
COVID-19 Alcoholic Cirrhosis and Non-Alcoholic Steatohepatitis Cirrhosis Outcomes among Hospitalized Patients in the United States: Insight from National Inpatient Sample Database

 , , ,
, , , 
 and
and 
Abstract
1. Introduction
2. Materials and Method
2.1. Data Source
2.2. Covariates
- a.
- Patient-level: Age, race, sex, comorbidities, insurance status, income in patient’s zip code, disposition.
- b.
- Hospital level: Location, teaching status, bed size, region.
- c.
- Illness severity: Length of stay (LOS), mortality, hospitalization cost, Elixhauser comorbidity score, in-hospital complications, mechanical ventilation, circulatory support and vasopressor use, NACSELD-ALF score.
2.3. Study Outcomes
2.4. Statistical Methods
3. Results
3.1. Patient Characteristics
3.2. In-Hospital Outcomes
3.3. Subgroup Analysis
3.4. Mortality Predictors
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gasmi, A.; Peana, M.; Pivina, L.; Srinath, S.; Gasmi Benahmed, A.; Semenova, Y.; Menzel, A.; Dadar, M.; Bjørklund, G. Interrelations between COVID-19 and other disorders. Clin. Immunol. 2021, 224, 108651. [Google Scholar] [CrossRef] [PubMed]
- Cheemerla, S.; Balakrishnan, M. Global epidemiology of chronic liver disease. Clin. Liver Dis. 2021, 17, 365–370. [Google Scholar] [CrossRef] [PubMed]
- Albillos, A.; Martin-Mateos, R.; Van der Merwe, S.; Wiest, R.; Jalan, R.; Álvarez-Mon, M. Cirrhosis-associated immune dysfunction. Nat. Rev. Gastroenterol. Hepatol. 2022, 19, 112–134. [Google Scholar] [CrossRef] [PubMed]
- Chela, H.K.; Tallon, E.M.; Baskett, W.; Gangu, K.; Tahan, V.; Shyu, C.-R.; Daglilar, E. Liver injury on admission linked to worse outcomes in COVID-19: An analysis of 14,138 patients. Transl. Gastroenterol. Hepatol. 2021, 1–23. [Google Scholar] [CrossRef]
- Chela, H.K.; Pasha, S.B.; Basar, O.; Daglilar, E.; Tahan, V. Liver in the limelight in the corona (COVID-19) time. World J. Clin. Cases 2020, 8, 3405–3410. [Google Scholar] [CrossRef]
- Jeon, D.; Son, M.; Choi, J. Impact of liver cirrhosis on the clinical outcomes of patients with COVID-19: A nationwide cohort study of Korea. Korean J. Intern. Med. 2021, 36, 1092–1101. [Google Scholar] [CrossRef] [PubMed]
