
Management and Prevention of Traveler’s Diarrhea: A Cross-Sectional Study on Knowledge, Attitudes, and Practices in Italian Occupational Physicians (2019 and 2022)

 ,
, 
 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Population
- (a)
- A summary of the aims of the survey;
- (b)
- A link to the full informed consent, whose acceptance through a specific dichotomous question (yes vs. no) was mandatory for receiving;
- (c)
- The direct link to the questionnaire (Google Forms, Google LLC, Menlo Park, CA, USA);
- (d)
- A preliminary question about the respondent’s occupational settings, i.e., whether he/she was actually working as OP or not.
2.2. Questionnaire
2.2.1. Characteristics of the Participants
2.2.2. Knowledge Status
2.2.3. Risk Perception
2.2.4. Practices
2.3. Data Analysis
2.4. Ethical Considerations
3. Results
3.1. Individual Characteristics of Respondents
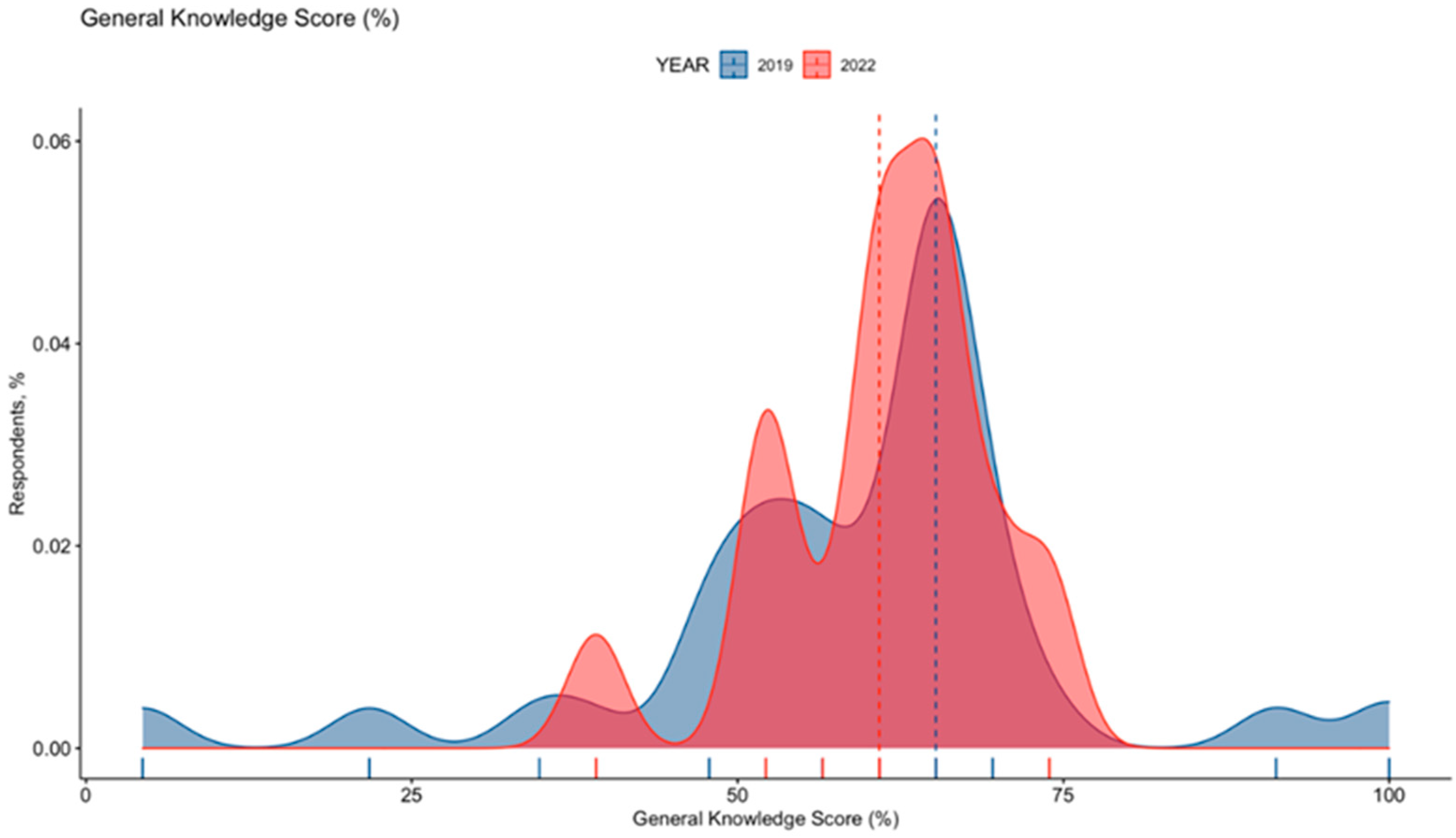
3.2. Knowledge Status
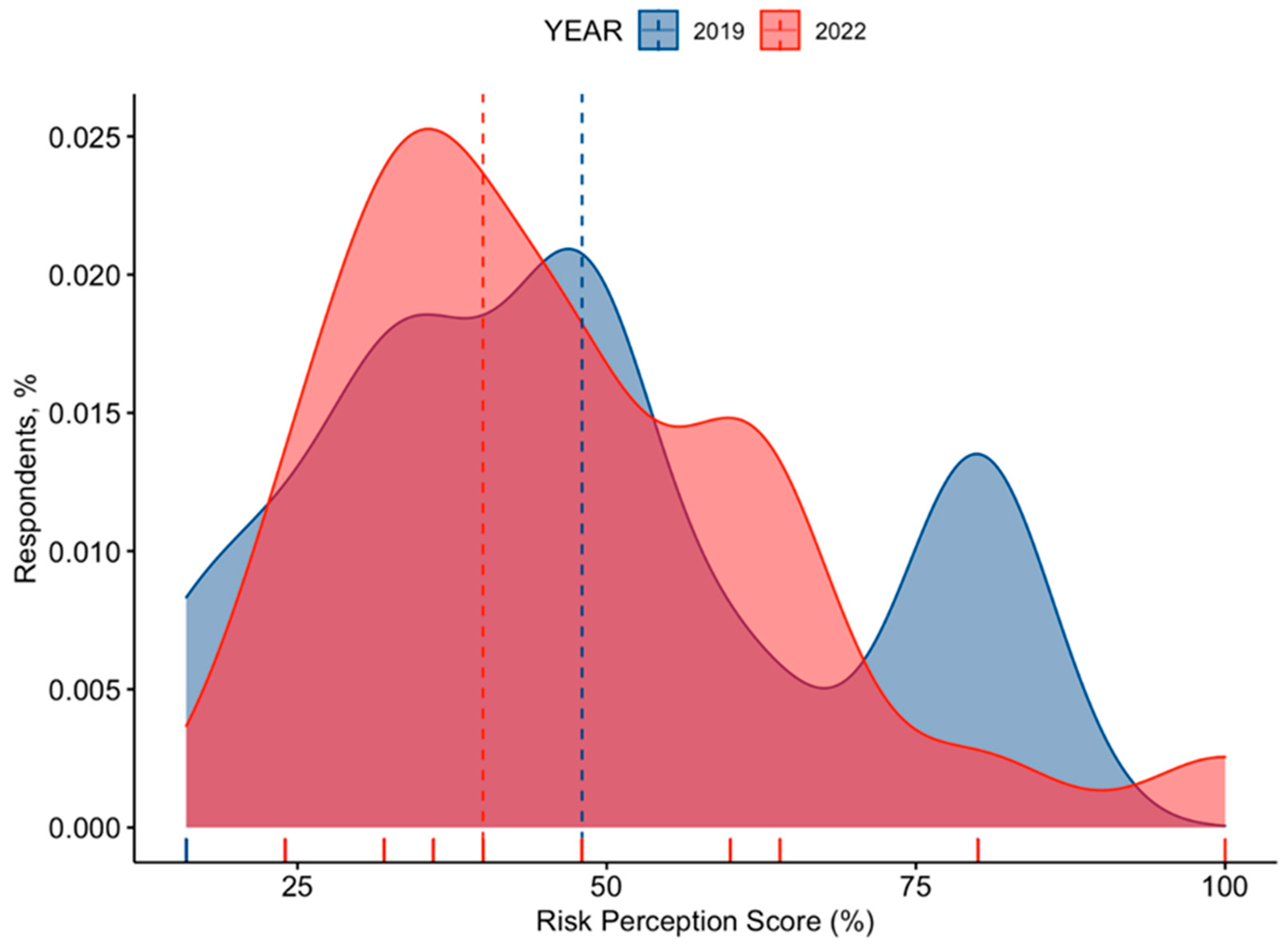
3.3. Risk Perception
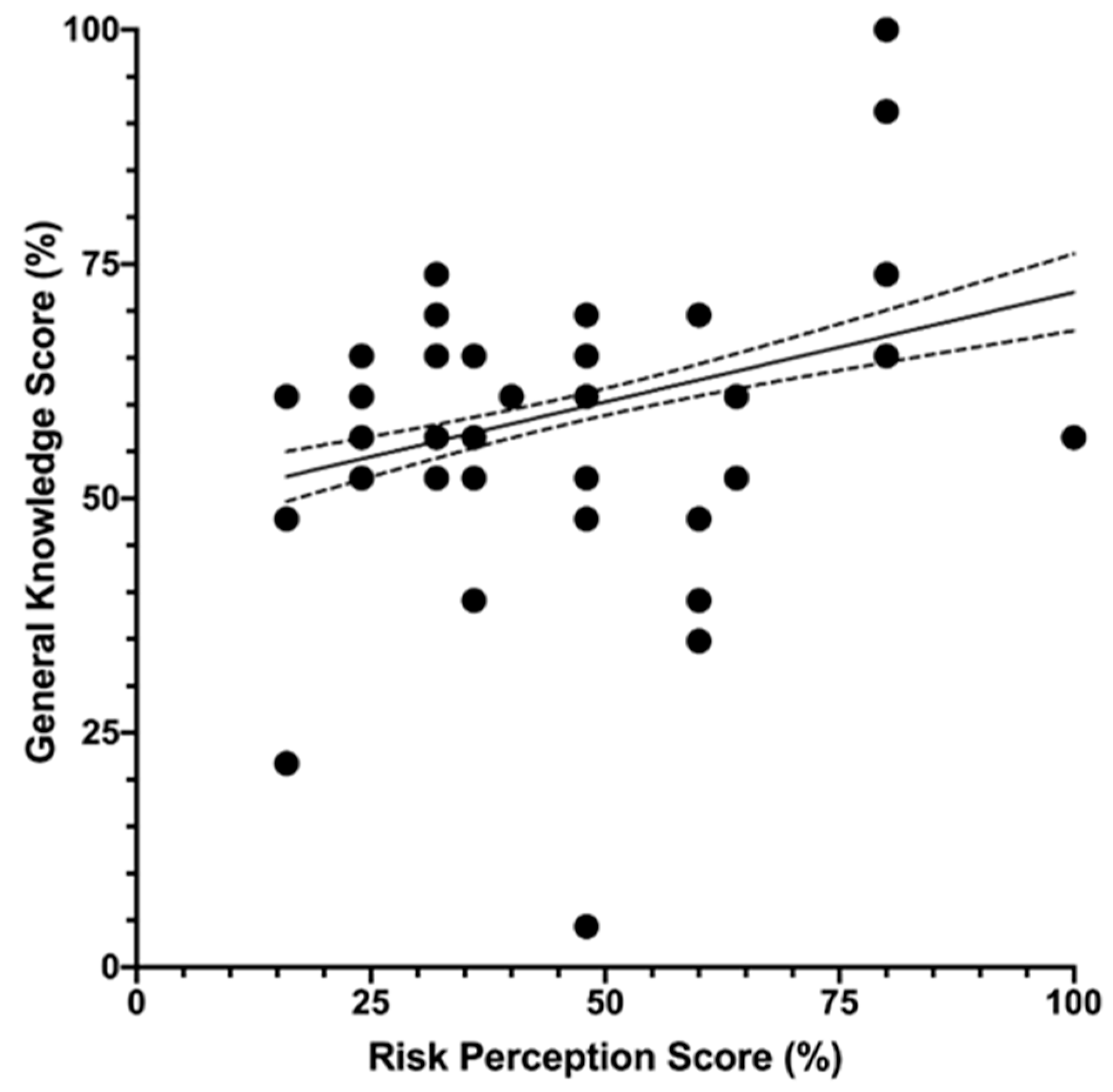
3.4. Univariate Analysis
3.5. Multivariable Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Item No | Recommendation | Page No. | |
|---|---|---|---|
| Title and Abstract | |||
| 1 | (a) Indicate the study’s design with a commonly used term in the title or the abstract | 1 | |
| (b) Provide in the abstract an informative and balanced summary of what was done and what was found | 1 | ||
| Introduction | |||
| Background/rationale | 2 | Explain the scientific background and rationale for the investigation being reported | 2,3 |
| Objectives | 3 | State specific objectives, including any prespecified hypotheses | 2,3 |
| Methods | |||
| Study design | 4 | Present key elements of study design early in the paper | 3 |
| Setting | 5 | Describe the setting, locations, and relevant dates, including periods of recruitment, exposure, follow-up, and data collection | 2–4 |
| Participants | 6 | (a) Give the eligibility criteria, and the sources and methods of selection of participants | 2 |
| Variables | 7 | Clearly define all outcomes, exposures, predictors, potential confounders, and effect modifiers. Give diagnostic criteria, if applicable | 2–4 |
| Data sources/measurement | 8 * | For each variable of interest, give sources of data and details of methods of assessment (measurement). Describe comparability of assessment methods if there is more than one group | 3,4 |
| Bias | 9 | Describe any efforts to address potential sources of bias | 3 |
| Study size | 10 | Explain how the study size was arrived at | 4 |
| Quantitative variables | 11 | Explain how quantitative variables were handled in the analyses. If applicable, describe which groupings were chosen and why | 4 |
| Statistical methods | 12 | (a) Describe all statistical methods, including those used to control for confounding | 4 |
| (b) Describe any methods used to examine subgroups and interactions | 4 | ||
| (c) Explain how missing data were addressed | 4 | ||
| (d) If applicable, describe analytical methods taking account of sampling strategy | 3 | ||
| (e) Describe any sensitivity analyses | - | ||
| Results | |||
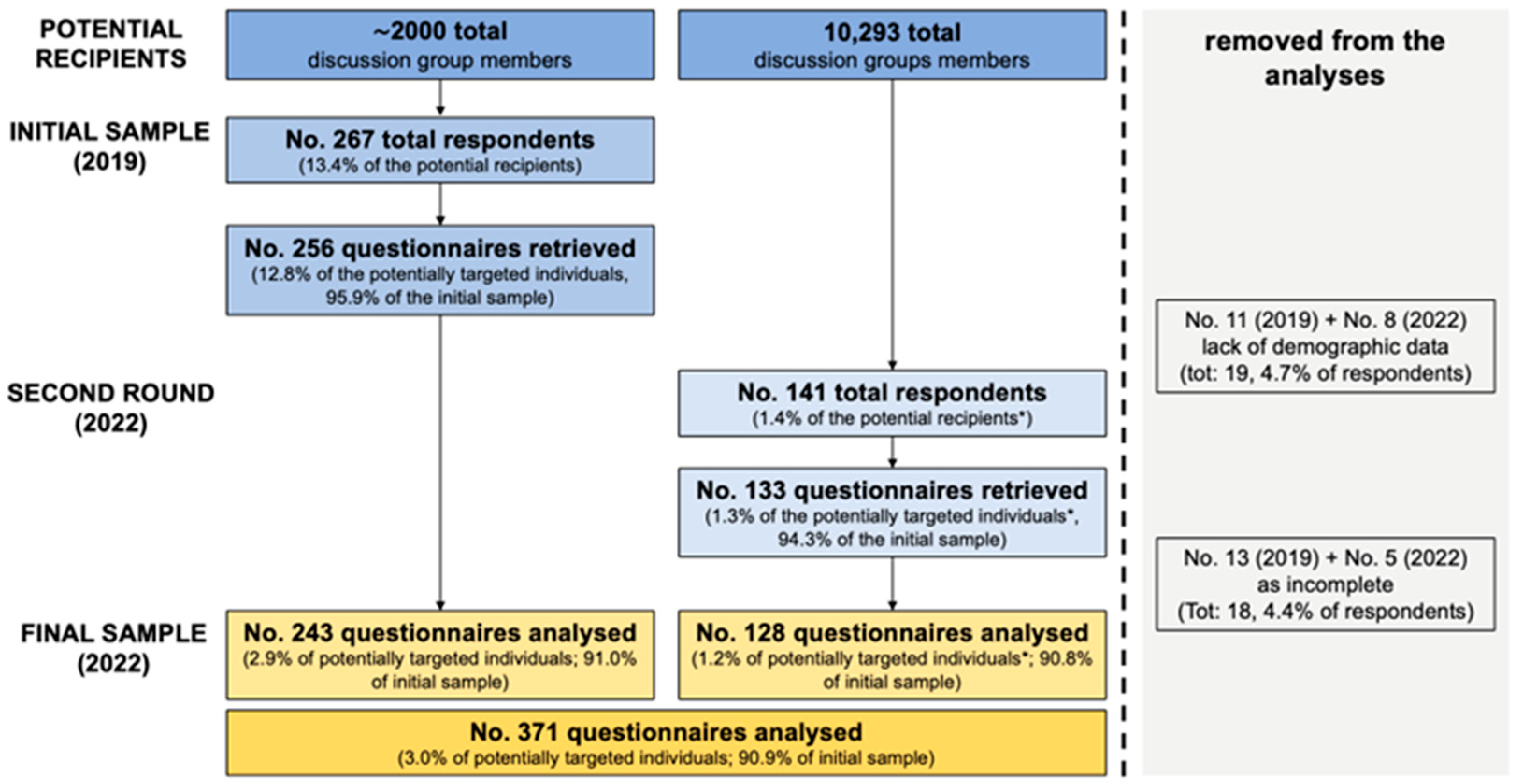
| Participants | 13 * | (a) Report numbers of individuals at each stage of study—eg numbers potentially eligible, examined for eligibility, confirmed eligible, included in the study, completing follow-up, and analysed | 5 |
| (b) Give reasons for non-participation at each stage | 5 | ||
| (c) Consider use of a flow diagram | 5 | ||
| Descriptive data | 14 * | (a) Give characteristics of study participants (e.g., demographic, clinical, social) and information on exposures and potential confounders | 6 |
| (b) Indicate number of participants with missing data for each variable of interest | 5,6 | ||
| Outcome data | 15 * | Report numbers of outcome events or summary measures | 7 |
| Main results | 16 | (a) Give unadjusted estimates and, if applicable, confounder-adjusted estimates and their precision (e.g., 95% confidence interval). Make clear which confounders were adjusted for and why they were included | 7–10 |
| (b) Report category boundaries when continuous variables were categorized | 10 | ||
| (c) If relevant, consider translating estimates of relative risk into absolute risk for a meaningful time period | - | ||
| Other analyses | 17 | Report other analyses done—e.g., analyses of subgroups and interactions, and sensitivity analyses | Annex 2,3 |
| Discussion | |||
| Key results | 18 | Summarise key results with reference to study objectives | 12 |
| Limitations | 19 | Discuss limitations of the study, taking into account sources of potential bias or imprecision. Discuss both direction and magnitude of any potential bias | 14,15 |
| Interpretation | 20 | Give a cautious overall interpretation of results considering objectives, limitations, multiplicity of analyses, results from similar studies, and other relevant evidence | 12–14 |
| Generalisability | 21 | Discuss the generalisability (external validity) of the study results | 14 |
