
Predictors of Death in Patients with Neonatal Sepsis in a Peruvian Hospital

 ,
,  ,
,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Environment and Research Design
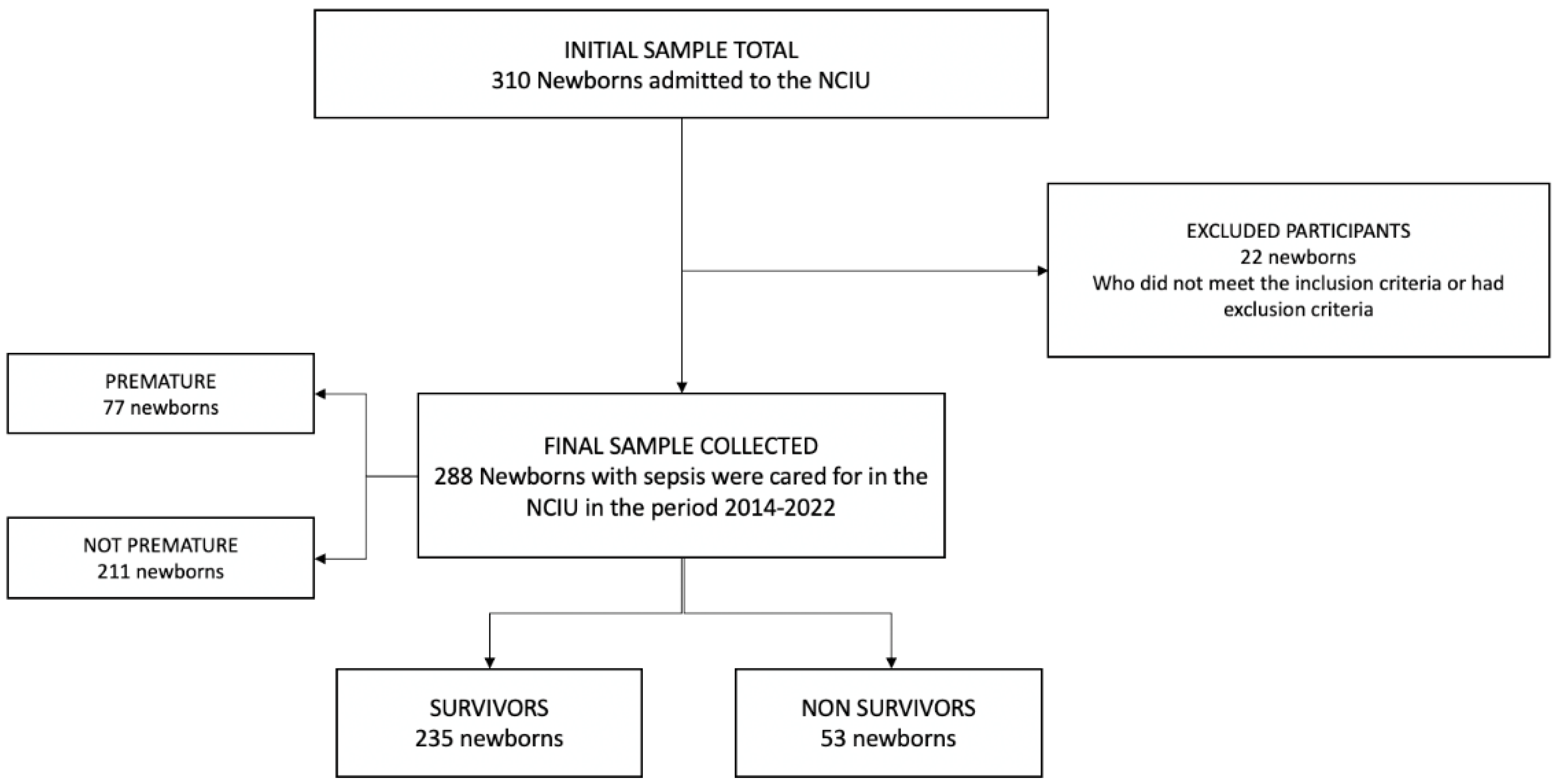
2.2. Population and Sample
2.3. Data Collection and Variable Definition
2.3.1. Outcome Variables
2.3.2. Exposure Variables
2.4. Statistic Analysis
2.5. Ethics
3. Results
3.1. Population Characteristics
3.2. Bivariate Analysis according to Mortality in the Study Population
3.3. Predictors of Mortality in Patients with Neonatal Sepsis
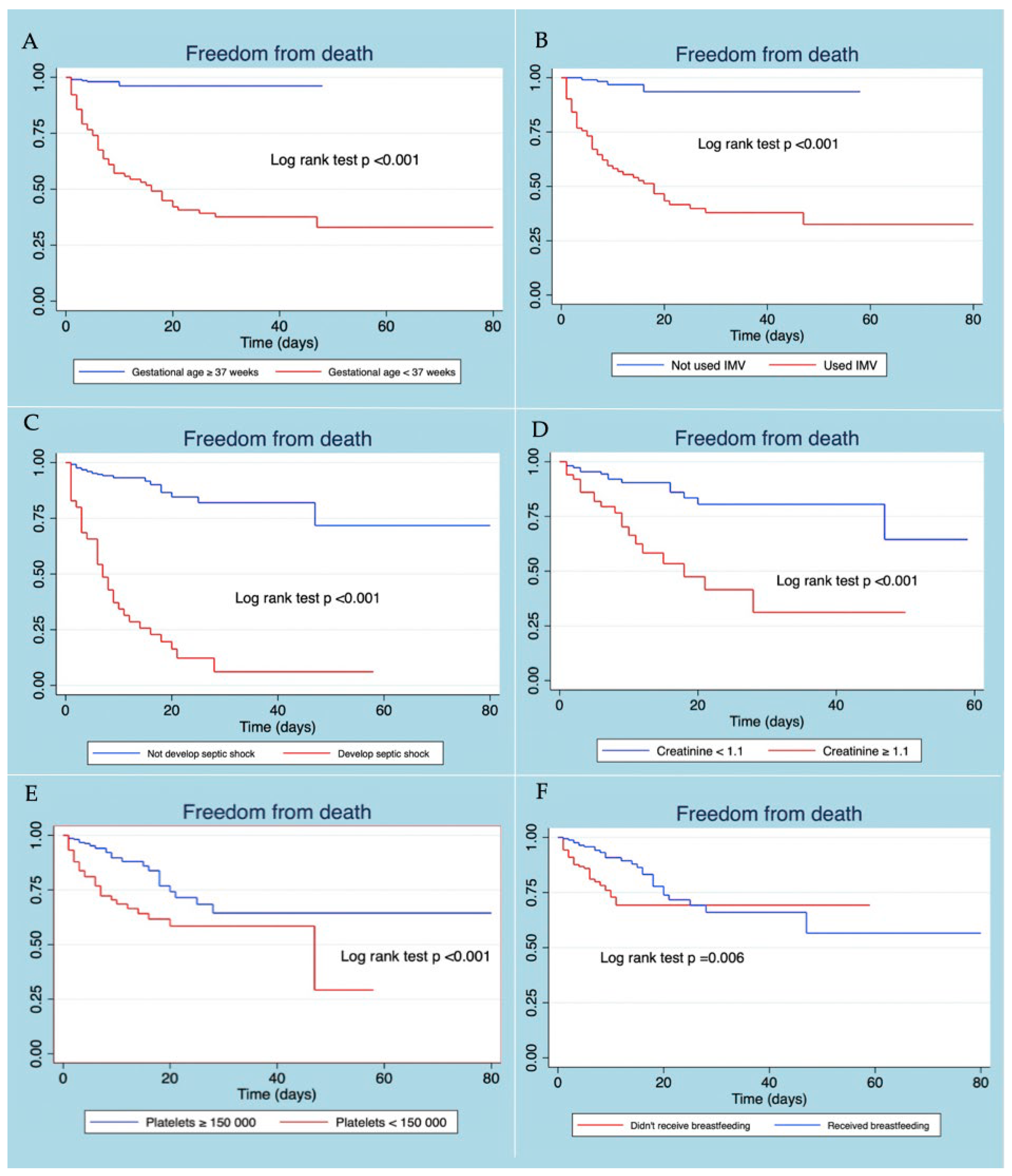
3.4. Survival Estimated by Kaplan–Meier Curve
4. Discussion
4.1. Neonatal Mortality Predictors
4.2. Implications
4.3. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- United Nations. Available online: https://www.un-ilibrary.org/content/books/9789210574662 (accessed on 25 June 2022).
