
Different Factors Influencing Postural Stability during Transcutaneous Electrical Stimulation of the Cervical Spinal Cord


 , , , , ,
, , , , , 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants of This Study
2.2. Transcutaneous Electrical Stimulation of the Spinal Cord
2.3. Stabilography
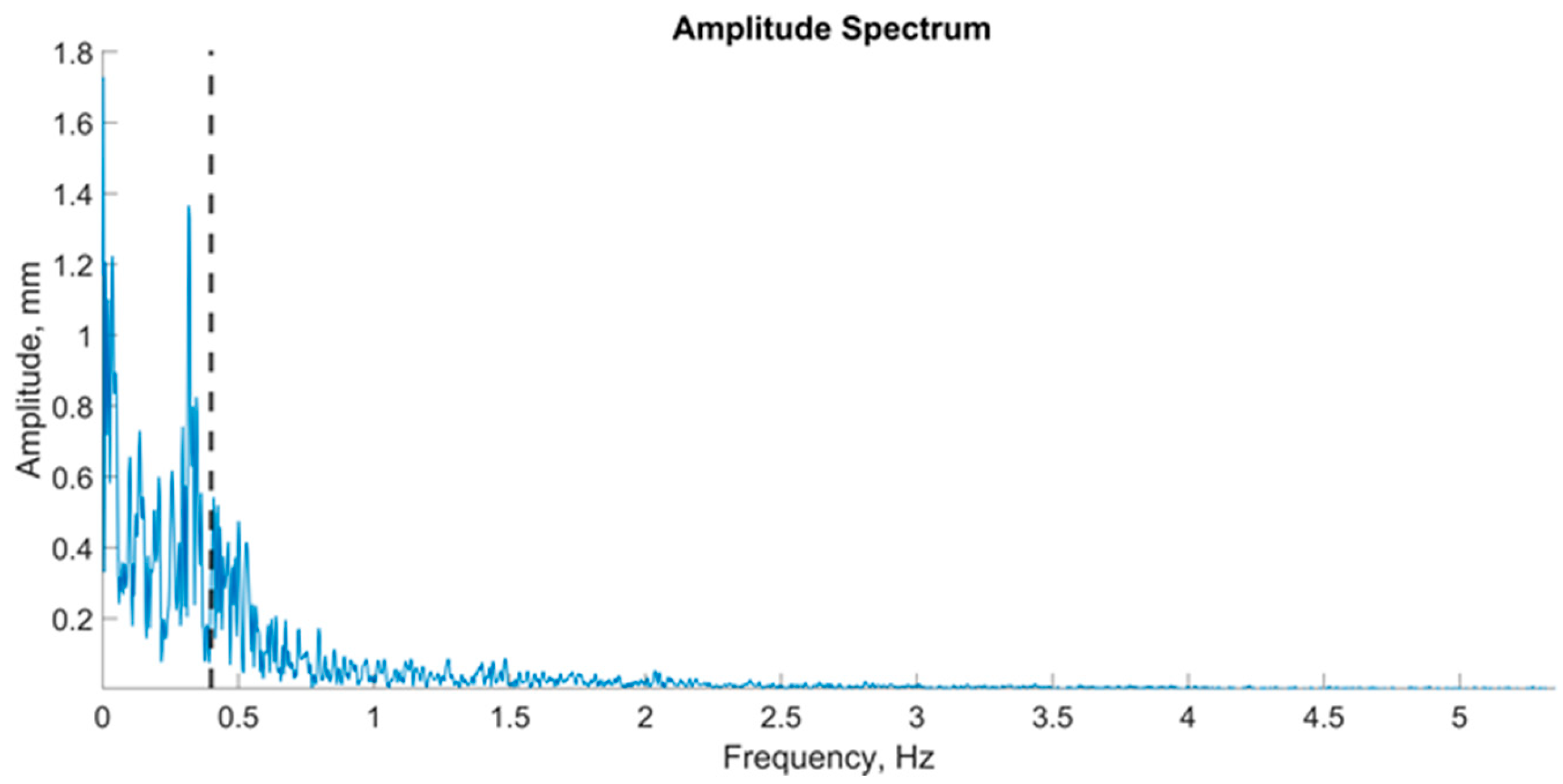
2.4. Spectral Analysis of the Stabilogram
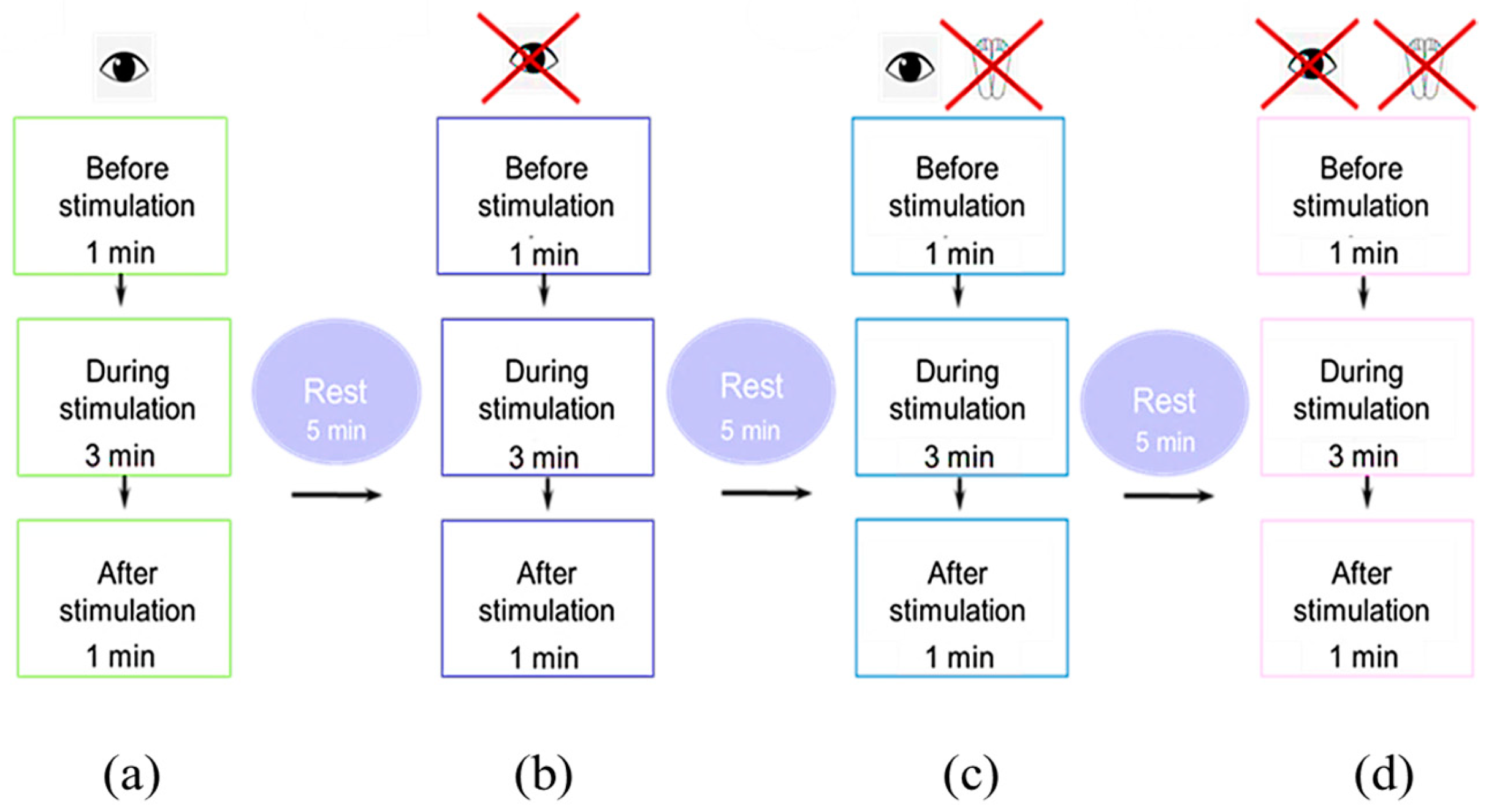
2.5. The Experimental Protocol and Data Collection
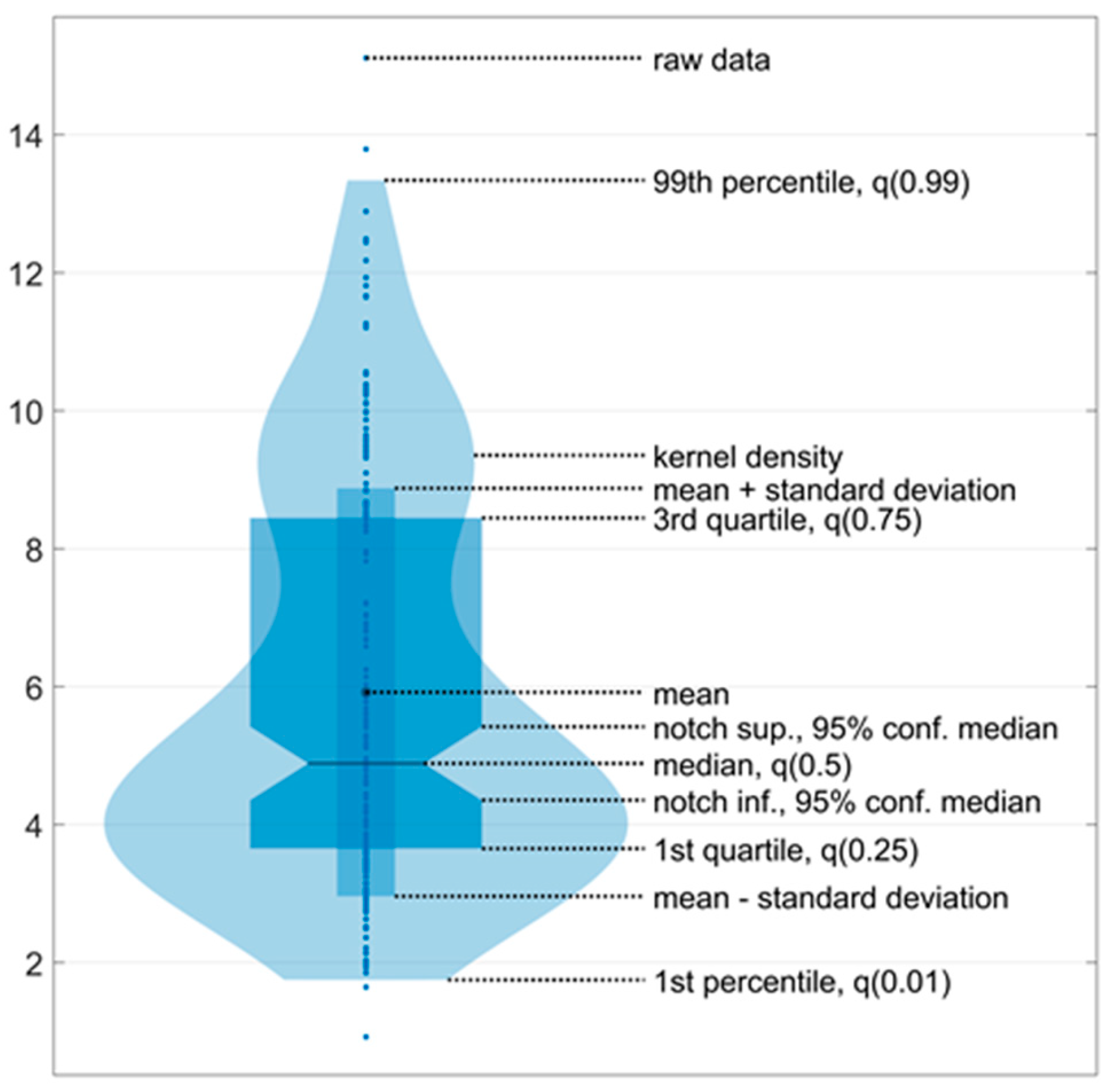
2.6. Statistical Analysis
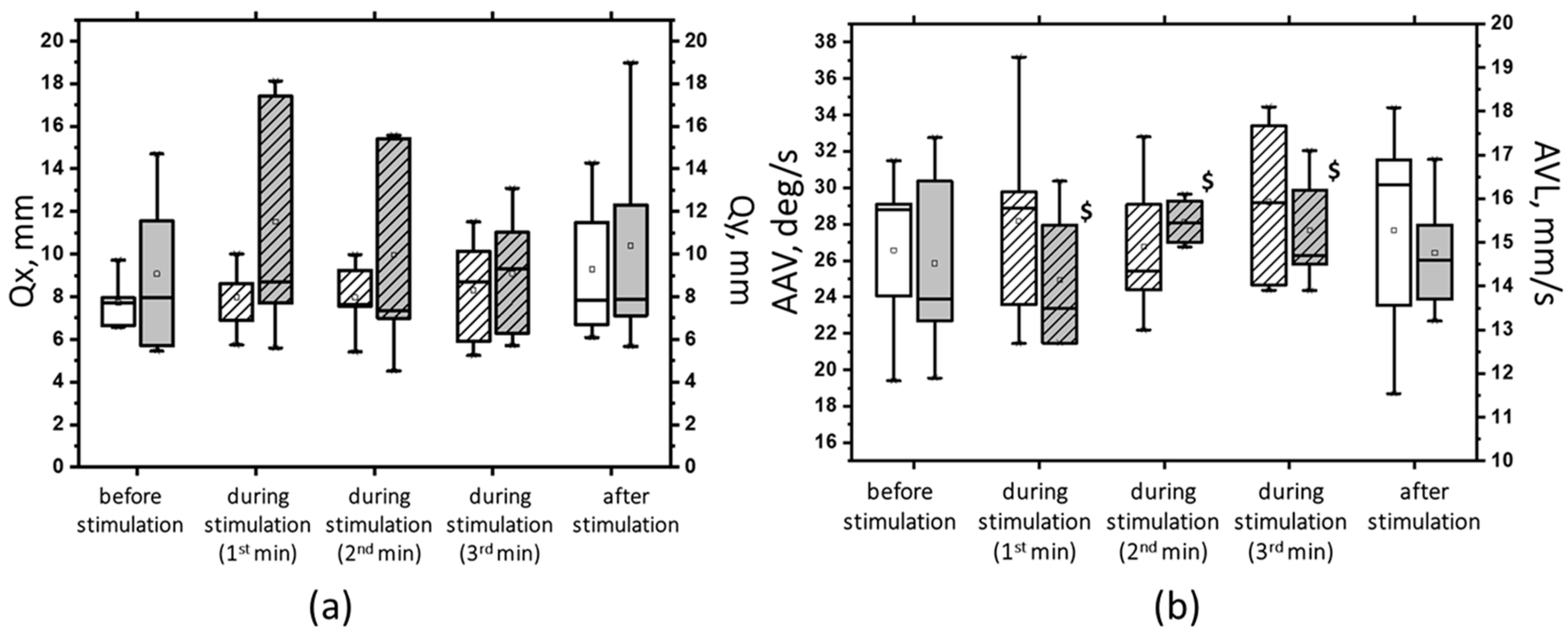
3. Results
3.1. Use of 5 Hz
3.2. Use of 30 Hz
4. Discussion
4.1. Postural Stability of Healthy Participants
4.2. Cervical Spinal Cord and Postural Stability
4.3. The tSC at 5 Hz and 30 Hz Frequencies
4.4. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zhu, M.; van Stiphout, L.; Karabulut, M.; Pérez Fornos, A.; Guinand, N.; Meijer, K.; van de Berg, R.; McCrum, C. Assessing balance in people with bilateral vestibulopathy using the Mini-Balance Evaluation Systems Test (Mini-BESTest): Feasibility and comparison with healthy control data. J. Neurol. 2023, 270, 4423–4433. [Google Scholar] [CrossRef]
- Almeida, G.P.L.; Monteiro, I.O.; Marizeiro, D.F.; Maia, L.B.; de Paula Lima, P.O. Y balance test has no correlation with the Stability Index of the Biodex Balance System. Musculoskelet. Sci. Pract. 2017, 27, 1–6. [Google Scholar] [CrossRef]
- Morningstar, M.W.; Pettibon, B.R.; Schlappi, H.; Schlappi, M.; Ireland, T.V. Reflex control of the spine and posture: A review of the literature from a chiropractic perspective. Chiropr. Osteopat. 2005, 13, 16. [Google Scholar] [CrossRef]
- Wannaprom, N.J.; Treleaven, J.; Jull, G.; Uthaikhup, S. Neck muscle vibration produces diverse responses in balance and gait speed between individuals with and without neck pain. Musculoskelet. Sci. Pract. 2018, 35, 25–29. [Google Scholar] [CrossRef] [PubMed]
- Cheever, K.; King, J.; Kawata, K. The association between contact sport exposure and cervical sensorimotor dysfunction: A scoping review of implications for future musculoskeletal injury risk. Chiropr. Man. Ther. 2022, 30, 50. [Google Scholar] [CrossRef]
- Boyd-Clark, L.C.; Briggs, C.A.; Galea, M.P. Muscle spindle distribution, morphology, and density in longus colli and multifidus muscles of the cervical spine. Spine 2002, 27, 694–701. [Google Scholar] [CrossRef] [PubMed]
- Campbell, D.; Murphy, B.A.; Burkitt, J.; La Delfa, N.; Sanmugananthan, P.; Ambalavanar, U.; Yielder, P. Cervico-Ocular and Vestibulo-Ocular Reflexes in Subclinical Neck Pain and Healthy Individuals: A Cross-Sectional Study. Brain Sci. 2023, 13, 1603. [Google Scholar] [CrossRef]
