
Nodding Syndrome: A Scoping Review

Abstract
1. Introduction
2. Methods
2.1. Inclusion and Exclusion Criteria
2.2. Systematic Identification of Relevant Studies
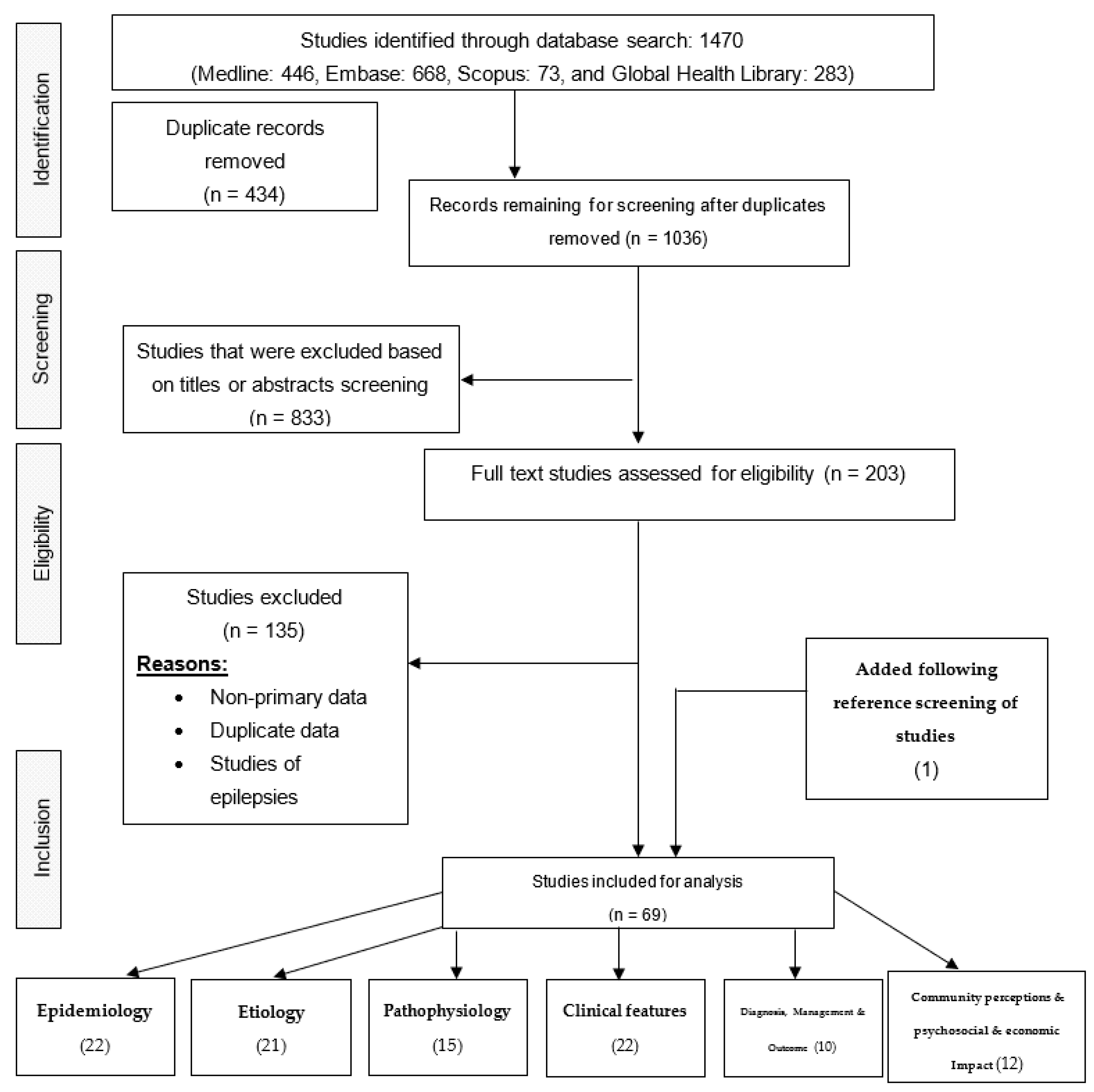
2.3. Selection of Relevant Studies, Data Extraction, and Reporting of Results
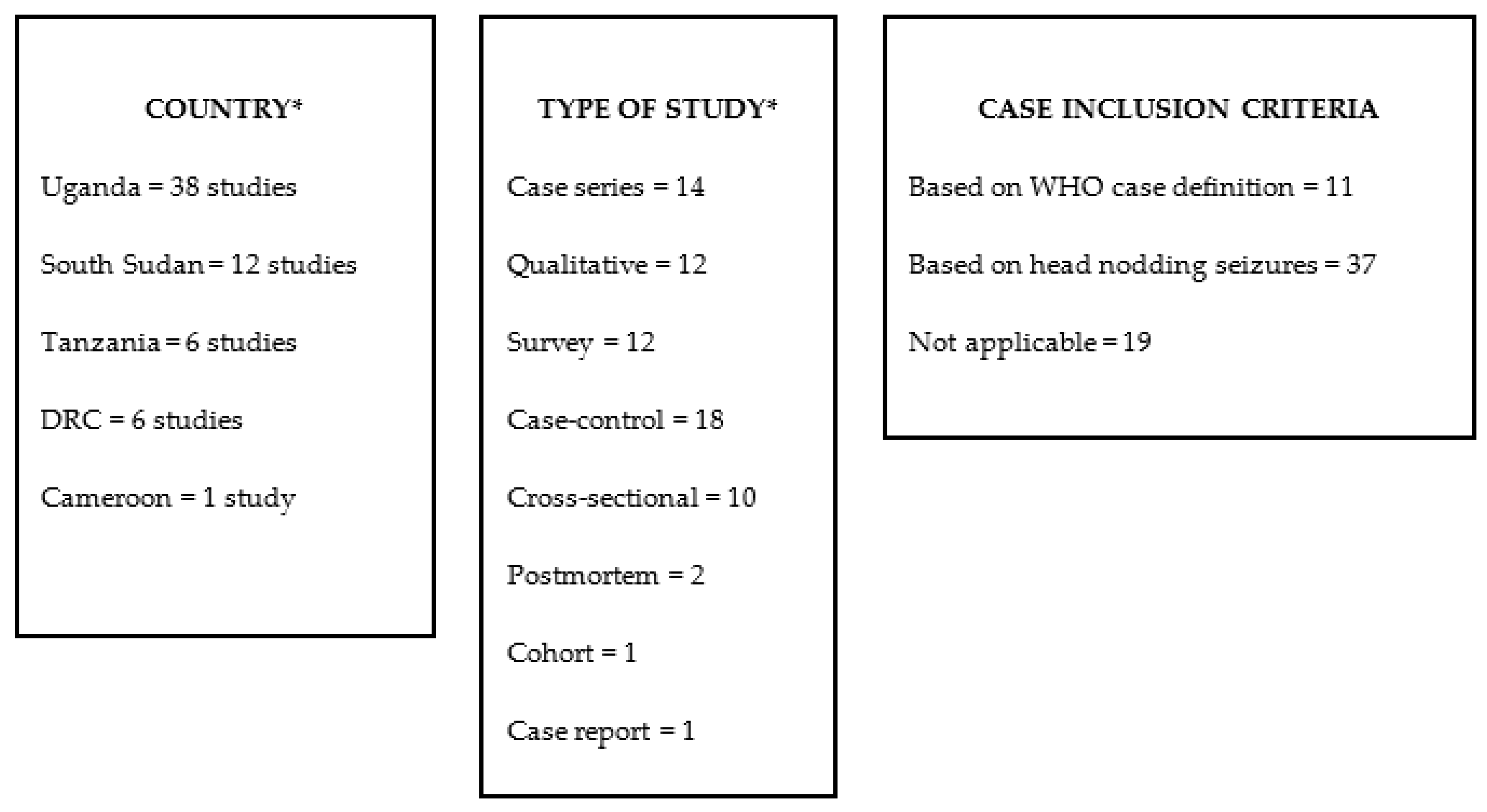
3. Results
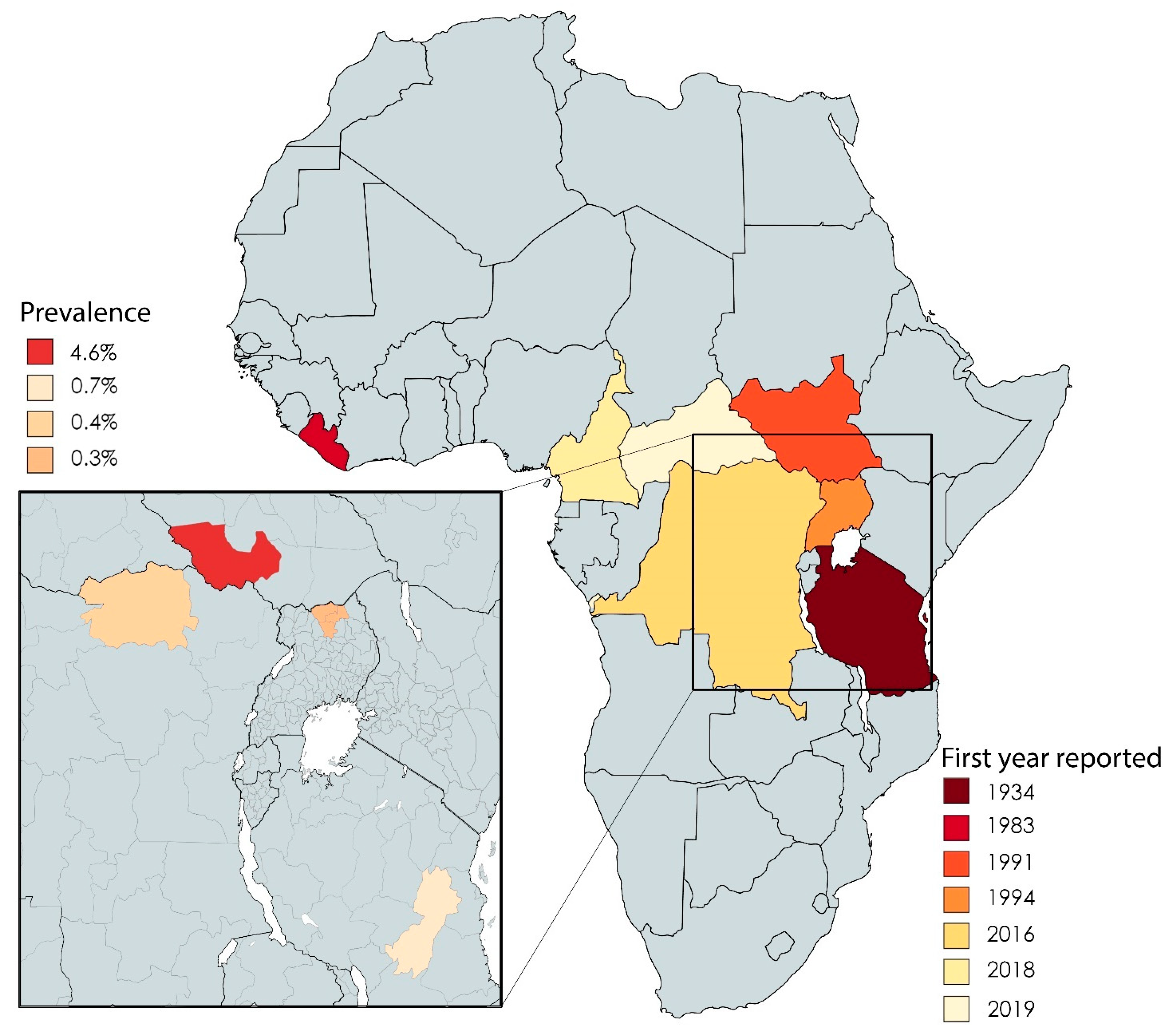
3.1. Epidemiology
3.2. Aetiology
3.2.1. Infection
3.2.2. Nutritional Deficiency
3.2.3. Toxins
3.2.4. Autoimmunity
3.2.5. Hormonal, Metabolic, and Genetic Factors
3.3. Pathophysiology
3.4. Clinical Features
3.5. Diagnosis and Management
3.6. Community Perceptions and Psychosocial and Economic Impact
3.6.1. Perceptions and Beliefs
3.6.2. Transmission, Presentation, and Treatment
3.6.3. Health-Seeking Behaviour of Caretakers
3.6.4. Psychosocial and Economic Burden
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dowell, S.F.; Sejvar, J.J.; Riek, L.; Vandemaele, K.A.; Lamunu, M.; Kuesel, A.C.; Schmutzhard, E.; Matuja, W.; Bunga, S.; Foltz, J.; et al. Nodding syndrome. Emerg. Infect. Dis. 2013, 19, 1374–1384. [Google Scholar] [CrossRef] [PubMed]
- Lacey, M. Nodding disease: Mystery of southern Sudan. Lancet Neurol. 2003, 2, 714. [Google Scholar] [CrossRef]
- Nodding Syndrome. Available online: http://www.who.int/onchocerciasis/symptoms/nodding_syndrome/en/ (accessed on 27 September 2019).