- Msanga, D.R.; Parpia, F.; Konje, E.T.; Hokororo, A.; Mshana, S.E. High Mortality among Premature Neonates with Positive Blood Culture Neonatal Sepsis in a Tertiary Hospital, Tanzania: A Call for Action. Children 2021, 8, 1037. [Google Scholar] [CrossRef] [PubMed]
- Mekonnen, Y.; Tensou, B.; Telake, D.S.; Degefie, T.; Bekele, A. Neonatal mortality in Ethiopia: Trends and determinants. BMC Public Health 2013, 13, 483. [Google Scholar] [CrossRef] [PubMed]
- Rudd, K.E.; Johnson, S.C.; Agesa, K.M.; Shackelford, K.A.; Tsoi, D.; Kievlan, D.R.; Colombara, D.V.; Ikuta, K.S.; Kissoon, N.; Finfer, S.; et al. Global, regional, and national sepsis incidence and mortality, 1990–2017: Analysis for the Global Burden of Disease Study. Lancet 2020, 395, 200–211. [Google Scholar] [CrossRef]
- Shane, A.L.; Sánchez, P.J.; Stoll, B.J. Neonatal sepsis. Lancet 2017, 390, 1770–1780. [Google Scholar] [CrossRef]
- López, O.J.; Buriticá, H.M. Letalidad por sepsis neonatal, factores de riesgo y características microbiológicas [Lethality by neonatal sepsis, risk factors and microbiological characteristics]. Andes Pediatrica 2021, 92, 690–698. [Google Scholar] [CrossRef]
- Bakhuizen, S.E.; De Haan, T.R.; Teune, M.J.; Van Wassenaer-Leemhuis, A.G.; Van Der Heyden, J.L.; Van Der Ham, D.P.; Mol, B.W.J.; Wassenaer-Leemhuis, A.G. Meta-analysis shows that infants who have suffered neonatal sepsis face an increased risk of mortality and severe complications. Acta Paediatr. 2014, 103, 1211–1218. [Google Scholar] [CrossRef]
- Kabwe, M.; Tembo, J.; Chilukutu, L.; Chilufya, M.; Ngulube, F.; Lukwesa, C.; Kapasa, M.; Enne, V.; Wexner, H.; Mwananyanda, L.; et al. Etiology, Antibiotic Resistance and Risk Factors for Neonatal Sepsis in a Large Referral Center in Zambia. Pediatr. Infect. Dis. J. 2016, 35, e191–e198. [Google Scholar] [CrossRef]
- Weston, E.J.; Pondo, T.; Lewis, M.M.; Martell-Cleary, P.; Morin, C.; Jewell, B.; Daily, P.; Apostol, M.; Petit, S.; Farley, M.; et al. The Burden of Invasive Early-onset Neonatal Sepsis in the United States, 2005–2008. Pediatr. Infect. Dis. J. 2011, 30, 937–941. [Google Scholar] [CrossRef]
- Wynn, J.L.; Wong, H.R.; Shanley, T.P.; Bizzarro, M.J.; Saiman, L.; Polin, R.A. Time for a Neonatal-Specific Consensus Definition for Sepsis. Pediatr. Crit. Care Med. 2014, 15, 523–528. [Google Scholar] [CrossRef]
- El-Din, E.M.R.S.; El-Sokkary, M.M.A.; Bassiouny, M.R.; Hassan, R. Epidemiology of Neonatal Sepsis and Implicated Pathogens: A Study from Egypt. BioMed Res. Int. 2015, 2015, 509484. [Google Scholar] [CrossRef]
- Draiko, C.V.; McKague, K.; Maturu, J.D.; Joyce, S. The effect of umbilical cord cleansing with chlorhexidine gel on neonatal mortality among the community births in South Sudan: A quasi-experimental study. Pan Afr. Med. J. 2021, 38, 78. [Google Scholar] [CrossRef] [PubMed]
- Dávila, C.; Hinojosa, R.; Mendoza, E.; Gómez, W.; Espinoza, Y.; Torres, E.; Velásquez, C.; Ayque-Rosas, F.; Alvarado-Zelada, J.; Corcuera, G.; et al. Prevención, diagnóstico y tratamiento de la sepsis neonatal: Guía de práctica clínica basada en evidencias del Instituto Nacional Materno Perinatal del Perú. An. Fac. Med. 2020, 81, 354–364. [Google Scholar] [CrossRef]
- Gamarra, G.A.; Alcalá-Marcos, K.M.; Abarca-Alfaro, D.M.; Bao-Castro, V. Características microbiológicas y terapéuticas de la sepsis neonatal confirmada en un hospital de Lima, Perú. Rev. Peru. Med. Exp. Salud Pública 2016, 33, 74–82. [Google Scholar] [CrossRef][Green Version]
- Makhoul, I.R.; Sujov, P.; Smolkin, T.; Lusky, A.; Reichman, B.; In Collaboration with the Israel Neonatal Network. Epidemiological, Clinical, and Microbiological Characteristics of Late-Onset Sepsis Among Very Low Birth Weight Infants in Israel: A National Survey. Pediatrics 2002, 109, 34–39. [Google Scholar] [CrossRef]
- Adams-Chapman, I.; Stoll, B.J. Neonatal infection and long-term neurodevelopmental outcome in the preterm infant. Curr. Opin. Infect. Dis. 2006, 19, 290–297. [Google Scholar] [CrossRef]
- Stoll, B.J.; Hansen, N.I.; Adams-Chapman, I.; Fanaroff, A.A.; Hintz, S.R.; Vohr, B.; Higgins, R.D.; National Institute of Child Health and Human Development Neonatal Research Network. Neurodevelopmental and Growth Impairment Among Extremely Low-Birth-Weight Infants with Neonatal Infection. JAMA 2004, 292, 2357–2365. [Google Scholar] [CrossRef]
- Kocabaş, E.; Sarikçioğlu, A.; Aksaray, N.; Seydaoğlu, G.; Seyhun, Y.; Yaman, A. Role of procalcitonin, C-reactive protein, interleukin-6, interleukin-8 and tumor necrosis factor-alpha in the diagnosis of neonatal sepsis. Turk. J. Pediatr. 2007, 49, 7–20. [Google Scholar]
- Vazzalwar, R.; Pina-Rodrigues, E.; Puppala, B.L.; Angst, D.B.; Schweig, L. Procalcitonin as a Screening Test for Late-Onset Sepsis in Preterm Very Low Birth Weight Infants. J. Perinatol. 2005, 25, 397–402. [Google Scholar] [CrossRef]
- Panamerican Health Organization. Available online: https://www.paho.org/es/noticias/27-10-2020-intervenciones-costo-efectivas-asociaciones-estrategicas-contribuirian-salvar#:~:text=Algunas%20cifras%20que%20avalan%20que,entre%20pa%C3%ADses%20de%20la%20regi%C3%B3n (accessed on 27 June 2022).
- Vandenbroucke, J.P.; Von Elm, E.; Altman, D.G.; Gøtzsche, P.C.; Mulrow, C.D.; Pocock, S.J.; Poole, C.; Schlesselman, J.J.; Egger, M.; STROBE Initiative. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): Explanation and elaboration. Int. J. Surg. 2014, 12, 1500–1524. [Google Scholar] [CrossRef]
- Bekele, T.; Merga, H.; Tesfaye, T.; Asefa, H. Predictors of mortality among neonates hospitalized with neonatal sepsis: A case control study from southern Ethiopia. BMC Pediatr. 2022, 22, 1–9. [Google Scholar] [CrossRef]
- Rodwell, R.L.; Leslie, A.L.; Tudehope, D.I. Early diagnosis of neonatal sepsis using a hematologic scoring system. J. Pediatr. 1988, 112, 761–767. [Google Scholar] [CrossRef]
- Procianoy, R.S.; Silveira, R.D.C. The challenges of neonatal sepsis management. J. Pediatr. 2019, 96, 80–86. [Google Scholar] [CrossRef] [PubMed]
- Spanish Association of Paediatrics. Available online: https://www.aeped.es/documentos/protocolos-sociedad-cubiertas-intensivos-pediatricos (accessed on 20 July 2022).
