Cost of Caregivers for Treating Hospitalized Diarrheal Patients in Bangladesh

 , ,
, ,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Design and Study Population
2.2. Cost Estimates
2.3. Data Collection
2.4. Data Analysis
2.5. Ethical Approval
3. Results
3.1. Background Characteristics of Study Participants
3.2. Average Caregivers’ Cost
3.3. Distribution of Caregivers’ Cost by Socio-Demographic Characteristics
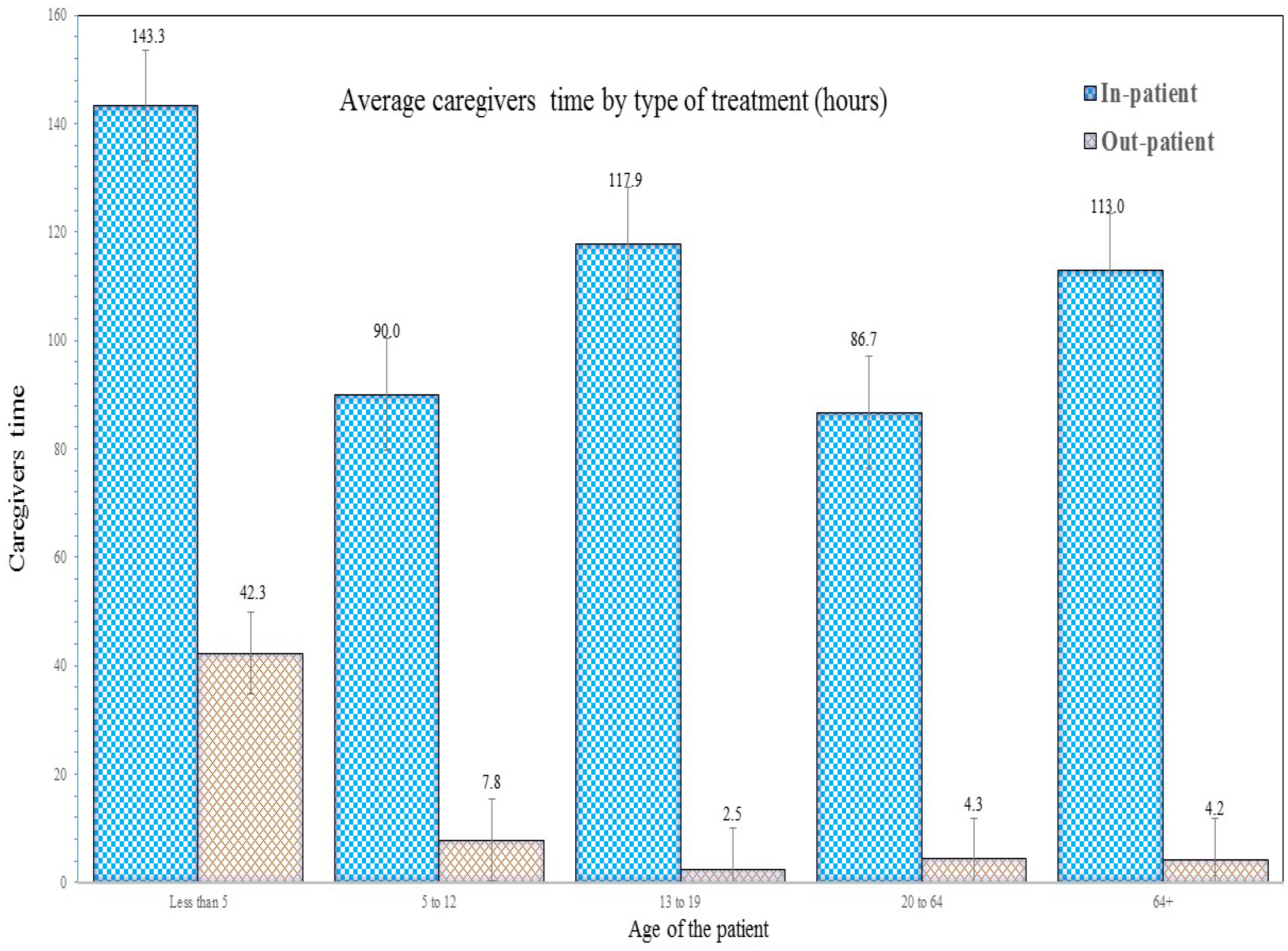
3.4. Caregivers’ Time
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Fullman, N.; Yearwood, J.; Abay, S.M.; Abbafati, C.; Abd-Allah, F.; Abdela, J.; Zuhlke, L.J.; Murray, C.J.L.; Lozano, R. Measuring performance on the Healthcare Access and Quality Index for 195 countries and territories and selected subnational locations: A systematic analysis from the Global Burden of Disease Study 2016. Lancet 2018. [Google Scholar] [CrossRef]
- Vos, T.; Allen, C.; Arora, M.; Barber, R.M.; Bhutta, Z.A.; Brown, A.; Zhou, M.; Zodpey, S.; Liesl, J.; Murray, C.J.L. Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1545–1602. [Google Scholar] [CrossRef]
- UNICEF. Diarrhoea Remains a Leading Killer of Young Children, Despite the Availability of a Simple Treatment Solution. In UNICEF DATA: Monitoring the Situation of Children and Women. 2016, p. 1. Available online: http://data.unicef.org/child-health/diarrhoeal-disease.html (accessed on 28 June 2016).