- Medhat, M.A.; El Kassas, M. Letter regarding “High rates of 30-day mortality in patients with cirrhosis and COVID-19”. J. Hepatol. 2020, 73, 1569–1570. [Google Scholar] [CrossRef]
- Bajaj, J.S.; Garcia-Tsao, G.; Biggins, S.W.; Kamath, P.S.; Wong, F.; McGeorge, S.; Shaw, J.; Pearson, M.; Chew, M.; Fagan, A.; et al. Comparison of mortality risk in patients with cirrhosis and COVID-19 compared with patients with cirrhosis alone and COVID-19 alone: Multicentre matched cohort. Gut 2021, 70, 531–536. [Google Scholar] [CrossRef] [PubMed]
- Moon, A.M.; Webb, G.J.; Aloman, C.; Armstrong, M.J.; Cargill, T.; Dhanasekaran, R.; Genescà, J.; Gill, U.S.; James, T.W.; Jones, P.D.; et al. High mortality rates for SARS-CoV-2 infection in patients with pre-existing chronic liver disease and cirrhosis: Preliminary results from an international registry. J. Hepatol. 2020, 73, 705–708. [Google Scholar] [CrossRef] [PubMed]
- Schütte, A.; Ciesek, S.; Wedemeyer, H.; Lange, C.M. Influenza virus infection as precipitating event of acute-on-chronic liver failure. J. Hepatol. 2019, 70, 797–799. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, M.L.; Barritt, A.S.; Orman, E.S.; Hayashi, P.H. Decreasing mortality among patients hospitalized with cirrhosis in the United States from 2002 through 2010. Gastroenterology 2015, 148, 967–977.e2. [Google Scholar] [CrossRef]
- Ge, J.; Pletcher, M.J.; Lai, J.C. N3C Consortium Outcomes of SARS-CoV-2 Infection in Patients with Chronic Liver Disease and Cirrhosis: A National COVID Cohort Collaborative Study. Gastroenterology 2021, 161, 1487–1501.e5. [Google Scholar] [CrossRef]
- Grgurevic, I.; Lucijanić, M.; Pastrovic, F.; Barisic Jaman, M.; Tjesic Drinkovic, I.; Zelenika, M.; Milosevic, M.; Medic, B.; Kardum, D.; Bokun, T.; et al. Short-term outcomes of patients with chronic liver disease hospitalised with COVID-19. Intern. Med. J. 2022, 52, 1891–1899. [Google Scholar] [CrossRef] [PubMed]
- Yoo, H.W.; Jin, H.Y.; Yon, D.K.; Effenberger, M.; Shin, Y.H.; Kim, S.Y.; Yang, J.M.; Kim, M.S.; Koyanagi, A.; Jacob, L.; et al. Non-alcoholic Fatty Liver Disease and COVID-19 Susceptibility and Outcomes: A Korean Nationwide Cohort. J. Korean Med. Sci. 2021, 36, e291. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.; Adeniji, N.; Latt, N.; Kumar, S.; Bloom, P.P.; Aby, E.S.; Perumalswami, P.; Roytman, M.; Li, M.; Vogel, A.S.; et al. Predictors of Outcomes of COVID-19 in Patients with Chronic Liver Disease: US Multi-center Study. Clin. Gastroenterol. Hepatol. 2021, 19, 1469–1479.e19. [Google Scholar] [CrossRef] [PubMed]
