
Stretching for Recovery from Groin Pain or Injury in Athletes: A Critical and Systematic Review

 ,
,  ,
,  ,
, 

 and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Protocol and Registration
2.2. Eligibility Criteria
2.3. Information Sources
2.4. Search Strategy
(((“groin pain” [Title/Abstract] OR “groin strain” [Title/Abstract] OR “groin injur *” [Title/Abstract] OR “pubalgia” [Title/Abstract] OR “symphysis syndrome” [Title/Abstract] OR “osteitis pubis” [Title/Abstract] OR “adductor tendin *” [Title/Abstract] OR “incipient hernia” [Title/Abstract] OR “inguinal hernia” [Title/Abstract]) AND (“stretch *” [Title/Abstract] OR “mobility” [Title/Abstract] OR “range of motion” [Title/Abstract] OR “flexi *” [Title/Abstract])) AND (“player” [Title/Abstract] OR “athlet *” [Title/Abstract] OR “practitioner” [Title/Abstract] OR “sport *” [Title/Abstract] OR “training” [Title/Abstract] OR “exercise” [Title/Abstract] OR “rehabilitation” [Title/Abstract])) AND (random * [Title/Abstract])
2.5. Selection Process
2.6. Data Collection Process and Data Items
2.7. Study Risk of Bias Assessment
2.8. Effect Measures and Synthesis Methods
2.9. Reporting Bias Assessment
2.10. Certainty Assessment
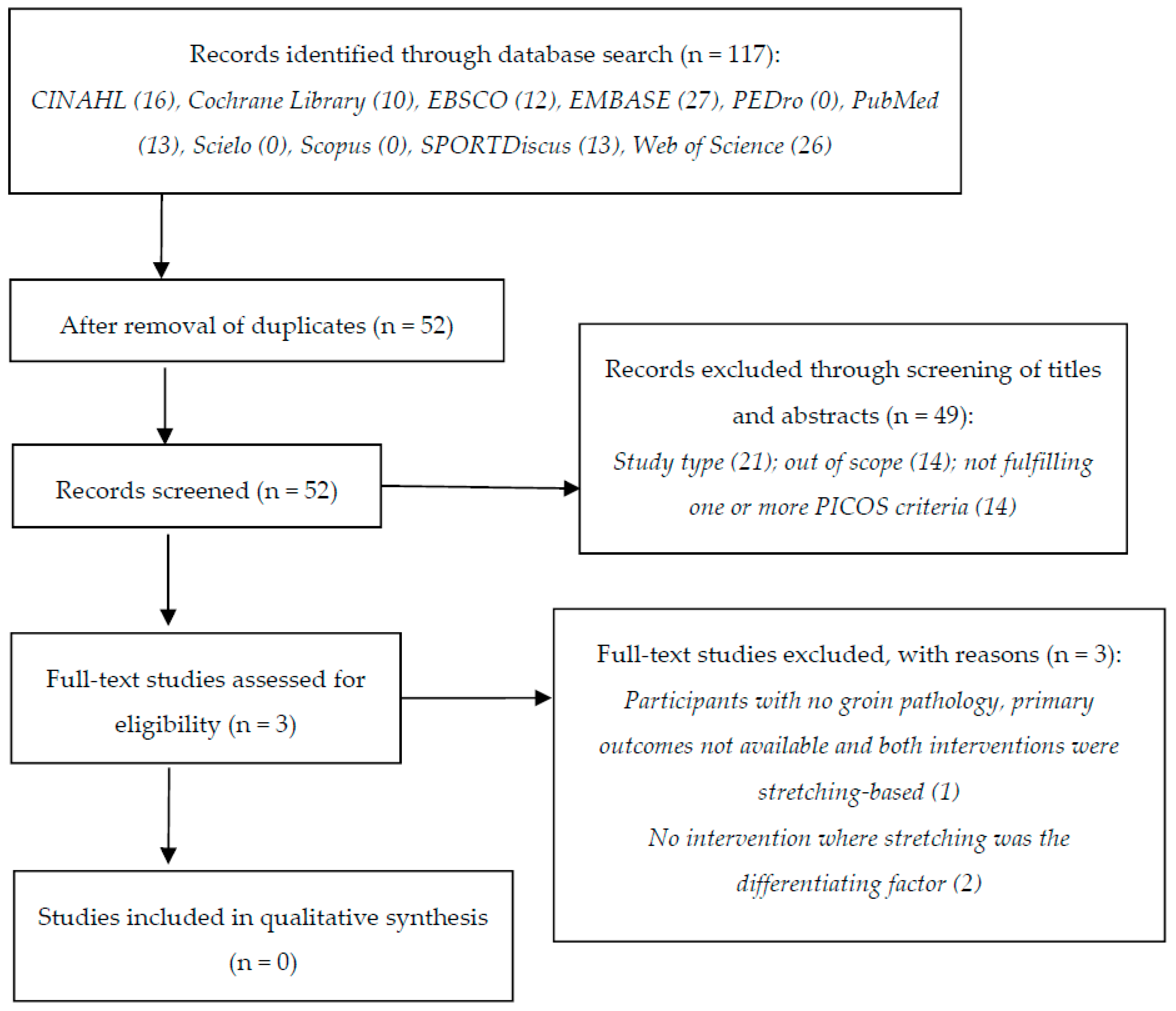
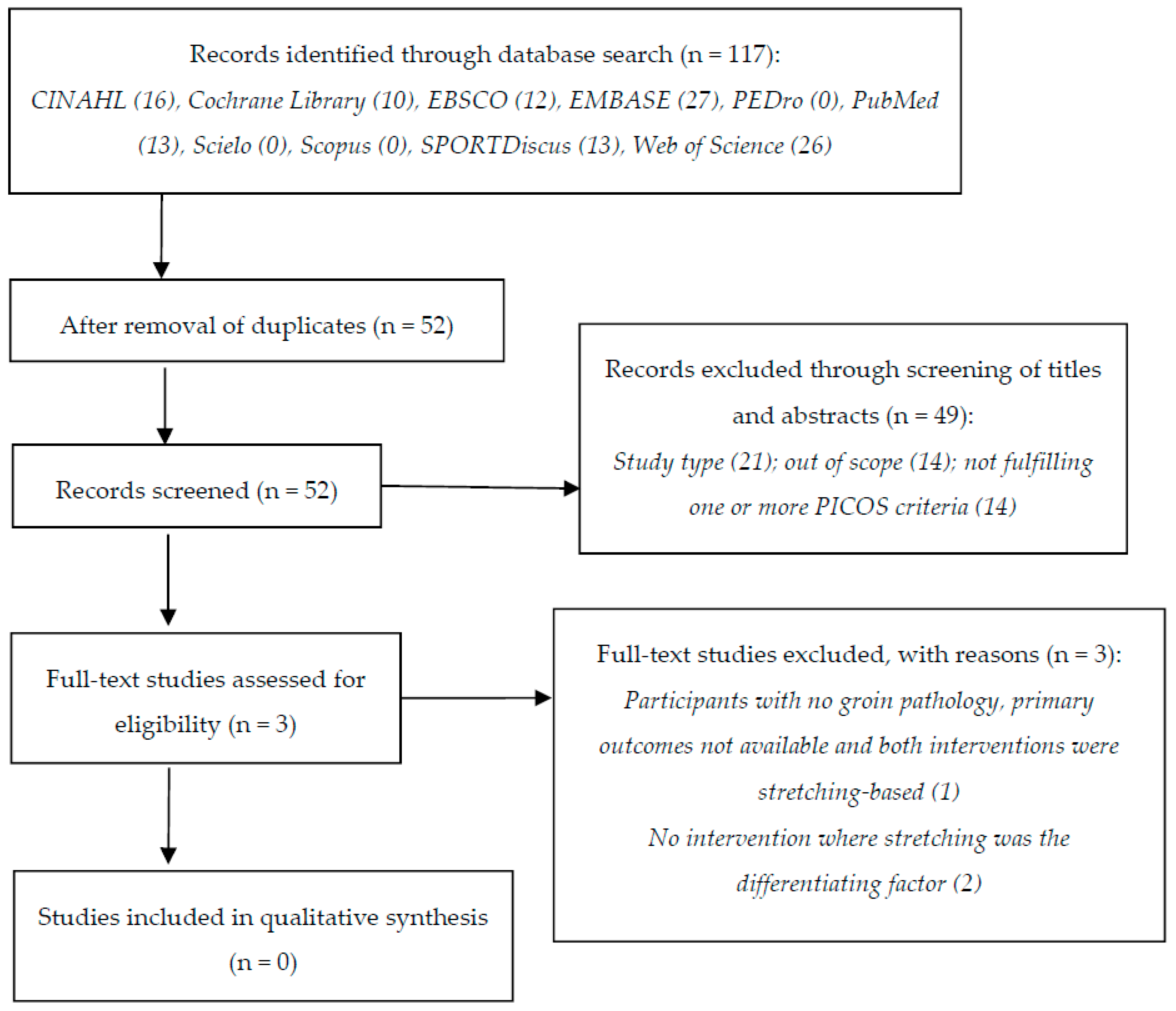
3. Results
4. Discussion
4.1. Summary of Evidence
4.2. Evidence from Other Study Designs
4.3. The Implications of an Empty Review for the Field
4.4. Limitations and Strengths
5. Conclusions
6. Other Information
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Charlton, P.C.; Drew, M.K.; Mentiplay, B.F.; Grimaldi, A.; Clark, R.A. Exercise interventions for the prevention and treatment of groin pain and injury in athletes: A critical and systematic review. Sports Med. 2017, 47, 2011–2026. [Google Scholar] [CrossRef]
- Delahunt, E.; Thorborg, K.; Khan, K.M.; Robinson, P.; Hölmich, P.; Weir, A. Minimum reporting standards for clinical research on groin pain in athletes. Br. J. Sports Med. 2015, 49, 775. [Google Scholar] [CrossRef] [PubMed]
- Serner, A.; Van Eijck, C.H.; Beumer, B.R.; Hölmich, P.; Weir, A.; DeVos, R.J. Study quality on groin injury management remains low: A systematic review on treatment of groin pain in athletes. Br. J. Sports Med. 2015, 49, 813. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wörner, T.; Thorborg, K.; Eek, F. Hip and groin problems in the previous season are associated with impaired function in the beginning of the new season among professional female Ice Hockey player—A cross sectional study. Int. J. Sports Phys. Ther. 2020, 15, 763–769. [Google Scholar] [CrossRef] [PubMed]
