
Antimicrobial Resistance among Neonates with Bacterial Sepsis and Their Clinical Outcomes in a Tertiary Hospital in Kathmandu Valley, Nepal

 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Setting
2.2.1. General Setting
2.2.2. Specific Setting
2.2.3. Laboratory Testing of Microorganisms
2.3. Study Population and Duration
2.4. Management of Neonatal Sepsis in KIST MCTH
2.5. Definitions
2.5.1. Suspected Sepsis
2.5.2. Clinical Sepsis
2.5.3. Proven Sepsis
2.6. Data Collection, Analysis, and Statistics
2.7. Ethics Considerations
Data Confidentiality
3. Results
3.1. Characteristics of Neonates Admitted with Suspected Sepsis at KIST MCTH
3.2. Turnaround Time of Bacterial CDST and Change in Antibiotic after CDST Results
3.3. Antibiotic Resistance Pattern of Isolates
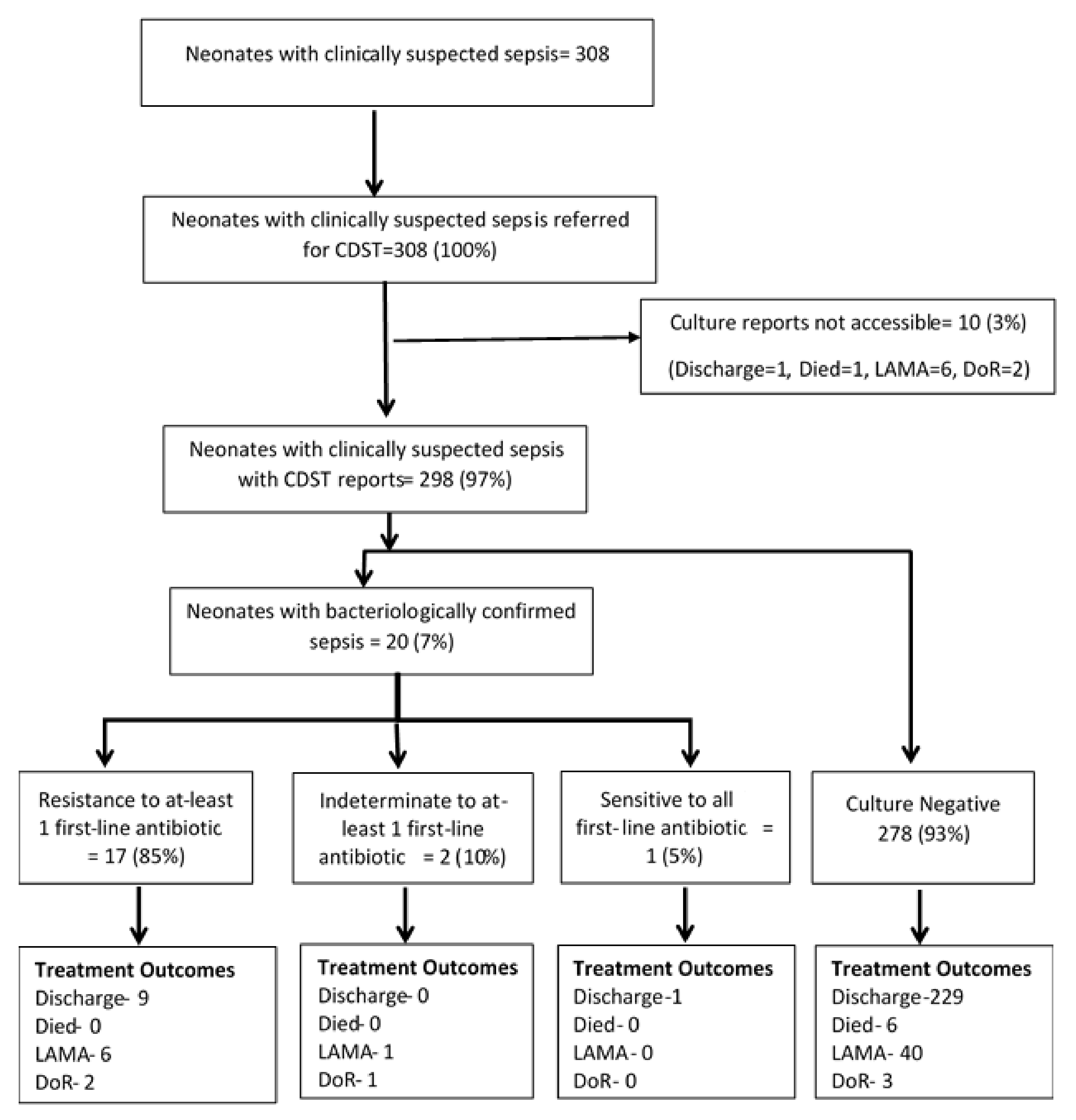
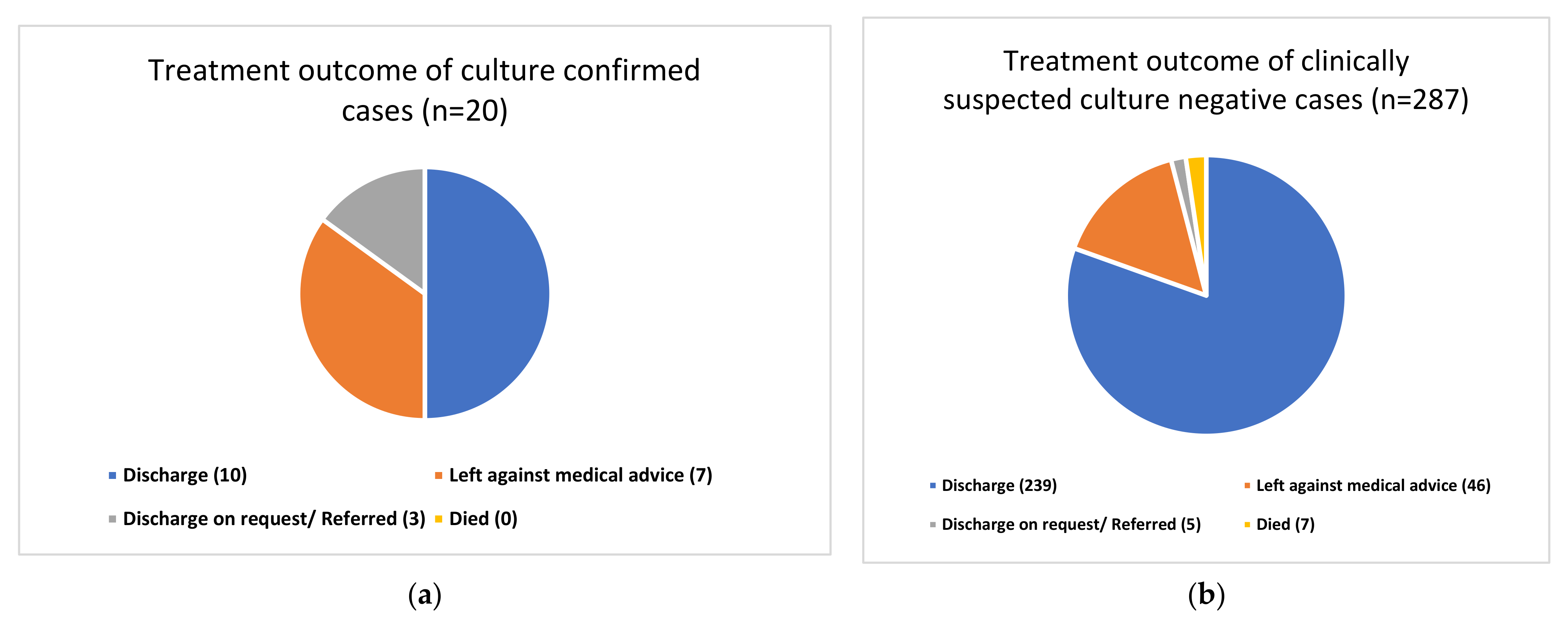
3.4. Treatment Outcome of Clinically Suspected Sepsis Neonates
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
Open Access Statement and Disclaimer
References
- World Health Organization. Improving the Prevention, Diagnosis and Clinical Management of Sepsis; WHO: Geneva, Switzerland, 2017. [Google Scholar]
- Lawn, J.E.; Cousens, S.; Zupan, S. 4 million neonatal deaths: When? where? why? Lancet 2005, 365, 891–900. [Google Scholar] [CrossRef]
- GBD 2016 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national age-sex specific mortality for 264 causes of death, 1980–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet 2017, 390, 1151–1210. [Google Scholar] [CrossRef]
- Liu, L.; Oza, S.; Hogan, D.; Perin, J.; Rudan, I.; Lawn, J.E.; Cousens, S.; Mathers, C.; Black, R.E. Global, regional, and national causes of child mortality in 2000–13, with projections to inform post-2015 priorities: An updated systematic analysis. Lancet 2015, 385, 430–440. [Google Scholar] [CrossRef]
- Ministry of Health, Nepal; New ERA; ICF International Inc. Nepal Demographic and Health Survey 2016; Ministry of Health & Population of Nepal: Kathmandu, Nepal, 2017; 411p. Available online: https://www.dhsprogram.com/pubs/pdf/FR336/FR336.pdf (accessed on 1 December 2017).