- Idro, R.; Opoka, R.O.; Aanyu, H.T.; Kakooza-Mwesige, A.; Piloya-Were, T.; Namusoke, H.; Musoke, S.B.; Nalugya, J.; Bangirana, P.; Mwaka, A.D.; et al. Nodding syndrome in Ugandan children—Clinical features, brain imaging and complications: A case series. BMJ Open 2013, 3, 3. [Google Scholar] [CrossRef]
- Abd-Elfarag, G.; van Hensbroek, M.B. Nodding Syndrome: The Unresolved Mystery of a Pediatric Disease in Sub-Saharan Africa. Pediatr. Infect. Dis. J. 2019, 38, S67–S71. [Google Scholar] [CrossRef]
- Mwaka, A.D.; Semakula, J.R.; Abbo, C.; Idro, R. Nodding syndrome: Recent insights into etiology, pathophysiology, and treatment. Res. Rep. Trop. Med. 2018, 9, 89–93. [Google Scholar] [CrossRef]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef]
- Levac, D.; Colquhoun, H.; O’Brien, K.K. Scoping studies: Advancing the methodology. Implement. Sci. 2010, 5, 69. [Google Scholar] [CrossRef] [PubMed]
- WHO. International Scientific Meeting on Nodding Syndrome Kampala, Uganda; WHO: Geneva, Switzerland, 2012; pp. 1–42. [Google Scholar]
- Spencer, P.S.; Palmer, V.S.; Jilek-Aall, L. Nodding syndrome: Origins and natural history of a longstanding epileptic disorder in sub-Saharan Africa. Afr. Health Sci. 2013, 13, 176–182. [Google Scholar] [CrossRef][Green Version]
- Waals, F.W.V.D.; Goudsmit, J.; Gajdusek, D.C. Characteristics of Highly Prevalent Seizure Disorders in the Gbawein and Wroughbarh Clan Region of Grand Bassa County, Liberia. Neuroepidemiology 1983, 1983, 35–44. [Google Scholar] [CrossRef]
- Spencer, P.S.; Vandemaele, K.; Richer, M.; Palmer, V.S.; Chungong, S.; Anker, M.; Ayana, Y.; Opoka, M.L.; Klaucke, B.N.; Quarello, A.; et al. Nodding syndrome in Mundri county, South Sudan: Environmental, nutritional and infectious factors. Afr. Health Sci. 2013, 13, 183–204. [Google Scholar] [CrossRef]
- Kaiser, C.; Rubaale, T.; Tukesiga, E.; Kipp, W.; Asaba, G. Nodding syndrome, western Uganda, 1994. Am. J. Trop. Med. Hyg. 2015, 93, 198–202. [Google Scholar] [CrossRef][Green Version]
- Sejvar, J.J.; Kakooza, A.M.; Foltz, J.L.; Makumbi, I.; Atai-Omoruto, A.D.; Malimbo, M.; Ndyomugyenyi, R.; Alexander, L.N.; Abang, B.; Downing, R.G.; et al. Clinical, neurological, and electrophysiological features of nodding syndrome in Kitgum, Uganda: An observational case series. Lancet Neurol. 2013, 12, 166–174. [Google Scholar] [CrossRef]
- Lenaerts, E.; Mandro, M.; Mukendi, D.; Suykerbuyk, P.; Dolo, H.; Wonya’Rossi, D.; Ngave, F.; Ensoy-Musoro, C.; Laudisoit, A.; Hotterbeekx, A.; et al. High prevalence of epilepsy in onchocerciasis endemic health areas in Democratic Republic of the Congo. Infect. Dis. Poverty 2018, 7, 68. [Google Scholar] [CrossRef] [PubMed]
- Siewe, J.F.N.; Ngarka, L.; Tatah, G.; Mengnjo, M.K.; Nfor, L.N.; Chokote, E.S.; Boullé, C.; Nkouonlack, C.; Dema, F.; Nkoro, G.A.; et al. Clinical presentations of onchocerciasis-associated epilepsy (OAE) in Cameroon. Epilepsy Behav. 2019, 90, 70–78. [Google Scholar] [CrossRef] [PubMed]
- Metanmo, S.; Boumediene, F.; Preux, P.M.; Colebunders, R.; Siewe Fodjo, J.N.; de Smet, E.; Yangatimbi, E.; Winkler, A.S.; Mbelesso, P.; Ajzenberg, D. First description of Nodding Syndrome in the Central African Republic. PLoS Negl. Trop. Dis. 2021, 15, e0009430. [Google Scholar] [CrossRef]
- Tumwine, J.K.; Vandemaele, K.; Chungong, S.; Richer, M.; Anker, M.; Ayana, Y.; Opoka, M.L.; Klaucke, D.N.; Quarello, A.; Spencer, P.S. Clinical and epidemiologic characteristics of nodding syndrome in Mundri County, southern Sudan. Afr. Health Sci. 2012, 12, 242–248. [Google Scholar] [CrossRef]
- Iyengar, P.J.; Wamala, J.; Ratto, J.; Blanton, C.; Malimbo, M.; Lukwago, L.; Becknell, S.; Downing, R.; Bunga, S.; Sejvar, J.; et al. Prevalence of nodding syndrome—Uganda, 2012–2013. CDC MMWR—Morb. Mortal. Wkly. Rep. 2014, 63, 603–606. [Google Scholar] [PubMed]
- Mukendi, D.; Tepage, F.; Akonda, I.; Siewe, J.N.F.; Rotsaert, A.; Ndibmun, C.N.; Laudisoit, A.; Couvreur, S.; Kabutako, B.; Menon, S.; et al. High prevalence of epilepsy in an onchocerciasis endemic health zone in the Democratic Republic of the Congo, despite 14 years of community-directed treatment with ivermectin: A mixed-method assessment. Int. J. Infect. Dis. 2019, 79, 187–194. [Google Scholar] [CrossRef]
- Mmbando, B.P.; Suykerbuyk, P.; Mnacho, M.; Kakorozya, A.; Matuja, W.; Hendy, A.; Greter, H.; Makunde, W.H.; Colebunders, R. High prevalence of epilepsy in two rural onchocerciasis endemic villages in the Mahenge area, Tanzania, after 20 years of community directed treatment with ivermectin. Infect. Dis. Poverty 2018, 7, 64. [Google Scholar] [CrossRef]
- Colebunders, R.; Carter, J.Y.; Olore, P.C.; Puok, K.; Bhattacharyya, S.; Menon, S.; Abd-Elfarag, G.; Ojok, M.; Ensoy-Musoro, C.; Lako, R.; et al. High prevalence of onchocerciasis-associated epilepsy in villages in Maridi County, Republic of South Sudan: A community-based survey. Seizure 2018, 63, 93–101. [Google Scholar] [CrossRef]