| Other Information | |||
| Funding | 22 | Give the source of funding and the role of the funders for the present study and, if applicable, for the original study on which the present article is based | 16 |
Appendix B
Author’s Translation of the Informed Consent
- (1)
- Data controller, processor, as well as responsible for their retention during the analyses will be Dr. **********, whom you can ask about the process through his personal email (*********). Collected data are generic ones, with SOLE SCIENTIFIC AIMES that have been previously reported. Please be aware that all personal data must be shared with Criminal Law Authorities, without previous personal consent; in the cases that are specifically reported by the current legal framework, without a specific request, retrieved will not be shared with third parties.
- (2)
- After the completion of the questionnaire, we cannot identify in any way the compiler; as the questionnaire is totally anonymous by design, we cannot perform any modification, correction of data collected, and their removal as well.
- (3)
- Data will be retained only for the time strictly required for the aforementioned analyses.
- (4)
- Are you a Medical Professional licensed to practice Occupational Medicine in Italy? YES/NO
| Section 1. Your personal experience with TD… | |
|---|---|
| Have you managed any TD case in the previous 12 months? | [YES] [NO] [NO ANSWER] |
| Have you been involved in pre-travel consultations in the previous 12 months? | [YES] [NO] [NO ANSWER] |
| Have you been previously affected by TD? | [YES] [NO] [NO ANSWER] |
| Section 2. At your knowledge (please mark the correct answer) | |
| 1. Usually, travelers’ diarrhea resolves spontaneously in 3 to 5 days | [TRUE] [FALSE] [DON’T KNOW] |
| 2. Fluoroquinolones are specifically recommended for patients at high risk of medical complications | [TRUE] [FALSE] [DON’T KNOW] |
| 3. Rifaximin should be preventively employed in patients at high risk of complications | [TRUE] [FALSE] [DON’T KNOW] |
| 4. Fluoroquinolone antibiotics should be avoided as first- line option in patients affected by travelers’ diarrhea | [TRUE] [FALSE] [DON’T KNOW] |
| 5. Rifaximin may be used to treat severe, non-dysenteric travelers’ diarrhea | [TRUE] [FALSE] [DON’T KNOW] |
| 6. There is insufficient evidence to recommend the use of commercially available prebiotics or probiotics to prevent or treat travelers’ diarrhea | [TRUE] [FALSE] [DON’T KNOW] |
| 7. Anti-cholera immunization is somewhat protective for travelers’ diarrhea | [TRUE] [FALSE] [DON’T KNOW] |
| 8. Anti-rotavirus immunization is somewhat protective for travelers’ diarrhea | [TRUE] [FALSE] [DON’T KNOW] |
| 9. Treating liquids/beverages at 100°C for 1′ reduces risk of travelers’ diarrhea | [TRUE] [FALSE] [DON’T KNOW] |
| 10. Consumption of ice drinks reduces risk of travelers’ diarrhea | [TRUE] [FALSE] [DON’T KNOW] |
| 12. Most infections associated with travelers’ diarrhea are of bacterial etiology | [TRUE] [FALSE] [DON’T KNOW] |
| 13. The most frequently reported cause of watery diarrhea is… | [ ] Campylobacter spp. |
| [ ] Escherichia coli (ETEC) | |
| [ ] Amoebic infections | |
| [ ] Norwalk virus infections | |
| [ ] Shigella spp. | |
| [ ] Vibrio cholerae | |
| 14. The most frequently reported cause of dysentery is… | [ ] Campylobacter spp. |
| [ ] Escherichia coli (ETEC) | |
| [ ] Amoebic infections | |
| [ ] Norwalk virus infections | |
| [ ] Shigella spp. | |
| [ ] Vibrio cholerae | |
| 15. The most frequently reported cause of gastrointestinal syndrome characterized by diarrhea and vomiting is… | [ ] Campylobacter spp. |
| [ ] Escherichia coli (ETEC) | |
| [ ] Amoebic infections | |
| [ ] Norwalk virus infections | |
| [ ] Shigella spp. | |
| [ ] Vibrio cholerae | |
| 16. Use of loperamide and analogous is not supported by available evidence | [TRUE] [FALSE] [DON’T KNOW] |
| 17. Bismuth Subsalicylate (BSS) may be considered for any traveler to prevent travelers’ diarrhea | [TRUE] [FALSE] [DON’T KNOW] |
| 18. Fresh fruits/vegetables reduce risk of travelers’ diarrhea | [TRUE] [FALSE] [DON’T KNOW] |
| 19. Drinks on tap are associated with reduced risk of travelers’ diarrhea | [TRUE] [FALSE] [DON’T KNOW] |
| 20. A typhoid vaccine is available in Italy | [TRUE] [FALSE] [DON’T KNOW] |
| 21. Globally, incidence of travelers’ diarrhea is decreasing | [TRUE] [FALSE] [DON’T KNOW] |
| 22. The geographic area at highest risk of travelers’ diarrhea is Southern Asia | [TRUE] [FALSE] [DON’T KNOW] |
| 23. Risk of travelers’ diarrhea is usually higher in Northern Africa than in South America | [TRUE] [FALSE] [DON’T KNOW] |
| Section 3. Please rate the following items from “not significant” (1) to “very significant” (5) | |
| Ho do you perceive the frequency of TD in occupational settings? | [1] [2] [3] [4] [5] |
| Ho do you perceive the severity of TD in occupational settings? | [1] [2] [3] [4] [5] |