- Malmström, E.M.; Fransson, P.A.; Jaxmar Bruinen, T.; Facic, S.; Tjernström, F. Disturbed cervical proprioception affects perception of spatial orientation while in motion. Exp. Brain Res. 2017, 235, 2755–2766. [Google Scholar] [CrossRef]
- Lubetzky, A.V.; Harel, D.; Krishnamoorthy, S.; Fu, G.; Morris, B.; Medlin, A.; Wang, Z.; Perlin, K.; Roginska, A.; Cosetti, M.; et al. Decrease in head sway as a measure of sensory integration following vestibular rehabilitation: A randomized controlled trial. J. Vestib. Res. Equilib. Orientat. 2023, 33, 213–226. [Google Scholar] [CrossRef]
- Parhizi, B.; Barss, T.S.; Mushahwar, V.K. Simultaneous Cervical and Lumbar Spinal Cord Stimulation Induces Facilitation of Both Spinal and Corticospinal Circuitry in Humans. Front. Neurosci. 2021, 15, 615103. [Google Scholar] [CrossRef]
- Megía García, A.; Serrano-Muñoz, D.; Taylor, J.; Avendaño-Coy, J.; Gómez-Soriano, J. Transcutaneous spinal cord stimulation and motor rehabilitation in spinal cord injury: A systematic review. Neurorehabilit. Neural Repair 2020, 34, 3–12. [Google Scholar] [CrossRef] [PubMed]
- Martin, R. Utility and feasibility of Transcutaneous spinal cord stimulation for patients with incomplete SCI in therapeutic settings: A review of topic. Front. Rehabil. Sci. 2021, 2, 724003. [Google Scholar] [CrossRef] [PubMed]
- Barss, T.S.; Parhizi, B.; Porter, J.; Mushahwar, V.K. Neural Substrates of Transcutaneous Spinal Cord Stimulation: Neuromodulation across Multiple Segments of the Spinal Cord. J. Clin. Med. 2022, 3, 639. [Google Scholar] [CrossRef]
- Atkinson, D.A.; Steele, A.G.; Manson, G.A.; Sheynin, J.; Oh, J.; Gerasimenko, Y.P.; Sayenko, D.G. Characterization of interlimb interaction via transcutaneous spinal stimulation of cervical and lumbar spinal enlargements. J. Neurophysiol. 2022, 127, 1075–1085. [Google Scholar] [CrossRef] [PubMed]
- Gerasimenko, Y.; Gorodnichev, R.; Moshonkina, T.; Sayenko, D.; Gad, P.; Edgerton, V.R. Transcutaneous electrical spinal-cord stimulation in humans. Ann. Phys. Rehabil. Med. 2015, 58, 225–231. [Google Scholar] [CrossRef] [PubMed]
- Sayenko, D.G.; Rath, M.; Ferguson, A.R.; Burdick, J.W.; Havton, L.A.; Edgerton, V.R.; Gerasimenko, Y.P. Self-Assisted Standing Enabled by Non-Invasive Spinal Stimulation after Spinal Cord Injury. J. Neurotrauma 2019, 36, 1435–1450. [Google Scholar] [CrossRef]