- Barron, K.S.; Aksentijevich, I.; Deuitch, N.T.; Stone, D.L.; Hoffmann, P.; Videgar-Laird, R.; Soldatos, A.; Bergerson, J.; Toro, C.; Cudrici, C.; et al. The spectrum of the deficiency of adenosine deaminase 2: An observational analysis of a 60 patient cohort. Front. Immunol. 2021, 12, 811473. [Google Scholar] [CrossRef] [PubMed]
- Middleton, P.; Hsu, C.; Lythgoe, M.P. Clinical outcomes in COVID-19 and cirrhosis: A systematic review and meta-analysis of observational studies. BMJ Open Gastroenterol. 2021, 8, e000739. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.; Alshuwaykh, O.; Dennis, B.B.; Cholankeril, G.; Ahmed, A. Trends in Etiology-based Mortality From Chronic Liver Disease Before and During COVID-19 Pandemic in the United States. Clin. Gastroenterol. Hepatol. 2022, 20, 2307–2316.e3. [Google Scholar] [CrossRef]
- Marjot, T.; Eberhardt, C.S.; Boettler, T.; Belli, L.S.; Berenguer, M.; Buti, M.; Jalan, R.; Mondelli, M.U.; Moreau, R.; Shouval, D.; et al. Impact of COVID-19 on the liver and on the care of patients with chronic liver disease, hepatobiliary cancer, and liver transplantation: An updated EASL position paper. J. Hepatol. 2022, 77, 1161–1197. [Google Scholar] [CrossRef] [PubMed]
- Brozat, J.F.; Hanses, F.; Haelberger, M.; Stecher, M.; Dreher, M.; Tometten, L.; Ruethrich, M.M.; Vehreschild, J.J.; Trautwein, C.; Borgmann, S.; et al. LEOSS study group COVID-19 mortality in cirrhosis is determined by cirrhosis-associated comorbidities and extrahepatic organ failure: Results from the multinational LEOSS registry. United Eur. Gastroenterol. J. 2022, 10, 409–424. [Google Scholar] [CrossRef]
- Marjot, T.; Moon, A.M.; Cook, J.A.; Abd-Elsalam, S.; Aloman, C.; Armstrong, M.J.; Pose, E.; Brenner, E.J.; Cargill, T.; Catana, M.-A.; et al. Outcomes following SARS-CoV-2 infection in patients with chronic liver disease: An international registry study. J. Hepatol. 2021, 74, 567–577. [Google Scholar] [CrossRef]