- Ekhtiari, S.; Khan, M.; Burrus, T.; Madden, K.; Gagnier, J.; Rogowski, J.P.; Maerz, T.; Bedi, A. Hip and groin injuries in professional basketball players: Impact on playing career and quality of life after retirement. Sports Health 2019, 11, 218–222. [Google Scholar] [CrossRef]
- Kerbel, Y.E.; Smith, C.M.; Prodromo, J.P.; Nzeogu, M.I.; Mulcahey, M.K. Epidemiology of hip and groin injuries in collegiate athletes in the United States. Orthop. J. Sports Med. 2018, 6, 2325967118771676. [Google Scholar] [CrossRef] [Green Version]
- Thorborg, K.; Rathleff, M.S.; Petersen, P.; Branci, S.; Hölmich, P. Prevalence and severity of hip and groin pain in sub-elite male football: A cross-sectional cohort study of 695 players. Scand. J. Med. Sci. Sports 2017, 27, 107–114. [Google Scholar] [CrossRef]
- Ramazzina, I.; Bernazzoli, B.; Braghieri, V.; Costantino, C. Groin pain in athletes and non-interventional rehabilitative treatment: A systematic review. J. Sports Med. Phys. Fit. 2019, 59, 1001–1010. [Google Scholar] [CrossRef]
- Langhout, R.; Weir, A.; Litjes, W.; Gozeling, M.; Stubbe, J.H.; Kerkhoffs, G.; Tak, I. Hip and groin injury is the most common non-time-loss injury in female amateur football. Knee Surg. Sports Traumatol. Arthrosc. 2019, 27, 3133–3141. [Google Scholar] [CrossRef] [Green Version]
- Jansen, J.A.; Mens, J.M.; Backx, F.J.; Kolfschoten, N.; Stam, H.J. Treatment of longstanding groin pain in athletes: A systematic review. Scand. J. Med. Sci. Sports 2008, 18, 263–274. [Google Scholar] [CrossRef] [PubMed]
- King, E.; Ward, J.; Small, L.; Falvey, E.; Franklyn-Miller, A. Athletic groin pain: A systematic review and meta-analysis of surgical versus physical therapy rehabilitation outcomes. Br. J. Sports Med. 2015, 49, 1447–1451. [Google Scholar] [CrossRef]
- Machotka, Z.; Kumar, S.; Perraton, L.G. A systematic review of the literature on the effectiveness of exercise therapy for groin pain in athletes. Sports Med. Arthrosc. Rehabil. Ther. Technol. 2009, 1, 5. [Google Scholar] [CrossRef] [Green Version]