- Roberts, B.W.R.; Atkinson, D.A.; Manson, G.A.; Markley, R.; Kaldis, T.; Britz, G.W.; Horner, P.J.; Vette, A.H.; Sayenko, D.G. Transcutaneous spinal cord stimulation improves postural stability in individuals with multiple sclerosis. Mult. Scler. Relat. Disord. 2021, 52, 103009. [Google Scholar] [CrossRef]
- Hofstoetter, U.S.; Freundl, B.; Binder, H.; Minassian, K. Common neural structures activated by epidural and transcutaneous lumbar spinal cord stimulation: Elicitation of posterior root–muscle reflexes. PLoS ONE 2018, 13, e0192013. [Google Scholar] [CrossRef]
- Benavides, F.D.; Jo, H.J.; Lundell, H.; Edgerton, V.R.; Gerasimenko, Y.; Perez, M.A. Cortical and Subcortical Effects of Transcutaneous Spinal Cord Stimulation in Humans with Tetraplegia. J. Neurosci. 2020, 40, 2633–2643. [Google Scholar] [CrossRef]
- Gorodnichev, R.M.; Pivovarova, E.A.; Pukhov, A.; Moiseev, S.A.; Savokhin, A.A.; Moshonkina, T.R.; Shcherbakova, N.A.; Kilimnik, V.A.; Selionov, V.A.; Kozlovskaia, I.B.; et al. Transcutaneous electrical stimulation of the spinal cord: Non-invasive tool for activation of locomotor circuitry in human. Fiziol. Cheloveka 2012, 38, 46–56. [Google Scholar]
- Singh, G.; Lucas, K.; Keller, A.; Martin, R.; Behrman, A.; Vissarionov, S.; Gerasimenko, Y.P. Transcutaneous Spinal Stimulation from Adults to Children: A Review. Top. Spinal Cord Inj. Rehabil. 2023, 29, 16–32. [Google Scholar] [CrossRef] [PubMed]
- Gerasimenko, Y.P.; Sayenko, D.G.; Gad, P.; Edgerton, V.R.; Gorodnichev, R.M.; McKinney, Z.; Grundfest, W.; Kozlovskaya, I.B. Spinal and sensory neuromodulation of spinal neuronal networks in humans. Hum. Physiol. 2017, 43, 492–500. [Google Scholar] [CrossRef]
- Oh, J.; Steele, A.G.; Varghese, B.; Martin, C.A.; Scheffler, M.S.; Markley, R.L.; Lo, Y.K.; Sayenko, D.G. Cervical transcutaneous spinal stimulation for spinal motor mapping. iScience 2022, 25, 105037. [Google Scholar] [CrossRef] [PubMed]
- Oh, J.; Scheffler, M.S.; Mahan, E.E.; King, S.T.; Martin, C.A.; Dinh, J.; Steele, A.G.; O’Malley, M.K.; Sayenko, D.G. Combinatorial Effects of Transcutaneous Spinal Stimulation and Task-Specific Training to Enhance Hand Motor Output after Paralysis. Top. Spinal Cord Inj. Rehabil. 2023, 29, 15–22. [Google Scholar] [CrossRef] [PubMed]
- Chandrasekaran, S.; Bhagat, N.A.; Ramdeo, R.; Ebrahimi, S.; Sharma, P.D.; Griffin, D.G.; Stein, A.; Harkema, S.J.; Bouton, C.E. Targeted transcutaneous spinal cord stimulation promotes persistent recovery of upper limb strength and tactile sensation in spinal cord injury: A pilot study. Front. Neurosci. 2023, 17, 1210328. [Google Scholar] [CrossRef] [PubMed]