- Mashoto, K.O.; Malebo, H.M.; Msisiri, E.; Peter, E. Prevalence, one week incidence and knowledge on causes of diarrhea: Household survey of under-fives and adults in Mkuranga district, Tanzania. BMC Public Health 2014, 14, 985. [Google Scholar] [CrossRef] [PubMed]
- MOHFW. Health Bulletin 2017; MOHFW: Dhaka, Bangladesh, 2017. Available online: www.dghs.gov.bd (accessed on 15 November 2018).
- Bangladesh Bureau of Statistics. Health and Morbidity Status Survey—2012; Bangladesh Bureau of Statistics: Dhaka, Bangladesh, 2013.
- Streatfield, P.K.; Baumgartner, J. Bangladesh Urban Health Survey. Dhaka, Bangladesh, 2013. Available online: http://www.niport.gov.bd/wp-content/uploads/download/1413705060-UHS2013Preliminary Results.pdf (accessed on 15 November 2018).
- Drasar, B.S.; Tomkins, A.M.; Feacham, R.G. Seasonal Aspects of Diarrhoeal Disease. Seasonal Dimensions to Rural Poverty; Report to UK Overseas Development Association; London School of Hygiene and Tropical Medicine: London, UK, 1978. [Google Scholar]
- Black, R.E.; Lanata, C.F. Epidemiology of diarrhoeal diseases in developing countries. In Infections of the Gastrointestinal Tract; Blaser, M.J., Smith, P.D., Ravdin, J.I., Greenberg, H.P., Guerrant, R.I., Eds.; Raven Press: New York, NY, USA, 1995. [Google Scholar]
- Ozguler, M. Febril Neutropenia: An Approach as an Infectious Disease Specialist; Scientific Research Publishing, Inc.: Wuhan, China, 2015; Available online: www.scirp.org (accessed on 15 November 2018).
- Deen, J.L.; Seidlein, L.; Sur, D.; Agtini, M.; Lucas, M.; Lopez, A.N.; Lopez, L.; Deok, R.K.; Ali, M.; Clemens, J.D. The High Burden of Cholera in Children: Comparison of Incidence from Endemic Areas in Asia and Africa. PLoS Negl. Trop. Dis. 2008, 2. [Google Scholar] [CrossRef] [PubMed]
- Rabbani, G.H.; Larson, C.P.; Islam, R.; Saha, U.R.; Kabir, A. Green banana-supplemented diet in the home management of acute and prolonged diarrhoea in children: A community-based trial in rural Bangladesh. Trop. Med. Int. Health 2010, 15, 1132–1139. [Google Scholar] [CrossRef] [PubMed]
- Lamberti, L.M.; Walker, F.C.L.; Black, R. Systematic review of diarrhea duration and severity in children and adults in low- and middle-income countries. BMC Public Health 2012, 12, 2–11. [Google Scholar] [CrossRef]
- Gebru, T.; Taha, M.; Kassahun, W. Risk factors of diarrhoeal disease in under-five children among health extension model and non-model families in Sheko district rural community, Southwest Ethiopia: Comparative cross-sectional study. BMC Public Health 2014, 14, 395. [Google Scholar] [CrossRef] [PubMed]
- Sultana, M.; Mahumud, R.A.; Sarker, A.R. Emerging Patterns of Mortality and Morbidity in District Level Hospitals in Bangladesh. Ann. Public Health Res. 2015, 2, 2–4. [Google Scholar]