- Mendizabal, M.; Ridruejo, E.; Piñero, F.; Anders, M.; Padilla, M.; Toro, L.G.; Torre, A.; Montes, P.; Urzúa, A.; Gonzalez Ballerga, E.; et al. Comparison of different prognostic scores for patients with cirrhosis hospitalized with SARS-CoV-2 infection. Ann. Hepatol. 2021, 25, 100350. [Google Scholar] [CrossRef] [PubMed]
- COVID-ICU Group on behalf of the REVA Network and the COVID-ICU Investigators. Clinical characteristics and day-90 outcomes of 4244 critically ill adults with COVID-19: A prospective cohort study. Intensive Care Med. 2021, 47, 60–73. [Google Scholar] [CrossRef]
- Gao, F.; Zheng, K.I.; Fan, Y.-C.; Targher, G.; Byrne, C.D.; Zheng, M.-H. ACE2: A Linkage for the Interplay between COVID-19 and Decompensated Cirrhosis. Am. J. Gastroenterol. 2020, 115, 1544. [Google Scholar] [CrossRef]
- Mackey, K.; Ayers, C.K.; Kondo, K.K.; Saha, S.; Advani, S.M.; Young, S.; Spencer, H.; Rusek, M.; Anderson, J.; Veazie, S.; et al. Racial and Ethnic Disparities in COVID-19-Related Infections, Hospitalizations, and Deaths: A Systematic Review. Ann. Intern. Med. 2021, 174, 362–373. [Google Scholar] [CrossRef] [PubMed]
- Gu, T.; Mack, J.A.; Salvatore, M.; Prabhu Sankar, S.; Valley, T.S.; Singh, K.; Nallamothu, B.K.; Kheterpal, S.; Lisabeth, L.; Fritsche, L.G.; et al. Characteristics Associated with Racial/Ethnic Disparities in COVID-19 Outcomes in an Academic Health Care System. JAMA Netw. Open 2020, 3, e2025197. [Google Scholar] [CrossRef] [PubMed]
- Gaspar, R.; Liberal, R.; Branco, C.C.; Macedo, G. Trends in cirrhosis hospitalizations during the COVID-19 pandemic. Dig. Liver Dis. 2020, 52, 942–943. [Google Scholar] [CrossRef] [PubMed]
- Marot, A.; Henrion, J.; Knebel, J.-F.; Moreno, C.; Deltenre, P. Alcoholic liver disease confers a worse prognosis than HCV infection and non-alcoholic fatty liver disease among patients with cirrhosis: An observational study. PLoS ONE 2017, 12, e0186715. [Google Scholar] [CrossRef]
- Szabo, G.; Mandrekar, P. A recent perspective on alcohol, immunity, and host defense. Alcohol. Clin. Exp. Res. 2009, 33, 220–232. [Google Scholar] [CrossRef] [PubMed]
- Kapuria, D.; Upadhyay, S.; Shekhar, R.; Torrazza-Perez, E. Alcoholic Liver Disease and COVID-19 Pneumonia: A Case Series. J. Clin. Transl. Hepatol. 2020, 8, 463–466. [Google Scholar] [CrossRef] [PubMed]
