
Lessons Learned and Paths Forward for Rabies Dog Vaccination in Madagascar: A Case Study of Pilot Vaccination Campaigns in Moramanga District

 , ,
, ,
Abstract
1. Introduction
2. Methods
2.1. Study Area
2.2. 2018 Campaign
2.3. 2019 Campaign
2.4. Analyses
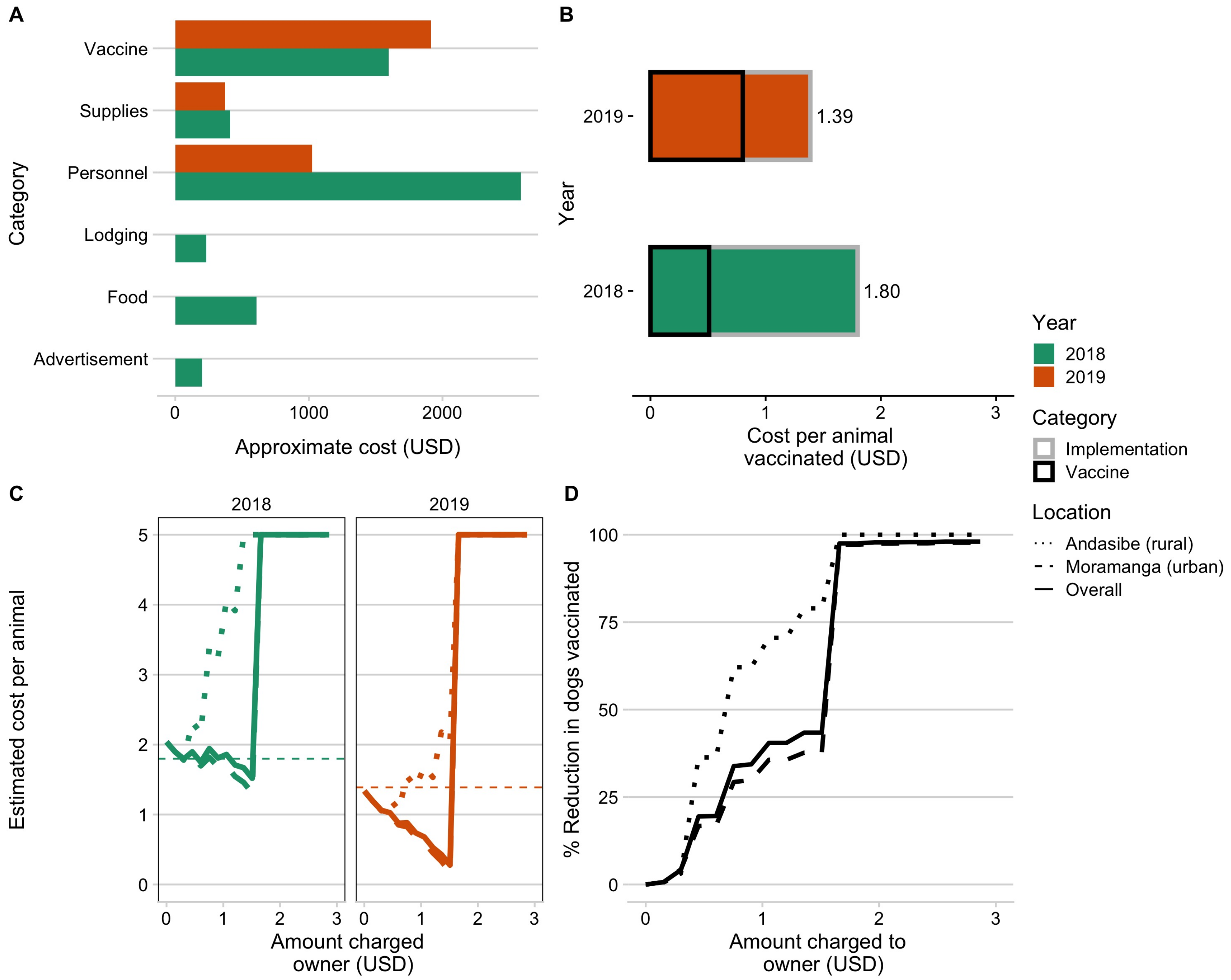
2.4.1. Campaign Resource and Cost Comparisons
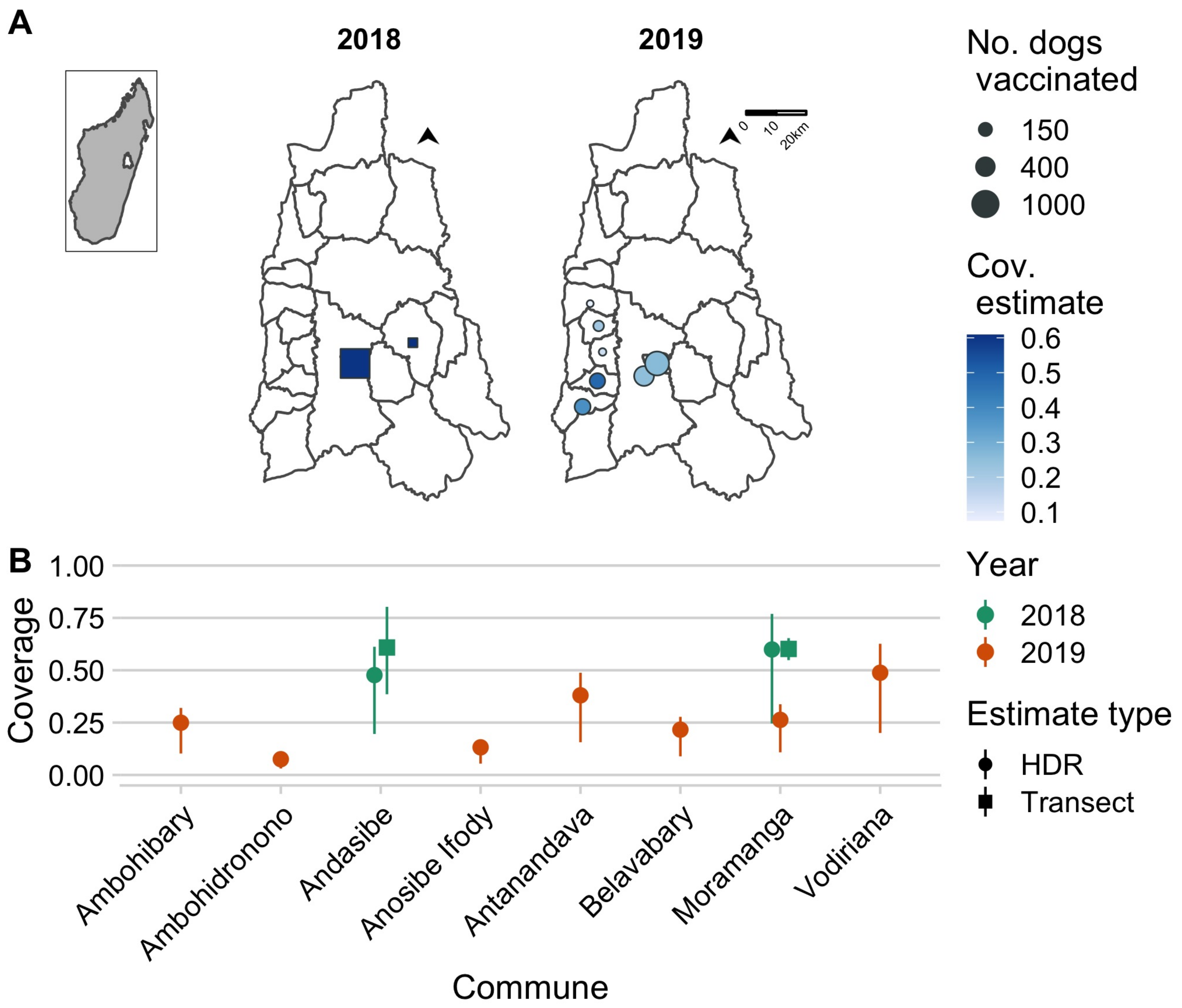
2.4.2. Coverage Estimates
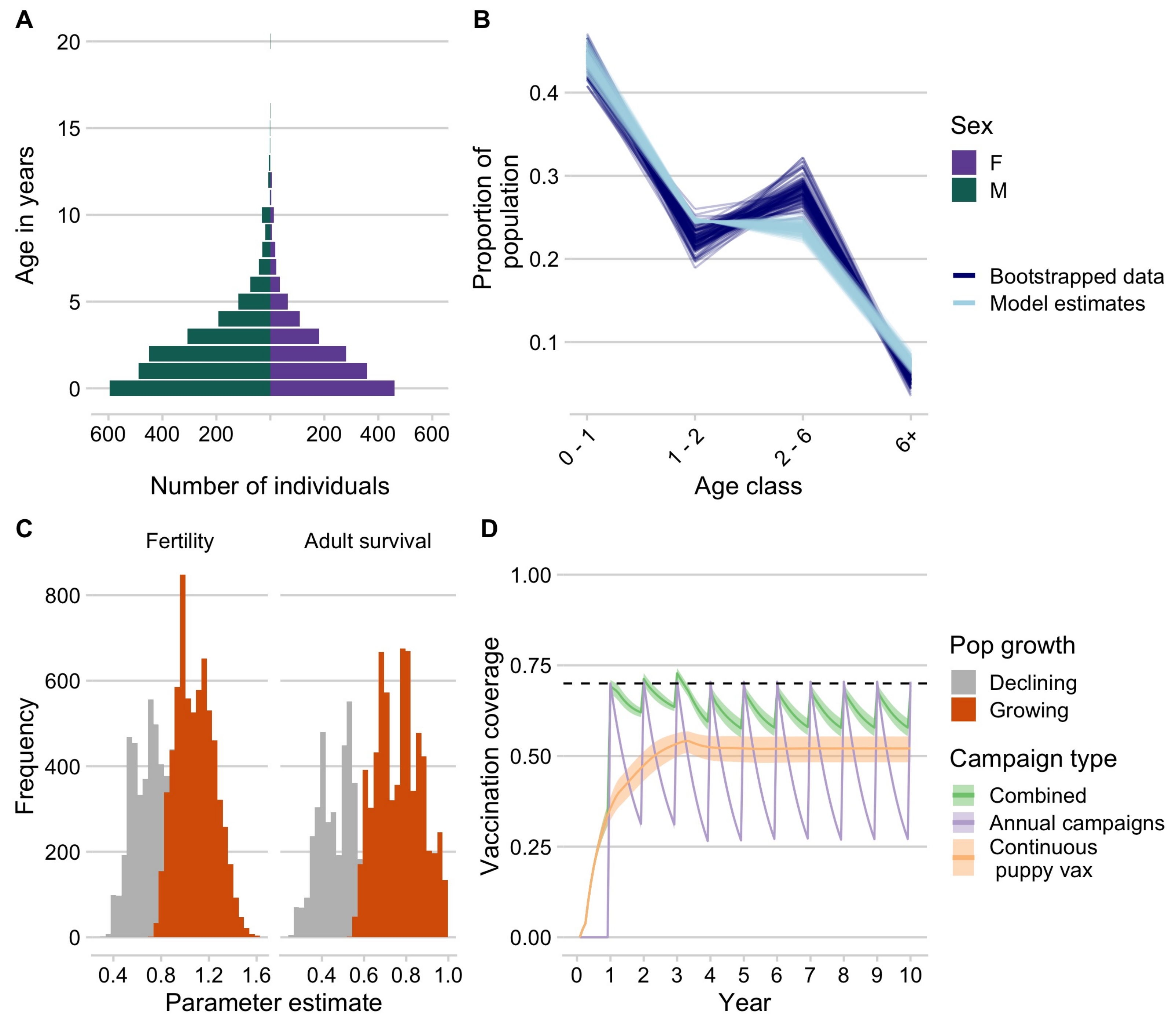
2.4.3. Dog Demography
2.4.4. Modeling Vaccination Campaign Strategies
- (1)
- annual vaccination campaigns occurring within the same month each year targeting dogs of all ages
- (2)
- continuous vaccination of new puppies throughout the year targeting puppies that reach the age of 3 months
- (3)
- a combined approach with annual campaigns (as 1) and routine puppy vaccination (as 2)
2.5. Data and Ethics Statement
3. Results
3.1. Summary of the 2018 and 2019 Campaigns
3.2. Cost Comparison and Willingness to Pay
3.3. Comparing Campaign Coverage Estimates
3.4. Dog Demography and Simulating Vaccination Strategies
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hampson, K.; Coudeville, L.; Lembo, T.; Sambo, M.; Kieffer, A.; Attlan, M.; Barrat, J.; Blanton, J.D.; Briggs, D.J.; Cleaveland, S.; et al. Estimating the global burden of endemic canine rabies. PLoS Negl. Trop. Dis. 2015, 9, e0003709. [Google Scholar]
- Fooks, A.; Banyard, A.; Horton, D.; Johnson, N.; McElhinney, L.; Jackson, A. Current status of rabies and prospects for elimination. Lancet 2014, 384, 1389–1399. [Google Scholar] [CrossRef]
- Abela-Ridder, B.; Knopf, L.; Martin, S.; Taylor, L.; Torres, G.; de Balogh, K. 2016: The beginning of the end of rabies? Lancet Glob. Health 2016, 4, e780–e781. [Google Scholar] [CrossRef]
- World Health Organization. WHO Expert Consultation on Rabies: Third Report; World Health Organization: Geneva, Switzerland, 2018; Volume 1012. [Google Scholar]