- Barss, T.S.; Parhizi, B.; Mushahwar, V.K. Transcutaneous spinal cord stimulation of the cervical cord modulates lumbar networks. J. Neurophysiol. 2020, 123, 158–166. [Google Scholar] [CrossRef]
- Gerasimenko, Y.P.; Lu, D.C.; Modaber, M.; Zdunowski, S.; Gad, P.; Sayenko, D.G.; Morikawa, E.; Haakana, P.; Ferguson, A.R.; Roy, R.R.; et al. Noninvasive Reactivation of Motor Descending Control after Paralysis. J. Neurotrauma 2015, 32, 1968–1980. [Google Scholar] [CrossRef]
- Moshonkina, T.; Grishin, A.; Bogacheva, I.; Gorodnichev, R.; Ovechkin, A.; Siu, R.; Edgerton, V.R.; Gerasimenko, Y. Novel Non-invasive Strategy for Spinal Neuromodulation to Control Human Locomotion. Front. Hum. Neurosci. 2021, 14, 622533. [Google Scholar] [CrossRef]
- Sharma, P.; Panta, T.; Ugiliweneza, B.; Bert, R.J.; Gerasimenko, Y.; Forrest, G.; Harkema, S. Multi-Site Spinal Cord Transcutaneous Stimulation Facilitates Upper Limb Sensory and Motor Recovery in Severe Cervical Spinal Cord Injury: A Case Study. J. Clin. Med. 2023, 12, 4416. [Google Scholar] [CrossRef]
- Grishin, A.A.; Moshonkina, T.R.; Solopova, I.A.; Gorodnichev, R.M.; Gerasimenko, Y.P. A five-channel noninvasive electrical stimulator of the spinal cord for rehabilitation of patients with severe motor disorders. Biomed. Eng. 2017, 50, 300–304. [Google Scholar] [CrossRef]
- Stålberg, E.; van Dijk, H.; Falck, B.; Kimura, J.; Neuwirth, C.; Pitt, M.; Podnar, S.; Rubin, D.I.; Rutkove, S.; Sanders, D.B.; et al. Standards for quantitative assessment of EMG and neurography. Clin. Neurophysiol. 2019, 130, 1688–1729. [Google Scholar] [CrossRef] [PubMed]
- Besomi, M.; Devecchi, V.; Falla, D.; McGill, K.; Kiernan, M.C.; Merletti, R.; van Dieën, J.H.; Tucker, K.; Clancy, E.A.; Søgaard, K.; et al. Consensus for experimental design in electromyography (CEDE) project: Checklist for reporting and critically appraising studies using EMG (CEDE-Check). J. Electromyogr. Kinesiol. 2024, 76, 102874. [Google Scholar] [CrossRef] [PubMed]
- Sliva, S.S. Domestic computer stabilography: Technical standards, functionality and areas of application. Biomed. Eng. 2005, 39, 31–34. [Google Scholar] [CrossRef]
- Dakinova, M.V.; Bikchentaeva, L.M.; Tagirova, I.S.; Baltina, T.V.; Yafarova, G.G.; Sachenkov, O.A. Spectral analysis of stabilographic signals by Fourier and Hilbert–Huang methods. In Proceedings of the 2022 VIII International Conference on Information Technology and Nanotechnology (ITNT), Samara, Russia, 23–27 May 2022; pp. 1–4. [Google Scholar] [CrossRef]
