatment limitations exist for drug-resistant CNS bacterial infections. Inadequate CNS penetration and intravenous (IV) antibiotic treatment failure represent a major clinical challenge. However, patients with antibiotic-resistant bacterial CNS infections may benefit from intrathecal (IT) or intraventricular (IVT) colistin. The authors aimed to assess the safety and effectiveness of IT/IVT colistin therapy in the pediatric population, with or without other antibiotics, for the treatment of antibiotic-resistant CNS infections. A comprehensive literature search was conducted using the electronic databases of PubMed, Ovid, and Embase for relevant articles using the following terms: “Colistin”, “CNS infection”, and “Outcome”, as well as their combinations. The retrieved articles were filtered by age (Child), language (English), route of administration (IT/IVT), and species (Humans). The present systematic review comprised 20 articles that included 31 children (19; 61.2% were boys) with multidrug-resistant CNS infection. Their ages ranged from less than one month to 18 years (median: 9 months). Acinetobacter baumannii was the main causative organism in 22 patients (70.9%), and infection occurred mainly after neurosurgical interventions (83.8%). An external ventricular drain was inserted to administer colistin into the ventricular system in 29 cases (93.5%). The median duration for colistin therapy was 18 days. Twenty-three patients (74%) recovered, while five patients (16%) had residual disability, and three patients (10%) died. The authors concluded that IT/IVT colistin therapy is safe and effective as either the primary or adjunct treatment for antibiotic-resistant cases with CNS infection.
1. Introduction
Infections of the central nervous system (CNS) may develop in patients with traumatic brain injury after external ventricular drainage insertion and, broadly, after any neurosurgery procedure. Various bacteria are responsible for these infections, especially Staphylococcus epidermidis, but Gram-negative bacteria are responsible for almost 15% of CNS infections. Many patients with CNS infections develop systemic and neurologic complications, with potential sequelae in the survivors and substantial mortality. These infections require prompt diagnosis and management, which depend mainly on the local epidemiology and patterns of antibiotic resistance of common pathogens [1,2].
It has been shown that the extensive use of antibiotics after neurosurgical CNS infections might alter their epidemiology. External ventricular drainage is one of the common procedures performed in neurosurgery associated with a variable infection rate ranging from 2% to 33% [3].
Due to the increasing emergence of multidrug-resistant bacteria (MDR) (e.g., Acinetobacter, A. baumannii, Pseudomonas aeruginosa, and Klebsiella pneumoniae) [4,5], treatment of CNS infections has become increasingly difficult. Several bacteria have become susceptible only to colistin and polymyxin B. Colistin is a complex mixture of polymyxins, mainly polymyxin E1 and polymyxin E2. It was the first antibiotic with notable in vitro activity against P. aeruginosa [1].
Colistin began to be used in the treatment of multidrug-resistant A. baumannii infections [6]. However, since there is a limited penetration of intravenous colistin to the cerebrospinal fluid, IT or IVT treatment is commonly applied in CNS infections [7].
This study aimed to assess the effectiveness of IT/IVT colistin therapy, with or without other antibiotics, for the treatment of antibiotic-resistant CNS infections in the pediatric population, as the existing evidence in the literature is mostly about adult patients, with little emphasis on pediatric patients apart from scattered case reports and case series [6].
2. Materials and Methods
We conducted a comprehensive literature search using the electronic databases of PubMed, Ovid, and Embase for relevant articles during the period 2000–2021. The following terms were used: “Colistin”, “CNS infection”, and “Outcome”, as well as their combinations. A total of 244 articles was retrieved. After the removal of duplicates (six articles), the articles were filtered by age (Child), language (English), and species (Humans); 28 articles were eligible. However, eight articles were also removed because of the unavailability of the full text. Finally, this study included 20 articles with 31 cases (Figure 1). The PRISMA 2020 checklist is attached in the Supplementary Materials.
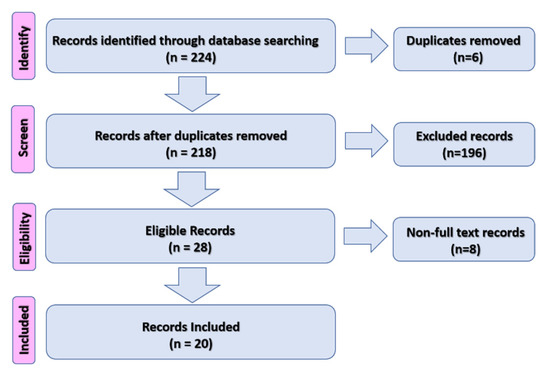
Figure 1.
Flow chart of the study procedures.