- Shillcutt, S.D.; Lefevre, A.E.; Walker, C.L.F.; Taneja, S.; Black, R.E.; Mazumder, S. Economic costs to caregivers of diarrhoea treatment among children below 5 in rural Gujarat India: Findings from an external evaluation of the DAZT programme. Health Policy Plan. 2016, 31, 1411–1422. [Google Scholar] [CrossRef] [PubMed]
- Sarker, A.R.; Sultana, M.; Mahumud, R.A.; Ali, N.; Huda, T.M.; Salim uzzaman, M.; Haider, S.; Rahman, H.; Islam, Z.; Khan, J.A.M.; et al. Economic costs of hospitalized diarrheal disease in Bangladesh: A societal perspective. Glob. Health Res. Policy 2018, 3, 1. [Google Scholar] [CrossRef]
- Sarker, A.R.; Sultana, M.; Mahumud, R.A.; Sheikh, N.; Van Der Meer, R.; Morton, A. Prevalence and Health Care–Seeking Behavior for Childhood Diarrheal Disease in Bangladesh. Glob. Pediatr. Health 2016, 3, 2333794X1668090. [Google Scholar] [CrossRef] [PubMed]
- Yaprak, S.; Bulut, U.; Okudan, Y.E.; Gokdemir, O.; Colak, M.; Yıldırım, E.; Guldal, D. Caregiver reasons for tertiary health-care seeking for children aged ≤12 years. Pediatr. Int. 2016, 58, 1037–1041. [Google Scholar] [CrossRef] [PubMed]
- Burke, R.M.; Rebolledo, P.A.; Embrey, S.R.; Wagner, L.D.; Cowden, C.L.; Kelly, F.M.; Smith, E.R.; Iñiguez, V.; Leon, J.S. The burden of pediatric diarrhea: A cross-sectional study of incurred costs and perceptions of cost among Bolivian families. BMC Public Health 2013, 13, 708. [Google Scholar] [CrossRef] [PubMed]
- Kosek, M.; Bern, C.; Guerrant, R.L. The global burden of diarrhoeal disease, as estimated from studies published between 1992 and 2000. Bull. World Health Organ. 2003, 81, 197–204. [Google Scholar] [CrossRef] [PubMed]
- Bartsch, S.M.; Lee, B.Y. Economics and financing of vaccines for diarrheal diseases. Hum. Vaccine Immunother. 2014, 10, 1568–1581. [Google Scholar] [CrossRef]
- MacIntyre, U.; Villiers, F. Economic Burden of Diarrheal Disease in a Tertiary Level Hospital, Gauteng, South Africa. J. Infect. Dis. 2010, 202, 116–125. [Google Scholar] [CrossRef] [PubMed]
- Bhuiyan, M.U.; Luby, S.P.; Zaman, R.U.; Rahman, M.W.; Sharker, M.A.Y.; Hossain, M.J.; Rasul, C.H.; Ekram, A.R.M.S.; Rahman, M.; Sturm-Ramirez, K.; et al. Incidence of and Risk Factors for Hospital-Acquired Diarrhea in Three Tertiary Care Public Hospitals in Bangladesh. Am. J. Trop. Med. Hyg. 2014, 91, 165–172. [Google Scholar] [CrossRef] [PubMed]
- Pham-Duc, P.; Nguyen-Viet, H.; Hattendorf, J.; Cam, P.D.; Zurbrügg, C.; Zinsstag, J.; Odermatt, P. Diarrhoeal diseases among adult population in an agricultural community Hanam province, Vietnam, with high wastewater and excreta re-use. BMC Public Health 2014, 14, 978. [Google Scholar] [CrossRef]
- Ali, Q.L. Calculation of Total Unit Cost for Diarrhoeal Management at District and Thana Health Complex; Ministry of Health and Family Welfare: Dhaka, Bangladesh, 2001.