- Fahrion, A.; Taylor, L.; Torres, G.; Müller, T.; Dürr, S.; Knopf, L.; de Balogh, K.; Nel, L.; Gordoncillo, M.; Abela-Ridder, B. The Road to Dog Rabies Control and Elimination—What Keeps Us from Moving Faster? Front. Public Health 2017, 5. [Google Scholar] [CrossRef]
- Borse, R.; Atkins, C.; Gambhir, M.; Undurraga, E.; Blanton, J.; Kahn, E.; Dyer, J.; Rupprecht, C.; Meltzer, M. Cost-effectiveness of dog rabies vaccination programs in East Africa. PLoS Negl. Trop. Dis. 2018, 12, e0006490. [Google Scholar] [CrossRef] [PubMed]
- Morters, M.; McKinley, T.; Restif, O.; Conlan, A.; Cleaveland, S.; Hampson, K.; Whay, H.; Damriyasa, I.; Wood, J. The demography of free-roaming dog populations and applications to disease and population control. J. Appl. Ecol. 2014, 51, 1096–1106. [Google Scholar] [CrossRef] [PubMed]
- Jibat, T.; Hogeveen, H.; Mourits, M. Review on Dog Rabies Vaccination Coverage in Africa: A Question of Dog Accessibility or Cost Recovery? PLoS Negl. Trop. Dis. 2015, 9, e0003447. [Google Scholar] [CrossRef]
- Reynes, J.; Andriamandimby, S.; Razafitrimo, G.; Razainirina, J.; Jeanmaire, E.; Bourhy, H.; Heraud, J. Laboratory surveillance of rabies in humans, domestic animals, and bats in madagascar from 2005 to 2010. Adv. Prev. Med. 2011, 2011, 727821. [Google Scholar] [CrossRef] [PubMed]
- Rajeev, M.; Guis, H.; Edosoa, G.; Hanitriniaina, C.; Randrianarijaona, A.; Mangahasimbola, R.; Hierink, F.; Ramiandrasoa, R.; Nely, J.; Heraud, J.; et al. How geographic access to care shapes disease burden: The current impact of post-exposure prophylaxis and potential for expanded access to prevent human rabies deaths in Madagascar. medRxiv 2020. [Google Scholar] [CrossRef]
- Rajeev, M.; Edosoa, G.; Hanitriniaina, C.; Andriamandimby, S.; Guis, H.; Ramiandrasoa, R.; Ratovoson, R.; Randrianasolo, L.; Andriamananjara, M.; Heraud, J.; et al. Healthcare utilization, provisioning of post-exposure prophylaxis, and estimation of human rabies burden in Madagascar. Vaccine 2019, 37, A35–A44. [Google Scholar] [CrossRef] [PubMed]