- Viera, O.A.; Rendon, M.T.; Apaza, D.H. Resultados perinatales del recién nacido con Apgar bajo en el Hospital Hipólito Unanue de Tacna, 2002–2016. Rev. Peru. Ginecol. Obstet. 2019, 65, 21–26. [Google Scholar] [CrossRef]
- Cannizzaro, C.; Paladino, M. Fisiología y fisiopatología de la adaptación neonatal. Anest. Analg. Reanim. 2011, 24, 59–74. [Google Scholar]
- Simsek, D.G.; Ecevit, A.; Hatipoglu, N.; Coban, A.; Arisoy, A.E.; Bas, F.; Mutlu, G.Y.; Bideci, A.; Ozek, E. Neonatal Hyperglycemia, which threshold value, diagnostic approach and treatment? Turkish Neonatal and Pediatric Endocrinology and Diabetes Societies consensus report. Turk. Arch. Pediatr. 2018, 53, 234–238. [Google Scholar] [CrossRef]
- Terry, N.; Cabrera, C. Hemograma, frotis de sangre periférica, conteo de plaquetas y conteo de reticulocitos en el recién nacido normal y sus variaciones fisiológicas. MediSur 2022, 20, 129–136. [Google Scholar]
- Román, E.; Barrio, J.; San José, D.; Albañil, R. Hipertransaminasemia. Rev. Gastrohnup. 2007, 9, 19–27. [Google Scholar]
- Manroe, B.L.; Weinberg, A.G.; Rosenfeld, C.R.; Browne, R. The neonatal blood count in health and disease. I. Reference values for neutrophilic cells. J. Pediatr. 1979, 95, 89–98. [Google Scholar] [CrossRef]
- Limdi, J.K.; Hyde, G.M. Evaluation of abnormal liver function tests. Postgrad. Med. J. 2003, 79, 307–312. [Google Scholar] [CrossRef]
- Said, A.S.; Spinella, P.C.; Hartman, M.E.; Steffen, K.M.; Jackups, R.; Holubkov, R.; Wallendorf, M.; Doctor, A. RBC Distribution Width: Biomarker for red cell dysfunction and critical illness outcome? Pediatr. Crit. Care Med. 2017, 18, 134–142. [Google Scholar] [CrossRef]
- Dufour, D.R.; A Lott, J.; Nolte, F.S.; Gretch, D.R.; Koff, R.S.; Seeff, L.B. Diagnosis and Monitoring of Hepatic Injury. II. Recommendations for Use of Laboratory Tests in Screening, Diagnosis, and Monitoring. Clin. Chem. 2000, 46, 2050–2068. [Google Scholar] [CrossRef] [PubMed]
- Hughes, J.; Bardell, D. Determination of reference intervals for equine arterial blood-gas, acid-base and electrolyte analysis. Veter-Anaesth. Analg. 2019, 46, 765–771. [Google Scholar] [CrossRef] [PubMed]
- Zapata, M.; Jaimes, B. Fisiopatología, importancia y utilidad del lactato en pacientes con sepsis. Iatria 2010, 23, 278–285. [Google Scholar]
- Zevallos, J.A.C.; Jesús, C.B.O. Características de los electrolitos de pacientes adultos que acuden por emergencia médica a un hospital general de Lima, Perú. Rev. Med. Herediana 2018, 29, 158–167. [Google Scholar] [CrossRef]
- Oretga, P.J.; Sanahua, M.J.; Lucas, J.; Alvarez, O.; Zamora, I. Insuficiencia renal aguda en el periodo neonatal. In Protocolos Diagnóstico Terapeúticos de la AEP: Neonatología; Asociación Española de Pediatría: Madrid, Spain, 2008; Volume 43, pp. 411–422. [Google Scholar]
- Mitra, S.; Rennie, J. Neonatal jaundice: Aetiology, diagnosis and treatment. Br. J. Hosp. Med. 2017, 78, 699–704. [Google Scholar] [CrossRef]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.-D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef]
- ARDS Definition of Task Force; Ranieri, V.M.; Rubenfeld, G.D.; Thompson, B.T.; Ferguson, N.D.; Caldwell, E.; Fan, E.; Camporota, L.; Slutsky, A.S. Acute Respiratory Distress Syndrome: The Berlin Definition. JAMA 2012, 307, 2526–2533. [Google Scholar] [CrossRef]
- Agras, P.I.; Tarcan, A.; Baskin, E.; Cengiz, N.; Gürakan, B.; Saatci, U. Acute Renal Failure in the Neonatal Period. Ren. Fail. 2004, 26, 305–309. [Google Scholar] [CrossRef][Green Version]
- Mohamed, H.A.; Shiferaw, Z.; Roble, A.K.; Kure, M.A. Neonatal mortality and associated factors among neonates admitted to neonatal intensive care unit at public hospitals of Somali Regional State, Eastern Ethiopia: A multicenter retrospective analysis. PLoS ONE 2022, 17, e0268648. [Google Scholar] [CrossRef]
- Samuel, D.; Zinabu, D.; Alemu, B. Magnitude of neonatal mortality and associated factors among neonates at Arba Minch general Hospital. Asp. J. Pediatr. Child Health 2019, 1, 20–28. [Google Scholar]
- Osman, M.O.; Nur, A.M.; Nour, T.Y.; Hashi, M.H.; Osman, A.A. Prevalence and Causes of Neonatal Mortality Among Neonates Admitted in Neonatal Intensive Care Unit at Sultan Hassan Yabare Referral Hospital, East Ethiopia 2019. Sci. J. Clin. Med. 2020, 9, 11–17. [Google Scholar] [CrossRef]
- Ndombo, P.K.; Ekei, Q.M.; Tochie, J.N.; Temgoua, M.N.; Angong, F.T.E.; Ntock, F.N.; Mbuagbaw, L. A cohort analysis of neonatal hospital mortality rate and predictors of neonatal mortality in a sub-urban hospital of Cameroon. Ital. J. Pediatr. 2017, 43, 52. [Google Scholar] [CrossRef] [PubMed]
- Audu, L.I.; Otuneye, A.T.; Mairami, A.B.; Mukhtar-Yola, M.; Mshelia, L.J. Determination of neonatal case-specific fatality rates in a tertiary health institution in North Central Nigeria. BMC Pediatr. 2021, 21, 302. [Google Scholar] [CrossRef] [PubMed]
- Schrag, S.J.; Farley, M.M.; Petit, S.; Reingold, A.; Weston, E.J.; Pondo, T.; Jain, J.H.; Lynfield, R. Epidemiology of Invasive Early-Onset Neonatal Sepsis, 2005 to 2014. Pediatrics 2016, 138, e20162013. [Google Scholar] [CrossRef] [PubMed]
- Testoni, D.; Hayashi, M.; Cohen-Wolkowiez, M.; Benjamin, D.K., Jr.; Lopes, R.D.; Clark, R.; Smith, P.B. Late-onset Bloodstream Infections in Hospitalized Term Infants. Pediatr. Infect. Dis. J. 2014, 33, 920–923. [Google Scholar] [CrossRef]
- Parappil, H.; Rahman, S.; Salama, H.; Al Rifai, H.; Parambil, N.K.; El Ansari, W. Outcomes of 28+1 to 32+0 Weeks Gestation Babies in the State of Qatar: Finding Facility-Based Cost Effective Options for Improving the Survival of Preterm Neonates in Low Income Countries. Int. J. Environ. Res. Public Health 2010, 7, 2526–2542. [Google Scholar] [CrossRef]