3. Results
The present systematic review comprised 20 articles that included 31 children (16; 61.2% were boys) with CNS infections. Table 1 shows the summary of the main findings of included studies.

Table 1.
Summary of the main findings of the included studies.
Their ages ranged from less than one month to 18 years (median: 9 months). In all cases, IT/IVT colistin was administered.
Acinetobacter baumannii was the main causative organism in 22 cases (70.9%), while P. aeruginosa was the causative organism in three cases (9.6%), Enterobacter cloacae was the causative organisms in two cases (≈6.5%), and more than one organism was seen in three patients (9.6%). K. pneumoniae was the causative organism in four cases (≈13%); however, three of them were associated with another organism (Figure 2).
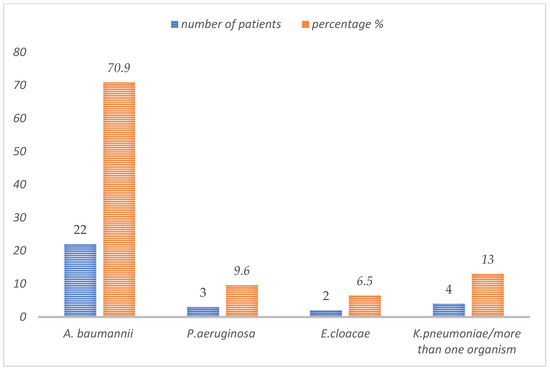
Figure 2.
Causative organisms of CNS infections in pediatric patients treated with IV/IT colistin.
The route of infection in the review cases was mainly after neurosurgical interventions (26 cases, 83.8%). An external ventricular drain was inserted in 29 cases (93.5%). The median duration for colistin therapy was 18 days. Twenty-three patients (74%) recovered, while five patients (16%) had residual disability, and three patients (10%) died.
4. Discussion
CNS infections are associated with high morbidity and the case fatality rate, in addition to a significant cost to the healthcare system.
Despite colistin being introduced in clinical practice in 1947, it was not until recent years that concerns were raised regarding the low level of colistin concentration in the cerebrospinal fluid, leading to a concern for poor penetration of the blood–brain barrier, which has led to the possibility of IT/IVT administration to achieve direct eradication of the causative organism [6]. It was also reported that only 5–25% of IV colistin crosses into the CSF [18]. Even in patients with meningitis, with a disrupted blood–brain barrier, this rate does not exceed 25%. On the other hand, several studies proved the efficacy of IT and IVT colistin administration [14,26]. However, the first report of intrathecal administration of colistin in a pediatric patient was back in 1990 [8].
In recent years, A. baumannii has appeared as an important pathogen, especially in hospital-acquired infections [27]. The risk factors for infection are neurosurgical procedures, CSF leak, a prolonged use of intravascular devices, prior treatment with broad-spectrum antibiotics, prior colonization with Acinetobacter, prolonged mechanical ventilation, and ICU stay, as well as intracranial hemorrhage [6].
It was reported that the incidence of CNS infections is associated with ventricular devices, with more than 50% of the episodes occurring within the first month of implant placement [17]. Therefore, it is generally advised in cases of CSF shunt infections that all components of infected shunts or external drainage devices be removed and appropriate antimicrobial therapy be administered in combinations [28].
In the USA, there are no FDA-approved antimicrobial agents for intraventricular use [25]. Intraventricular colistin is being used off-label to sterilize the cerebrospinal fluid. Moreover, the dosages for antimicrobials have been empiric, with dose adjustments and dosing intervals mainly based on pharmacokinetic calculations to achieve adequate CNS concentrations [28].
Polymyxins are increasingly used for the treatment of CNS infections caused by multidrug-resistant Gram-negative bacteria. Four polymyxins exhibit rapid bacterial killing against most Gram-negative microorganisms by disturbing the bacterial cell membrane and can block the biologic effects of endotoxins [26]. However, intravenously administered polymyxins do not achieve high concentrations in the CNS. Therefore, IVT and ITH have been recommended in patients with CNS device infections that are difficult to eradicate or who cannot undergo the surgical removal of infected devices [7].
Many studies addressed the safety and effectiveness of IT/IVT colistin administration in adults, and some of these studies included pediatric patients. However, no study was encountered during our search that focused on the pediatric population, apart from case reports and case series or being involved with adult patients in some review [6].
The authors noticed a drop in the number of published cases of IT/IVT colistin in the pediatric population over the last five years in comparison to the years before. This may reflect that clinicians are widely using it, being convinced of its safety from the existing literature, or it may reflect the flip side of the coin, where it is not widely accepted in practice.