- Shaheen, A.A.; Kong, K.; Ma, C.; Doktorchik, C.; Coffin, C.S.; Swain, M.G.; Burak, K.W.; Congly, S.E.; Lee, S.S.; Sadler, M.; et al. Impact of the COVID-19 Pandemic on Hospitalizations for Alcoholic Hepatitis or Cirrhosis in Alberta, Canada. Clin. Gastroenterol. Hepatol. 2022, 20, e1170–e1179. [Google Scholar] [CrossRef] [PubMed]
- Elhence, A.; Vaishnav, M.; Biswas, S.; Anand, A.; Gunjan, D.; Kedia, S.; Mahapatra, S.J.; Nayak, B.; Sheikh, S.; Soni, K.D.; et al. Shalimar Predictors of in-hospital Outcomes in Patients with Cirrhosis and Coronavirus Disease-2019. J. Clin. Exp. Hepatol. 2022, 12, 876–886. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristics | COVID + Cirrhosis | COVID-Cirrhosis | p Value |
|---|---|---|---|
| N = 822,604 | N= 28,610 (3.47%) | N = 793,994 (96.53%) | |
| SEX (Female) | 40.74% | 41.25% | 0.47 |
| Mean age years (SD) | <0.001 | ||
| Male | 60.51 (12.88) | 59.64 (12.6) | |
| Female | 63.18 (13.4) | 61.03 (13.8) | |
| Age Groups | <0.001 | ||
| ≥18–29 | 321 (1.12%) | 10,242 (1.29%) | |
| 30–49 | 4629 (16.18%) | 146,571 (18.46%) | |
| 50–69 | 15,604 (54.54%) | 447,019 (56.3%) | |
| ≥70 | 8054 (28.15%) | 190,162 (23.95%) | |
| Race | <0.001 | ||
| Caucasians | 14,505 (50.7%) | 539,043 (67.89%) | |
| African American | 3313 (11.58%) | 80,035 (10.08%) | |
| Hispanics | 8059 (28.17%) | 122,672 (15.45%) | |
| Asian or Pacific Islander | 724 (2.53%) | 16,118 (2.03%) | |
| Native American | 796 (2.78%) | 13,895 (1.75%) | |
| Others | 1216 (4.25%) | 22,232 (2.8%) | |
| Median Household Income | <0.001 | ||
| <49,999$ | 10,912 (38.14%) | 265,909 (33.49%) | |
| 50,000–64,999$ | 7482 (26.15%) | 222,556 (28.03%) | |
| 65,000–85,999$ | 5885 (20.57%) | 177,061 (22.3%) | |
| >86,000$ | 4332 (15.14%) | 128,468 (16.18%) | |
| Insurance Status | <0.001 | ||
| Medicare | 14,602 (51.04%) | 385,484 (48.55%) | |
| Medicaid | 6978 (24.39%) | 205,168 (25.84%) | |
| Private | 5791 (20.24%) | 159,116 (20.04%) | |
| Self-pay | 1239 (4.33%) | 442,256 (5.57%) | |
| Hospital Division | <0.001 | ||
| New England | 1416 (4.95%) | 41,844 (5.27%) | |
| Middle Atlantic | 3599 (12.58%) | 88,133 (11.1%) | |
| East North Central | 4160 (14.54%) | 115,129 (14.5%) | |
| West North Central | 1851 (6.47%) | 48,672 (6.13%) | |
| South Atlantic | 4575 (15.99%) | 159,593 (20.1%) | |
| East South Central | 1631 (5.7%) | 56,056 (7.06%) | |