- Das, J.; Das, S.K.; Ahmed, S.; Ferdous, F.; Farzana, F.D.; Sarker, M.H.R.; Ahmed, M.S.; Chisti, M.J.; Malek, M.; Rahman, A.; et al. Determinants of percent expenditure of household income due to childhood diarrhoea in rural Bangladesh. Epidemiol. Infect. 2015, 143, 2700–2706. [Google Scholar] [CrossRef] [PubMed]
- Chitunhu, S.; Musenge, E. Direct and indirect determinants of childhood malaria morbidity in Malawi: A survey cross—Sectional analysis based on malaria indicator survey data for 2012. Malaria J. 2015, 14, 265. [Google Scholar] [CrossRef] [PubMed]
- Sur, D.; Chatterjee, S.; Riewpaiboon, A.; Manna, B.; Kanungo, S.; Bhattacharya, S.K. Treatment cost for typhoid fever at two hospitals in Kolkata, India. J. Health Popul. Nutr. 2009, 27, 725–732. [Google Scholar] [PubMed]
- Poulos, C.; Riewpaiboon, A.; Stewart, J.F.; Clemens, J.; Guh, S.; Agtini, M.; Sur, D.; Islam, Z.; Lucas, M.; Whittington, D. Costs of illness due to endemic cholera. Epidemiol. Infect. 2012, 140, 500–509. [Google Scholar] [CrossRef] [PubMed]
- Drummond, M.; Sculpher, M.J.; Laxton, K.C.; Stoddart, G.L.; Torrance, G.W. Methods for the Economic Evaluation of Health Care Programmes, 3rd ed.; Oxford University Press: Oxford, UK, 2005. [Google Scholar]
- Van Roijen, L.; Essink-Bot, M.L.; Koopmanschap, M.A.; Bonsel, G.; Rutten, F.F. Labor and health status in economic evaluation of health care. The Health and Labor Questionnaire. Int. J. Technol. Assess. Health Care 1996, 12, 405–415. [Google Scholar] [CrossRef]
- Sarker, A.R.; Islam, Z.; Khan, I.A.; Saha, A.; Chowdhury, F.; Khan, A.I.; Qadri, F.; Khan, J.A.M. Cost of illness for cholera in a high risk urban area in Bangladesh: An analysis from household perspective. BMC Infect. Dis. 2013, 13, 518. [Google Scholar] [CrossRef] [PubMed]
- Rice, D.P. Estimating cost of illness. Am. J. Public Health Nations Health 1967, 57, 424–440. [Google Scholar] [CrossRef] [PubMed]
- Chima, R.I.; Goodman, C.A.; Mills, A. The economic impact of malaria in Africa: A critical review of the evidence. Health Policy 2003, 63, 17–36. [Google Scholar] [CrossRef]
- GOB. Monthly Report on Fiscal-Macro Position. Dhaka, Bangladesh, 2016. Available online: http://www.mof.gov.bd/en/budget/mfmu/mfmu_February_16.pdf (accessed on 15 November 2018).
- Alwin, J.; Öberg, B.; Krevers, B. Support/services among family caregivers of persons with dementia—Perceived importance and services received. Int. J. Geriatr. Psychiatry 2010, 25, 240–248. [Google Scholar] [CrossRef]
- Chaudhuri, J.D.; Das, S. The role of caregivers in the management of alzheimer’s disease: Examples from Asian countries. Sultan Qaboos Univ. Med. J. 2006, 6, 11–18. [Google Scholar]
- Haro, J.M.; Kahle-Wrobleski, K.; Bruno, G.; Belger, M.; Dell’Agnello, G.; Dodel, R.; Jones, R.W.; Reed, C.C.; Vellas, B.; Wimo, A.; et al. Analysis of burden in caregivers of people with Alzheimer’s disease using self-report and supervision hours. J. Nutr. Aging 2014, 18, 677–684. [Google Scholar] [CrossRef]
- Rheingans, R.; Kukla, M.; Faruque, A.S.G.; Sur, D.; Zaidi, A.K.M.; Nasrin, D.; Farag, T H.; Levine, M.; Kotloff, K. Determinants of Household Costs Associated With Childhood Diarrhea in 3 South Asian Settings. Clin. Infect. Dis. 2012, 55, 327–335. [Google Scholar] [CrossRef]
- Sultana, S.; Ahmed, S.; Hossen, S.S. Diarrhoeal Diseases in the Slums of Khulna City: Prevalence and Cost Analysis. J. Asian Dev. Stud. 2013, 2, 60–70. [Google Scholar]
- Halim, F.B.; Haider, M.Z. Prevalence and economic costs of diarrheal illness among adult slum dwellers in Khulna City, Bangladesh. J. Health Soc. Sci. 2017, 120, 83–98. [Google Scholar] [CrossRef]
- MOHFW. Bangladesh National Health Accounts 1997–2015: Preliminary Results; MOHFW: Dhaka, Bangladesh, 2015. Available online: http://www.thedailystar.net/backpage/people-fork-out-most-1465246 (accessed on 15 November 2018).