- Costa, S.; Rodrigues, M.; Centeno, M.J.; Martins, A.; Vilan, A.; Brandão, O.; Guimarães, H. Diagnosis and cause of death in a neonatal intensive care unit—How important is autopsy? J. Matern. Fetal Neonatal Med. 2010, 24, 760–763. [Google Scholar] [CrossRef]
- Chow, S.; Chow, R.; Popovic, M.; Lam, M.; Popovic, M.; Merrick, J.; Margalit, R.N.S.; Lam, H.; Milakovic, M.; Chow, E.; et al. A Selected Review of the Mortality Rates of Neonatal Intensive Care Units. Front. Public Health 2015, 3, 225. [Google Scholar] [CrossRef]
- Scheer, C.; Fuchs, C.; Gründling, M.; Vollmer, M.; Bast, J.; Bohnert, J.; Zimmermann, K.; Hahnenkamp, K.; Rehberg, S.; Kuhn, S.-O. Impact of antibiotic administration on blood culture positivity at the beginning of sepsis: A prospective clinical cohort study. Clin. Microbiol. Infect. 2019, 25, 326–331. [Google Scholar] [CrossRef]
- Gonzalez, M.D.; Chao, T.; Pettengill, M.A. Modern Blood Culture: Management decisions and method options. Clin. Lab. Med. 2020, 40, 379–392. [Google Scholar] [CrossRef]
- Weitkamp, J.-H.; Aschner, J.L.; Carlo, W.A.; Bancalari, E.; Perez, J.A.; Navarrete, C.T.; Schelonka, R.L.; Walker, M.W.; Porcelli, P., Jr.; O’Shea, T.M.; et al. Meningitis, urinary tract, and bloodstream infections in very low birth weight infants enrolled in a heart rate characteristics monitoring trial. Pediatr. Res. 2020, 87, 1226–1230. [Google Scholar] [CrossRef] [PubMed]
- Tareen, Z.; Jirapradittha, J.; Sirivichayakul, C.; Chokejindachai, W. Factors Associated with Mortality Outcomes in Neonatal Septicemia in Srinagarind Hospital, Thailand. Neonatal Pediatr. Med. 2017, 3, 131. [Google Scholar] [CrossRef]
- Greco, E.; Lupia, E.; Bosco, O.; Vizio, B.; Montrucchio, G. Platelets and Multi-Organ Failure in Sepsis. Int. J. Mol. Sci. 2017, 18, 2200. [Google Scholar] [CrossRef] [PubMed]
- Weiss, S.L.; Peters, M.J.; Alhazzani, W.; Agus, M.S.D.; Flori, H.R.; Inwald, D.P.; Nadel, S.; Schlapbach, L.J.; Tasker, R.C.; Argent, A.C.; et al. Surviving sepsis campaign international guidelines for the management of septic shock and sepsis-associated organ dysfunction in children. Intensive Care Med. 2020, 46, 10–67. [Google Scholar] [CrossRef] [PubMed]
- Sozio, E.; Bertini, A.; Bertolino, G.; Sbrana, F.; Ripoli, A.; Carfagna, F.; Giacinta, A.; Viaggi, B.; Meini, S.; Ghiadoni, L.; et al. Recognition in Emergency Department of Septic Patients at Higher Risk of Death: Beware of Patients without Fever. Medicina 2021, 57, 612. [Google Scholar] [CrossRef]
- Spaggiari, V.; Passini, E.; Crestani, S.; Roversi, M.F.; Bedetti, L.; Rossi, K.; Lucaccioni, L.; Baraldi, C.; Della Casa Muttini, E.; Lugli, L.; et al. Neonatal septic shock, a focus on first line interventions. Acta Biomed. 2022, 93, e2022141. [Google Scholar] [CrossRef]
- Sankar, J.; Garg, M.; Ghimire, J.J.; Sankar, M.J.; Lodha, R.; Kabra, S.K. Delayed Administration of Antibiotics Beyond the First Hour of Recognition Is Associated with Increased Mortality Rates in Children with Sepsis/Severe Sepsis and Septic Shock. J. Pediatr. 2021, 233, 183–190.e3. [Google Scholar] [CrossRef] [PubMed]
- Thatrimontrichai, A.; Premprat, N.; Janjindamai, W.; Dissaneevate, S.; Maneenil, G. Risk Factors for 30-Day Mortality in Neonatal Gram-Negative Bacilli Sepsis. Am. J. Perinatol. 2020, 37, 689–694. [Google Scholar] [CrossRef]
- Ree, I.M.C.; Fustolo-Gunnink, S.F.; Bekker, V.; Fijnvandraat, K.J.; Steggerda, S.J.; Lopriore, E. Thrombocytopenia in neonatal sepsis: Incidence, severity and risk factors. PLoS ONE 2017, 12, e0185581. [Google Scholar] [CrossRef]
- Torres, M.D. Factores de riesgo asociados a mortalidad en sepsis neonatal en la unidad de cuidados intensivos e intermedios del Hospital Nacional Guillermo Almenara Irigoyen desde enero a noviembre del 2016. Descriptive Study. Ph.D. Thesis, Universidad Nacional de Cajamarca, Cajamarca, Peru, 2017. [Google Scholar]
- Adane, T.; Worku, M.; Tigabu, A.; Aynalem, M. Hematological Abnormalities in Culture Positive Neonatal Sepsis. Pediatr. Health Med. Ther. 2022, 13, 217–225. [Google Scholar] [CrossRef]
- Danese, E.; Montagnana, M.; Favaloro, E.J.; Lippi, G. Drug-Induced Thrombocytopenia: Mechanisms and Laboratory Diagnostics. Semin. Thromb. Hemost. 2020, 46, 264–274. [Google Scholar] [CrossRef] [PubMed]
- Thiery-Antier, N.; Binquet, C.; Vinault, S.; Meziani, F.; Boisramé-Helms, J.; Quenot, J.-P.; Epidemiology of Septic Shock Group. Is Thrombocytopenia an Early Prognostic Marker in Septic Shock? Crit. Care Med. 2016, 44, 764–772. [Google Scholar] [CrossRef]
- Youssef, D.; Abd-Elrahman, H.; Shehab, M.M.; Abd-Elrheem, M. Incidence of acute kidney injury in the neonatal intensive care unit. Saudi J. Kidney Dis. Transplant. 2015, 26, 67–72. [Google Scholar] [CrossRef] [PubMed]
- Sabzehei, M.K.; Rasuli, B.; Torabian, S.; Momtaz, H.E. The main etiologies of acute Kidney injury in the newborns hospitalized in the neonatal intensive care unit. J. Clin. Neonatol. 2014, 3, 99–102. [Google Scholar] [CrossRef] [PubMed]
- Coggins, S.A.; Laskin, B.; Harris, M.C.; Grundmeier, R.W.; Passarella, M.; McKenna, K.J.; Srinivasan, L. Acute Kidney Injury Associated with Late-Onset Neonatal Sepsis: A Matched Cohort Study. J. Pediatr. 2021, 231, 185–192.e4. [Google Scholar] [CrossRef]
- Copaja-Corzo, C.; Hueda-Zavaleta, M.; Benites-Zapata, V.A.; Rodriguez-Morales, A.J. Antibiotic use and fatal outcomes among critically Ill patients with COVID-19 in Tacna, Peru. Antibiotics 2021, 10, 959. [Google Scholar] [CrossRef]