| Section 4. In the previous months… (Notes: 1, “never” = i.e., you did deliberately exclude the use of antimicrobial prophylaxis/treatment in all consultations; 2, “rarely” = antimicrobial prophylaxis/treatment as usually avoided, but rare exceptions are possible; 3, “sometimes” = prophylaxis/treatment is usually avoided, but selected cases may still be targeted; 4, “often” = prophylaxis/treatment is recommended in the majority of travelers, according to their clinical conditions and environmental features of the travel; 5, “always” = prophylaxis/treatment is recommended to all travelers). | |
| Have you recommended any antimicrobial prophylaxis for overseas workers? | [1] [2] [3] [4] [5] |
| Have you recommended any antimicrobial treatment for TD in overseas workers? | [1] [2] [3] [4] [5] |
| Section 5. Please provide some general information about you | |
| Year of birth: | ______________ |
| Year of medical qualification: | ______________ |
| Are you practicing as General Practitioner alongside Occupational Physician? | [Yes] [No] [No Answer] |
| Background qualification in Hygiene and Public Health? | [Yes] [No] [No Answer] |
| You identify yourself as: | [Male] [Female] [No Answer] |
| Any Previous Interaction with TD | p Value (Chi-Squared Test) | ||
|---|---|---|---|
| YES (No./249, %) | NO (No./122, %) | ||
| Individual factors | |||
| Male sex | 106, 42.6% | 55, 45.1% | 0.647 |
| Age ≥ 35 years | 183, 73.5% | 82, 67.2% | 0.208 |
| Seniority ≥ 10 years | 149, 59.8% | 57, 46.7% | 0.017 |
| Working as General Practitioner | 43, 17.3% | 7, 5.7% | 0.002 |
| Background qualification in Hygiene and Public Health | 11, 4.4% | 28, 23.0% | <0.001 |
| Participating in pre-travel consultations (in the previous 12 months) | 93, 37.3% | 5, 4.1% | <0.001 |
| General Knowledge Score > median (65.2%) | 42, 16.9% | 25, 20.5% | 0.394 |
| Recognizing TD as a frequently reported disorder | 165, 66.3% | 58, 47.5% | 0.001 |
| Recognizing TD as a severe disorder | 55, 22.1% | 67, 54.9% | <0.001 |
| Practices (often to always) | |||
| Recommends antimicrobial prophylaxis | 6, 2.4%- | 7, 5.7% | 0.101 |
| Recommends antimicrobial treatment | 0, - | 7, 5.7%% | <0.001 |
| Questionnaire collected in 2022 | 69, 27.% | 59, 48.4% | <0.001 |
| Participating in Pret-Ravel Consultations (in the Previous 12 Months) | p Value (Chi-Squared Test) | ||
|---|---|---|---|
| YES (No./98, %) | NO (No./273, %) | ||
| Individual factors | |||
| Male sex | 50, 51.0% | 111, 40.7% | 0.076 |
| Age ≥ 35 years | 73, 74.5% | 192, 70.3% | 0.434 |
| Seniority ≥ 10 years | 59, 60.2% | 147, 53.8% | 0.277 |
| Working as General Practitioner | 22, 22.4% | 28, 10.3% | 0.002 |
| Background qualification in Hygiene and Public Health | 0, - | 39, 14.3% | <0.001 |
| Professional encounters with TD | |||
| Managed at least one case of TD in the last 12 months | 78, 79.6% | 120, 44.0% | <0.001 |
| Previously affected by TD | 57, 58.2% | 77, 28.2% | <0.001 |
| General Knowledge Score > median (65.2%) | 15, 15.3% | 52, 19.0% | 0.409 |
| Recognizing TD as a frequently reported disorder | 55, 56.1% | 168, 61.5% | 0.348 |
| Recognizing TD as a severe disorder | 15, 15.3% | 107, 39.2% | <0.001 |
| Practices (often to always) | |||
| Recommends antimicrobial prophylaxis | 0, - | 13, 4.8% | 0.028 |
| Recommends antimicrobial treatment | 0, - | 7, 2.3% | 0.110 |
| Questionnaire collected in 2022 | 20, 20.4% | 108, 39.6% | 0.001 |
References
- Olson, S.; Hall, A.; Riddle, M.S.; Porter, C.K. Travelers’ Diarrhea: Update on the Incidence, Etiology and Risk in Military and Similar Populations—1990–2005 versus 2005–2015, Does a Decade Make a Difference? Trop. Dis. Travel Med. Vaccin. 2019, 5, 1. [Google Scholar] [CrossRef] [PubMed]
- Riddle, M.S.; Connor, B.A.; Beeching, N.J.; DuPont, H.L.; Hamer, D.H.; Kozarsky, P.; Libman, M.; Steffen, R.; Taylor, D.; Tribble, D.R.; et al. Guidelines for the Prevention and Treatment of Travelers’ Diarrhea: A Graded Expert Panel Report. J. Travel Med. 2017, 24, S57–S74. [Google Scholar] [CrossRef] [PubMed]
- Steffen, R.; Hill, D.R.; DuPont, H.L. Traveler’s Diarrhea a Clinical Review. JAMA-J. Am. Med. Assoc. 2015, 313, 71–80. [Google Scholar] [CrossRef]
- Butler, D.; McLoughlin, R.; Flaherty, G.T. Travel-related Gastrointestinal Diseases: Assessment and Management. Public Health Chall. 2022, 1, e30. [Google Scholar] [CrossRef]
- Barrett, J.; Brown, M. Travellers’ Diarrhoea. BMJ Open 2016, 353, i1937. [Google Scholar] [CrossRef]
- Adler, A.V.; Ciccotti, H.R.; Trivitt, S.J.H.; Watson, R.C.J.; Riddle, M.S. What’s New in Travellers’ Diarrhoea: Updates on Epidemiology, Diagnostics, Treatment and Long-Term Consequences. J. Travel Med. 2022, 29, taab099. [Google Scholar] [CrossRef] [PubMed]
- Lόpez-Vélez, R.; Lebens, M.; Bundy, L.; Barriga, J.; Steffen, R. Bacterial Travellers’ Diarrhoea: A Narrative Review of Literature Published over the Past 10 Years. Travel Med. Infect. Dis. 2022, 47, 102293. [Google Scholar] [CrossRef]
- Leder, K.; Torresi, J.; Brownstein, J.S.; Wilson, M.E.; Keystone, J.S.; Barnett, E.; Schwartz, E.; Schlagenhauf, P.; Wilder-Smith, A.; Castelli, F.; et al. Travel-Associated Illness Trends and Clusters, 2000–2010. Emerg. Infect. Dis. 2013, 19, 1049–1073. [Google Scholar] [CrossRef]