- Poulos, C.; Riewpaiboon, A.; Stewart, J.F.; Clemens, J.; Guh, S.; Agtini, M.; Anh, D.D.; Dong, B.; Bhutta, Z.; Sur, D.; et al. Cost of illness due to typhoid fever in five Asian countries. Trop. Med. Int. Health 2011, 16, 314–323. [Google Scholar] [CrossRef] [PubMed]
- Sarker, A.R.; Sultana, M.; Mahumud, R.A.; Van Der Meer, R.; Morton, A.; Sarker, A.R. Cost-effectiveness analysis of introducing universal childhood rotavirus vaccination in Bangladesh. Hum. Vaccines Immunother. 2017, 14, 189–198. [Google Scholar] [CrossRef]
- IVI. Country Investment Case Study on Cholera Vaccination: Bangladesh; IVI: Seoul, Korea, 2013; Available online: http://www.ivi.int/web/www/0403 (accessed on 15 November 2018).
- Chowdhury, F.; Khan, I.A.; Patel, S.; Siddiq, A.U.; Saha, N.C.; Khan, A.I.; Saha, A.; Cravioto, A.; Clemens, J.; Qadri, F.; et al. Diarrheal illness and healthcare seeking behavior among a population at high risk for diarrhea in Dhaka, Bangladesh. PLoS ONE 2015, 10, e0130105. [Google Scholar] [CrossRef]
- Bhutta, Z.A.; Das, J.K.; Walker, N.; Rizvi, A.; Campbell, H.; Rudan, I.; Black, R.E. Interventions to address deaths from childhood pneumonia and diarrhoea equitably: What works and at what cost? Lancet 2013, 381, 1417–1429. [Google Scholar] [CrossRef]
- Diouf, K.; Tabatabai, P.; Rudolph, J.; Marx, M. Diarrhoea prevalence in children under five years of age in rural Burundi: An assessment of social and behavioural factors at the household level. Glob. Health Act. 2014, 7, 24895. [Google Scholar] [CrossRef]
- Ejemot-Nwadiaro, R.I.; Ehiri, J.E.; Arikpo, D.; Meremikwu, M.M.; Critchley, J.A. Hand washing promotion for preventing diarrhoea. Cochrane Database Syst Rev. 2015. [Google Scholar] [CrossRef]
- Clasen, T.; Roberts, I.; Rabie, T.; Schmidt, W.; Cairncross, S. Interventions to improve water quality for preventing diarrhoea. Cochrane Database Syst. Rev. 2006, 3, CD004794. [Google Scholar]
- Cairncross, S.; Hunt, C.; Boisson, S.; Bostoen, K.; Curtis, V.; Fung, I.C.H.; Schmidt, W.P. Water, sanitation and hygiene for the prevention of diarrhoea. Int. J. Epidemiol. 2010, 39, i193–i205. [Google Scholar] [CrossRef]
- Ruxin, J.N. Magic bullet: The history of oral rehydration therapy. Med. Hist. 1994, 38, 363–397. [Google Scholar] [CrossRef] [PubMed]
- Munos, M.K.; Fischer Walker, C.L.; Black, R.E. The effect of oral rehydration solution and recommended home fluids on diarrhoea mortality. Int. J. Epidemiol. 2010, 39, i75–i87. [Google Scholar] [CrossRef] [PubMed]
- WHO Collaborative Study Team. Effect of breastfeeding on infant and child mortality due to infectious diseases in less developed countries: A pooled analysis. Lancet 2000, 355, 451–455. [Google Scholar] [CrossRef]
- Jones, G.; Steketee, R.W.; Black, R.E.; Bhutta, Z.A.; Morris, S.S. How many child deaths can we prevent this year? Lancet 2003, 362, 65–71. [Google Scholar] [CrossRef]
- Levine, M.M.; Kotloff, K.L.; Nataro, J.P.; Muhsen, K. The Global Enteric Multicenter Study (GEMS): Impetus, rationale, and genesis. Clin. Infect. Dis. 2012, 55, 215–224. [Google Scholar] [CrossRef]