- Kirchner, M.; Schubert, P.; Schmidtbleicher, D.; Haas, C.T. Evaluation of the temporal structure of postural sway fluctuations based on a comprehensive set of analysis tools. Phys. A Stat. Mech. Appl. 2012, 391, 4692–4703. [Google Scholar] [CrossRef]
- Lin, I.S.; Lai, D.M.; Ding, J.J.; Chien, A.; Cheng, C.H.; Wang, S.F.; Wang, J.L.; Kuo, C.L.; Hsu, W.L. Reweighting of the sensory inputs for postural control in patients with cervical spondylotic myelopathy after surgery. J. Neuroeng. Rehabil. 2019, 16, 96. [Google Scholar] [CrossRef] [PubMed]
- Jeka, J.; Kiemel, T.; Creath, R.; Horak, F.; Peterka, R. Controlling human upright posture: Velocity information is more accurate than position or acceleration. J. Neurophysiol. 2004, 92, 2368–2379. [Google Scholar] [CrossRef] [PubMed]
- Peterka, R.J. Sensory integration for human balance control. Handb. Clin. Neurol. 2018, 159, 27–42. [Google Scholar] [CrossRef]
- Sozzi, S.; Nardone, A.; Schieppati, M. Specific Posture-Stabilising Effects of Vision and Touch Are Revealed by Distinct Changes of Body Oscillation Frequencies. Front. Neurol. 2021, 12, 756984. [Google Scholar] [CrossRef]
- Morasso, P. Centre of pressure versus centre of mass stabilization strategies: The tightrope balancing case. R. Soc. Open Sci. 2020, 7, 200111. [Google Scholar] [CrossRef]
- Lhomond, O.; Juan, B.; Fornerone, T.; Cossin, M.; Paleressompoulle, D.; Prince, F.; Mouchnino, L. Learned Overweight Internal Model Can Be Activated to Maintain Equilibrium When Tactile Cues Are Uncertain: Evidence From Cortical and Behavioral Approaches. Front. Hum. Neurosci. 2021, 15, 635611. [Google Scholar] [CrossRef]
- Patel, M.; Fransson, P.A.; Johansson, R.; Magnusson, M. Foam posturography: Standing on foam is not equivalent to standing with decreased rapidly adapting mechanoreceptive sensation. Exp. Brain Res. 2011, 208, 519–527. [Google Scholar] [CrossRef] [PubMed]
- Hsiao, D.; Belur, P.; Myers, P.S.; Earhart, G.M.; Rawson, K.S. The impact of age, surface characteristics, and dual-tasking on postural sway. Arch. Gerontol. Geriatr. 2020, 87, 103973. [Google Scholar] [CrossRef] [PubMed]
- Sozzi, S.; Do, M.C.; Schieppati, M. Vertical ground reaction force oscillation during standing on hard and compliant surfaces: The “postural rhythm”. Front. Neurol. 2022, 13, 975752. [Google Scholar] [CrossRef]
- Armstrong, B.; McNair, P.; Taylor, D. Head and neck position sense. Sports Med. (Auckl. N.Z.) 2008, 38, 101–117. [Google Scholar] [CrossRef]
- Artz, N.J.; Adams, M.A.; Dolan, P. Sensorimotor function of the cervical spine in healthy volunteers. Clin. Biomech. (Bristol. Avon.) 2015, 30, 260–268. [Google Scholar] [CrossRef] [PubMed]