- Kitara, D.L.; Oh, J.; Mwaka, A.D. Nodding Syndrome in Uganda—A Disease Cluster: An Epidemiological Dilemma. Pac. J. Med Sci. 2013, 11, 21–33. [Google Scholar]
- Kaiser, C.; Asaba, G.; Rubaale, T.; Tukesiga, E.; Kipp, W. Onchocerciasis-Associated Epilepsy with Head Nodding Seizures-Nodding Syndrome: A Case Series of 15 Patients from Western Uganda, 1994. Am. J. Trop. Med. Hyg. 2018, 99, 1211–1218. [Google Scholar] [CrossRef] [PubMed]
- Lakwo, T.L.; Raimon, S.; Tionga, M.; Siewe Fodjo, J.N.; Alinda, P.; Sebit, W.J.; Carter, J.Y.; Colebunders, R. The Role of the Maridi Dam in Causing an Onchocerciasis-Associated Epilepsy Epidemic in Maridi, South Sudan: An Epidemiological, Sociological, and Entomological Study. Pathogens 2020, 9, 315. [Google Scholar] [CrossRef] [PubMed]
- De Polo, G.; Romaniello, R.; Otim, A.; Benjamin, K.; Bonanni, P.; Borgatti, R. Neurophysiological and clinical findings on Nodding Syndrome in 21 South Sudanese children and a review of the literature. Seizure 2015, 31, 64–71. [Google Scholar] [CrossRef][Green Version]
- Colebunders, R.; Hendy, A.; Mokili, J.L.; Wamala, J.F.; Kaducu, J.; Kur, L.; Tepage, F.; Mandro, M.; Mucinya, G.; Mambandu, G.; et al. Nodding syndrome and epilepsy in onchocerciasis endemic regions: Comparing preliminary observations from South Sudan and the Democratic Republic of the Congo with data from Uganda. BMC Res. Notes 2016, 9, 182. [Google Scholar] [CrossRef] [PubMed]
- Idro, R. Nodding syndrome in Uganda: Prevalence, clinical characteristics and management. Trop. Med. Int. Health 2013, 18, 29. [Google Scholar]
- Winkler, A.S.; Friedrich, K.; Konig, R.; Meindl, M.; Helbok, R.; Unterberger, I.; Gotwald, T.; Dharsee, J.; Velicheti, S.; Kidunda, A.; et al. The head nodding syndrome--clinical classification and possible causes. Epilepsia 2008, 49, 2008–2015. [Google Scholar] [CrossRef]
- CDC. Nodding syndrome—South Sudan, 2011. MMWR Morb. Mortal. Wkly. Rep. 2012, 61, 52–54. [Google Scholar]
- Foltz, J.L.; Makumbi, I.; Sejvar, J.J.; Malimbo, M.; Ndyomugyenyi, R.; Atai-Omoruto, A.D.; Alexander, L.N.; Abang, B.; Melstrom, P.; Kakooza, A.M.; et al. An Epidemiologic Investigation of Potential Risk Factors for Nodding Syndrome in Kitgum District, Uganda. PLoS ONE 2013, 8, e66419. [Google Scholar] [CrossRef] [PubMed]
- Abd-Elfarag, G.; Carter, J.Y.; Raimon, S.; Sebit, W.; Suliman, A.; Fodjo, J.N.S.; Olore, P.C.; Biel, K.P.; Ojok, M.; Logora, M.Y.; et al. Persons with onchocerciasis-associated epilepsy and nodding seizures have a more severe form of epilepsy with more cognitive impairment and higher levels of Onchocerca volvulus infection. Epileptic Disord. 2020, 22, 301–308. [Google Scholar] [CrossRef]
- Hotterbeekx, A.; Raimon, S.; Abd-Elfarag, G.; Carter, J.Y.; Sebit, W.; Suliman, A.; Siewe Fodjo, J.N.; De Witte, P.; Logora, M.Y.; Colebunders, R.; et al. Onchocerca volvulus is not detected in the cerebrospinal fluid of persons with onchocerciasis-associated epilepsy. Int. J. Infect. Dis. 2020, 91, 119–123. [Google Scholar] [CrossRef] [PubMed]
- Winkler, A.S.; Friedrich, K.; Velicheti, S.; Dharsee, J.; Konig, R.; Nassri, A.; Meindl, M.; Kidunda, A.; Muller, T.H.; Jilek-Aall, L.; et al. MRI findings in people with epilepsy and nodding syndrome in an area endemic for onchocerciasis: An observational study. Afr. Health Sci. 2013, 13, 529–540. [Google Scholar] [CrossRef] [PubMed]
- Spencer, P.S.; Mazumder, R.; Palmer, V.S.; Lasarev, M.R.; Stadnik, R.C.; King, P.; Kabahenda, M.; Kitara, D.L.; Stadler, D.; McArdle, B.; et al. Environmental, dietary and case-control study of Nodding Syndrome in Uganda: A post-measles brain disorder triggered by malnutrition? J. Neurol. Sci. 2016, 369, 191–203. [Google Scholar] [CrossRef]
- Roach, M.; Cantu, A.; Vieri, M.K.; Cotten, M.; Kellam, P.; Phan, M.; Hoek, L.V.; Mandro, M.; Tepage, F.; Mambandu, G.; et al. No Evidence Known Viruses Play a Role in the Pathogenesis of Onchocerciasis-Associated Epilepsy. An Explorative Metagenomic Case-Control Study. Pathogens 2021, 10, 787. [Google Scholar] [CrossRef] [PubMed]
- Gumisiriza, N.; Kugler, M.; Brusselaers, N.; Mubiru, F.; Anguzu, R.; Ningwa, A.; Ogwang, R.; Akun, P.; Mwaka, A.D.; Abbo, C.; et al. Risk Factors for Nodding Syndrome and Other Forms of Epilepsy in Northern Uganda: A Case-Control Study. Pathogens 2021, 10, 1451. [Google Scholar] [CrossRef]
- Obol, J.H.; Arony, D.A.; Wanyama, R.; Luryama Moi, K.; Bodo, B.; Odong, P.O.; Odida, M. Reduced plasma concentrations of vitamin B6 and increased plasma concentrations of the neurotoxin 3-hydroxykynurenine are associated with nodding syndrome: A case control study in Gulu and Amuru Districts, Northern Uganda. Trans. R. Soc. Trop. Med. Hyg. 2019, 113, S102–S103. [Google Scholar] [CrossRef]
- Soldatos, A.; Nutman, T.; Groden, C.; Wahl, C.; Inati, S.; Buckler, G.; O’Connell, E.; Opar, B.; Aryek-Kwe, J.; Downing, R.; et al. Evaluation and immunomodulatory treatment at the NIH of children with nodding syndrome from northern Uganda. Neurology 2015, 84, S37.005. [Google Scholar]