| West South Central | 4680 (16.36%) | 103,854 (13.08%) | |
| Mountain | 2615 (9.14%) | 57,485 (7.24%) | |
| Pacific | 4085 (14.28%) | 123,228 (15.52%) | |
| Hospital Bedsize | 0.51 | ||
| Small | 5816 (20.33%) | 164,039 (20.66%) | |
| Medium | 8266 (28.89%) | 222,318 (28%) | |
| Large | 14,531 (50.79%) | 407,716 (51.35%) | |
| Hosptal Teaching Status | 0.02 | ||
| Rural | 1971 (6.89%) | 58,835 (7.41%) | |
| Urban non-teaching | 4701 (16.43%) | 140,934 (17.75%) | |
| Urban teaching | 21,941 (76.69%) | 594,304 (74.85%) | |
| Comorbidities | |||
| Coronary Artery Disease | 5130 (17.93%) | 148,396 (18.69%) | 0.16 |
| Congestive Heart Failure | 7069 (24.71%) | 197,863 (24.92%) | 0.73 |
| Hypertension | 10,025 (35.04%) | 258,127 (32.51%) | <0.001 |
| Diabetes Mellitus | 14,345 (50.14%) | 313,628 (39.5%) | <0.001 |
| Chronic kidney disease | 8274 (28.92%) | 212,552 (26.77%) | <0.001 |
| Chronic pulmonary disease | 6375 (22.28%) | 196,752 (24.78%) | <0.001 |
| Obesity | 7104 (24.83%) | 155,623 (19.6%) | <0.001 |
| Smoking | 9816 (34.31%) | 363,808 (45.82%) | <0.001 |
| Nacseld-ACLF Score | <0.001 | ||
| 0 | 21,349 (74.62%) | 672,275 (84.67%) | |
| 1 | 3954 (13.82%) | 80,352 (10.12%) | |
| ≥2 | 3304 (11.55%) | 41,367 (5.21%) | |
| Complications | |||
| Portal Hypertension | 5685 (19.87%) | 230,179 (28.99%) | <0.001 |
| Hyponatremia | 7584 (26.51%) | 200,007 (25.19%) | 0.03 |
| Hepatorenal syndrome | 1004 (3.51%) | 41,288 (5.2%) | <0.001 |
| Portal vein thrombosis | 486 (1.7%) | 23,740 (2.99%) | <0.001 |
| SBP # | 555 (1.94%) | 25,249 (3.18%) | <0.001 |
| Variceal bleed | 781 (2.73%) | 42,796 (5.39%) | <0.001 |
| Hepatic encephalopathy | 46 (0.16%) | 1985 (0.25%) | 0.16 |
| Variable | COVID+ | COVID− | p Value |
|---|---|---|---|
| Disposition | <0.001 | ||
| Home/Routine | 15,395 (53.81%) | 455,356 (57.35%) | |
| SNF/LTAC/Nursing home 2 | 7393 (25.84%) | 140,934 (17.75%) | |
| Home health | 5033 (17.59%) | 168,962 (21.28%) | |
| AMA 3 | 790 (2.76%) | 28,743 (3.62%) | |
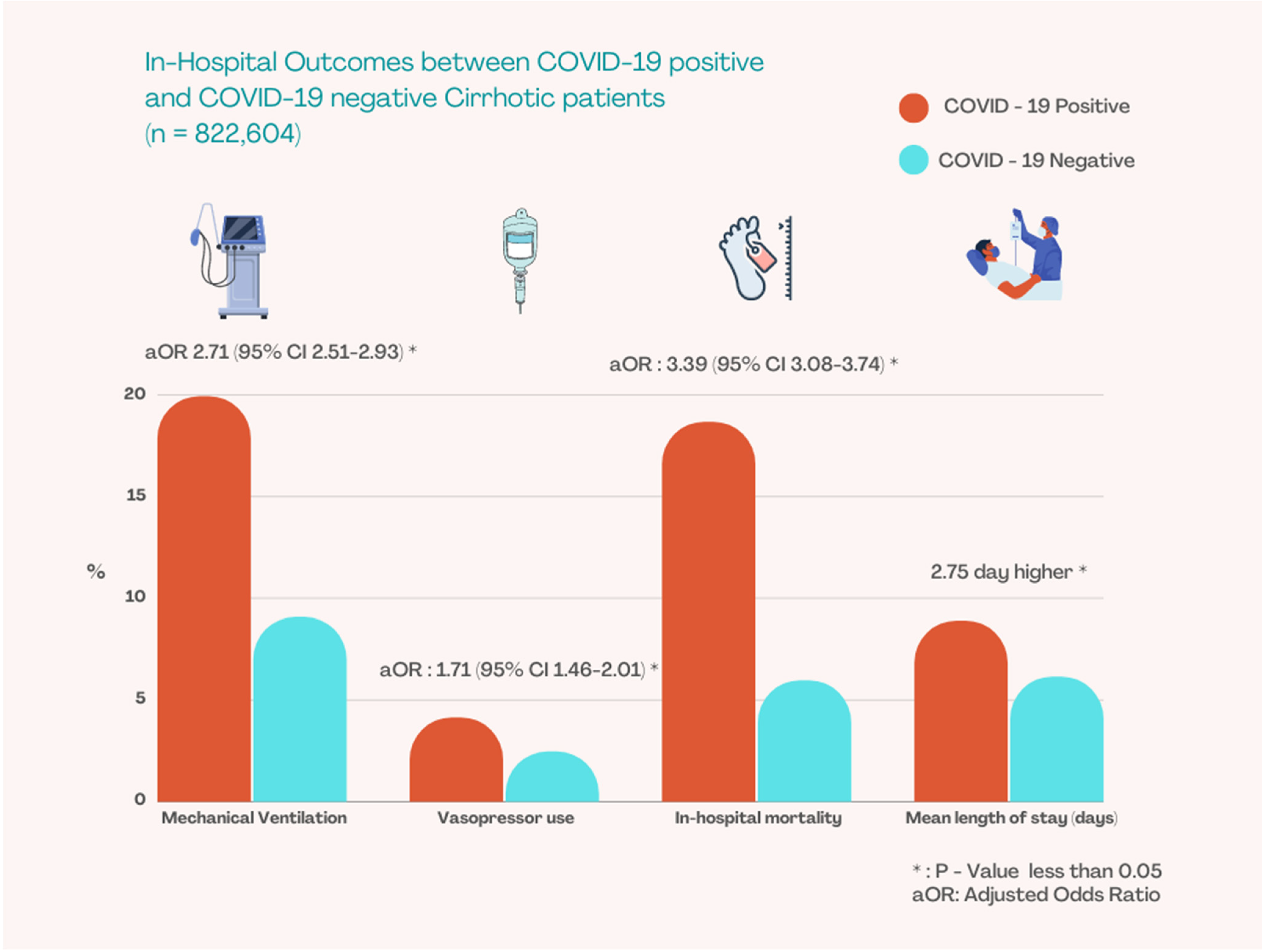
| Mechanical Ventilation | 5699 (19.92%) | 72,015 (9.07%) | |
| Adjusted odds ratio 1 2.71 (95% CI 2.51–2.93) | <0.001 | ||
| Vasopressor use | 1179 (4.12%) | 19,453 (2.45%) | |
| Adjusted odds ratio 1 1.71 (95% CI 1.46–2.01) | <0.001 | ||