The toxicity from intrathecal or intraventricular therapy with colistin is a major challenge, especially with respect to aseptic or chemical meningitis, which is very hard to differentiate clinically from bacterial meningitis. However, the CSF parameters are the only key in differentiating the two [6]. Despite that, the three deaths that were encountered in our review were not related directly to the intrathecal toxicity, as one child, for instance, died from consequences of hydrocephalus, and the team with the family reached the conclusion of withdrawing care after the EVD was inadvertently dislodged [25], and another child died from the consequences of sepsis [15].
A recent study addressed the use of colistin in neonates, which is one of the largest series of its kind, and the authors found that six out of seven patients who received IT/IVT colistin survived, where five of them received it in combination with IV colistin, and the one that died received only IT/IVY colistin [29]. The study went on further to report the neurodevelopmental outcome. The authors reported three patients who had a seizure disorder on follow-up, and the only patient with moderate disability had both hearing and visual impairments [29].
The current review is the first of its kind to address the safety and effectiveness of IT/IVT colistin in the pediatric population. Despite the mortality and disability that were reported, it is difficult to determine whether this is a result of the primary pathology or adverse effects of colistin [10]. The authors believe that IT/IVT as a last resort of the management of serious CNS infections should be pursued without delay. However, caution throughout the treatment period should be implemented by all treating teams, which should include pediatric neurosurgeons, infectious disease specialists, neurologists, clinical pharmacologists, etc.
There was no consistency regarding the dosage of IT/IVT used in these studies. However, a dose of 0.16–0.24 mg/kg every 24 h was most commonly used [6,15]. Some studies used up to 10 mg every 24 h, which appeared to be a high dose in, for instance, a three-year-old child; despite that, it is hard to comment on the appropriateness of the dose with the lack of data on the weight of children [13].
5. Limitations of the Review
The small number of patients was one of the challenges encountered. However, based on the search flowchart, we included all studies that met the criteria, and to the best of our knowledge, this review has the biggest number of pediatric patients who received IT/IVT in the literature. The other challenge is the inconsistency in the reporting of the time of initiation of IV/IVT, whether it was immediately after diagnosis or after failure of intravenous treatment; in the case of the latter, there is also inconsistency regarding the wait time for the intravenous medication before declaring its failure and, consequently, starting IV/IVT colistin.
The authors recommend further studies and suggest that a well-structured randomized control trial may be able address this concern.
6. Conclusions
IT/IVT colistin therapy is a safe and effective last resort of management as either the primary or adjunct treatment for antibiotic-resistant cases with CNS infections in the pediatric population.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/tropicalmed7030041/s1. Table S1: Summary of the main findings of included studies.
Author Contributions
Conceptualization, I.A.; methodology, I.A.; software, I.A.; validation, I.A. and Z.A.; formal analysis, I.A. and Z.A.; investigation, I.A. and Z.A.; resources, I.A. and Z.A.; data curation I.A. and Z.A.; writing—original draft preparation, I.A. and Z.A.; writing—review and editing, I.A.; visualization, I.A. and Z.A.; project administration, I.A.; funding acquisition, I.A. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The paper is exempt from ethical committee approval/written informed consent, as this paper is based on reviewing existing literature.
Informed Consent Statement
Not applicable.
Data Availability Statement
All data generated or analyzed during this study are included in this article. Further enquiries can be directed to the corresponding author.
Conflicts of Interest
The authors have no conflict of interest to declare.