- World Health Organization. Every Newborn: An Action Plan to End Preventable Deaths; WHO: Geneva, Switzerland, 2014. [Google Scholar]
- Ranjeva, S.L.; Warf, B.C.; Schiff, S.J. Economic burden of neonatal sepsis in sub-Saharan Africa. BMJ Glob. Health 2018, 3, e000347. [Google Scholar] [CrossRef] [PubMed]
- Sharma, S.; Chapagain, R.H.; Pathak, O.K.; Gupta, A.; Rai, K.R.; Karn, S.; Sah, S.K. The Economic burden of Neonatal Intensive Care Unit Admission at a Community Hospital of Central Nepal. J. Nepal Paediatr. Soc. 2020, 40, 41–47. [Google Scholar] [CrossRef]
- Thaver, D.; Zaidi, A.K.M. Burden of Neonatal Infections in Developing Countries. Pediatr. Infect. Dis. J. 2009, 28, S3–S9. [Google Scholar] [CrossRef]
- Sharma, A.; Rijal, P.; Bichha, R.P. Neonatal status in Nepal Medical College Teaching Hospital. Nepal Med. Coll. J. 2011, 13, 197–198. [Google Scholar] [PubMed]
- Thapa, B.; Thapa, A.; Aryal, D.R.; Thapa, K.; Pun, A.; Khanal, S.; Mahat, K. Neonatal sepsis as a major cause of morbidity in a tertiary center in Kathmandu. J. Nepal Med. Assoc. 2013, 52, 549–556. [Google Scholar] [CrossRef]
- Shrestha, S.; Adhikari, N.; Rai, B.K.; Shreepaili, A. Antibiotic resistance pattern of bacterial isolates in neonatal care unit. J. Nepal Med. Assoc. 2010, 50. [Google Scholar] [CrossRef]
- Shrestha, A.; Shrestha, S. A Study of Clinico-pathological Profile of Suspected and Confirmed Neonatal Sepsis at Kathmandu Medical College. Nepal Med. Coll. J. 2020, 22, 82–87. [Google Scholar] [CrossRef]
- Belachew, A.; Tewabe, T. Neonatal sepsis and its association with birth weight and gestational age among admitted neonates in Ethiopia: Systematic review and meta-analysis. BMC Pediatr. 2020, 20, 55. [Google Scholar] [CrossRef]
- Greenhow, T.L.; Hung, Y.-Y.; Herz, A.M. Changing Epidemiology of Bacteremia in Infants Aged 1 Week to 3 Months. Pediatrics 2012, 129, e590–e596. [Google Scholar] [CrossRef] [PubMed]