- Organization Mondiale de la Sante. Evaluation Externe Conjointe des Principales Capacites RSI de la Republique de Madagascar: Resume de Mission, 10 au 14 juillet 2017; Technical Report; Organisation Mondiale de la Sante: Geneva, Switzerland, 2017. [Google Scholar]
- INSTAT-CCER. Resultats Globaux du Recensement General de la Population et de L’habitation de 2018 de Madagascar (RGPH-3): Tableaux Statistiques; Technical Report; INSTAT-CCER: Antananarivo, Madagascar, 2021. [Google Scholar]
- Morters, M.; McNabb, S.; Horton, D.; Fooks, A.; Schoeman, J.; Whay, H.; Wood, J.; Cleaveland, S. Effective vaccination against rabies in puppies in rabies endemic regions. Vet. Rec. 2015, 177, 150. [Google Scholar] [CrossRef] [PubMed]
- Sambo, M.; Johnson, P.; Hotopp, K.; Changalucha, J.; Cleaveland, S.; Kazwala, R.; Lembo, T.; Lugelo, A.; Lushasi, K.; Maziku, M.; et al. Comparing Methods of Assessing Dog Rabies Vaccination Coverage in Rural and Urban Communities in Tanzania. Front. Vet. Sci. 2017, 4, 33. [Google Scholar] [CrossRef] [PubMed]
- Gibson, A.; Ohal, P.; Shervell, K.; Handel, I.; Bronsvoort, B.; Mellanby, R.; Gamble, L. Vaccinate-assess-move method of mass canine rabies vaccination utilising mobile technology data collection in Ranchi, India. BMC Infect. Dis. 2015, 15, 589. [Google Scholar] [CrossRef]
- Mazeri, S.; Burdon Bailey, J.; Mayer, D.; Chikungwa, P.; Chulu, J.; Grossman, P.; Lohr, F.; Gibson, A.; Handel, I.; Bronsvoort, B.; et al. Using data-driven approaches to improve delivery of animal health care interventions for public health. Proc. Natl. Acad. Sci. USA 2021, 118, e2003722118. [Google Scholar] [CrossRef] [PubMed]
- Cleaveland, S.; Kaare, M.; Tiringa, P.; Mlengeya, T.; Barrat, J. A dog rabies vaccination campaign in rural Africa: Impact on the incidence of dog rabies and human dog-bite injuries. Vaccine 2003, 21, 1965–1973. [Google Scholar] [CrossRef]
- Athingo, R.; Tenzin, T.; Coetzer, A.; Hikufe, E.; Peter, J.; Hango, L.; Haimbodi, T.; Lipinge, J.; Haufiku, F.; Naunyango, M.; et al. Application of the GARC Data Logger—A custom-developed data collection device—To capture and monitor mass dog vaccination campaigns in Namibia. PLoS Negl. Trop. Dis. 2020, 14, e0008948. [Google Scholar] [CrossRef] [PubMed]