- Hamilton, B.; Alonso, J.-M.; Best, T.M. Time for a paradigm shift in the classification of muscle injuries. J. Sport Health Sci. 2017, 6, 255–261. [Google Scholar] [CrossRef] [PubMed]
- Bisciotti, G.N.; Chamari, K.; Cena, E.; Garcia, G.R.; Vuckovic, Z.; Bisciotti, A.; Bisciotti, A.; Zini, R.; Corsini, A.; Volpi, P. The conservative treatment of longstanding adductor-related groin pain syndrome: A critical and systematic review. Biol. Sport 2021, 38, 45–63. [Google Scholar] [CrossRef] [PubMed]
- Serner, A.; Hölmich, P.; Tol, J.L.; Thorborg, K.; Lanzinger, S.; Otten, R.; Whiteley, R.; Weir, A. Progression of strength, flexibility, and palpation pain during rehabilitation of athletes with acute adductor injuries: A prospective cohort study. J. Orthop. Sports Phys. Ther. 2020, 1–39. [Google Scholar] [CrossRef]
- Hölmich, P.; Uhrskou, P.; Ulnits, L.; Kanstrup, I.L.; Nielsen, M.B.; Bjerg, A.M.; Krogsgaard, K. Effectiveness of active physical training as treatment for long-standing adductor-related groin pain in athletes: Randomised trial. Lancet 1999, 353, 439–443. [Google Scholar] [CrossRef]
- Yousefzadeh, A.; Shadmehr, A.; Olyaei, G.R.; Naseri, N.; Khazaeipour, Z. Effect of Holmich protocol exercise therapy on long-standing adductor-related groin pain in athletes: An objective evaluation. BMJ Open Sport Exerc. Med. 2018, 4, e000343. [Google Scholar] [CrossRef]
- Kachingwe, A.F.; Grech, S. Proposed algorithm for the management of athletes with athletic pubalgia (sports hernia): A case series. J. Orthop. Sports Phys. Ther. 2008, 38, 768–781. [Google Scholar] [CrossRef] [Green Version]
- Afonso, J.; Ramirez-Campillo, R.; Moscão, J.; Rocha, T.; Zacca, R.; Martins, A.; Milheiro, A.A.; Ferreira, J.; Sarmento, H.; Clemente, F.M. Strength Training versus stretching for improving range of motion: A systematic review and meta-analysis. Healthcare 2021, 9, 427. [Google Scholar] [CrossRef]
- Afonso, J.; Olivares-Jabalera, J.; Andrade, R. Time to move from mandatory stretching? We need to differentiate “Can I?” from “Do I have to?”. Front. Physiol. 2021, 12, 1110. [Google Scholar] [CrossRef]
- Bisconti, A.V.; Cè, E.; Longo, S.; Venturelli, M.; Coratella, G.; Limonta, E.; Doria, C.; Rampichini, S.; Esposito, F. Evidence for improved systemic and local vascular function after long-term passive static stretching training of the musculoskeletal system. J. Physiol. 2020, 598, 3645–3666. [Google Scholar] [CrossRef]