- Schlagenhauf, P.; Weld, L.; Goorhuis, A.; Gautret, P.; Weber, R.; von Sonnenburg, F.; Lopez-Vélez, R.; Jensenius, M.; Cramer, J.P.; Field, V.K.; et al. Travel-Associated Infection Presenting in Europe (2008–12): An Analysis of EuroTravNet Longitudinal, Surveillance Data, and Evaluation of the Effect of the Pre-Travel Consultation. Lancet Infect. Dis. 2015, 15, 55–64. [Google Scholar] [CrossRef]
- Leder, K.; Torresi, J.; Libman, M.D.; Cramer, J.P.; Castelli, F.; Schlagenhauf, P.; Wilder-Smith, A.; Wilson, M.E.; Keystone, J.S.; Schwartz, E.; et al. GeoSentinel Surveillance of Illness in Returned Travelers, 2007–2011. Ann. Intern. Med. 2013, 158, 456–468. [Google Scholar] [CrossRef]
- España-Cueto, S.; Salvador, F.; Oliveira, I.; Goterris, L.; Treviño, B.; Sánchez-Montalvá, A.; Serre-Delcor, N.; Sulleiro, E.; Rodríguez, V.; Aznar, M.L.; et al. Epidemiological and Clinical Profile of Adult Patients with Diarrhoea after International Travel Attended in an International Health Referral Center. Travel Med. Infect. Dis. 2022, 45, 102216. [Google Scholar] [CrossRef] [PubMed]
- Hayat, A.M.; Tribble, D.R.; Sanders, J.W.; Faix, D.J.; Shiau, D.; Armstrong, A.W.; Riddle, M.S. Knowledge, Attitudes, and Practice of Travelers’ Diarrhea Management among Frontline Providers. J. Travel Med. 2011, 18, 310–317. [Google Scholar] [CrossRef] [PubMed]
- Wendt, S.; Beier, D.; Paquet, D.; Trawinski, H.; Fuchs, A.; Lübbert, C. Medical Advice for Travelers. Dtsch. Arztebl. Int. 2021, 118, 349–356. [Google Scholar] [CrossRef] [PubMed]
- Danis, R.; Wawruch, M. Travellers’ diarrhoea—Prevention, trends and role of microbiome. Cent. Eur. J. Public Health 2022, 30, 20–25. [Google Scholar] [CrossRef]
- Peretti-Watel, P.; Seror, V.; Cortaredona, S.; Launay, O.; Raude, J.; Verger, P.; Beck, F.; Legleye, S.; L’Haridon, O.; Ward, J. A Future Vaccination Campaign against COVID-19 at Risk of Vaccine Hesitancy and Politicisation. Lancet 2020, 20, 769–770. [Google Scholar] [CrossRef]
- Verger, P.; Dubé, E. Restoring Confidence in Vaccines in the COVID-19 Era. Expert Rev. Vaccines 2020, 19, 991–993. [Google Scholar] [CrossRef]
- Verger, P.; Scronias, D.; Dauby, N.; Adedzi, K.A.; Gobert, C.; Bergeat, M.; Gagneur, A.; Dubé, E. Attitudes of Healthcare Workers towards COVID-19 Vaccination: A Survey in France and French-Speaking Parts of Belgium and Canada, 2020. Eurosurveillance 2021, 26, 2002047. [Google Scholar] [CrossRef]
- Betsch, C.; Wicker, S. Personal Attitudes and Misconceptions, Not Official Recommendations Guide Occupational Physicians’ Vaccination Decisions. Vaccine 2014, 32, 4478–4484. [Google Scholar] [CrossRef]
- Riccò, M.; Cattani, S.; Casagranda, F.; Gualerzi, G.; Signorelli, C. Knowledge, Attitudes, Beliefs and Practices of Occupational Physicians towards Vaccinations of Health Care Workers: A Cross Sectional Pilot Study in North-Eastern Italy. Int. J. Occup. Med. Environ. Health 2017, 30, 775–790. [Google Scholar] [CrossRef]
- Riccò, M.; Gualerzi, G.; Ranzieri, S.; Ferraro, P.; Bragazzi, N.L. Knowledge, Attitudes, Practices (KAP) of Italian Occupational Physicians towards Tick Borne Encephalitis. Trop. Med. Infect. Dis. 2020, 5, 117. [Google Scholar] [CrossRef]
- Hitch, G. A Review of Guidelines/Guidance from Various Countries Around the World for the Prevention and Management of Travellers’ Diarrhoea: A Pharmacist’s Perspective. Pharmacy 2019, 7, 107. [Google Scholar] [CrossRef] [PubMed]
- Falato, R.; Ricciardi, S.; Franco, G. Influenza Risk Perception and Vaccination Attitude in Medical and Nursing Students during the Vaccination Campaigns of 2007/2008 (Seasonal Influenza) and 2009/2010 (H1N1 Influenza). Med. Lav. 2011, 102, 208–215. [Google Scholar]
- La Torre, G.; Scalingi, S.; Garruto, V.; Siclari, M.; Chiarini, M.; Mannocci, A. Knowledge, Attitude and Behaviours towards Recommended Vaccinations among Healthcare Workers. Healthcare 2017, 5, 13. [Google Scholar] [CrossRef] [PubMed]
- Loulergue, P.; Moulin, F.; Vidal-Trecan, G.; Absi, Z.; Demontpion, C.; Menager, C.; Gorodetsky, M.; Gendrel, D.; Guillevin, L.; Launay, O. Knowledge, Attitudes and Vaccination Coverage of Healthcare Workers Regarding Occupational Vaccinations. Vaccine 2009, 27, 4240–4243. [Google Scholar] [CrossRef] [PubMed]
- Riccò, M.; Ferraro, P.; Peruzzi, S.; Balzarini, F.; Ranzieri, S. Mandate or Not Mandate: Knowledge, Attitudes, and Practices of Italian Occupational Physicians towards SARS-CoV-2 Immunization at the Beginning of Vaccination Campaign. Vaccines 2021, 9, 889. [Google Scholar] [CrossRef] [PubMed]
- Ricco, M.; Gualerzi, G.; Ranzieri, S. Personal Beliefs and Misconceptions, Not Evidence Guide General Practitioners in the Managing of Travelers’ Diarrhea: Results from a Pilot Study (North-Western Italy, 2019). Infect. Dis. Now 2020, 51, 266–272. [Google Scholar] [CrossRef]
- Caumes, E.; Legros, F.; Duhot, D.; Cohen, J.M.; Arnould, P.; Mosnier, A. Health Problems in Returning Travelers Consulting General Practitioners. J. Travel Med. 2008, 15, 457–459. [Google Scholar] [CrossRef][Green Version]