- Viswanathan, R.; Singh, A.K.; Basu, S.; Chatterjee, S.; Sardar, S.; Isaacs, D. Multi-drug resistant gram negative bacilli causing early neonatal sepsis in India. Arch. Dis. Child. 2011, 97, F182–F187. [Google Scholar] [CrossRef]
- Awad, H.A.; Mohamed, M.H.; Badran, N.F.; Mohsen, M.; Abd-Elrhman, A.-S.A. Multidrug-resistant organisms in neonatal sepsis in two tertiary neonatal ICUs, Egypt. J. Egypt. Public Health Assoc. 2016, 91, 31–38. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health and Population (MOHP) [Nepal]; New ERA; ICF International Inc. Nepal Demographic and Health Survey; Ministry of Health and Population: Kathmandu, Nepal; ICF International Inc.: Claverton, MD, USA, 2011; p. 2012. [Google Scholar]
- Shrestha, R.K.; Rai, S.K.; Khanal, L.K.; Manda, P.K. Bacteriological study of neonatal sepsis and antibiotic susceptibility pattern of isolates in Kathmandu, Nepal. Nepal Med. Coll. J. 2013, 15, 71–73. [Google Scholar] [PubMed]
- Naas, T.; Cuzon, G.; Robinson, A.L.; Andrianirina, Z.; Imbert, P.; Ratsima, E.; Ranosiarisoa, Z.N.; Nordmann, P.; Raymond, J. Neonatal infections with multidrug-resistant ESBL-producing E. cloacae and K. pneumoniae in Neonatal Units of two different Hospitals in Antananarivo, Madagascar. BMC Infect. Dis. 2016, 16, 275. [Google Scholar] [CrossRef]
- Nepal. Available online: https://en.wikipedia.org/wiki/Nepal (accessed on 4 July 2019).
- Mahalakshmi Muncipality. Available online: www.mahalaxmimun.gov.np/ne/node/10 (accessed on 4 July 2019).
- Clinical and Laboratory Standards Institute. Performance Standards for Antimicrobial Susceptibility Testing, 28th ed.; CLSI Supplement M100; Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2018. [Google Scholar]
- Odabasi, I.O.; Bulbul, A. Neonatal Sepsis. Med Bull. Sisli Etfal Hosp. 2020, 54, 142–158. [Google Scholar] [CrossRef]
- Bhattarai, S.; Chapagain, R.H.; Mishra, D.; Shrestha, A.K.; Shrestha, S.M. Bacteriological Profile and Antibiotic Sensitivity Pattern of Neonatal Sepsis in Central Paediatric Referral Hospital in Nepal. J. Nepal Paediatr. Soc. 2019, 39, 1–5. [Google Scholar] [CrossRef]