- Fischer Walker, C.L.; Rudan, I.; Liu, L.; Nair, H.; Theodoratou, E.; Bhutta, Z.A.; O’Brien, K.L.; Campbell, H.; Black, R.E. Global burden of childhood pneumonia and diarrhoea. Lancet 2013, 381, 1405–1416. [Google Scholar] [CrossRef]
- Das, S.K.; Begum, D.; Ahmed, S.; Ferdous, F.; Farzana, F.D.; Chisti, M.J.; Latham, J.R.; Talukder, K.A.; Rahman, M.M.; et al. Geographical diversity in seasonality of major diarrhoeal pathogens in Bangladesh observed between 2010 and 2012. Epidemiol. Infect. 2014, 142, 2530–2541. [Google Scholar] [CrossRef] [PubMed]
- Aikins, M.; Armah, G.; Akazili, J.; Hodgson, A. Hospital health care cost of diarrheal disease in Northern Ghana. J. Infect. Dis. 2010, 202 (Suppl. 1), S126–S130. [Google Scholar] [CrossRef]


{kind=link}
| Variables | n or mean | % or SD | 95% CI |
|---|---|---|---|
| Patient age in years (%) | |||
| Less than 5 | 460 | 57.43 | (53.97, 60.82) |
| 5 to 12 | 52 | 6.49 | (04.98, 08.43) |
| 13 to 19 | 38 | 4.74 | (03.47, 06.46) |
| 20 to 64 | 199 | 24.84 | (21.97, 27.96) |
| 64+ | 52 | 6.49 | (04.98, 08.43) |
| Gender (%) | |||
| Male | 404 | 50.44 | (46.97, 53.90) |
| Female | 397 | 49.56 | (46.10, 53.03) |
| Types of patient (%) | |||
| Inpatient | 404 | 50.44 | (46.97, 53.90) |
| Outpatient | 397 | 49.56 | (46.10, 53.03) |
| Patient education (%) | |||
| Not applicable (Child < 5 years) | 458 | 57.18 | (53.72, 60.57) |
| No formal education | 95 | 11.86 | (09.79, 14.29) |
| Up to primary | 112 | 13.98 | (11.74, 16.57) |
| Secondary | 103 | 12.86 | (10.71, 15.37) |
| Higher | 33 | 4.12 | (02.94, 05.74) |
| Patient occupation (%) | |||
| Not applicable (Child < 5 years) | 458 | 57.18 | (53.72, 60.57) |
| Housewife | 130 | 16.23 | (13.83, 18.95) |
| Students | 83 | 10.36 | (08.43, 12.68) |
| Self-employment | 49 | 6.12 | (04.65, 08.01) |
| Unemployed | 7 | 0.87 | (00.42, 01.82) |
| Salaried employee | 31 | 3.87 | (02.73, 05.45) |
| Business | 18 | 2.25 | (01.42, 03.54) |
| Others | 25 | 3.12 | (02.12, 04.58) |
| Mother education level (%) | |||
| No formal education | 270 | 33.71 | (30.51, 37.06) |
| Up to primary | 199 | 24.84 | (21.97, 27.96) |
| Secondary | 274 | 34.21 | (30.99, 37.57) |
| Higher | 58 | 7.24 | (05.64, 09.26) |
| Father education level (%) | |||
| No formal education | 278 | 34.71 | (31.48, 38.08) |
| Up to primary | 191 | 23.85 | (21.01, 26.93) |
| Secondary | 241 | 30.09 | (27.00, 33.36) |
| Higher | 91 | 11.36 | (09.34, 13.76) |
| Patient-respondent relationship (%) | |||
| Parent | 509 | 63.55 | (60.14, 66.82) |
| Sibling | 17 | 2.12 | (01.32, 03.39) |
| Grandparent | 17 | 2.12 | (01.32, 03.39) |
| Relative | 29 | 3.62 | (02.53, 05.17) |
| Spouse | 52 | 6.49 | (04.98, 08.43) |
| Offspring | 49 | 6.12 | (04.65, 08.01) |
| Others (i.e., neighbour, friend, self) | 128 | 15.98 | (13.60, 18.69) |
| Caregivers occupation (considered multiple responses) | |||
| Housewife | 702 | 90.00 | - |
| Students | 73 | 09.36 | - |
| Self-employment | 114 | 14.62 | - |
| Unemployed | 31 | 03.97 | - |
| Salaried employee | 103 | 13.21 | - |
| Business | 118 | 15.13 | - |
| Others | 130 | 16.67 | - |
| Household size (%) | |||
| Less than 3 | 32 | 4.00 | (02.84, 05.60) |
| 3 to 5 | 458 | 57.18 | (53.72, 60.57) |
| More than 5 | 311 | 38.83 | (35.50, 42.26) |