References
- Imberti, R.; Iotti, G.A.; Regazzi, M. Intraventricular or intrathecal colistin for the treatment of central nervous system infections caused by multidrug-resistant Gram-negative bacteria. Expert Rev. Anti-Infective Ther. 2014, 12, 471–478. [Google Scholar] [CrossRef] [PubMed]
- Brouwer, M.; van de Beek, D. Management of bacterial central nervous system infections. In Critical Care Neurology. Part I. Handbook of Clinical Neurology, 1st ed.; 3rd Series; Wijdicks, E.F.M., Kramer, A.H., Eds.; Elsevier: Amsterdam, The Netherlands, 2017; Volume 140. [Google Scholar] [CrossRef]
- De Pascale, G.; Pompucci, A.; Maviglia, R.; Spanu, T.; Bello, G.; Mangiola, A.; Scoppettuolo, G. Successful treatment of multidrug-resistant Acinetobacter baumannii ventriculitis with intrathecal and intravenous colistin. Minerva Anestesiol. 2010, 76, 957–960. [Google Scholar] [PubMed]
- Tartor, Y.H.; Gharieb, R.M.A.; El-Aziz, N.K.A.; El Damaty, H.M.; Enany, S.; Khalifa, E.; Attia, A.S.A.; Abdellatif, S.S.; Ramadan, H. Virulence Determinants and Plasmid-Mediated Colistin Resistance mcr Genes in Gram-Negative Bacteria Isolated from Bovine Milk. Front. Cell. Infect. Microbiol. 2021, 11, 761417. [Google Scholar] [CrossRef] [PubMed]
- Tartor, Y.H.; El-Aziz, N.K.A.; Gharieb, R.M.A.; El Damaty, H.M.; Enany, S.; Soliman, E.A.; Abdellatif, S.S.; Attia, A.S.A.; Bahnass, M.M.; El-Shazly, Y.A.; et al. Whole-Genome Sequencing of Gram-Negative Bacteria Isolated from Bovine Mastitis and Raw Milk: The First Emergence of Colistin mcr-10 and Fosfomycin fosA5 Resistance Genes in Klebsiella pneumoniae in Middle East. Front. Microbiol. 2021, 12, 770813. [Google Scholar] [CrossRef]
- Karaiskos, I.; Galani, L.; Baziaka, F.; Giamarellou, H. Intraventricular and intrathecal colistin as the last therapeutic resort for the treatment of multidrug-resistant and extensively drug-resistant Acinetobacter baumannii ventriculitis and meningitis: A literature review. Int. J. Antimicrob. Agents 2013, 41, 499–508. [Google Scholar] [CrossRef] [PubMed]
- Markantonis, S.L.; Markou, N.; Fousteri, M.; Sakellaridis, N.; Karatzas, S.; Alamanos, I.; Dimopoulou, E.; Baltopoulos, G. Penetration of Colistin into Cerebrospinal Fluid. Antimicrob. Agents Chemother. 2009, 53, 4907–4910. [Google Scholar] [CrossRef]
- Kaplan, S.L.; Patrick, C.C. Cefotaxime and aminoglycoside treatment of meningitis caused by Gram-negative enteric organisms. Pediatr. Infect. Dis. J. 1990, 9, 810–814. [Google Scholar] [CrossRef]
- Fernandez-Viladrich, P.; Corbella, X.; Corral, L.; Tubau, F.; Mateu, A. Successful Treatment of Ventriculitis Due to Carbapenem-ResistantAcinetobacter baumanniiwith Intraventricular Colistin Sulfomethate Sodium. Clin. Infect. Dis. 1999, 28, 916–917. [Google Scholar] [CrossRef][Green Version]
- Ng, J.; Gosbell, I.B.; Kelly, J.A.; Boyle, M.J.; Ferguson, J.K. Cure of multiresistant Acinetobacter baumannii central nervous system infections with intraventricular or intrathecal colistin: Case series and literature review. J. Antimicrob. Chemother. 2006, 58, 1078–1081. [Google Scholar] [CrossRef]
- Yagmur, R.; Esen, F. Intrathecal colistin for treatment of Pseudomonas aeruginosa ventriculitis: Report of a case with successful outcome. Crit. Care 2006, 10, 428. [Google Scholar] [CrossRef][Green Version]
- Dalgic, N.; Ceylan, Y.; Sancar, M.; Telhan, L.; Kafadar, I.; Cavusoglu, H.; Ceylan, O.; Hasim, O. Successful treatment of multidrug-resistant Acinetobacter baumannii ventriculitis with intravenous and intraventricular colistin. Ann. Trop. Paediatr. 2009, 29, 141–147. [Google Scholar] [CrossRef] [PubMed]
- Özdemir, H.; Tapısız, A.; Çiftçi, E.; Ince, E.; Mokhtari, H.; Güriz, H.; Aysev, A.D.; Doğru, Ü.; Tapisiz, A. Successful treatment of three children with post-neurosurgical multidrug-resistant Acinetobacter baumannii meningitis. Infection 2010, 38, 241–244. [Google Scholar] [CrossRef] [PubMed]