- Mogollón, C.A.; Mogollón, C.A.; Bautista, E.E.; Hernández-Arriaga, G.; Bueso-Pineda, L.; Tovani-Palone, M.R. Factors Associated with Early-onset Neonatal Sepsis in Children of Peruvian Military Personnel. Electron. J. Gen. Med. 2019, 16, em156. [Google Scholar] [CrossRef]
- Yadav, S.K.; Giri, A. Bacteriological Profile of Neonatal Sepsis in a Neonatal Intensive Care Unit of a Tertiary Care Hospital of Eastern Nepal. J. Coll. Med Sci. 2019, 15, 93–97. [Google Scholar] [CrossRef]
- Marwah, P.; Chawla, D.; Chander, J.; Guglani, V.; Marwah, A. Bacteriological profile of neonatal sepsis in a tertiary-care hospital of Northern India. Indian Pediatr. 2015, 52, 158–159. [Google Scholar] [PubMed]
- Pokhrel, B.; Koirala, T.; Shah, G.; Joshi, S.; Baral, P. Bacteriological profile and antibiotic susceptibility of neonatal sepsis in neonatal intensive care unit of a tertiary hospital in Nepal. BMC Pediatr. 2018, 18, 208. [Google Scholar] [CrossRef]
- Jatsho, J.; Nishizawa, Y.; Pelzom, D.; Sharma, R. Clinical and Bacteriological Profile of Neonatal Sepsis: A Prospective Hospital-Based Study. Int. J. Pediatr. 2020, 2020, 1835945. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristics | Clinically Suspected N = 308 | Culture Confirmed N = 20 | Resistant to at Least One First-Line Antibiotic N = 18 |
|---|---|---|---|
| N (%) | N (%) | N (%) | |
| Demographic | |||
| Age in days | |||
| ≤3 | 280 (91) | 15 (75) | 13 (72) |
| 4–7 | 14 (4.5) | 4 (20) | 4 (22) |
| >8 | 14 (4.5) | 1 (5) | 1 (6) |
| Gender | |||
| Male | 172 (56) | 11 (55) | 9 (50) |
| Female | 133 (43) | 8 (40) | 8 (44) |
| Missing | 3 (1) | 1 (5) | 1 (6) |
| Year of admission | |||
| 2018 (June–December) | 116 (38) | 10 (50) | 10 (56) |
| 2019 (January–December) | 192 (62) | 10 (50) | 8 (44) |
| Perinatal characteristics | |||
| Gestational age | |||
| Preterm (<37 w) | 46 (15) | 4 (20) | 4 (22) |
| Early-term (37–38 w + 6 d) | 68 (22) | 8 (40) | 10 (55) |