| In-hospital mortality (N = 52,620) | 5339 (18.66%) | 47,322 (5.96%) | |
| Adjusted odds ratio 1 3.39 (95% CI 3.08–3.74) | <0.001 | ||
| Mean total hospitalization charge ($) | 107,915$ | 79,340$ | |
| Adjusted total charge 1 26,253$ higher | <0.001 | ||
| Mean length of stay (days) | 8.88 | 6.14 | |
| Adjusted length of stay 1 2.75 day higher | <0.001 | ||
| Variable | COVID+ Alc Cirrhosis | COVID+ Nash Cirrhosis | p Value |
|---|---|---|---|
| N = 28,610 | 9198 (32.15%) | 19,306 (67.48%) | |
| Sex (Female) | 7058 (24.67%) | 13,833 (48.35%) | <0.001 |
| Age Groups | <0.001 | ||
| ≥18–29 | 312 (1.09%) | 323 (1.13%) | |
| 30–49 | 7324 (25.6%) | 3353 (11.72%) | |
| 50–69 | 16,871 (58.97%) | 15,005 (52.45%) | |
| ≥70 | 4106 (14.35%) | 9928 (34.7%) | |
| Nacseld-ACLF Score | 0.055 | ||
| 0 | 21,086 (73.7%) | 21,475 (75.06%) | |
| 1 | 3811 (13.32%) | 4023 (14.06%) | |
| ≥2 | 3717 (12.99%) | 3110 (10.87%) | |
| Complications | |||
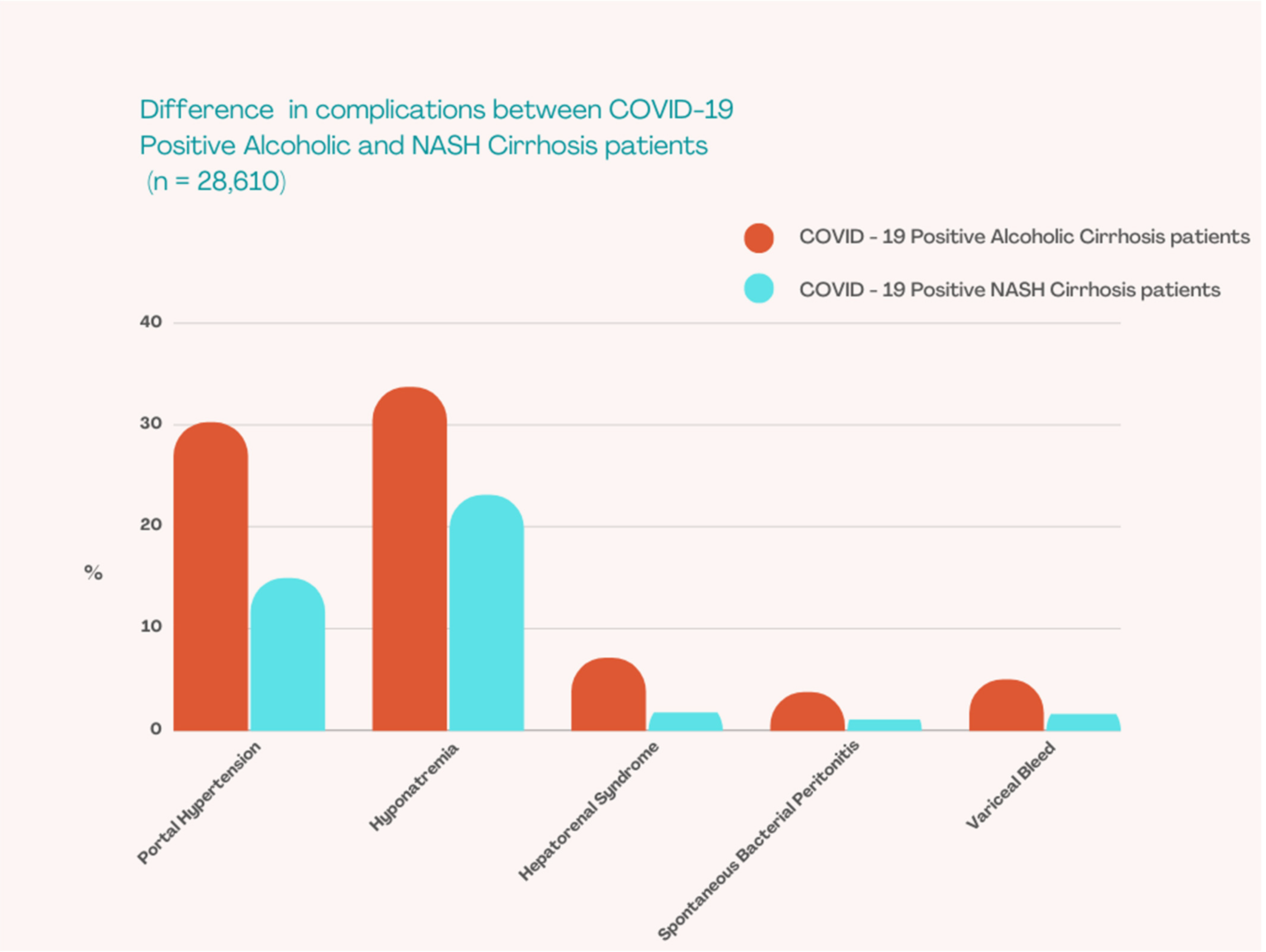
| Portal Hypertension | 8646 (30.22%) | 4283 (14.97%) | <0.001 |
| Hyponatremia | 9642 (33.7%) | 6612 (23.11%) | <0.001 |
| Hepatorenal syndrome | 2037 (7.12%) | 515 (1.8%) | <0.001 |
| Portal vein thrombosis | 684 (2.39%) | 392 (1.37%) | 0.006 |
| SBP 1 | 1073 (3.75%) | 309 (1.08%) | <0.001 |
| Variceal bleed | 1431 (5%) | 472 (1.65%) | <0.001 |
| Hepatic encephalopathy | 63 (0.22%) | 37 (0.13%) | 0.42 |
| Disposition | <0.001 | ||
| Home/Routine | 15,349 (53.65%) | 15,418 (53.89%) | |
| SNF/LTAC/Nursing home 2 | 7542 (26.36%) | 7324 (25.6%) | |
| Home health | 4401 (15.38%) | 5324 (18.61%) | |
| AMA 3 | 1319 (4.61%) | 544 (1.9%) | |
| Mechanical Ventilation | 5691 (19.89%) | 5705 (19.94%) | |
| Adjusted odds ratio 0.81 (95% CI 0.69–0.95) | 0.01 | ||
| Vasopressor use | 1167 (4.08%) | 1187 (4.15%) | |
| Adjusted odds ratio 0.83 (95% CI 0.6–1.15) | 0.26 | ||
| In-hospital mortality (N = 5335) | 5685 (19.87%) | 5176 (18.09%) | |
| Adjusted odds ratio 1.44 (95% CI 1.17–1.77) | 0.001 | ||
| Mean total hospitalization charge ($) | 114,751$ | 104,671$ | |
| Adjusted total charge 9053$ lower | 0.10 | ||
| Mean length of stay (days) | 9.31 | 8.67 | |
| Adjusted length of stay 0.28 day lower | 0.36 | ||
| Variable | HR (95% CI LL-UL) | p Value |
|---|---|---|