- McGrath, C.M.; Leder, K. Travellers’ Diarrhoea-a Survey of Practice. J. Travel Med. 2017, 24, taw085. [Google Scholar] [CrossRef]
- Riddle, M.S.; Tribble, D.R.; Jobanputra, N.K.; Jones, J.J.; Putnam, S.D.; Frenck, R.W.; Sanders, J.W. Knowledge, Attitudes, and Practices Regarding Epidemiology and Management of Travelers’ Diarrhea: A Survey of Front-Line Providers in Iraq and Afghanistan. Mil. Med. 2005, 170, 492–495. [Google Scholar] [CrossRef]
- McIntosh, I.B.; Swanson, V.; Howell, K. Health Professionals’ Attitudes toward Acute Diarrhea Management. J. Travel Med. 2006, 8, 60–065. [Google Scholar] [CrossRef][Green Version]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtsche, P.C.; Vandenbroucke, J.P. STROBE Initiative Strengthening the Reporting of Observational Studies in Epidemiology (StroBE) Statement: Guidelines for Reporting Observational Studies. BMJ 2007, 335, 806–808. [Google Scholar] [CrossRef] [PubMed]
- Riccò, M.; Vezzosi, L.; Balzarini, F.; Bragazzi, N.L. Inappropriate Risk Perception for SARS-CoV-2 Infection among Italian HCWs in the Eve of COVID-19 Pandemic. Acta Biomed. 2020, 91, e2020040. [Google Scholar] [CrossRef]
- Matteo Riccò Excess Mortality in Mountain Areas of Emilia Romagna Region during the First Months of SARS-CoV-2 Pandemic: A “Canary in the Coal Mine”? Acta Biomed. 2022, 93, e20222247. [CrossRef]
- Riccò, M.; Ferraro, P.; Peruzzi, S.; Zaniboni, A.; Satta, E.; Ranzieri, S. Excess Mortality on Italian Small Islands during the SARS-CoV-2 Pandemic: An Ecological Study. Infect. Dis. Rep. 2022, 14, 391–412. [Google Scholar] [CrossRef]
- Janz, N.K.; Becker, M.H. The Health Belief Model: A Decade Later. Health Educ. Q. 1984, 11, 1–47. [Google Scholar] [CrossRef]
- Carpenter, C.J. A Meta-Analysis of the Effectiveness of Health Belief Model Variables in Predicting Behavior. Health Commun. 2010, 25, 661–669. [Google Scholar] [CrossRef]
- Rosenstock, I.M. Historical Origins of the Health Belief Model. Health Educ. Monogr. 1974, 2, 328–335. [Google Scholar] [CrossRef]
- Zingg, A.; Siegrist, M. Measuring People’s Knowledge about Vaccination: Developing a One-Dimensional Scale. Vaccine 2012, 30, 3771–3777. [Google Scholar] [CrossRef]
- Riccò, M.; Ferraro, P.; Camisa, V.; di Palma, P.; Minutolo, G.; Ranzieri, S.; Zaffina, S.; Baldassarre, A.; Restivo, V. Managing of Migraine in the Workplaces: Knowledge, Attitudes and Practices of Italian Occupational Physicians. Medicina 2022, 58, 686. [Google Scholar] [CrossRef]
- Riccò, M.; Cattani, S.; Casagranda, F.; Gualerzi, G.; Signorelli, C. Knowledge, Attitudes, Beliefs and Practices of Occupational Physicians towards Seasonal Influenza Vaccination: A Cross-Sectional Study from North-Eastern Italy. J. Prev. Med. Hyg. 2017, 58, E141–E154. [Google Scholar]
- Yates, F.J.; Stone, E.R. The Risk Construct. In Risk-Taking Behaviour; Yates, F.J., Ed.; John Wiley & Sons: Chichester, UK, 1992; pp. 1–25. ISBN 0471922501. [Google Scholar]
- Çiftci, F.; Şen, E.; Demir, N.; Çiftci, O.; Erol, S.; Kayacan, O. Beliefs, Attitudes, and Activities of Healthcare Personnel about Influenza and Pneumococcal Vaccines. Hum. Vaccin. Immunother. 2018, 14, 111–117. [Google Scholar] [CrossRef] [PubMed]
- Riccò, M.; Ferraro, P.; Peruzzi, S.; Zaniboni, A.; Ranzieri, S. Respiratory Syncytial Virus: Knowledge, Attitudes and Beliefs of General Practitioners from North-Eastern Italy (2021). Pediatr. Rep. 2022, 14, 147–165. [Google Scholar] [CrossRef] [PubMed]
- Cronbach, L.J. Coefficient Alpha and the Internal Structure of Tests. Psychometrika 1951, 16, 297–332. [Google Scholar] [CrossRef]
- Ashbaugh, H.R.; Early, J.M.; Johnson, M.E.; Simons, M.P.; Graf, P.C.F.; Riddle, M.S.; Swierczewski, B.E. A Prospective Observational Study Describing Severity of Acquired Diarrhea among U.S. Military and Western Travelers Participating in the Global Travelers’ Diarrhea Study. Travel Med. Infect. Dis. 2021, 43, 102139. [Google Scholar] [CrossRef] [PubMed]
- Johnson, J.Y.M.; McMullen, L.M.; Hasselback, P.; Louie, M.; Saunders, L.D. Travelers’ Knowledge of Prevention and Treatment of Travelers’ Diarrhea. J. Travel Med. 2006, 13, 351–355. [Google Scholar] [CrossRef] [PubMed]
- Parment, P.A. Current Perceptions of Travelers’ Diarrhea Treatments and Vaccines. J. Travel Med. 2007, 14, 416. [Google Scholar] [CrossRef]
- Diptyanusa, A.; Ngamprasertchai, T.; Piyaphanee, W. A Review of Antibiotic Prophylaxis for Traveler’s Diarrhea: Past to Present. Trop. Dis. Travel Med. Vaccin. 2018, 4, 14. [Google Scholar] [CrossRef]
- Schweitzer, L.; Singh, B.; Rupali, P.; Libman, M. Emerging Concepts in the Diagnosis, Treatment, and Prevention of Travelers’ Diarrhea. Curr. Opin. Infect. Dis. 2019, 32, 468–474. [Google Scholar] [CrossRef]
- Abbritti, G.; Apostoli, P.; Iavicoli, S.; Murgia, N.; Persechino, B.; Soleo, L.; Ambrosi, L. Needs, Education and Accreditation in Occupational Medicine in Italy. Int. Arch. Occup. Environ. Health 2005, 78, 75–78. [Google Scholar] [CrossRef]