| Full-term (39−40 w + 6 d) | 136 (44) | 5 (25) | 2 (11) |
| Late-term (40−41 w + 6 d) | 32 (10) | 0 (0) | 0 (0) |
| Post-term (>42 w) | 7 (2) | 1 (5) | 1 (6) |
| Missing | 18 (6) | 2 (10) | 1 (6) |
| Mode of delivery | |||
| Normal | 162 (52) | 10 (50) | 9 (50) |
| Cesarean section | 141 (46) | 8 (40) | 7 (39) |
| Missing | 5 (2) | 2 (10) | 2 (11) |
| Birth weight in grams | |||
| Very low (<1500 gm) | 6 (2) | 0 (0) | 0 (0) |
| Low (1501–<2500 gm) | 55 (18) | 5 (25) | 5 (28) |
| Normal (≥2500 gm) | 247 (80) | 15 (75) | 13 (72) |
| Clinical Characteristics | |||
| Jaundice | |||
| Negative | 184 (60) | 12 (60) | 12 (67) |
| Positive | 119 (39) | 7 (35) | 5 (28) |
| Missing | 5 (1) | 1 (5) | 1 (5) |
| Hyperbilirubinemia (Bilirubin level) (mg/dL) | |||
| ≥5 | 4 (1) | 0 (0) | 0 (0) |
| 6–15 | 70(23) | 2 (10) | 2 (11) |
| >15 | 44(14) | 5 (25) | 3 (17) |
| No | 190(62) | 13 (65) | 13 (72) |
| Baseline C-reactive protein | |||
| High(+ve) | 33 (10) | 1 (5) | 1 (6) |
| Low(−ve) | 267 (87) | 18 (90) | 16 (88) |
| Missing | 8 (3) | 1 (5) | 1 (6) |
| Variables | All Neonates n (%) | Culture Positive Neonates n (%) |
|---|---|---|
| Receipt of CDST results | ||
| Yes | 298 (97) | 20 |
| No | 10 (3) | 0 |
| Day of receipt of CDST results after admission | ||
| 3 | 269 (87) | 10 (50%) |
| 4 | 14 (5) | 7 (35%) |
| 5 | 3 (1) | 3 (15%) |
| ≥5 | 1 (0) | - |
| Missing | 2 (1) | - |
| Antibiotic change made | ||
| Yes | 32 (10) | 3 (15%) |
| No | 18 (6) | 17 (85%) |
| Not applicable | 258 (84) | - |
| Gram-Positive Isolates | Gram-Negative Isolates | ||||
|---|---|---|---|---|---|
| Drugs | S. aureus | CoNS | Enterococcus Species | Acinetobacter Species | Klebsiella pneumoniae |
| Total isolates | 8 | 5 | 1 | 3 | 3 |
| 1st line antibiotics (no. of resistance/no. of isolates tested) | |||||
| Amikacin (6/18) | 1 | 2 | 1 | 1 | 1 |
| Ampicillin (17/18) | 7 | 4 | 1 | 2 | 3 |
| Cefotaxime (16/19) | 7 | 3 | 1 | 2 | 3 |
| Ceftriaxone (6/14) | 2 | 1 | 1 | 1 | 1 |
| Ciprofloxacin (8/18) | 2 | 2 | 1 | 1 | 2 |
| Cotrimoxazole (8/19) | 3 | 1 | 1 | 1 | 2 |