- Coleman, C.; Perez, A.T.; Selewski, D.T.; Steflik, H.J. Neonatal Acute Kidney Injury. Front. Pediatr. 2022, 10, 842544. [Google Scholar] [CrossRef]
- Charlton, J.R.; Guillet, R. Neonatal Acute Kidney Injury: Diagnosis, Exposures, and Long-term Outcomes. NeoReviews 2018, 19, e322–e336. [Google Scholar] [CrossRef]
- Ryan, D.; Sutherland, M.; Flores, T.J.; Kent, A.L.; Dahlstrom, J.; Puelles, V.; Bertram, J.; McMahon, A.P.; Little, M.H.; Moore, L.; et al. Development of the Human Fetal Kidney from Mid to Late Gestation in Male and Female Infants. eBioMedicine 2018, 27, 275–283. [Google Scholar] [CrossRef]
- Mañalich, R.; Reyes, L.; Herrera, M.; Melendi, C.; Fundora, I. Relationship between weight at birth and the number and size of renal glomeruli in humans: A histomorphometric study. Kidney Int. 2000, 58, 770–773. [Google Scholar] [CrossRef]
- Sweetman, D.U. Neonatal acute kidney injury—Severity and recovery prediction and the role of serum and urinary biomarkers. Early Hum. Dev. 2017, 105, 57–61. [Google Scholar] [CrossRef] [PubMed]
- Plotnikov, E.Y.; Pevzner, I.B.; Zorova, L.D.; Chernikov, V.P.; Prusov, A.N.; Kireev, I.I.; Silachev, D.N.; Skulachev, V.P.; Zorov, D.B. Mitochondrial Damage and Mitochondria-Targeted Antioxidant Protection in LPS-Induced Acute Kidney Injury. Antioxidants 2019, 8, 176. [Google Scholar] [CrossRef] [PubMed]
- Spector, B.L.; Misurac, J.M. Renal Replacement Therapy in Neonates. NeoReviews 2019, 20, e697–e710. [Google Scholar] [CrossRef] [PubMed]
- Taneja, R.; Batra, P. Biomarkers as point of care tests (POCT) in neonatal sepsis: A state of science review. J. Neonatal-Perinat. Med. 2021, 14, 331–338. [Google Scholar] [CrossRef] [PubMed]
- Zhou, H.; Cui, J.; Lu, Y.; Sun, J.; Liu, J. Meta-analysis of the diagnostic value of serum, plasma and urine neutrophil gelatinase-associated lipocalin for the detection of acute kidney injury in patients with sepsis. Exp. Ther. Med. 2021, 21, 386. [Google Scholar] [CrossRef]
- Parravicini, E.; Nemerofsky, S.L.; A Michelson, K.; Huynh, T.K.; E Sise, M.; A Bateman, D.; Lorenz, J.M.; Barasch, J.M. Urinary Neutrophil Gelatinase-Associated Lipocalin Is a Promising Biomarker for Late Onset Culture-Positive Sepsis in Very Low Birth Weight Infants. Pediatr. Res. 2010, 67, 636–640. [Google Scholar] [CrossRef]
- Midan, D.; El-Gendy, F.; Elalla, D.A.; Kotb, M. Clinical assessment of neutrophil gelatinase-associated lipocalin as a potential diagnostic marker for neonatal sepsis: A prospective cohort study. Ann. Med. 2022, 54, 1725–1731. [Google Scholar] [CrossRef]
- Cai, Q.; Zhang, X.; Shen, L.; Wang, T. Clinical application value of serum neutrophil gelatinase-associated lipocalin in neonatal sepsis. Transl. Pediatr. 2022, 11, 120–126. [Google Scholar] [CrossRef]
- Cortés, J.S.; Losada, P.X.; Fernández, L.X.; Beltrán, E.; DeLaura, I.; Narváez, C.F.; Fonseca-Becerra, C.E. Interleukin-6 as a Biomarker of Early-Onset Neonatal Sepsis. Am. J. Perinatol. 2021, 38, e338–e346. [Google Scholar] [CrossRef]
- Berka, I.; Korček, P.; Straňák, Z. C-Reactive Protein, Interleukin-6, and Procalcitonin in Diagnosis of Late-Onset Bloodstream Infection in Very Preterm Infants. J. Pediatr. Infect. Dis. Soc. 2021, 10, 1004–1008. [Google Scholar] [CrossRef]
- Eichberger, J.; Resch, B. Reliability of Interleukin-6 Alone and in Combination for Diagnosis of Early Onset Neonatal Sepsis: Systematic Review. Front. Pediatr. 2022, 10, 840778. [Google Scholar] [CrossRef] [PubMed]
- Boskabadi, H.; Maamouri, G.; Tavakol Afshari, J.; Mafinejad, S.; Hosseini, G.; Mostafavi-Toroghi, H.; Saber, H.; Ghayour-Mobarhan, M.; Ferns, G. Evaluation of serum interleukins-6, 8 and 10 levels as diagnostic markers of neonatal in-fection and possibility of mortality. Iran. J. Basic Med. Sci. 2013, 16, 1232–1237. [Google Scholar] [PubMed]
- Kurul, Ş.; Simons, S.H.P.; Ramakers, C.R.B.; De Rijke, Y.B.; Kornelisse, R.F.; Reiss, I.K.M.; Taal, H.R. Association of inflammatory biomarkers with subsequent clinical course in suspected late onset sepsis in preterm neonates. Crit. Care 2021, 25, 12. [Google Scholar] [CrossRef] [PubMed]
- Ruetsch, V.; Barreault, S.; Le Sache, N.; Tissères, P. Procalcitonin is a prognosis biomarker in very preterm neonates with late onset sepsis: A pilot study. Eur. J. Pediatr. 2022, 181, 1459–1464. [Google Scholar] [CrossRef]
- Godínez-Vidal, A.R.; Alcántara-Gordillo, R.; Aguirre-Rojano, V.I.; López-Romero, S.C.; González-Calatayud, M.; González-Pérez, L.G.; Pulido-Cejudo, A.; Gracida-Mancilla, N.I. Evaluation of C-reactive protein, procalcitonin and the PCR/PCT index as indicators of mortality in abdominal sepsis. Cirugía Cir. 2020, 88, 150–153. [Google Scholar] [CrossRef]
- Adem, A.; Dache, A.; Dona, A. Determinants of neonatal mortality among newborns admitted in neonatal intensive care unit at Dilla University Referral Hospital in Gedeo Zone, Southern, Ethiopia: Unmatched case control study. BMC Pediatr. 2021, 21, 307. [Google Scholar] [CrossRef]
- Kolola, T.; Ekubay, M.; Tesfa, E.; Morka, W. Determinantes de la mortalidad neonatal en la zona de North Shoa, estado regional de Amhara, Etiopía. PLoS ONE 2016, 11, 1–11. [Google Scholar] [CrossRef]
- Bitew, Z.W.; Alemu, A.; Ayele, E.G.; Jember, D.A.; Haile, M.T.; Worku, T. Incidence Density Rate of Neonatal Mortality and Predictors in Sub-Saharan Africa: A Systematic Review and Meta-Analysis. Int. J. Pediatr. 2020, 2020, 3894026. [Google Scholar] [CrossRef]
- Torres Roldan, V.D.; Urtecho, S.M.; Gupta, J.; Yonemitsu, C.; Cárcamo, C.P.; Bode, L.; Ochoa, T.J. Human milk oligosaccharides and their association with late-onset neonatal sepsis in Peruvian very-low-birth-weight infants. Am. J. Clin. Nutr. 2020, 112, 106–112. [Google Scholar] [CrossRef]