- Bretischwerdt, C.; Rivas-Cano, L.; Palomeque-del-Cerro, L.; Fernández-de-las-Peñas, C.; Alburquerque-Sendín, F. Immediate effects of hamstring muscle stretching on pressure pain sensitivity and active mouth opening in healthy subjects. J. Manip. Physiol. Ther. 2010, 33, 42–47. [Google Scholar] [CrossRef] [PubMed]
- Weir, A.; Jansen, J.A.; van de Port, I.G.; Van de Sande, H.B.; Tol, J.L.; Backx, F.J. Manual or exercise therapy for long-standing adductor-related groin pain: A randomised controlled clinical trial. Man Ther. 2011, 16, 148–154. [Google Scholar] [CrossRef]
- Harris-Hayes, M.; Steger-May, K.; Bove, A.M.; Foster, S.N.; Mueller, M.J.; Clohisy, J.C.; Fitzgerald, G.K. Movement pattern training compared with standard strengthening and flexibility among patients with hip-related groin pain: Results of a pilot multicentre randomised clinical trial. BMJ Open Sport Exerc. Med. 2020, 6, e000707. [Google Scholar] [CrossRef]
- Abouelnaga, W.A.; Aboelnour, N.H. Effectiveness of active rehabilitation program on sports hernia: Randomized control trial. Ann. Rehabil. Med. 2019, 43, 305–313. [Google Scholar] [CrossRef]
- Gopalakrishnan, S.; Ganeshkumar, P. Systematic Reviews and meta-analysis: Understanding the best evidence in primary healthcare. J. Fam. Med. Prim. Care 2013, 2, 9–14. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V. Cochrane Handbook for Systematic Reviews of Interventions, 2nd ed.; John Wiley & Sons: Chichester, UK, 2019. [Google Scholar]
- Schlosser, R.W.; Sigafoos, J. ‘Empty’ reviews and evidence-based practice. Evid.-Based Commun. Assess. Interv. 2009, 3, 1–3. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; Group, P.-P. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shea, B.J.; Reeves, B.C.; Wells, G.; Thuku, M.; Hamel, C.; Moran, J.; Moher, D.; Tugwell, P.; Welch, V.; Kristjansson, E.; et al. AMSTAR 2: A critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ 2017, 358, j4008. [Google Scholar] [CrossRef] [Green Version]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Guyatt, G.H.; Oxman, A.D.; Akl, E.A.; Kunz, R.; Vist, G.; Brozek, J.; Norris, S.; Falck-Ytter, Y.; Glasziou, P.; DeBeer, H.; et al. GRADE guidelines: 1. Introduction-GRADE evidence profiles and summary of findings tables. J. Clin. Epidemiol. 2011, 64, 383–394. [Google Scholar] [CrossRef] [PubMed]