- Ferris, D.P.; Huang, H.J.; Kao, P.C. Moving the arms to activate the legs. Exerc. Sport Sci. Rev. 2006, 34, 113–120. [Google Scholar] [CrossRef]
- Arellano, C.J.; Vega, D. Exploring How the Arms Can Help the Legs in Facilitating Gait Rehabilitation. Adv. Biol. 2024, 8, e2300661. [Google Scholar] [CrossRef]
- Zhou, R.; Parhizi, B.; Assh, J.; Alvarado, L.; Ogilvie, R.; Chong, S.L.; Mushahwar, V.K. Effect of cervicolumbar coupling on spinal reflexes during cycling after incomplete spinal cord injury. J. Neurophysiol. 2018, 120, 3172–3186. [Google Scholar] [CrossRef]
- Gerasimenko, Y.; Gorodnichev, R.; Puhov, A.; Moshonkina, T.; Savochin, A.; Selionov, V.; Roy, R.R.; Lu, D.C.; Edgerton, V.R. Initiation and modulation of locomotor circuitry output with multisite transcutaneous electrical stimulation of the spinal cord in noninjured humans. J. Neurophysiol. 2015, 113, 834–842. [Google Scholar] [CrossRef]
- Inanici, F.; Brighton, L.N.; Samejima, S.; Hofstetter, C.P.; Moritz, C.T. Transcutaneous Spinal Cord Stimulation Restores Hand and Arm Function After Spinal Cord Injury. IEEE Trans. Neural Syst. Rehabil. Eng. A Publ. IEEE Eng. Med. Biol. Soc. 2021, 29, 310–319. [Google Scholar] [CrossRef]
- Militskova, A.; Mukhametova, E.; Fatykhova, E.; Sharifullin, S.; Cuellar, C.A.; Calvert, J.S.; Grahn, P.J.; Baltina, T.; Lavrov, I. Supraspinal and Afferent Signaling Facilitate Spinal Sensorimotor Network Excitability After Discomplete Spinal Cord Injury: A Case Report. Front. Neurosci. 2020, 14, 552. [Google Scholar] [CrossRef] [PubMed]
- Shamantseva, N.; Timofeeva, O.; Gvozdeva, A.; Andreeva, I.; Moshonkina, T. Posture of Healthy Subjects Modulated by Transcutaneous Spinal Cord Stimulation. Life 2023, 13, 1909. [Google Scholar] [CrossRef] [PubMed]
- Carrera, R.M.; Omofuma, I.; Yasin, B.; Agrawal, S.K. The Effect of Transcutaneous Spinal Cord Stimulation on Standing Postural Control in Healthy Adults. IEEE Robot. Autom. Lett. 2022, 7, 8268–8275. [Google Scholar] [CrossRef]
- Horak, F.B.; Henry, S.M.; Shumway-Cook, A. Postural perturbations: New insights for treatment of balance disorders. Phys. Ther. 1997, 77, 517–533. [Google Scholar] [CrossRef] [PubMed]
- Welch, T.D.J.; Ting, L.H. Mechanisms of motor adaptation in reactive balance control. PLoS ONE 2014, 9, e96440. [Google Scholar] [CrossRef]
- Babič, J.; Oztop, E.; Kawato, M. Human motor adaptation in whole body motion. Sci. Rep. 2016, 6, 32868. [Google Scholar] [CrossRef]