- Ratsitorahina, M.; Rasambainarivo, J.; Raharimanana, S.; Rakotonandrasana, H.; Andriamiarisoa, M.; Rakalomanana, F.; Richard, V. Dog ecology and demography in Antananarivo, 2007. BMC Vet. Res. 2009, 5, 1–7. [Google Scholar] [CrossRef]
- Leblanc, C. Rabies in Madagascar: A Three-Pronged Survey of Knowledge and Practices among Health Care Providers from Anti-Rabies Treatment Centers, Veterinarians and the Community of Moramanga. Ph.D. Thesis, Cnam de Sante Publique, Paris, France, 2019. [Google Scholar]
- Czupryna, A.; Brown, J.; Bigambo, M.; Whelan, C.; Mehta, S.; Santymire, R.; Lankester, F.; Faust, L. Ecology and Demography of Free-Roaming Domestic Dogs in Rural Villages near Serengeti National Park in Tanzania. PLoS ONE 2016, 11, e0167092. [Google Scholar]
- Davlin, S.; VonVille, H. Canine rabies vaccination and domestic dog population characteristics in the developing world: A systematic review. Vaccine 2012, 30, 3492–3502. [Google Scholar] [CrossRef]
- Fujiwara, M.; Diaz-Lopez, J. Constructing stage-structured matrix population models from life tables: Comparison of methods. PeerJ 2017, 5, e3971. [Google Scholar] [CrossRef] [PubMed]
- Hampson, K.; Dushoff, J.; Cleaveland, S.; Haydon, D.; Kaare, M.; Packer, C.; Dobson, A. Transmission dynamics and prospects for the elimination of canine rabies. PLoS Biol. 2009, 7, e1000053. [Google Scholar] [CrossRef]
- Del Rio Vilas, V.; Freire de Carvalho, M.; Vigilato, M.; Rocha, F.; Vokaty, A.; Pompei, J.; Molina Flores, B.; Fenelon, N.; Cosivi, O. Tribulations of the Last Mile: Sides from a Regional Program. Front. Vet. Sci. 2017, 4. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2020. [Google Scholar]
- Wickham, H.; Averick, M.; Bryan, J.; Chang, W.; McGowan, L.; François, R.; Grolemund, G.; Hayes, A.; Henry, L.; Hester, J.; et al. Welcome to the Tidyverse. J. Open Source Softw. 2019, 4, 1686. [Google Scholar] [CrossRef]