- Dessu, S.; Habte, A.; Melis, T.; Gebremedhin, M. Survival Status and Predictors of Mortality among Newborns Admitted with Neonatal Sepsis at Public Hospitals in Ethiopia. Int. J. Pediatr. 2020, 2020, 8327028. [Google Scholar] [CrossRef]
- Bandyopadhyay, T.; Kumar, A.; Saili, A.; Randhawa, V. Distribution, antimicrobial resistance and predictors of mortality in neonatal sepsis. J. Neonatal-Perinat. Med. 2018, 11, 145–153. [Google Scholar] [CrossRef] [PubMed]
- Hanson, L.A.; Korotkova, M. The role of breastfeeding in prevention of neonatal infection. Semin. Neonatol. 2002, 7, 275–281. [Google Scholar] [CrossRef]
- Odabaşı, I.O.; Bulbul, A. Neonatal Sepsis. Med. Bull. Sisli Etfal Hosp. 2020, 54, 142–158. [Google Scholar] [CrossRef]
- Athalye-Jape, G.; Patole, S. Probiotics for preterm infants—Time to end all controversies. Microb. Biotechnol. 2019, 12, 249–253. [Google Scholar] [CrossRef] [PubMed]
- Schüller, S.S.; Kramer, B.W.; Villamor, E.; Spittler, A.; Berger, A.; Levy, O. Immunomodulation to Prevent or Treat Neonatal Sepsis: Past, Present, and Future. Front. Pediatr. 2018, 6, 199. [Google Scholar] [CrossRef]
- Santacroce, L.; Charitos, I.A.; Bottalico, L. A successful history: Probiotics and their potential as antimicrobials. Expert Rev. Anti-Infect. Ther. 2019, 17, 635–645. [Google Scholar] [CrossRef]
- Sinha, A.P.; The ProSPoNS Study Group; Gupta, S.S.; Poluru, R.; Raut, A.V.; Arora, N.K.; Pandey, R.M.; Sahu, A.R.; Bethou, A.; Sazawal, S.; et al. Evaluating the efficacy of a multistrain probiotic supplementation for prevention of neonatal sepsis in 0–2-month-old low birth weight infants in India—the “ProSPoNS” Study protocol for a phase III, multicentric, randomized, double-blind, placebo-controlled trial. Trials 2021, 22, 242. [Google Scholar] [CrossRef]
- Akker, C.H.V.D.; Van Goudoever, J.B.; Shamir, R.; Domellöf, M.; Embleton, N.D.; Hojsak, I.; Lapillonne, A.; Mihatsch, W.A.; Canani, R.B.; Bronsky, J.; et al. Probiotics and Preterm Infants: A Position Paper by the European Society for Paediatric Gastroenterology Hepatology and Nutrition Committee on Nutrition and the European Society for Paediatric Gastroenterology Hepatology and Nutrition Working Group for Probiotics and Prebiotics. J. Pediatr. Gastroenterol. Nutr. 2020, 70, 664–680. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | All Patients (n = 288) | Survivors (n = 235) | Non-Survivors (n = 53) | p-Value |
|---|---|---|---|---|
| Demographic Characteristics | ||||
| Gender | 0.689 a | |||
| - Male | 145 (50.35) | 117 (80.69) | 28 (19.35) | |
| - Woman | 143 (49.65) | 118 (82.52) | 25 (17.48) | |
| Gestational age (weeks) * | 39 (35–39) | 39 (38–40) | 30 (27–34) | <0.001 b |
| Birth weight (grams) * | 3270 (2325–3685) | 3430 (2970–3820) | 1160 (890–1890) | <0.001 b |
| Type of birth | 0.981 a | |||
| - Vaginal | 130 (45.14) | 106 (80.54) | 24 (18.46) | |
| - Cesarean section | 158 (54.86) | 129 (81.65) | 29 (18.35) | |
| Reason for cesarean section | 0.510 a | |||
| - Fetal pathology | 101 (63.92) | 84 (83.17) | 17 (16.83) | |
| - Maternal pathology | 57 (36.08) | 45 (78.95) | 12 (21.05) | |
| In-hospital birth | 0.554 a | |||
| - No | 34 (11.81) | 29 (85.29) | 5 (14.71) | |
| - Yes | 254 (88.19) | 206 (81.1) | 48 (18.9) | |
| APGAR score at 1 min * | 8 (6–9) | 9 (7–9) | 5(3–8) | <0.001 b |
| APGAR score at 5 min * | 9 (8–9) | 9 (9–9) | 7 (6–9) | <0.001 b |
| APGAR score at 10 min | 9 (7–9) | 8 (8–9) | 8 (6–8) | 0.185 b |
| Congenital disease | 0.001 a | |||
| - No | 244 (84.72) | 207 (84.84) | 37 (15.16) | |
| - Yes | 44 (15.28) | 28 (63.64) | 16 (36.36) | |
| Type of congenital disease | 0.295 c | |||
| - Fetal malformations | 27 (61.36) | 19 (70.37) | 8 (29.63) | |
| - Genetic disease | 8 (18.18) | 3 (37.50) | 5 (62.50) | |
| - Fetal infections | 8 (18.18) | 5 (62.50) | 3 (37.50) | |
| - Neonatal complication | 1 (2.27) | 1 (100) | 0 (0) | |
| Time to diagnosis sepsis (days) * | 0 (0–1) | 0 (0–1) | 0 (0) | <0.001 b |
| Hospitalized time (days) * | 7 (6–14) | 8 (6–14) | 6 (3–12) | <0.001 b |
| Time in NCIU (days) * | 7 (5–13) | 7 (5–13) | 6 (3–12) | <0.004 b |
| Classification of neonatal sepsis according to appearance | ||||
| Early sepsis | 0.706 a | |||
| - No | 65 (22.57) | 52 (80.00) | 13 (20.00) | |
| - Yes | 223 (77.43) | 183 (82.06) | 40 (17.94) | |
| Late sepsis | 0.773 c | |||
| - No | 227 (78.82) | 186 (81.94) | 41 (18.06) | |
| - Yes | 61 (21.18) | 49 (80.33) | 12 (19.67) | |
| Characteristics of NCIU management | ||||
| Use of invasive mechanical ventilation (IMV) | <0.001 a | |||
| - No | 206 (71.53) | 201 (97.57) | 5 (2.43) | |
| - Yes | 82 (28.47) | 34 (41.46) | 48 (58.54) | |
| Central venous catheter | 0.999 c | |||
| - No | 283 (98.26) | 231 (81.63) | 52 (18.37) | |
| - Yes | 5 (1.74) | 4 (80.00) | 1 (20.00) | |
| Umbilical venous catheter | <0.001 a | |||
| - No | 237 (82.29) | 217 (91.56) | 20 (8.44) | |
| - Yes | 51 (17.71) | 18 (35.29) | 33 (64.71) | |
| Umbilical artery catheter | <0.001 a | |||
| - No | 278 (96.53) | 234 (84.17) | 44 (15.83) | |
| - Yes | 10 (3.47) | 1 (10.00) | 9 (90.00) | |
| Lumbar puncture | 0.999 c | |||
| - No | 276 (95.83) | 225 (81.52) | 51 (18.48) | |
| - Yes | 12 (4.17) | 10 (83.33) | 2 (16.67) | |
| Use of Breastfeeding | 0.162 a | |||
| - No | 122 (42.36) | 95 (77.87) | 27 (22.13) | |
| - Yes | 166 (57.64) | 140 (84.34) | 26 (15.66) | |
| Use of infant formula | <0.001 a | |||
| - No | 108 (37.5) | 61 (56.48) | 47 (43.52) | |
| - Yes | 180 (62.5) | 174 (96.67) | 6 (3.33) | |
| Total parenteral nutrition | 0.184 c | |||
| - No | 287 (99.65) | 235 (81.88) | 52 (18.12) | |