| Age ≥ 70 | 2.59 (1.23–5.46) | 0.01 |
| Male sex | 0.93 (0.82–1.06) | 0.33 |
| Nacseld-ACLF score | ||
| Score = 1 | 2.94 (2.45–3.53) | <0.001 |
| Score ≥ 2 | 4.79 (4.03–5.69) | <0.001 |
| Hypertension | 0.94 (0.79–1.13) | 0.56 |
| Obesity | 0.89 (0.76–1.04) | 0.15 |
| Chronic Kidney Disease | 1.14 (0.96–1.35) | 0.11 |
| Hepatorenal Syndrome | 1.30 (0.99–1.69) | 0.051 |
| Portal Hypertension | 0.79 (0.67–0.94) | 0.008 |
| Variceal bleed | 1.19 (0.86–1.65) | 0.28 |
| SBP 1 | 1.45 (1.01–2.08) | 0.04 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kapuria, D.; Gangu, K.; Chourasia, P.; Boba, A.; Nguyen, A.; Ryu, M.; Peicher, M.; Flores, M.; Chela, H.K.; Daglilar, E.S.; et al. COVID-19 Alcoholic Cirrhosis and Non-Alcoholic Steatohepatitis Cirrhosis Outcomes among Hospitalized Patients in the United States: Insight from National Inpatient Sample Database. Trop. Med. Infect. Dis. 2022, 7, 421. https://doi.org/10.3390/tropicalmed7120421
Kapuria D, Gangu K, Chourasia P, Boba A, Nguyen A, Ryu M, Peicher M, Flores M, Chela HK, Daglilar ES, et al. COVID-19 Alcoholic Cirrhosis and Non-Alcoholic Steatohepatitis Cirrhosis Outcomes among Hospitalized Patients in the United States: Insight from National Inpatient Sample Database. Tropical Medicine and Infectious Disease. 2022; 7(12):421. https://doi.org/10.3390/tropicalmed7120421
Chicago/Turabian StyleKapuria, Devika, Karthik Gangu, Prabal Chourasia, Aniesh Boba, Anthony Nguyen, Moon Ryu, Mark Peicher, Mario Flores, Harleen Kaur Chela, Ebubekir S. Daglilar, and et al. 2022. "COVID-19 Alcoholic Cirrhosis and Non-Alcoholic Steatohepatitis Cirrhosis Outcomes among Hospitalized Patients in the United States: Insight from National Inpatient Sample Database" Tropical Medicine and Infectious Disease 7, no. 12: 421. https://doi.org/10.3390/tropicalmed7120421
APA StyleKapuria, D., Gangu, K., Chourasia, P., Boba, A., Nguyen, A., Ryu, M., Peicher, M., Flores, M., Chela, H. K., Daglilar, E. S., Sheikh, A. B., & Shekhar, R. (2022). COVID-19 Alcoholic Cirrhosis and Non-Alcoholic Steatohepatitis Cirrhosis Outcomes among Hospitalized Patients in the United States: Insight from National Inpatient Sample Database. Tropical Medicine and Infectious Disease, 7(12), 421. https://doi.org/10.3390/tropicalmed7120421