- Pebesma, E. Simple Features for R: Standardized Support for Spatial Vector Data. R J. 2018, 10, 439–446. [Google Scholar] [CrossRef]
- Arief, R.; Hampson, K.; Jatikusumah, A.; Widyastuti, M.; Basri, C.; Putra, A.; Willyanto, I.; Estoepangestie, A.; Mardiana, I.; Kesuma, I.K.G.N.; et al. Determinants of Vaccination Coverage and Consequences for Rabies Control in Bali, Indonesia. Front. Vet. Sci. 2017, 3, 123. [Google Scholar] [CrossRef]
- Sanchez-Soriano, C.; Gibson, A.; Gamble, L.; Bailey, J.; Mayer, D.; Lohr, F.; Chikungwa, P.; Chulu, J.; Handel, I.; Bronsvoort, B.; et al. Implementation of a mass canine rabies vaccination campaign in both rural and urban regions in southern Malawi. PLoS Negl. Trop. Dis. 2020, 14, e0008004. [Google Scholar] [CrossRef] [PubMed]
- Mazeri, S.; Gibson, A.; de Clare Bronsvoort, B.; Handel, I.; Lohr, F.; Bailey, J.; Mayer, D.; Gamble, L.; Mellanby, R. Sociodemographic factors which predict low private rabies vaccination coverage in dogs in Blantyre, Malawi. Vet. Rec. 2019, 184, 281. [Google Scholar] [CrossRef]
- Minyoo, A.; Steinmetz, M.; Czupryna, A.; Bigambo, M.; Mzimbiri, I.; Powell, G.; Gwakisa, P.; Lankester, F. Incentives Increase Participation in Mass Dog Rabies Vaccination Clinics and Methods of Coverage Estimation Are Assessed to Be Accurate. PLoS Negl. Trop. Dis. 2015, 9, e0004221. [Google Scholar] [CrossRef] [PubMed]
- Taylor, L.; Wallace, R.; Balaram, D.; Lindenmayer, J.; Eckery, D.; Mutonono-Watkiss, B.; Parravani, E.; Nel, L. The Role of Dog Population Management in Rabies Elimination—A Review of Current Approaches and Future Opportunities. Front. Vet. Sci. 2017, 4. [Google Scholar] [CrossRef] [PubMed]
- Schildecker, S.; Millien, M.; Blanton, J.; Boone, J.; Emery, A.; Ludder, F.; Fenelon, N.; Crowdis, K.; Destine, A.; Etheart, M.; et al. Dog Ecology and Barriers to Canine Rabies Control in the Republic of Haiti, 2014-2015. Transbound. Emerg. Dis. 2016, 64, 1433–1442. [Google Scholar] [CrossRef]