| - Yes | 1 (100.00) | 0 (0) | 1 (100.00) | |
| Complications in the NCIU | ||||
| Septic shock | <0.001 a | |||
| - No | 253 (87.85) | 231 (91.30) | 22 (8.70) | |
| - Yes | 35 (12.15) | 4 (11.43) | 31 (88.57) | |
| Breathing difficulty | <0.001 a | |||
| - No | 200 (69.44) | 191 (95.5) | 9 (4.50) | |
| - Yes | 88 (30.56) | 44 (50.00) | 44 (50.00) | |
| Multiple organ failure | <0.001 a | |||
| - No | 278 (96.53) | 235 (84.53) | 43 (15.47) | |
| - Yes | 10 (3.47) | 0 (0.00) | 10 (100.00) | |
| Jaundice | 0.478 a | |||
| - No | 186 (64.58) | 154 (82.80) | 32 (17.20) | |
| - Yes | 102 (35.42) | 81 (79.41) | 21 (20.59) | |
| Respiratory distress syndrome | <0.001 a | |||
| - No | 203 (70.49) | 197 (97.04) | 6 (2.96) | |
| - Yes | 85 (29.51) | 38 (44.71) | 47 (55.29) | |
| Renal failure | 0.012 c | |||
| - No | 282 (97.92) | 233 (82.62) | 49 (17.38) | |
| - Yes | 6 (2.08) | 2 (33.33) | 4 (66.67) | |
| Seizures | 0.218 c | |||
| - No | 279 (96.88) | 229 (82.08) | 50 (17.92) | |
| - Yes | 9 (3.13) | 6 (66.67) | 3 (33.33) | |
| Vital signs | ||||
| Temperature (°C) * | 36.6 (36.4–36.9) | 36.7 (36.4–37) | 36.2 (35.1–36.6) | <0.001 b |
| Respiratory rate (Bpm) * | 55 (50–60) | 54 (48–60) | 60 (52–66) | 0.003 b |
| Heart rate (bpm) * | 136.5 (126–150) | 135 (126–146) | 146 (132–159) | 0.001 b |
| Oxygen saturation (%) * | 96 (93–98) | 96 (94–98) | 93 (87–97) | <0.001 b |
| Weight loss at diagnosis of sepsis (grams) * | 125 (70–200) | 130 (70–217.5) | 90 (30–150) | 0.023 b |
| Gain weight at diagnosis of sepsis (grams) * | 90 (40–290) | 90 (40–295) | 70 (20–100) | 0.361 b |
| Variables | All Patients (n = 288) | Survivors (n = 235) | Non-Survivors (n = 53) | p-Value |
|---|---|---|---|---|
| Blood culture | 0.796 a | |||
| - Negative | 262 (90.97) | 213 (81.30) | 49 (18.70) | |
| - Positive | 26 (9.03) | 22 (84.62) | 4 (15.38) | |
| Isolated bacteria | 0.813 b | |||
| - Klebsiella Pneumoniae (ESBL) | 16 (61.54) | 12 (75.00) | 4 (25.00) | |
| - Staphylococcus Coagulase-negative | 5 (19.23) | 5 (100.00) | 0 (0.00) | |
| - Escherichia coli (ESBL) | 3 (11.54) | 3 (100.00) | 0 (0.00) | |
| - Enterobacter cloacae | 2 (7.69) | 2 (100.00) | 0 (0.00) | |
| Leukocytes (cells/mm3) * | 17,400 (12,790–22,600) | 17,600 (13,300–22,400) | 14,380 (8200–25,000) | 0.157 b |
| Platelets (cells × 103/L) * | 200,000 (149,000–269,000) | 209,000 (164,000–272,000) | 145,000 (96,000–230,000) | <0.001 b |
| Total neutrophils (cells/mm3) * | 11,704 (7592–16,776) | 12,109 (8052–16,605) | 9310 (4488–17,250) | 0.073 b |
| Total band neutrophils (cells/mm3) * | 0 (0–318) | 0 (0–268) | 0 (0–453) | 0.253 b |
| Ratio of immature to total neutrophils (I:T) * | 0 (0–0.02) | 0 (0–0.02) | 0 (0–0.02) | 0.185 b |
| Hemoglobin (g/dL) * | 16.6 (14.3–18.9) | 16.90 (14.9–18.9) | 15.3 (12.5–18.9) | 0.019 b |
| Hematocrit (%) * | 49.75 (42.9–56) | 50 (44–56) | 47 (38.3–55.7) | 0.028 b |
| Red blood cell distribution width (%) * | 15.3 (14.6–16.2) | 15.3 (14.6–15.9) | 16.2 (14.6–16.7) | 0.550 b |
| Albumin (g/dL) * | 3.68 (2.77–4.5) | 3.75 (1.39–4.16) | 4.17 (3.16–5.52) | 0.219 b |
| Glucose (mg/dL) * | 71.9 (57.6–98.65) | 69 (57.2–88.3) | 101 (63–187) | 0.001 b |
| Lactic dehydrogenase (U/L) * | 1280 (462–1966) | 951 (462–1966) | 1468 (811.5–2705.5) | 0.685 b |
| C-reactive protein (mg/dL) * | 24.70 (14.05–57) | 24.89 (14.2–46.6) | 22 (12.5–65.6) | 0.992 b |
| Creatinine (mg/dL) * | 0.97 (0.7–1.18) | 0.91 (0.69–1.09) | 1.21 (0.96–1.4) | <0.001 b |
| AST (U/L) * | 63 (38–133) | 71.8 (37–133) | 62 (44.15–149) | 0.999 b |
| ALT (U/L) * | 17.5 (8–72) | 22.5 (12–153) | 8.5 (6–24.5) | 0.029 b |
| Cpk-Mb (U/L) * | 75.93 (25–237) | 115 (32.7–262) | 24 (12–25) | 0.054 b |
| Alkaline phosphatase (U/L)* | 254.5 (189–342) | 260.5 (213–446) | 220.5 (174–260.5) | 0.308 b |
| Lactate (mmol/L) * | 2.8 (2–4.8) | 2.76 (2–4.5) | 2.8 (2.2–6.1) | 0.789 b |
| Sodium (mmol/L) * | 136 (130–142) | 137.5 (131.8–143) | 134.5 (123.5–138) | 0.024 b |
| Potassium (mmol/L) * | 4.3 (3.76–5.01) | 4.3 (3.83–4.9) | 4.25 (3.35–5.65) | 0.908 b |
| Chlorine (mmol/L) * | 101 (96–107) | 102 (97–107) | 100.5 (95–106) | 0.271 b |
| Bicarbonate (mmol/L) * | 17.4 (13.5–20.1) | 18.65 (15.5–20.85) | 14.7 (12–17.5) | 0.006 b |
| Ph * | 7.28 (7.16–7.37) | 7.34 (7.25–7.41) | 7.19 (7.01–7.27) | <0.001 b |
| CO2 pressure (mmHg) * | 35.2 (27–47.6) | 32.8 (24.9–41.4) | 46.2 (33.1–59.5) | 0.002 b |
| O2 pressure mmHg) * | 64 (46–98) | 61 (45–98) | 64 (50.5–96.5) | 0.671 b |
| FiO2 contribution (%) * | 25 (21–50) | 21 (21–30) | 40 (30–70) | <0.001 b |
| PaFiO2 * | 214.28 (151.42–323.80) | 223.80 (171.42–432.38) | 177.32 (91.44–265.71) | 0.004 b |
| Oxacillin use | 0.999 c | |||
| - No | 264 (91.67) | 215 (81.44) | 49 (18.56) | |
| - Yes | 24 (8.33) | 20 (83.33) | 4 (16.67) | |
| Use of ampicillin | 0.999 c | |||
| - No | 17 (5.90) | 14 (82.35) | 3 (17.65) | |
| - Yes | 271 (94.10) | 221 (81.55) | 50 (18.45) | |
| Use of aminoglycosides | 0.778 c | |||
| - No | 23 (7.99) | 20 (86.96) | 3 (13.04) | |
| - Yes | 265 (92.01) | 215 (81.13) | 50 (18.87) | |
| Use of cefotaxime | 0.013 a | |||
| - No | 248 (86.11) | 208 (83.87) | 40 (16.13) | |
| - Yes | 40 (13.89) | 27 (67.50) | 13 (32.50) | |
| Use of ceftazidime | 0.744 c | |||
| - No | 273 (94.79) | 223 (81.68) | 50 (18.32) | |
| - Yes | 15 (5.21) | 12 (80.00) | 3 (20.00) | |
| Use of imipenem/meropenem | <0.001 a | |||
| - No | 223 (77.43) | 202 (90.58) | 21 (9.42) | |
| - Yes | 65 (22.57) | 33 (50.77) | 32 (49.23) | |
| Use of vancomycin | <0.001 a | |||
| - No | 217 (75.35) | 198 (91.24) | 19 (8.76) | |
| - Yes | 71 (24.65) | 37 (52.11) | 34 (47.89) | |
| Use of metronidazole | 0.040 c | |||