| Household size (Mean, SD) | 5.59 | 02.93 | (05.59, 02.93) |
| Patient household monthly income in BDT (Mean, SD) | 19,603 | 26,642 | (17,756, 21,451) |
| Patient household monthly expenditure in BDT (Mean, SD) | 15,470 | 10,702 | (14,727, 16,212) |
| Overall healthcare expenditure last 3 months in BDT (Mean, SD) | 5191 | 17,745 | (3961, 6422) |
| Income quintile in BDT (Mean, SD) | |||
| Poorest quintile | 190 | 7042 | (6786, 7298) |
| 2nd | 168 | 10,938 | (10,789, 11,086) |
| 3rd | 123 | 14,638 | (14,513, 14,763) |
| 4th | 178 | 20,288 | (19,893, 20,683) |
| Upper quintile | 142 | 50,106 | (41,466, 58,746) |
| Cost | Parameter | Overall Cost | Inpatient Cost | Outpatient Cost | |||
|---|---|---|---|---|---|---|---|
| Average | SD | Average | SD | Average | SD | ||
| Out-of-pocket cost | Transportation cost | 123.29 (01.57) | 213.88 (02.72) | 189.18 (02.41) | 242.4 (03.09) | 56.24 (0.72) | 153.89 (01.96) |
| Informal payment (e.g., tips) | 07.40 (0.09) | 22.65 (0.29) | 14.23 (0.18) | 29.94 (0.38) | 0.45 (0.01) | 05.35 (0.07) | |
| Caregiver’s payment | 0.01 (0.00) | 0.35 (0.00) | 0.00 (0.00) | 0.00 (0.00) | 0.03 (0.00) | 0.50 (0.01) | |
| Caregivers expenditure (e.g., food, lodging) | 127.87 (01.63) | 456.8 (05.82) | 228.99 (02.92) | 438.94 (05.59) | 24.97 (0.32) | 452.15 (05.76) | |
| Total direct cost | 258.57 (03.29) | 541.07 (06.89) | 432.4 (05.51) | 542.34 (06.91) | 81.69 (01.04) | 479.48 (06.11) | |
| In-direct cost | Caregivers income loss | 1985.21 (25.29) | 2467.44 (31.43) | 3057.31 (38.95) | 2540.84 (32.37) | 894.2 (11.39) | 1834.02 (23.36) |
| Total cost | 2243.38 (28.58) | 2756.87 (35.12) | 3489.67 (44.45) | 2789.05 (35.53) | 975.11 (12.42) | 2059.31 (26.23) | |
| Variables | In-Patients | Out-Patients | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Total Cost | Direct | Indirect | Total Cost | Direct | Indirect | |||||||
| Average | SD | Average | SD | Average | SD | Average | SD | Average | SD | Average | SD | |
| Patient age in years | ||||||||||||
| Less than 5 | 4407 (56.14) | 2639 (33.62) | 558 (7.11) | 566 (7.21) | 3848 (49.02) | 2400 (30.57) | 1173 (14.94) | 2256 (28.74) | 94 (1.20) | 535 (6.82) | 1079 (13.75) | 2006 (25.55) |
| 5 to 12 | 2529 (32.22) | 1619 (20.62) | 411 (5.24) | 532 (6.78) | 2119 (26.99) | 1563 (19.91) | 246 (3.13) | 230 (2.93) | 34 (0.43) | 43 (0.55) | 212 (2.70) | 217 (2.76) |
| 13 to 19 | 3405 (43.38) | 2884 (36.74) | 261 (3.32) | 305 (3.89) | 3144 (40.05) | 2808 (35.77) | 58 (0.74) | 98 (1.25) | 34 (0.43) | 25 (0.32) | 44 (0.56) | 72 (0.92) |
| 20 to 64 | 2714 (34.57) | 2741 (34.92) | 318 (4.05) | 388 (4.94) | 2396 (30.52) | 2525 (32.17) | 132 (1.68) | 159 (2.03) | 40 (0.51) | 35 (0.45) | 110 (1.40) | 128 (1.63) |
| 64+ | 3777 (48.11) | 2833 (36.09) | 568 (7.24) | 852 (10.85) | 3209 (40.88) | 2441 (31.10) | 130 (1.66) | 183 (2.33) | 40 (0.51) | 18 (0.23) | 110 (1.40) | 155 (1.97) |
| P-value | <0.001 | <0.001 | <0.001 | <0.001 | 0.89 | <0.001 | ||||||
| Gender | ||||||||||||
| Male | 3616 (46.06) | 3081 (39.25) | 437 (5.56) | 616 (7.85) | 3179 (40.50) | 2774 (35.33) | 953 (12.14) | 1896 (24.15) | 67 (0.85) | 213 (2.71) | 887 (11.29) | 1816 (23.14) |