- Sambo, M.; Lembo, T.; Cleaveland, S.; Ferguson, H.; Sikana, L.; Simon, C.; Urassa, H.; Hampson, K. Knowledge, Attitudes and Practices (KAP) about Rabies Prevention and Control: A Community Survey in Tanzania. PLoS Negl. Trop. Dis. 2014, 8, e3310. [Google Scholar] [CrossRef]
- Barbosa Costa, G.; Ludder, F.; Monroe, B.; Dilius, P.; Crowdis, K.; Blanton, J.; Pieracci, E.; Head, J.; Gibson, A.; Wallace, R. Barriers to attendance of canine rabies vaccination campaigns in Haiti, 2017. Transbound. Emerg. Dis. 2020, 67, 2679–2691. [Google Scholar] [CrossRef]
- Yoak, A.; Haile, A.; O’Quin, J.; Belu, M.; Birhane, M.; Bekele, M.; Murphy, S.; Medley, A.; Vincent, E.; Stewart, D.; et al. Barriers and opportunities for canine rabies vaccination campaigns in Addis Ababa, Ethiopia. Prev. Vet. Med. 2021, 187, 105256. [Google Scholar] [CrossRef] [PubMed]
- Birhane, M.; Miranda, M.; Dyer, J.; Blanton, J.; Recuenco, S. Willingness to Pay for Dog Rabies Vaccine and Registration in Ilocos Norte, Philippines (2012). PLoS Negl. Trop. Dis. 2016, 10, e0004486. [Google Scholar] [CrossRef]
- Mazeri, S.; Gibson, A.; Meunier, N.; Bronsvoort, B.; Handel, I.; Mellanby, R.; Gamble, L. Barriers of attendance to dog rabies static point vaccination clinics in Blantyre, Malawi. PLoS Negl. Trop. Dis. 2018, 12, e0006159. [Google Scholar] [CrossRef] [PubMed]
- Sambo, M.; Hampson, K.; Changalucha, J.; Cleaveland, S.; Lembo, T.; Lushasi, K.; Mbunda, E.; Mtema, Z.; Sikana, L.; Johnson, P. Estimating the size of dog populations in Tanzania to inform rabies control. Vet. Sci. 2018, 5, 77. [Google Scholar] [CrossRef] [PubMed]
- Conan, A.; Akerele, O.; Simpson, G.; Reininghaus, B.; van Rooyen, J.; Knobel, D. Population Dynamics of Owned, Free-Roaming Dogs: Implications for Rabies Control. PLoS Negl. Trop. Dis. 2015, 9, e0004177. [Google Scholar] [CrossRef] [PubMed]
- Undurraga, E.; Millien, M.; Allel, K.; Etheart, M.; Cleaton, J.; Ross, Y.; Wallace, R.; Crowdis, K.; Medley, A.; Vos, A.; et al. Costs and effectiveness of alternative dog vaccination strategies to improve dog population coverage in rural and urban settings during a rabies outbreak. Vaccine 2020, 38, 6162–6173. [Google Scholar] [CrossRef]