- Manzoli, L.; Sotgiu, G.; Magnavita, N.; Durando, P.; Barchitta, M.; Carducci, A.; Conversano, M.; de Pasquale, G.; Dini, G.; Firenze, A.; et al. Evidence-Based Approach for Continuous Improvement of Occupational Health. Epidemiol. Prev. 2015, 39, 81–85. [Google Scholar]
- Mo, P.K.H.; Lau, J.T.F. Influenza Vaccination Uptake and Associated Factors among Elderly Population in Hong Kong: The Application of the Health Belief Model. Health Educ. Res. 2015, 30, 706–718. [Google Scholar] [CrossRef] [PubMed]
- Fall, E.; Izaute, M.; Baggioni, N.C. How Can the Health Belief Model and Self-Determination Theory Predict Both Influenza Vaccination and Vaccination Intention ?A Longitudinal Study among University Students. Psychol. Health 2018, 33, 746–764. [Google Scholar] [CrossRef] [PubMed]
- Gaube, S.; Lermer, E.; Fischer, P. The Concept of Risk Perception in Health-Related Behavior Theory and Behavior Change. In Perceived Safety. Risk Engineering; Raue, M., Streicher, B., Lermer, E., Eds.; Springer: Cham, Switzerland, 2019; pp. 101–118. ISBN 9783030114565. [Google Scholar]
- Magnavita, N.; Capitanelli, I.; Garbarino, S.; la Milia, D.I.; Moscato, U.; Pira, E.; Poscia, A.; Ricciardi, W. Workplace Health Promotion Programs for Older Workers in Italy. Med. Lav. 2017, 108, 396–405. [Google Scholar] [CrossRef] [PubMed]
- Durando, P.; Dini, G.; Massa, E.; la Torre, G. Tackling Biological Risk in the Workplace: Updates and Prospects Regarding Vaccinations for Subjects at Risk of Occupational Exposure in Italy. Vaccines 2019, 7, 141. [Google Scholar] [CrossRef]
- Signorelli, C.; Riccò, M.; Odone, A. The Italian National Health Service Expenditure on Workplace Prevention and Safety (2006–2013): A National-Level Analysis. Ann. Ig 2016, 28, 313–318. [Google Scholar] [CrossRef] [PubMed]
- Khan, N.M.; Jentes, E.S.; Brown, C.; Han, P.; Rao, S.R.; Kozarsky, P.; Hagmann, S.H.F.; LaRocque, R.C.; Ryan, E.T. Pre-Travel Medical Preparation of Business and Occupational Travelers. J. Occup. Environ. Med. 2016, 58, 76–82. [Google Scholar] [CrossRef] [PubMed]
- Al-Dahshan, A.; Selim, N.; Al-Kubaisi, N.; Mahfoud, Z.; Kehyayan, V. Primary Care Physicians’ Knowledge of Travel Vaccine and Malaria Chemoprophylaxis and Associated Predictors in Qatar. PLoS ONE 2022, 17, e0265953. [Google Scholar] [CrossRef]
- Kurup, P.J.; al Abri, S.S.; Al Ajmi, F.; Khamis, H.A.; Singh, J. Knowledge, Attitude and Practice of Travel Medicine among Primary Care Physicians in Oman: The Need for Intervention. East. Mediterr. Health J. 2019, 25, 40–46. [Google Scholar] [CrossRef]
- Rovira, C.; Buffel du Vaure, C.; Partouche, H. Are French General Practitioners Consulted before Travel to Developing Countries? A Cross-Sectional Study Conducted in a French Airport. Rev. Epidemiol. Sante Publique 2015, 63, 253–258. [Google Scholar] [CrossRef]
- Kogelman, L.; Barnett, E.D.; Chen, L.H.; Quinn, E.; Yanni, E.; Wilson, M.E.; Benoit, C.; Karchmer, A.W.; Ooi, W.W.; Jentes, E.S.; et al. Knowledge, Attitudes, and Practices of US Practitioners Who Provide Pre-Travel Advice. J. Travel Med. 2014, 21, 104–114. [Google Scholar] [CrossRef][Green Version]
- Tan, E.M.; St Sauver, J.L.; Sia, I.G. Impact of Pre-Travel Consultation on Clinical Management and Outcomes of Travelers’ Diarrhea: A Retrospective Cohort Study. Trop. Dis. Travel Med. Vaccines 2018, 4, 16. [Google Scholar] [CrossRef] [PubMed]
- Wyss, M.N.; Steffen, R.; Dhupdale, N.Y.; Thitiphuree, S.; Mutsch, M. Management of Travelers’ Diarrhea by Local Physicians in Tropical and Subtropical Countries—A Questionnaire Survey. J. Travel Med. 2009, 16, 186–190. [Google Scholar] [CrossRef] [PubMed]
- Hussain, M.; Ali, M.; Ismail, M.; Soliman, M.; Muhsin, M.; Nazeer, A.; Solih, M.; Arifa, A.; Latheef, A.; Ziyan, A.; et al. Management of the First Severe Case of COVID-19 in the Small Islands of Maldives. Respir. Med. Case Rep. 2020, 30, 101118. [Google Scholar] [CrossRef]
- Pavli, A.; Maltezou, H.C. Travel Vaccines throughout History. Travel Med. Infect. Dis. 2022, 46, 102278. [Google Scholar] [CrossRef]
- Paquet, D.; Lübbert, C.; Jung, L.; Trawinski, H.; Wendt, S. Fieber Bei Reiserückkehrern. Dtsch. Arztebl. Int. 2022, 119, 400–407. [Google Scholar] [PubMed]
- Miller, N.; Saunders, I. Current Perceptions of Travelers’ Diarrhea Treatments and Vaccines: Results from a Postal Questionnaire Survey and Physician Interviews. J. Travel Med. 2007, 14, 158–167. [Google Scholar] [CrossRef][Green Version]
- Price, V.A.; Smith, R.A.S.; Douthwaite, S.; Thomas, S.; Almond, D.S.; Miller, A.R.O.; Beeching, N.J.; Thompson, G.; Ustianowski, A.; Beadsworth, M.B.J. General Physicians Do Not Take Adequate Travel Histories. J. Travel Med. 2011, 18, 271–274. [Google Scholar] [CrossRef][Green Version]
- The Medicines Utilisation Monitoring Centre. National Report on Antibiotics Use in Italy. Year 2019; Medicines Utilisation Monitoring Centre: Rome, Italy, 2020. Available online: https://www.aifa.gov.it/en/-/aifa-pubblica-il-rapporto-antibiotici-2019 (accessed on 8 November 2022).