- Sakanaka, T.E.; Lakie, M.; Reynolds, R.F. Idiosyncratic Characteristics of Postural Sway in Normal and Perturbed Standing. Front. Hum. Neurosci. 2021, 15, 660470. [Google Scholar] [CrossRef]
- Singh, N.B.; Taylor, W.R.; Madigan, M.L.; Nussbaum, M.A. The spectral content of postural sway during quiet stance: Influences of age, vision and somatosensory inputs. J. Electromyogr. Kinesiol. 2012, 22, 131–136. [Google Scholar] [CrossRef]
- Nashner, L.M.; Wolfson, P. Influence of head position and proprioceptive cues on short latency postural reflexes evoked by galvanic stimulation of the human labyrinth. Brain Res. 1974, 67, 255–268. [Google Scholar] [CrossRef]
- Welgampola, M.; Colebatch, J. Vestibulospinal reflexes: Quantitative effects of sensory feedback and postural task. Exp. Brain Res. 2001, 139, 345–353. [Google Scholar] [CrossRef]
- Rejc, E.; Angeli, C.; Harkema, S. Effects of Lumbosacral Spinal Cord Epidural Stimulation for Standing after Chronic Complete Paralysis in Humans. PLoS ONE 2015, 10, e0133998. [Google Scholar] [CrossRef] [PubMed]
- Choi, E.H.; Gattas, S.; Brown, N.J.; Hong, J.D.; Limbo, J.N.; Chan, A.Y.; Oh, M.Y. Epidural electrical stimulation for spinal cord injury. Neural Regen. Res. 2021, 16, 2367–2375. [Google Scholar] [CrossRef] [PubMed]
- Harkema, S.; Gerasimenko, Y.; Hodes, J.; Burdick, J.; Angeli, C.; Chen, Y.; Ferreira, C.; Willhite, A.; Rejc, E.; Grossman, R.G.; et al. Effect of epidural stimulation of the lumbosacral spinal cord on voluntary movement, standing, and assisted stepping after motor complete paraplegia: A case study. Lancet 2011, 377, 1938–1947. [Google Scholar] [CrossRef]
- Angeli, C.A.; Edgerton, V.R.; Gerasimenko, Y.P.; Harkema, S.J. Altering spinal cord excitability enables voluntary movements after chronic complete paralysis in humans. Brain 2014, 137 Pt 5, 1394–1409. [Google Scholar] [CrossRef]
- Angeli, C.A.; Boakye, M.; Morton, R.A.; Vogt, J.; Benton, K.; Chen, Y.; Ferreira, C.K.; Harkema, S.J. Recovery of Over-Ground Walking after Chronic Motor Complete Spinal Cord Injury. N. Engl. J. Med. 2018, 379, 1244–1250. [Google Scholar] [CrossRef] [PubMed]
- Omofuma, I.; Carrera, R.; King-Ori, J.; Agrawal, S.K. The effect of transcutaneous spinal cord stimulation on the balance and neurophysiological characteristics of young healthy adults. Wearable Technol. 2024, 5, e3. [Google Scholar] [CrossRef]
- Bedi, P.K.; Arumugam, N. Tapping the neural circuitry: Surface spinal stimulation in spinal cord injury: A case report. JESP 2016, 12, 69–75. [Google Scholar] [CrossRef]