- Cascio, A.; Conti, A.; Sinardi, L.; Iaria, C.; Angileri, F.F.; Stassi, G.; David, T.; Versaci, A.; Iaria, M.; David, A. Post-neurosurgical multidrug-resistant Acinetobacter baumannii meningitis successfully treated with intrathecal colistin. A new case and a systematic review of the literature. Int. J. Infect. Dis. 2010, 14, e572–e579. [Google Scholar] [CrossRef] [PubMed]
- Saleem, A.F.; Shah, M.S.; Shaikh, A.S.; Mir, F.; Zaidi, A.K.M. Acinetobacter species meningitis in children: A case series from Karachi, Pakistan. J. Infect. Dev. Ctries. 2011, 5, 809–814. [Google Scholar] [CrossRef]
- Wang, J.-H.; Lin, P.-C.; Chou, C.-H.; Ho, C.-M.; Lin, K.-H.; Tsai, C.-T.; Wang, J.-H.; Chi, C.-Y.; Ho, M.-W. Intraventricular antimicrobial therapy in postneurosurgical Gram-negative bacillary meningitis or ventriculitis: A hospital-based retrospective study. J. Microbiol. Immunol. Infect. 2014, 47, 204–210. [Google Scholar] [CrossRef]
- Bargiacchi, O.; Rossati, A.; Car, P.; Brustia, D.; Brondolo, R.; Rosa, F.; Garavelli, P.L.; DE Rosa, F.G. Intrathecal/intraventricular colistin in external ventricular device-related infections by multi-drug resistant Gram negative bacteria: Case reports and review. Infection 2014, 42, 801–809. [Google Scholar] [CrossRef]
- Tekgunduz, K.S.; Kara, M.; Caner, I.; Demirelli, Y. Safety and Efficacy of Intravenous Colistin in Neonates with Culture Proven Sepsis. Iran. J. Pediatr. 2015, 25, e453. [Google Scholar] [CrossRef]
- Santos, A.S.; Iraneta, A.; Matos, M.; Brito, M.J. Intraventricular colistin in Gram-negative ventriculoperitoneal shunt infection in two pediatric patients. Acta Neurochir. 2015, 157, 2219–2220. [Google Scholar] [CrossRef][Green Version]
- Tekgündüz, K.S.; Demirelli, Y.; Caner, I.; Kara, M. Intraventricular colistin use in a premature infant with cerebral abscess and ventriculitis. J. Clin. Neonatol. 2015, 4, 132–134. [Google Scholar] [CrossRef]
- Mahabeer, P.; Mzimela, B.W.; Lawler, M.A.; Singh-Moodley, A.; Singh, R.; Mlisana, K.P. Colistin-resistantAcinetobacter baumanniias a cause of neonatal ventriculitis. S. Afr. J. Infect. Dis. 2018, 33, 1–3. [Google Scholar] [CrossRef]
- Rao, K.; Rangappa, P.; Jacob, I.; Hiremath, P. Cerebrospinal fluid lactate as a prognostic indicator in postneurosurgical bacterial meningitis and use of intrathecal colistin. Indian J. Crit. Care Med. 2018, 22, 297–299. [Google Scholar] [CrossRef] [PubMed]
- Abad-Restrepo, J.; Díaz-Díaz, A.; Osorio-Cadavid, N. Post-surgical ventriculitis due to extensively resistant Pseudomonas aeruginosa treated with intrathecal colistin: Pediatric case report and literature review. Rev. Chil. Infectología 2018, 35, 321–325. [Google Scholar] [CrossRef] [PubMed]
- Alzailaie, A.K.; Aljarie, A.A.; Abdelwahab, H.M. Successful Outcome in Treating Ventriculitis with Intrathecal Colistin in a Child. Bahrain Med. Bull. 2018, 40, 59–60. [Google Scholar] [CrossRef]
- Al Yazidi, L.S.; McMullan, B.; Kohan, S.; Palasanthiran, P. Persistent Gram-negative Neurosurgical Meningitis in a Neonate, Successfully Treated with Intraventricular Colistin: Case Report and Review of the Literature. Pediatr. Infect. Dis. J. 2018, 37, e79–e81. [Google Scholar] [CrossRef]
- Falagas, M.E.; Bliziotis, I.A.; Tam, V.H. Intraventricular or intrathecal use of polymyxins in patients with Gram-negative meningitis: A systematic review of the available evidence. Int. J. Antimicrob. Agents 2007, 29, 9–25. [Google Scholar] [CrossRef]
- Giamarellou, H.; Antoniadou, A.; Kanellakopoulou, K. Acinetobacter baumannii: A universal threat to public health? Int. J. Antimicrob. Agents 2008, 32, 106–119. [Google Scholar] [CrossRef]
- Tunkel, A.R.; Hartman, B.J.; Kaplan, S.L.; Kaufman, B.A.; Roos, K.L.; Scheld, W.M.; Whitley, R.J. Practice Guidelines for the Management of Bacterial Meningitis. Clin. Infect. Dis. 2004, 39, 1267–1284. [Google Scholar] [CrossRef]
- Hussain, K.; Salat, M.S.; Ambreen, G.; Iqbal, J. Neurodevelopment Outcome of Neonates Treated with Intraventricular Colistin for Ventriculitis Caused by Multiple Drug-Resistant Pathogens—A Case Series. Front. Pediatr. 2021, 8, 843. [Google Scholar] [CrossRef]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).