- Dietmann, A.; Wallner, B.; Konig, R.; Friedrich, K.; Pfausler, B.; Deisenhammer, F.; Griesmacher, A.; Seger, C.; Matuja, W.; JilekAall, L.; et al. Nodding syndrome in Tanzania may not be associated with circulating anti-NMDA-and anti-VGKC receptor antibodies or decreased pyridoxal phosphate serum levels-a pilot study. Afr. Health Sci. 2014, 14, 434–438. [Google Scholar] [CrossRef][Green Version]
- Echodu, R.; Edema, H.; Malinga, G.M.; Hendy, A.; Colebunders, R.; Moriku Kaducu, J.; Ovuga, E.; Haesaert, G. Is nodding syndrome in northern Uganda linked to consumption of mycotoxin contaminated food grains? BMC Res. Notes 2018, 11, 678. [Google Scholar] [CrossRef]
- Duringer, J.; Mazumder, R.; Palmer, V.; Craig, M.; Spencer, P. Case-Control Study of Nodding Syndrome in Acholiland: Urinary Multi-Mycotoxin Screening. Toxins 2021, 13, 313. [Google Scholar] [CrossRef]
- Johnson, T.P.; Tyagi, R.; Lee, P.R.; Lee, M.H.; Johnson, K.R.; Kowalak, J.; Elkahloun, A.; Medynets, M.; Hategan, A.; Kubofcik, J.; et al. Nodding syndrome may be an autoimmune reaction to the parasitic worm Onchocerca volvulus. Sci. Transl. Med. 2017, 9, 15. [Google Scholar] [CrossRef]
- Hotterbeekx, A.; Vieri, M.K.; Ramberger, M.; Jozefzoon-Aghai, A.; Mandro, M.; Tepage, F.; Dusabimana, A.; Kumar-Singh, S.; Titulaer, M.J.; Colebunders, R. No Evidence for the Involvement of Leiomodin-1 Antibodies in the Pathogenesis of Onchocerciasis-Associated Epilepsy. Pathogens 2021, 10, 845. [Google Scholar] [CrossRef] [PubMed]
- Benedek, G.; Abed El Latif, M.; Miller, K.; Rivkin, M.; Ahmed Ramadhan Lasu, A.; Riek, L.P.; Lako, R.; Edvardson, S.; Arbel-Alon, S.; Galun, E.; et al. Macrophage migration inhibitory factor in Nodding syndrome. PLoS Negl. Trop. Dis. 2021, 15, e0009821. [Google Scholar] [CrossRef]
- Piloya-Were, T.; Odongkara-Mpora, B.; Namusoke, H.; Idro, R. Physical growth, puberty and hormones in adolescents with Nodding Syndrome; a pilot study. BMC Res. Notes 2014, 7, 858. [Google Scholar] [CrossRef]
- Kitara, D.L.; Mwaka, A.D.; Kigonya, E. High Anion Gap Metabolic Acidosis among Children with Nodding Syndrome (NS) in Northern Uganda: Case Series. Br. J. Med. Med. Res. 2014, 4, 1301–1314. [Google Scholar] [CrossRef]
- Vieri, M.K.; Hotterbeekx, A.; Mandro, M.; Siewe Fodjo, J.N.; Dusabimana, A.; Nyisi, F.; Mukendi, D.; Gwatsvaira, J.; Kumar-Singh, S.; Colebunders, R. Serotonin Levels in the Serum of Persons with Onchocerciasis-Associated Epilepsy: A Case-Control Study. Pathogens 2021, 10, 720. [Google Scholar] [CrossRef]
- Denis, A.A.; Galloway, P.; Collines, A.; Frederick, M.E.; David, D.P.K.L. Metabolic analysis of nodding syndrome in Uganda: A pilot study is a biotinidase and acetyl carnitine deficiency; a metabolic disorder. An observational study design. World J. Pharm. Med. Res. 2018, 4, 160–174. [Google Scholar]
- Benedek, G.; Abed El Latif, M.; Miller, K.; Rivkin, M.; Ramadhan Lasu, A.A.; Riek, L.P.; Lako, R.; Edvardson, S.; Alon, S.A.; Galun, E.; et al. Protection or susceptibility to devastating childhood epilepsy: Nodding Syndrome associates with immunogenetic fingerprints in the HLA binding groove. PLoS Negl. Trop. Dis. 2020, 14, e0008436. [Google Scholar] [CrossRef] [PubMed]
- Pollanen, M.S.; Onzivua, S.; Robertson, J.; McKeever, P.M.; Olawa, F.; Kitara, D.L.; Fong, A. Nodding syndrome in Uganda is a tauopathy. Acta Neuropathol. 2018, 136, 691–697. [Google Scholar] [CrossRef]
- Hotterbeekx, A.; Lammens, M.; Idro, R.; Akun, P.R.; Lukande, R.; Akena, G.; Nath, A.; Taylor, J.; Olwa, F.; Kumar-Singh, S.; et al. Neuroinflammation and Not Tauopathy Is a Predominant Pathological Signature of Nodding Syndrome. J. Neuropathol. Exp. Neurol. 2019, 78, 1049–1058. [Google Scholar] [CrossRef]
- Winkler, A.S.; Wallner, B.; Friedrich, K.; Pfausler, B.; Unterberger, I.; Matuja, W.; Jilek-Aall, L.; Schmutzhard, E. A longitudinal study on nodding syndrome--a new African epilepsy disorder. Epilepsia 2014, 55, 86–93. [Google Scholar] [CrossRef] [PubMed]
- Ogwang, R.; Muhanguzi, D.; Mwikali, K.; Anguzu, R.; Kubofcik, J.; Nutman, T.B.; Taylor, M.; Newton, C.R.; Vincent, A.; Conroy, A.L.; et al. Systemic and cerebrospinal fluid immune and complement activation in Ugandan children and adolescents with long-standing nodding syndrome: A case-control study. Epilepsia Open 2021, 6, 297–309. [Google Scholar] [CrossRef]
- Vieri, M.K.; Hotterbeekx, A.; Raimon, S.; Abd-Elfarag, G.; Mukendi, D.; Carter, J.Y.; Kumar-Singh, S.; Colebunders, R. Cytokines and Onchocerciasis-Associated Epilepsy, a Pilot Study and Review of the Literature. Pathogens 2021, 10, 310. [Google Scholar] [CrossRef]
- Idro, R.; Ogwang, R.; Kayongo, E.; Gumisiriza, N.; Lanyero, A.; Kakooza-Mwesige, A.; Opar, B. The natural history of nodding syndrome. Epileptic Disord. 2018, 20, 508–516. [Google Scholar] [CrossRef]