- Freyvert, Y.; Yong, N.A.; Morikawa, E.; Zdunowski, S.; Sarino, M.E.; Gerasimenko, Y.; Edgerton, V.R.; Lu, D.C. Engaging cervical spinal circuitry with non-invasive spinal stimulation and buspirone to restore hand function in chronic motor complete patients. Sci. Rep. 2018, 8, 15546. [Google Scholar] [CrossRef]
- Kanekar, N.; Lee, Y.J.; Aruin, A.S. Frequency analysis approach to study balance control in individuals with multiple sclerosis. J. Neurosci. Methods 2014, 222, 91–96. [Google Scholar] [CrossRef]
- Angeli, C.A.; Gerasimenko, Y. Combined cervical transcutaneous with lumbosacral epidural stimulation improves voluntary control of stepping movements in spinal cord injured individuals. Front. Bioeng. Biotechnol. 2023, 11, 1073716. [Google Scholar] [CrossRef]
- Hill, M.W.; Wdowski, M.M.; Rosicka, K.; Kay, A.D.; Muehlbauer, T. Exploring the relationship of static and dynamic balance with muscle mechanical properties of the lower limbs in healthy young adults. Front. Physiol. 2023, 14, 1168314. [Google Scholar] [CrossRef] [PubMed]





Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bikchentaeva, L.; Nikulina, M.; Shulman, A.; Baltin, M.; Zheltukhina, A.; Semenova, E.; Smirnova, V.; Klepikova, S.; Baltina, T. Different Factors Influencing Postural Stability during Transcutaneous Electrical Stimulation of the Cervical Spinal Cord. J. Funct. Morphol. Kinesiol. 2024, 9, 142. https://doi.org/10.3390/jfmk9030142
Bikchentaeva L, Nikulina M, Shulman A, Baltin M, Zheltukhina A, Semenova E, Smirnova V, Klepikova S, Baltina T. Different Factors Influencing Postural Stability during Transcutaneous Electrical Stimulation of the Cervical Spinal Cord. Journal of Functional Morphology and Kinesiology. 2024; 9(3):142. https://doi.org/10.3390/jfmk9030142
Chicago/Turabian StyleBikchentaeva, Leisan, Margarita Nikulina, Anna Shulman, Maxim Baltin, Angelina Zheltukhina, Elena Semenova, Viktoriya Smirnova, Svetlana Klepikova, and Tatyana Baltina. 2024. "Different Factors Influencing Postural Stability during Transcutaneous Electrical Stimulation of the Cervical Spinal Cord" Journal of Functional Morphology and Kinesiology 9, no. 3: 142. https://doi.org/10.3390/jfmk9030142
APA StyleBikchentaeva, L., Nikulina, M., Shulman, A., Baltin, M., Zheltukhina, A., Semenova, E., Smirnova, V., Klepikova, S., & Baltina, T. (2024). Different Factors Influencing Postural Stability during Transcutaneous Electrical Stimulation of the Cervical Spinal Cord. Journal of Functional Morphology and Kinesiology, 9(3), 142. https://doi.org/10.3390/jfmk9030142