| Chloramphenicol (4/15) | 1 | 0 | 0 | 2 | 1 |
| Carbenicillin (1/1) | 0 | 0 | 0 | 1 | 0 |
| Gentamycin (1st) (6/18) | 1 | 2 | 1 | 1 | 1 |
| Piperacilin + tazobactam (1/1) | 0 | 0 | 0 | 1 | 0 |
| 2nd line antibiotics | |||||
| Amoxicillin-clavulanic acid (5/6) | 1 | 0 | 0 | 2 | 2 |
| Ceftazidime (6/6) | 1 | 0 | 1 | 2 | 2 |
| Cefepime (3/4) | 1 | 0 | 0 | 1 | 1 |
| Imipenem (0/4) | 0 | 0 | 0 | 0 | 0 |
| Meropenem (2/10) | 0 | 0 | 1 | 1 | 0 |
| Ofloxacin (4/5) | 1 | 0 | 1 | 1 | 1 |
| Tetracycline (0/1) | 0 | 0 | 0 | 0 | 0 |
| Vancomycin (0/4) | 0 | 0 | 0 | 0 | 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Raghubanshi, B.R.; Sagili, K.D.; Han, W.W.; Shakya, H.; Shrestha, P.; Satyanarayana, S.; Karki, B.M.S. Antimicrobial Resistance among Neonates with Bacterial Sepsis and Their Clinical Outcomes in a Tertiary Hospital in Kathmandu Valley, Nepal. Trop. Med. Infect. Dis. 2021, 6, 56. https://doi.org/10.3390/tropicalmed6020056
Raghubanshi BR, Sagili KD, Han WW, Shakya H, Shrestha P, Satyanarayana S, Karki BMS. Antimicrobial Resistance among Neonates with Bacterial Sepsis and Their Clinical Outcomes in a Tertiary Hospital in Kathmandu Valley, Nepal. Tropical Medicine and Infectious Disease. 2021; 6(2):56. https://doi.org/10.3390/tropicalmed6020056
Chicago/Turabian StyleRaghubanshi, Bijendra Raj, Karuna D. Sagili, Wai Wai Han, Henish Shakya, Priyanka Shrestha, Srinath Satyanarayana, and Bal Man Singh Karki. 2021. "Antimicrobial Resistance among Neonates with Bacterial Sepsis and Their Clinical Outcomes in a Tertiary Hospital in Kathmandu Valley, Nepal" Tropical Medicine and Infectious Disease 6, no. 2: 56. https://doi.org/10.3390/tropicalmed6020056
APA StyleRaghubanshi, B. R., Sagili, K. D., Han, W. W., Shakya, H., Shrestha, P., Satyanarayana, S., & Karki, B. M. S. (2021). Antimicrobial Resistance among Neonates with Bacterial Sepsis and Their Clinical Outcomes in a Tertiary Hospital in Kathmandu Valley, Nepal. Tropical Medicine and Infectious Disease, 6(2), 56. https://doi.org/10.3390/tropicalmed6020056