| - No | 280 (97.22) | 231 (82.50) | 49 (17.50) | |
| - Yes | 8 (2.78) | 4 (50.00) | 4 (50.00) | |
| Use of clindamycin | 0.316 c | |||
| - No | 282 (99.30) | 234 (83.98) | 48 (17.02) | |
| - Yes | 2 (0.70) | 1 (50.00) | 1 (50.00) | |
| Use of fluconazole | <0.001 c | |||
| - No | 274 (95.14) | 230 (83.94) | 44 (16.06) | |
| - Yes | 14 (4.86) | 5 (35.71) | 9 (64.29) | |
| Use of amphotericin B | 0.458 c | |||
| - No | 285 (98.96) | 233 (81.75) | 52 (18.25) | |
| - Yes | 3 (1.04) | 2 (66.67) | 1 (33.33) | |
| Use of vasopressors | <0.001 a | |||
| - No | 258 (89.58) | 228 (88.37) | 30 (11.63) | |
| - Yes | 30 (10.42) | 7 (23.33) | 23 (76.67) | |
| Use of corticosteroids | 0.063 c | |||
| - No | 279 (96.88) | 230 (82.44) | 49 (17.56) | |
| - Yes | 9 (3.13) | 5 (55.56) | 4 (44.44) | |
| Use of diuretics | <0.001 a | |||
| - No | 251 (87.15) | 217 (86.45) | 34 (13.55) | |
| - Yes | 37 (12.85) | 18 (48.65) | 19 (51.35) | |
| Use of bovine pulmonary surfactant | <0.001 a | |||
| - No | 244 (84.72) | 218 (89.34) | 26 (10.66) | |
| - Yes | 44 (15.28) | 17 (38.64) | 27 (61.36) | |
| Use of phototherapy | <0.001 a | |||
| - No | 182 (63.19) | 162 (89.01) | 20 (10.99) | |
| - Yes | 106 (36.81) | 73 (68.87) | 33 (31.13) | |
| Blood transfusion | <0.001 c | |||
| - No | 264 (91.67) | 226 (85.61) | 38 (14.39) | |
| - Yes | 24 (8.33) | 9 (37.50) | 15 (62.50) | |
| Use of anticonvulsants | 0.011 c | |||
| - No | 269 (93.40) | 224 (83.77) | 45 (16.73) | |
| - Yes | 19 (6.60) | 11 (57.89) | 8 (42.11) | |
| Use of antipyretics | 0.999 c | |||
| - No | 283 (98.26) | 231 (81.63) | 52 (18.37) | |
| - Yes | 5 (1.74) | 4 (80.00) | 1 (20.00) |
| Variable | cHR (95% CI) | p-Value | aHR (95% CI) | p-Value |
|---|---|---|---|---|
| Gestational age | ||||
| - Term newborn (>37) | Ref | Ref | ||
| - Preterm newborn (<37) | 19.95 (7.85–50.69) | <0.001 | 13.92 (1.71–113.51) | 0.014 |
| Leukocytes (cells/mm3) | ||||
| - Normal (<12,000) | Ref | Ref | ||
| - Leukocytosis (>12,000) | 0.39 (0.22–0.67) | 0.001 | 0.58 (0.21–1.60) | 0.298 |
| Platelets (cells × 103/L) | ||||
| - Normal (>150,000) | Ref | Ref | ||
| - Low count (<150,000) | 2.53 (1.47–4.37) | 0.001 | 3.64 (1.22–10.88) | 0.021 |
| Ratio of immature to total neutrophils (I:T) | ||||
| - Normal (<0.12) | Ref | Ref | ||
| - High count (≥0.12) | 6.86 (2.12–22.16) | 0.001 | 2.74 (0.28–26.46) | 0.382 |
| Glucose (mg/dL) | ||||
| - Normal (<150) | Ref | Ref | ||
| - High count (≥150) | 4.01 (2.17–7.42) | <0.001 | 0.60 (0.18–2.03) | 0.411 |
| Creatinine (mg/dL) | ||||
| - Normal (<1.1) | Ref | Ref | ||
| - High count (≥1.1) | 3.86 (1.94–7.68) | <0.001 | 3.03 (1.09–8.45) | 0.034 |
| pH | ||||
| - Normal (≥7.35) | Ref | Ref | ||
| - Low count (<7.35) | 3.24 (1.13–9.26) | 0.028 | 2.36 (0.44–12.61) | 0.315 |
| CO2 pressure (mmHg) | ||||
| - Normal (<45) | Ref | Ref | ||
| - High count (≥45) | 2.11 (1.05–4.24) | 0.035 | 0.99 (0.34–2.90) | 0.985 |
| PaO2/FiO2 | ||||
| - Normal ≥400 | Ref | Ref | ||
| - ARDS <400 | 9.86 (1.34–72.60) | 0.025 | 2.83 (0.32–25.29) | 0.352 |
| Variable | cHR (95% CI) | p-Value | aHR (95% CI) | p-Value |
|---|---|---|---|---|
| Birth weight | ||||
| - Normal (≥2500 g) | Ref | Ref | ||
| - Low birth weight (<2500 g) | 15.37 (6.49–36.37) | <0.001 | 2.94 (1.04–8.30) | 0.042 |
| APGAR score at 1 min | ||||
| - Normal | Ref | Ref | ||
| - Moderate | 4.45 (2.33–8.47) | <0.001 | 0.78 (0.37–1.63) | 0.505 |
| - Low | 3.47 (1.72–6.99) | <0.001 | 0.50 (0.18–1.42) | 0.191 |
| APGAR score at 5 min | ||||
| - Normal | Ref | Ref | ||
| - Moderate | 3.30 (1.85–5.87) | <0.001 | 3.21 (1.37–7.56) | 0.007 |
| - Low | 1.89 (0.25–14.09) | 0.533 | 0.39 (0.04–3.46) | 0.401 |
| Septic Shock | ||||
| - No | Ref | Ref | ||
| - Yes | 11.47 (6.63–19.85) | <0.001 | 4.41 (2.23–8.74) | <0.001 |
| ARDS | ||||
| - No | Ref | Ref | ||
| - Yes | 14.40 (6.09–34.03) | <0.001 | 1.64 (0.52–5.21) | 0.400 |
| Use of IMV | ||||
| - No | Ref | Ref | ||
| - Yes | 19.22 (7.58–48.74) | <0.001 | 5.61 (1.86–16.88) | 0.002 |
| Use of CVC | ||||
| - No | Ref | Ref | ||
| - Yes | 0.41 (0.08–4.30) | 0.604 | 1.03 (0.11–9.52) | 0.979 |
| Use of exclusive breastfeeding | ||||
| - No | Ref | Ref | ||
| - Yes | 0.47 (0.27–0.82) | 0.008 | 0.25 (0.13–0.48) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vizcarra-Jiménez, D.; Copaja-Corzo, C.; Hueda-Zavaleta, M.; Parihuana-Travezaño, E.G.; Gutierrez-Flores, M.; Rivarola-Hidalgo, M.; Benites-Zapata, V.A. Predictors of Death in Patients with Neonatal Sepsis in a Peruvian Hospital. Trop. Med. Infect. Dis. 2022, 7, 342. https://doi.org/10.3390/tropicalmed7110342
Vizcarra-Jiménez D, Copaja-Corzo C, Hueda-Zavaleta M, Parihuana-Travezaño EG, Gutierrez-Flores M, Rivarola-Hidalgo M, Benites-Zapata VA. Predictors of Death in Patients with Neonatal Sepsis in a Peruvian Hospital. Tropical Medicine and Infectious Disease. 2022; 7(11):342. https://doi.org/10.3390/tropicalmed7110342
Chicago/Turabian StyleVizcarra-Jiménez, Dariela, Cesar Copaja-Corzo, Miguel Hueda-Zavaleta, Edgar G. Parihuana-Travezaño, Maykel Gutierrez-Flores, Marco Rivarola-Hidalgo, and Vicente A. Benites-Zapata. 2022. "Predictors of Death in Patients with Neonatal Sepsis in a Peruvian Hospital" Tropical Medicine and Infectious Disease 7, no. 11: 342. https://doi.org/10.3390/tropicalmed7110342
APA StyleVizcarra-Jiménez, D., Copaja-Corzo, C., Hueda-Zavaleta, M., Parihuana-Travezaño, E. G., Gutierrez-Flores, M., Rivarola-Hidalgo, M., & Benites-Zapata, V. A. (2022). Predictors of Death in Patients with Neonatal Sepsis in a Peruvian Hospital. Tropical Medicine and Infectious Disease, 7(11), 342. https://doi.org/10.3390/tropicalmed7110342