- Ferguson, A.; Muloi, D.; Ngatia, D.; Kiongo, W.; Kimuyu, D.; Webala, P.; Olum, M.; Muturi, M.; Thumbi, S.; Woodroffe, R.; et al. Volunteer based approach to dog vaccination campaigns to eliminate human rabies: Lessons from Laikipia County, Kenya. PLoS Negl. Trop. Dis. 2020, 14, e0008260. [Google Scholar] [CrossRef]
- Lugelo, A.; Hampson, K.; Bigambo, M.; Kazwala, R.; Lankester, F. Controlling Human Rabies: The Development of an Effective, Inexpensive and Locally Made Passive Cooling Device for Storing Thermotolerant Animal Rabies Vaccines. Trop. Med. Infect. Dis. 2020, 5, 130. [Google Scholar] [CrossRef]
- Gibson, A.; Handel, I.; Shervell, K.; Roux, T.; Mayer, D.; Muyila, S.; Maruwo, G.; Nkhulungo, E.; Foster, R.; Chikungwa, P.; et al. The Vaccination of 35,000 Dogs in 20 Working Days Using Combined Static Point and Door-to-Door Methods in Blantyre, Malawi. PLoS Negl. Trop. Dis. 2016, 10, e0004824. [Google Scholar] [CrossRef] [PubMed]
- Lushasi, K.; Steenson, R.; Bernard, J.; Changalucha, J.; Govella, N.; Haydon, D.; Hoffu, H.; Lankester, F.; Magoti, F.; Mpolya, E.; et al. One Health in Practice: Using Integrated Bite Case Management to Increase Detection of Rabid Animals in Tanzania. Front. Public Health 2020, 8. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 2018 | 2019 | |||
|---|---|---|---|---|
| Andasibe | Moramanga Ville | All Communes | All Communes | |
| Total animals vaccinated | 528 | 2609 | 3137 | 2385 |
| Total dogs vaccinated | 254 | 1803 | 2057 | 1898 |
| Dogs with history of vaccination | 5% | 16% | 15% | 13% |
| Dogs vaccinated within last year | 5% | 7% | 7% | 13% |
| Percent male dogs | 55% | 56% | 56% | 65% |
| Average dogs per owner | 0.8 | 1.1 | 1.0 | – |
| Percent of owners with free-roaming dogs | 67% | 19% | 28% | – |
| Animals vaccinated per day (total days) | 88 (6) | 372.7 (7) | 241.3 (13) | 49.7 (48) |
| Animals vaccinated per vaccination point (total points) | 75.4 (7) | 186.4 (14) | 149.4 (21) | 37.3 (64) |