| Female | 3357 (42.76) | 2446 (31.16) | 428 (5.45) | 454 (5.78) | 2929 (37.32) | 2271 (28.92) | 997 (12.7) | 2213 (28.19) | 96 (1.23) | 642 (8.18) | 902 (11.49) | 1856 (23.64) |
| P-value | 0.35 | 0.87 | 0.32 | 0.83 | 0.54 | 0.93 | ||||||
| Household size | ||||||||||||
| Less than 3 | 2360 (30.06) | 2148 (27.36) | 244 (3.11) | 262 (3.34) | 2116 (26.96) | 2036 (25.93) | 52 (0.67) | 81 (1.03) | 20 (0.25) | 12 (0.15) | 44 (0.56) | 69 (0.88) |
| 3 to 5 | 3372 (42.95) | 2659 (33.88) | 423 (5.39) | 547 (6.97) | 2949 (37.56) | 2367 (30.16) | 1096 (13.96) | 2343 (29.84) | 96 (1.22) | 594 (7.57) | 1000 (12.74) | 2037 (25.95) |
| More than 5 | 3794 (48.33) | 2974 (37.88) | 471 (6.00) | 563 (7.18) | 3323 (42.33) | 2763 (35.20) | 790 (10.06) | 1419 (18.07) | 57 (0.73) | 93 (1.18) | 733 (9.33) | 1406 (17.92) |
| P-value | 0.03 | 0.13 | 0.05 | 0.20 | 0.71 | 0.20 | ||||||
| Income quintile | ||||||||||||
| Poorest quintile | 3377 (43.02) | 2620 (33.37) | 379 (4.82) | 522 (6.65) | 2998 (38.19) | 2363 (30.11) | 1074 (13.68) | 2649 (33.75) | 125 (1.59) | 883 (11.25) | 950 (12.10) | 2065 (26.30) |
| 2nd | 3289 (41.90) | 2498 (31.82) | 433 (5.51) | 469 (5.98) | 2856 (36.39) | 2304 (29.35) | 790 (10.06) | 1424 (18.15) | 51 (0.65) | 70 (0.89) | 740 (9.43) | 1393 (17.75) |
| 3rd | 3568 (45.46) | 2468 (31.44) | 417 (5.31) | 518 (6.60) | 3151 (40.14) | 2296 (29.25) | 821 (10.46) | 1718 (21.89) | 48 (0.61) | 87 (1.11) | 774 (9.86) | 1708 (21.75) |
| 4th | 3334 (42.47) | 2880 (36.69) | 413 (5.26) | 473 (6.03) | 2921 (37.21) | 2599 (33.11) | 1096 (13.96) | 1975 (25.16) | 77 (0.98) | 285 (3.63) | 1019 (12.99) | 1875 (23.89) |
| Upper quintile | 3896 (49.62) | 3335 (42.48) | 519 (6.61) | 695 (8.86) | 3377 (43.02) | 3035 (38.66) | 1033 (13.16) | 2114 (26.93) | 89 (1.14) | 162 (2.06) | 945 (12.03) | 2052 (26.14) |
| P-value | 0.62 | 0.54 | 0.70 | 0.81 | 0.83 | 0.84 | ||||||
| Overall | 3490 (44.45) | 2789 (35.53) | 432 (5.51) | 542 (6.91) | 3057 (38.95) | 2541 (32.37) | 975 (12.42) | 2059 (26.23) | 82 (1.04) | 479 (6.11) | 894 (11.39) | 1834 (23.36) |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sarker, A.R.; Sultana, M.; Ali, N.; Akram, R.; Alam, K.; Khan, J.A.M.; Morton, A. Cost of Caregivers for Treating Hospitalized Diarrheal Patients in Bangladesh. Trop. Med. Infect. Dis. 2019, 4, 5. https://doi.org/10.3390/tropicalmed4010005
Sarker AR, Sultana M, Ali N, Akram R, Alam K, Khan JAM, Morton A. Cost of Caregivers for Treating Hospitalized Diarrheal Patients in Bangladesh. Tropical Medicine and Infectious Disease. 2019; 4(1):5. https://doi.org/10.3390/tropicalmed4010005
Chicago/Turabian StyleSarker, Abdur Razzaque, Marufa Sultana, Nausad Ali, Raisul Akram, Khorshed Alam, Jahangir A.M. Khan, and Alec Morton. 2019. "Cost of Caregivers for Treating Hospitalized Diarrheal Patients in Bangladesh" Tropical Medicine and Infectious Disease 4, no. 1: 5. https://doi.org/10.3390/tropicalmed4010005
APA StyleSarker, A. R., Sultana, M., Ali, N., Akram, R., Alam, K., Khan, J. A. M., & Morton, A. (2019). Cost of Caregivers for Treating Hospitalized Diarrheal Patients in Bangladesh. Tropical Medicine and Infectious Disease, 4(1), 5. https://doi.org/10.3390/tropicalmed4010005