- The Medicines Utilisation Monitoring Centre. National Report on Antibiotics Use in Italy. Year 2017; Medicines Utilisation Monitoring Centre: Rome, Italy, 2018. Available online: https://www.aifa.gov.it/documents/20142/241052/OsMed_2017_eng.pdf (accessed on 8 November 2022).
- Dall, L.B.; Lausch, K.R.; Gedebjerg, A.; Fuursted, K.; Storgaard, M.; Larsen, C.S. Do Probiotics Prevent Colonization with Multi-Resistant Enterobacteriaceae during Travel? A Randomized Controlled Trial. Travel Med. Infect. Dis. 2019, 27, 81–86. [Google Scholar] [CrossRef]
- Collinson, S.; Deans, A.; Padua-Zamora, A.; Gregorio, G.V.; Li, C.; Dans, L.F.; Allen, S.J. Probiotics for Treating Acute Infectious Diarrhoea. Cochrane Database Syst. Rev. 2020, 2020, CD003048. [Google Scholar]
- McFarland, L.V.; Goh, S. Are Probiotics and Prebiotics Effective in the Prevention of Travellers’ Diarrhea: A Systematic Review and Meta-Analysis. Travel Med. Infect. Dis. 2019, 27, 11–19. [Google Scholar] [CrossRef]
- Huang, Y.; Xu, S.; Wang, L.; Zhao, Y.; Liu, H.; Yao, D.; Xu, Y.; Lv, Q.; Hao, G.; Xu, Y.; et al. Knowledge, Attitudes, and Practices Regarding Zika: Paper and Internet—Based Survey in Zhejiang, China. JMIR Public Health Surveill. 2017, 3, e81. [Google Scholar] [CrossRef]
- Heiervang, E.; Goodman, R. Advantages and Limitations of Web-Based Surveys: Evidence from a Child Mental Health Survey. Soc. Psychiatry Epidemiol. 2011, 46, 69–76. [Google Scholar] [CrossRef]
- Bragazzi, N.L.; Riccò, M.; Pacifico, A.; Malagoli, P.; Khalaf Kridin, I.; Pigatto, P.; Damiani, G. COVID-19 Knowledge Prevents Biologics Discontinuation: Data from an Italian Multicenter Survey during RED-ZONE Declaration. Dermatol. Ther. 2020, 33, e13508. [Google Scholar] [CrossRef]
- Riccò, M.; Ferraro, P.; Camisa, V.; Satta, E.; Zaniboni, A.; Ranzieri, S.; Baldassarre, A.; Zaffina, S.; Marchesi, F. When a Neglected Tropical Disease Goes Global: Knowledge, Attitudes and Practices of Italian Physicians towards Monkeypox, Preliminary Results. Trop. Med. Infect. Dis. 2022, 7, 135. [Google Scholar] [CrossRef]
- Moßhammer, D.; Michaelis, M.; Mehne, J.; Wilm, S.; Rieger, M.A. General Practitioners’ and Occupational Health Physicians’ Views on Their Cooperation: A Cross-Sectional Postal Survey. Int. Arch. Occup. Environ. Health 2016, 89, 449–459. [Google Scholar] [CrossRef]
- Riccò, M.; Vezzosi, L.; Balzarini, F. Challenges Faced by the Italian Medical Workforce. Lancet 2020, 395, e55–e56. [Google Scholar] [CrossRef]
- Russo, F.; Pitter, G.; da Re, F.; Tonon, M.; Avossa, F.; Bellio, S.; Fedeli, U.; Gubian, L.; Monetti, D.; Saia, M.; et al. Epidemiology and Public Health Response in Early Phase of COVID-19 Pandemic, Veneto Region, Italy, 21 February to 2 April 2020. Eurosurveillance 2020, 25, 2000548. [Google Scholar] [CrossRef]
- Trumello, C.; Bramanti, S.M.; Ballarotto, G.; Candelori, C.; Cerniglia, L.; Cimino, S.; Crudele, M.; Lombardi, L.; Pignataro, S.; Viceconti, M.L.; et al. Psychological Adjustment of Healthcare Workers in Italy during the COVID-19 Pandemic: Differences in Stress, Anxiety, Depression, Burnout, Secondary Trauma, and Compassion Satisfaction between Frontline and Non-Frontline Professionals. Int. J. Environ. Res. Public Health 2020, 17, 8358. [Google Scholar] [CrossRef]




| Total Sample (No. 371) | 2019 (No. 243) | 2022 (No. 128) | p Value | |
|---|---|---|---|---|
| Age (years) (Average ± SD) | 40.8 ± 10.9 | 40.8 ± 11.8 | 40.8 ± 9.1 | 0.469 |
| 0.223 | ||||
| <35 years | 106, 28.6% | 75, 30.9% | 31, 24.2% | |
| 35–49 years | 215, 58.0% | 133, 54.7% | 82, 64.1% | |
| ≥50 years | 50, 13.4% | 35, 14.4% | 15, 11.7% | |
| Gender | 0.096 | |||
| Male | 161, 43.4% | 113, 46.5% | 48, 37.5% | |
| Female | 210, 56.6% | 130, 53.5% | 80, 62.5% | |
| Seniority (years) (Average ± SD) | 13.3 ± 11.7 | 13.2 ± 12.5 | 13.6 ± 10.1 | 0.100 |
| 0.002 | ||||
| 0–9 years | 165, 44.5% | 124, 51.0% | 41, 32.0% | |
| 10–19 years | 141, 38.0% | 84, 34.6% | 57, 44.5% | |
| ≥20 years | 65, 17.5% | 35, 14.4% | 30, 23.4% | |
| Working as General Practitioner | 50, 13.5% | 36, 14.6% | 14, 10.9% | 0.299 |
| Background qualification in Hygiene and Public Health | 39, 10.5% | 34, 14.0% | 5, 3.9% | 0.003 |
| Professional interaction with TD | ||||
| Managed at least one case of TD in the last 12 months | 198, 53.4% | 137, 56.4% | 61, 47.7% | 0.035 |
| Involved in preventive consultations in the previous 12 months | 98, 26.4% | 78, 32.1% | 20, 15.6% | <0.001 |
| Previously affected by TD | 134, 36.1% | 85, 35.0% | 49, 38.3% | 0.529 |
| General Knowledge Score (%); (Average ± SD) | 59.6 ± 14.6 | 58.9 ± 16.9 | 61.0 ± 8.5 | 0.334 |
| Recognizing TD as a frequent/highly frequent disease | 223, 60.1% | 147, 60.5% | 76, 59.4% | 0.834 |
| Recognizing TD as a severe/highly severe disease | 122, 32.9% | 76, 31.3% | 46, 36.0% | 0.364 |
| Risk Perception Score (%); (Average ± SD) | 47.1 ± 19.5 | 47.4 ± 20.4 | 46.5 ± 18.0 | 0.724 |
| Practices (often to always) | ||||
| Recommends antimicrobial prophylaxis | 13, 3.5% | 13, 5.3% | 0, - | 0.008 |
| Recommends antimicrobial treatment | 7, 1.9% | 7, 2.9% | 0, - | 0.053 |
| Correct Answer | Total (No./371, %) | 2019 (No./243, %) | 2022 (No./128, %) | p Value | |
|---|---|---|---|---|---|
| 1. Usually, travelers’ diarrhea resolves spontaneously in 3–5 days | TRUE | 313, 84.4% | 193, 79.4% | 120, 93.8% | <0.001 |
| 2. Fluoroquinolones are specifically recommended for patients at high risk of medical complications | FALSE | 136, 36.7% | 92, 37.9% | 44, 34.4% | 0.508 |
| 3. Rifaximin should be preventively employed in patients at high risk of complications | TRUE | 218, 58.8% | 139, 57.2% | 79, 61.7% | 0.401 |
| 4. Fluoroquinolone antibiotics should be avoided as first-line option in patients affected by travelers’ diarrhea | FALSE | 293, 79.0% | 186, 76.5% | 107, 83.6% | 0.113 |