| Animals vaccinated per person day (total person days) | 11.7 (45) | 21.6 (121) | 18.9 (166) | 49.7 (48) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Filla, C.; Rajeev, M.; Randriana, Z.; Hanitriniana, C.; Rafaliarison, R.R.; Edosoa, G.T.; Andriamananjara, M.; Razafindraibe, N.P.; Nely, J.; Ferreira, A.; et al. Lessons Learned and Paths Forward for Rabies Dog Vaccination in Madagascar: A Case Study of Pilot Vaccination Campaigns in Moramanga District. Trop. Med. Infect. Dis. 2021, 6, 48. https://doi.org/10.3390/tropicalmed6020048
Filla C, Rajeev M, Randriana Z, Hanitriniana C, Rafaliarison RR, Edosoa GT, Andriamananjara M, Razafindraibe NP, Nely J, Ferreira A, et al. Lessons Learned and Paths Forward for Rabies Dog Vaccination in Madagascar: A Case Study of Pilot Vaccination Campaigns in Moramanga District. Tropical Medicine and Infectious Disease. 2021; 6(2):48. https://doi.org/10.3390/tropicalmed6020048
Chicago/Turabian StyleFilla, Caitlynn, Malavika Rajeev, Zoavina Randriana, Chantal Hanitriniana, Radoniaina R. Rafaliarison, Glenn Torrencelli Edosoa, Mamitiana Andriamananjara, Nivohanitra P. Razafindraibe, José Nely, Angelique Ferreira, and et al. 2021. "Lessons Learned and Paths Forward for Rabies Dog Vaccination in Madagascar: A Case Study of Pilot Vaccination Campaigns in Moramanga District" Tropical Medicine and Infectious Disease 6, no. 2: 48. https://doi.org/10.3390/tropicalmed6020048
APA StyleFilla, C., Rajeev, M., Randriana, Z., Hanitriniana, C., Rafaliarison, R. R., Edosoa, G. T., Andriamananjara, M., Razafindraibe, N. P., Nely, J., Ferreira, A., Yang, A. L., Daniel, F., Clarke, T. A., Farris, Z., Stone, T., Lastdrager, J., Rajaonarivelo, T., Hampson, K., Metcalf, C. J. E., & Valenta, K. (2021). Lessons Learned and Paths Forward for Rabies Dog Vaccination in Madagascar: A Case Study of Pilot Vaccination Campaigns in Moramanga District. Tropical Medicine and Infectious Disease, 6(2), 48. https://doi.org/10.3390/tropicalmed6020048