- Colebunders, R.; Abd-Elfarag, G.; Carter, J.Y.; Olore, P.C.; Puok, K.; Menon, S.; Fodjo Siewe, J.N.; Bhattacharyya, S.; Ojok, M.; Lako, R.; et al. Clinical characteristics of onchocerciasis-associated epilepsy in villages in Maridi County, Republic of South Sudan. Seizure 2018, 62, 108–115. [Google Scholar] [CrossRef]
- Musisi, S.; Akena, D.; Nakimuli-Mpungu, E.; Abbo, C.; Okello, J. Neuropsychiatric perspectives on nodding syndrome in northern Uganda: A case series study and a review of the literature. Afr. Health Sci. 2013, 13, 205–218. [Google Scholar] [CrossRef]
- Gazda, S.; Kitara, D.L. Treatment and rehabilitation outcomes of children affected with nodding syndrome in Northern Uganda: A descriptive case series. Pan. Afr. Med. J. 2018, 29, 228. [Google Scholar] [CrossRef]
- Kakooza-Mwesige, A.; Dhossche, D.M.; Idro, R.; Akena, D.; Nalugya, J.; Opar, B.T. Catatonia in Ugandan children with nodding syndrome and effects of treatment with lorazepam: A pilot study. BMC Res. Notes 2015, 8, 825. [Google Scholar] [CrossRef] [PubMed]
- Idro, R.; Namusoke, H.; Abbo, C.; Mutamba, B.B.; Kakooza-Mwesige, A.; Opoka, R.O.; Musubire, A.K.; Mwaka, A.D.; Opar, B.T. Patients with nodding syndrome in Uganda improve with symptomatic treatment: A cross-sectional study. BMJ Open 2014, 4, e006476. [Google Scholar] [CrossRef] [PubMed]
- Gumisiriza, N.; Mubiru, F.; Siewe Fodjo, J.N.; Mbonye Kayitale, M.; Hotterbeekx, A.; Idro, R.; Makumbi, I.; Lakwo, T.; Opar, B.; Kaducu, J.; et al. Prevalence and incidence of nodding syndrome and other forms of epilepsy in onchocerciasis-endemic areas in northern Uganda after the implementation of onchocerciasis control measures. Infect. Dis. Poverty 2020, 9, 12. [Google Scholar] [CrossRef]
- Van Bemmel, K.; Derluyn, I.; Stroeken, K. Nodding syndrome or disease? On the conceptualization of an illness-in-the-making. Ethn. Health 2014, 19, 100–118. [Google Scholar] [CrossRef]
- Mitchell, K.B.; Kornfeld, J.; Adiama, J.; Mugenyi, A.; Schmutzhard, E.; Ovuga, E.; Kamstra, J.; Winkler, A.S. Nodding syndrome in northern Uganda: Overview and community perspectives. Epilepsy Behav. 2013, 26, 22–24. [Google Scholar] [CrossRef] [PubMed]
- Kitara, D.L.; Amone, C. Perception of the population in Northern Uganda to nodding syndrome. J. Med. Med. Sci. 2012, 3, 464–470. [Google Scholar]
- Buchmann, K. ‘These nodding people’: Experiences of having a child with nodding syndrome in postconflict Northern Uganda. Epilepsy Behav. 2015, 42, 71–77. [Google Scholar] [CrossRef]
- Buchmann, K. ‘You sit in fear’: Understanding perceptions of nodding syndrome in post-conflict northern Uganda. Glob. Health Action 2014, 7, 25069. [Google Scholar] [CrossRef]
- Irani, J.; Rujumba, J.; Mwaka, A.D.; Arach, J.; Lanyuru, D.; Idro, R.; Gerrets, R.; Grietens, K.P.; O’Neill, S. “Those who died are the ones that are cured”. Walking the political tightrope of Nodding Syndrome in northern Uganda: Emerging challenges for research and policy. PLoS Negl. Trop. Dis. 2019, 13, e0007344. [Google Scholar] [CrossRef] [PubMed]
- Mutamba, B.; Abbo, C.; Muron, J.; Idro, R.; Mwaka, A.D. Stereotypes on Nodding syndrome: Responses of health workers in the affected region of northern Uganda. Afr. Health Sci. 2013, 13, 986–991. [Google Scholar] [CrossRef][Green Version]
- Abbo, C.; Mwaka, A.D.; Opar, B.T.; Idro, R. Qualitative evaluation of the outcomes of care and treatment for children and adolescents with nodding syndrome and other epilepsies in Uganda. Infect. Dis. Poverty 2019, 8, 30. [Google Scholar] [CrossRef] [PubMed]
- Mwaka, A.D.; Okello, E.S.; Abbo, C.; Odwong, F.O.; Olango, W.; Etolu, J.W.; Oriyabuzu, R.; Lagoro, D.K.; Mutamba, B.B.; Idro, R.; et al. Is the glass half full or half empty? A qualitative exploration on treatment practices and perceived barriers to biomedical care for patients with nodding syndrome in post-conflict northern Uganda. BMC Res. Notes 2015, 8, 386. [Google Scholar] [CrossRef]
- Nakigudde, J.; Mutamba, B.B.; Bazeyo, W.; Musisi, S.; James, O. An exploration of caregiver burden for children with nodding syndrome (lucluc) in Northern Uganda. BMC Psychiatry 2016, 16, 255. [Google Scholar] [CrossRef]
- Mmbando, B.P.; Mnacho, M.; Makunde, M.; Kakorozya, A.; Matuja, W.; Greter, H.; Suykerbuyk, P.; Colebunders, R. High prevalence of epilepsy and onchocerciasis after 20 years of ivermectin use in four villages of the Mahenge area in Tanzania. Trop. Med. Int. Health 2017, 22, 61. [Google Scholar]
- Duke, B.O.L.; Vincelette, J.; Moore, P.J. Microfilariae in the Cerebrospinal Fluid, and Neurological Complications, during Treatment of Ochocerciasis with Diethyl-carbamazine. Trop. Parasitol. 1976, 27, 123–132. [Google Scholar] [CrossRef]
- Colebunders, R.; Titulaer, M.J. Nodding syndrome: Preventable and treatable. Sci. Transl. Med. 2017, 9, 15. [Google Scholar] [CrossRef] [PubMed]