| 5. Rifaximin may be used to treat severe, non-dysenteric travelers’ diarrhea | TRUE | 231, 62.3% | 152, 62.6% | 79, 61.7% | 0.875 |
| 6. There is insufficient evidence to recommend the use of commercially available prebiotics or probiotics to prevent or treat travelers’ diarrhea | TRUE | 219, 59.0% | 131, 53.9% | 88, 68.8% | 0.006 |
| 7. Anti-cholera immunization is somewhat protective for travelers’ diarrhea | TRUE | 169, 45.6% | 91, 37.4% | 78, 60.9% | <0.001 |
| 8. Anti-rotavirus immunization is somewhat protective for travelers’ diarrhea | FALSE | 130, 35.0% | 91, 37.4% | 39, 30.5% | 0.180 |
| 9. Treating liquids/beverages at 100°C for 1′ reduces risk of travelers’ diarrhea | TRUE | 313, 84.4% | 193, 79.4% | 120, 93.8% | <0.001 |
| 10. Consumption of ice drinks reduces risk of travelers’ diarrhea | FALSE | 350, 94.3% | 222, 91.4% | 128, 100% | 0.001 |
| 11. Travelers’ diarrhea affects up to 60% of wilderness travelers | TRUE | 230, 62.0% | 154, 63.4% | 76, 59.4% | 0.451 |
| 12. Most infections associated with travelers’ diarrhea are of bacterial etiology | TRUE | 222, 59.8% | 134, 55.1% | 88, 68.8% | 0.011 |
| 13. The most frequently reported cause of watery diarrhea is… | Escherichia coli | 151, 40.7% | 98, 40.3% | 53, 41.4% | 0.841 |
| 14. The most frequently reported cause of dysentery is… | Shigella spp. | 132, 35.6% | 111, 45.7% | 21, 16.4% | <0.001 |
| 15. The most frequently reported cause of gastrointestinal syndrome characterized by diarrhea and vomiting is… | Norwalk virus | 96, 25.9% | 64, 25.9% | 33, 25.8% | 0.976 |
| 16. Use of loperamide and analogous is not supported by available evidence | FALSE | 321, 62.3% | 130, 53.5% | 101, 78.9% | <0.001 |
| 17. Bismuth Subsalicylate (BSS) may be considered for any traveler to prevent travelers’ diarrhea | TRUE | 108, 29.1% | 101, 41.6% | 7, 5.5% | <0.001 |
| 18. Fresh fruits/vegetables reduce risk of travelers’ diarrhea | FALSE | 344, 92.7% | 216, 88.9% | 128, 100% | <0.001 |
| 19. Drinks on tap are associated with reduced risk of travelers’ diarrhea | FALSE | 332, 89.5% | 216, 88.9% | 116, 90.6% | 0.604 |
| 20. A typhoid vaccine is available in Italy | TRUE | 336, 90.6% | 215, 88.5% | 121, 94.5% | 0.058 |
| 21. Globally, incidence of travelers’ diarrhea is decreasing | TRUE | 101, 27.2% | 55, 22.6% | 46, 35.9% | 0.006 |
| 22. The geographic area at highest risk of travelers’ diarrhea is Southern Asia | TRUE | 249, 67.1% | 181, 74.5% | 68, 53.1% | <0.001 |
| 23. Risk of travelers’ diarrhea is usually higher in Northern Africa than in South America | FALSE | 184, 49.6% | 128, 52.7% | 56, 43.8% | 0.102 |
| Knowledge Status on Travelers Diarrhea | p Value (Chi-Squared Test) | ||
|---|---|---|---|
| High (No./67, %) | Low (No./304, %) | ||
| Individual factors | |||
| Male sex | 42, 62.7% | 119, 39.1% | <0.001 |
| Age ≥ 35 years | 53, 79.1% | 212, 69.7% | 0.124 |
| Seniority ≥ 10 years | 41, 61.2% | 165, 54.3% | 0.302 |
| Working as General Practitioner | 9, 13.4% | 41, 13.5% | 0.991 |
| Background qualification in Hygiene and Public Health | 18, 26.9% | 21, 6.9% | <0.001 |
| Professional encounters with TD | |||
| Managed at least one case of TD in the last 12 months | 42, 62.7% | 156, 51.3% | 0.091 |
| Involved in preventive consultations in the previous 12 months | 15, 22.4% | 83, 27.3% | 0.409 |
| Previously affected by TD | 20, 29.9% | 114, 37.5% | 0.238 |
| Recognizing TD as a frequently reported disorder | 60, 89.6% | 163, 53.6% | <0.001 |
| Recognizing TD as a severe disorder | 33, 49.3% | 89, 29.3% | 0.002 |
| Practices (often to always) | |||
| Recommends antimicrobial prophylaxis | 0, - | 13, 4.3% | 0.085 |
| Recommends antimicrobial treatment | 0, - | 7, 2.3% | 0.210 |
| Questionnaire collected in 2022 | 24, 35.8% | 104, 34.2% | 0.802 |
| Higher Knowledge Status | ||
|---|---|---|
| aOR | 95%CI | |
| Male gender | 3.509 | 0.807; 6.814 |
| Age ≥ 35 years | 1.058 | 0.516; 2.169 |
| Background qualification Hygiene and Public Health | 14.769 | 5.582; 39.073 |
| Previously managed TD | 3.107 | 1.484; 6.506 |
| Recognizing TD as a frequently reported disorder | 8.579 | 3.383; 21.756 |
| Recognizing TD as a severe disorder | 3.386 | 1.741; 6.585 |
| Questionnaire collected in 2022 | 1.916 | 0.931; 3.941 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Riccò, M.; Zaniboni, A.; Satta, E.; Baldassarre, A.; Cerviere, M.P.; Marchesi, F.; Peruzzi, S. Management and Prevention of Traveler’s Diarrhea: A Cross-Sectional Study on Knowledge, Attitudes, and Practices in Italian Occupational Physicians (2019 and 2022). Trop. Med. Infect. Dis. 2022, 7, 370. https://doi.org/10.3390/tropicalmed7110370
Riccò M, Zaniboni A, Satta E, Baldassarre A, Cerviere MP, Marchesi F, Peruzzi S. Management and Prevention of Traveler’s Diarrhea: A Cross-Sectional Study on Knowledge, Attitudes, and Practices in Italian Occupational Physicians (2019 and 2022). Tropical Medicine and Infectious Disease. 2022; 7(11):370. https://doi.org/10.3390/tropicalmed7110370
Chicago/Turabian StyleRiccò, Matteo, Alessandro Zaniboni, Elia Satta, Antonio Baldassarre, Milena Pia Cerviere, Federico Marchesi, and Simona Peruzzi. 2022. "Management and Prevention of Traveler’s Diarrhea: A Cross-Sectional Study on Knowledge, Attitudes, and Practices in Italian Occupational Physicians (2019 and 2022)" Tropical Medicine and Infectious Disease 7, no. 11: 370. https://doi.org/10.3390/tropicalmed7110370
APA StyleRiccò, M., Zaniboni, A., Satta, E., Baldassarre, A., Cerviere, M. P., Marchesi, F., & Peruzzi, S. (2022). Management and Prevention of Traveler’s Diarrhea: A Cross-Sectional Study on Knowledge, Attitudes, and Practices in Italian Occupational Physicians (2019 and 2022). Tropical Medicine and Infectious Disease, 7(11), 370. https://doi.org/10.3390/tropicalmed7110370