- Nauen, D.W.; Haffner, M.C.; Kim, J.; Zheng, Q.; Yin, H.; DeMarzo, A.M.; Mahairaki, V.; Colantuoni, C.; Pickering, J.G.; Johnson, T.P. Putative Autoantigen Leiomodin-1 Is Expressed in the Human Brain and in the Membrane Fraction of Newly Formed Neurons. Pathogens 2021, 9, 1036. [Google Scholar] [CrossRef]
- Garg, R.K. Subacute sclerosing panencephalitis. Postgrad. Med. J. 2002, 2002, 63–70. [Google Scholar] [CrossRef]
- Bhandari, N.R. Vitamin B6 Deficiency and Convulsions. Indian J. Pediat. 1959, 26, 371–374. [Google Scholar]
- Lee, D.-G.; Lee, Y.; Shin, H.; Kang, K.; Park, J.-M.; Kim, B.-K.; Kwon, O.; Lee, J.-J. Seizures Related to Vitamin B6 Deficiency in Adults. J. Epilepsy Res. 2015, 5, 23–24. [Google Scholar] [CrossRef] [PubMed]
- WHO. Traditional Medicine. In Provisional Agenda Item 1410; ASSEMBLY F-SWH, Ed.; WHO: Geneva, Switzerland, 2003. [Google Scholar]
- Breningstall, G.N. Carnitine Deficiency Syndromes. Pediatr. Neurol. Clin. 1990, 1990, 75–81. [Google Scholar] [CrossRef]
- Wolf, B. Biotinidase Deficiency. In GeneReviews; Adam, M.P., Ed.; University of Washington: Seattle, WA, USA, 2016; Volume 1993–2021. [Google Scholar]
- Smith, K.M.; Blessing, M.M.; Parisi, J.E.; Britton, J.W.; Mandrekar, J.; Cascino, G.D. Tau deposition in young adults with drug-resistant focal epilepsy. Epilepsia 2019, 2019, 2398–2403. [Google Scholar] [CrossRef]
- Tai, X.Y.; Koepp, M.; Duncan, J.S.; Fox, N.; Thompson, P.; Baxendale, S.; Liu, J.Y.W.; Reeves, C.; Michalak, Z.; Thom, M. Hyperphosphorylated tau in patients with refractory epilepsy correlates with cognitive decline: A study of temporal lobe resections. Brain 2016, 2016, 2441–2455. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria | |
|---|---|---|
| Study design and population | All study designs of persons with nodding syndrome (according to clinical case definition [9] or cases with features of nodding syndrome) of any age | Studies of known epilepsies other than NS and other known neurodegenerative diseases |
| Publications | All publications: Commentaries, editorials, letters, books, book chapters, dissertations, and conference proceedings with primary/original study data | Studies with nonprimary data |
| Outcome | Epidemiology, aetiology, pathophysiology, clinical features, diagnosis, and treatment of NS; community perceptions and the socioeconomic impact of NS | |
| Language, year, and country | English publications from 1946 onward, from any country |
| Database | Search Terms |
|---|---|
| Embase | #1. ‘nodding syndrome’/exp #2. (nodding NEAR/2 (head OR disease OR syndrome)):ti,ab,kw #3. river epilepsy’:ti,ab,kw #4. onchocerciasis’/exp OR ‘onchocerca’/exp OR onchocerc *:ti,ab,kw #5. epilepsy’/exp OR nodding:ti,ab,kw OR epilepsy *:ti,ab,kw OR seizure *:ti,ab,kw #6. #4 AND #5 #7. #1 OR #2 OR #3 OR #6 |
| Medline | #1. exp Nodding Syndrome/ #2. (nodding adj2 (head or disease or syndrome)).ti,ab,kf. #3. river epilepsy.ti,ab,kf. #4. exp Onchocerciasis/or exp Onchocerca/or onchocerc *.ti,ab,kf. #5. exp Epilepsy/or (nodding or epilepsy * or seizure *).ti,ab,kf. #6. 4 and 5 #7. 1 or 2 or 3 or 6 |
| Scopus | TITLE-ABS-KEY ((nodding AND near/2 (head OR disease OR syndrome)) OR ‘river AND epilepsy’ OR (onchocerc* AND (nodding OR epileps* OR seizure*))) |
| Global Health Library | ab:(nodding AND (disease OR syndrome OR head) OR ‘river epilepsy’ OR (onchocerc * and (nodding or epilepsy * or seizure *))) ti:((nodding AND (disease OR syndrome OR head) OR ‘river epilepsy’ OR (onchocerc * and (nodding or epilepsy * or seizure *)))) |
| Pathogen | Location | Test | Cases | Controls | Odds Ratio (95% CI) | p-Value | Reference | |||
|---|---|---|---|---|---|---|---|---|---|---|
| Country | Area (Year) | N | % | N | % | |||||
| Onchocerca volvulus | South Sudan | Lui (2001) | SSM | 39 | 89.7 | 31 | 48.3 | 9.2 (2.7–3.26) | 0.00003 | [12,18] |
| Amadi (2001) | SSM | 30 | 96.7 | 34 | 50 | 29 (3.5–237.7) | - | [18] | ||
| Lui (2002) | SSM | 13 | 92.3 | 16 | 43.7 | 15.4 (1.6–148.8) | 0.008 | [12,18] | ||
| Maridi and Witto (2011) | SSM | 38 | 76.3 | 38 | 47.4 | 3.2 (1.2–8.7) | 0.02 | [30] | ||
| Uganda | Kitgum (2009) | SSM | 45 | 71.1 | 39 | 53.9 | 1.11 (0.37–3.27) | - | [31] | |
| Ov16 IgG | 39 | 66.7 | 44 | 31.8 | 3.14 (1.08–9.13) | - | ||||
| OvFAR/MSA | 39 | 94.9 | 41 | 48.8 | 14.4 (2.65–78.3) | |||||
| Kitgum and Pader (2016/17) | Ov16 IgG | 154 | 93.5 | 153 | 54.9 | 8.79 (4.15–18.65) | 0.001 | [37] | ||
| Mansonella perstans | South Sudan | Lui (2001) | BM | 39 | 41 | 31 | 9.6 | 3.2 | 0.005 | [12] |
| Amadi (2001) | BM | 30 | 66.6 | 34 | 50 | |||||
| Loa loa | South Sudan | Lui and Amadi (2001) | BM | 69 | 0 | 65 | 0 | - | - | [12] |
| Wuchereria bancrofti | South Sudan | Lui (2001) | BM | 39 | 0 | 31 | 9 | - | 0.47 | [12] |
| Amadi (2001) | 30 | 0 | 34 | 7.6 | - | |||||
| Trypanosoma brucei | South Sudan | Lui (2021) | CATT | 39 | 12.8 | 31 | 9.6 | 0.84 | 0.94 | [12] |
| Amadi (2001) | 30 | 0 | 34 | 5.8 | ||||||
| Uganda | Kitgum (2009) | CATT | 36 | 0 | 40 | 0 | - | - | [31] | |
| Taenia soleum | Uganda | Kitgum (2009) | Antibody | 36 | 0 | 40 | 0 | - | - | [31] |
| Measles virus | Uganda | Kitgum (2009) | Past history | 23.5 | 6.1 | 3.3 (0.8–13.6) | [31] | |||
| PCR | 16 | 0 | 0 | - | - | - | ||||
| South Sudan | Lui and Amadi (2002) | Past history | 13 | 15.38 | 19 | 58 | 0.13 | 0.025 | [12] | |
| Uganda | Kitgum (2014) | Past history | 50 | 100 | 50 | - | 6 (1.02–113) | 0.047 | [35] | |
| Hepatitis E virus | Kitgum (2009) | IgM | 38 | 31.6 | 31 | 16.1 | 1.45 (0.37–5.58) | - | [31] | |
| IgG | 38 | 26.3 | 30 | 33.3 | 0.81 (0.24–2.75) | - | ||||
| Micronutrient | Location | Cases | Controls | Odds Ratio (95% CI) | p-Value | Reference | |||
|---|---|---|---|---|---|---|---|---|---|
| Country | Area (Year) | N | % | N | % | ||||
| Vitamin B6 (P5P) | Uganda | Gulu & Amuru district (2013) | 66 | 73 | 7.22 (2.24–23.26) | 0.001 | [38] | ||
| Uganda | Kitgum (2009) | 49 | 73 | 42 | 64 | 1.22 (0.41–3.59) | - | [31] | |
| Uganda | - | 3 | 100 | 5 | 100 | - | - | [39] | |
| Vitamin A | Uganda | Kitgum (2009) | 25 | 40 | 12 | 33 | 2.15 (0.41–11.12) | - | [31] |
| Vitamin B12 | Uganda | Kitgum (2009) | 25 | 8 | 12 | 8 | 1.46 (0.09–22.82) | - | [31] |
| Folate | Uganda | Kitgum (2009) | 11 | 9 | 9 | 0 | - | - | [31] |
| Zinc | Uganda | Kitgum (2009) | 17 | 47 | 12 | 67 | 0.72 (0.13–3.94) | - | [31] |
| Selenium | Uganda | Kitgum (2009) | 17 | 100 | 12 | 100 | - | - | [31] |
| Toxins | Location | Test | Cases | Controls | Odds Ratio (95% CI) | p-Value | Reference | |||
|---|---|---|---|---|---|---|---|---|---|---|
| Country | Area (Year) | N | % | N | % | |||||
| Mouldy maize | Uganda | Kitgum (2014) | DtH | 50 | 50 | 4.33 (1.4–18.9) | 0.009 | [35] | ||
| Maize | Uganda | Kitgum (2014) | DtH | 50 | 50 | 4 (1.0–26.5) | 0.05 | [35] | ||
| Emergency/relief food supplies | Uganda | Kitgum (2014) | DtH | 47 | 50 | 4 (1.3–17.6) | 0.016 | [35] | ||
| Gulu and Amuru (2016) | DtH | 40 | 67 | 18 | 27 | 4.05 (1.23–13.28) | 0.021 | [38] | ||
| Red/brown sorghum | South Sudan | Mundri (2002) | DtH | 13 | 54 | 19 | 16 | 6.22 (1.2–32.3) | 0.049 | [12] |
| Uganda | Kitgum (2009) | DtH | - | 98 | - | 100 | 1.3 (0.0–125.9) | - | [31] | |
| Spoiled relief food | Uganda | Kitgum (2009) | DtH | - | 43 | - | 47 | 0.3 (0.1–1.3) | - | [31] |
| Seeds meant for planting | Uganda | Kitgum (2009) | DtH | - | 61 | - | 65 | 0.6 (0.1–2.3) | - | [31] |
| South Sudan | Mundri (2002) | DtH | - | - | - | - | 5 (0.82–30.4) | 0.11 | [12] | |
| River fish | Uganda | Kitgum (2009) | DtH | - | 96 | - | 100 | 0.3 (0.0–11.6) | - | [31] |
| Insects | Uganda | Kitgum (2009) | DtH | - | 41 | - | 33 | 0.8 (0.2–2.9) | - | [31] |
| Rodent brain | Uganda | Kitgum (2009) | DtH | - | 55 | - | 51 | 1.8 (0.3–12.3) | - | [31] |
| Baboon brain | South Sudan | Mundri (2002) | DtH | - | - | - | - | 3 (0.63–14.2) | 0.25 | [12] |
| Baboon meat | South Sudan | Mundri (2002) | DtH | - | - | - | - | 4.5 (0.97–20.8) | 0.07 | [12] |
| Crushed roots as traditional medicines | Uganda | Kitgum (2009) | DrH | - | 39 | - | 16 | 5.4 (1.3–22.1) | - | [31] |
| Uganda | Kitgum (2014) | DrH | 50 | - | 50 | - | 1.29 (0.47–3.6) | 0.617 | [35] | |
| Crushed leaves | Uganda | Kitgum (2009) | DrH | - | 8 | - | 2 | 3.4 (0.2–45.8) | - | [31] |
| Crushed flowers | Uganda | Kitgum (2009) | DrH | - | 0 | - | 2 | 0.9 (0.1–5.6) | - | [31] |
| Inhaled medicines | Uganda | Kitgum (2009) | DrH | - | 2 | - | 0 | 0.2 (0.0–1.5) | - | [31] |
| Exposure to chemicals from munitions | Uganda | Kitgum (2009) | EH | - | 70 | - | 51 | 13.9 (1.4–135) | - | [31] |
| Suspected Case: | Reported Head Nodding in a Previously Healthy Person. Head Nodding Is Defined as Repetitive, Involuntary Drops of the Head towards the Chest on Two or More Occasions |
|---|---|
| Probable case | Suspected case of head nodding, with one major criterion plus at least one minor criterion Major criteria:
|
| Confirmed case | Probable case, with documented head-nodding episodes based on:
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abd-Elfarag, G.O.E.; Edridge, A.W.D.; Spijker, R.; Sebit, M.B.; van Hensbroek, M.B. Nodding Syndrome: A Scoping Review. Trop. Med. Infect. Dis. 2021, 6, 211. https://doi.org/10.3390/tropicalmed6040211
Abd-Elfarag GOE, Edridge AWD, Spijker R, Sebit MB, van Hensbroek MB. Nodding Syndrome: A Scoping Review. Tropical Medicine and Infectious Disease. 2021; 6(4):211. https://doi.org/10.3390/tropicalmed6040211
Chicago/Turabian StyleAbd-Elfarag, Gasim Omer Elkhalifa, Arthur Wouter Dante Edridge, René Spijker, Mohamed Boy Sebit, and Michaël B. van Hensbroek. 2021. "Nodding Syndrome: A Scoping Review" Tropical Medicine and Infectious Disease 6, no. 4: 211. https://doi.org/10.3390/tropicalmed6040211
APA StyleAbd-Elfarag, G. O. E., Edridge, A. W. D., Spijker, R., Sebit, M. B., & van Hensbroek, M. B. (2021). Nodding Syndrome: A Scoping Review. Tropical Medicine and Infectious Disease, 6(4), 211. https://doi.org/10.3390/tropicalmed6040211