- Hariton, E.; Locascio, J.J. Randomised controlled trials—The gold standard for effectiveness research: Study design: Randomised controlled trials. BJOG 2018, 125, 1716. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Breivik, H.; Rosseland, L.A.; Stubhaug, A. Statistical pearls: Importance of effect-size, blinding, randomization, publication bias, and the overestimated p-values. Scand. J. Pain 2013, 4, 217–219. [Google Scholar] [CrossRef]
- Spieth, P.M.; Kubasch, A.S.; Penzlin, A.I.; Illigens, B.M.-W.; Barlinn, K.; Siepmann, T. Randomized controlled trials—A matter of design. Neuropsychiatr. Dis. Treat. 2016, 12, 1341–1349. [Google Scholar] [CrossRef] [Green Version]
- Elbourne, D.R.; Altman, D.G.; Higgins, J.P.T.; Curtin, F.; Worthington, H.V.; Vail, A. Meta-analyses involving cross-over trials: Methodological issues. Int. J. Epidemiol. 2002, 31, 140–149. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [Green Version]
- Valentine, J.C.; Pigott, T.D.; Rothstein, H.R. How many studies do you need?: A primer on statistical power for meta-analysis. J. Educ. Behav. Stat. 2010, 35, 215–247. [Google Scholar] [CrossRef]
- García-Hermoso, A.; Ramírez-Campillo, R.; Izquierdo, M. Is muscular fitness associated with future health benefits in children and adolescents? A systematic review and meta-analysis of longitudinal studies. Sports Med. 2019, 49, 1079–1094. [Google Scholar] [CrossRef]
- Skrede, T.; Steene-Johannessen, J.; Anderssen, S.A.; Resaland, G.K.; Ekelund, U. The prospective association between objectively measured sedentary time, moderate-to-vigorous physical activity and cardiometabolic risk factors in youth: A systematic review and meta-analysis. Obes. Rev. 2019, 20, 55–74. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abt, G.; Boreham, C.; Davison, G.; Jackson, R.; Nevill, A.; Wallace, E.; Williams, M. Power, precision, and sample size estimation in sport and exercise science research. J. Sports Sci. 2020, 38, 1933–1935. [Google Scholar] [CrossRef]
- Lohse, K.R.; Sainani, K.L.; Taylor, J.A.; Butson, M.L.; Knight, E.J.; Vickers, A.J. Systematic review of the use of “magnitude-based inference” in sports science and medicine. PLoS ONE 2020, 15, e0235318. [Google Scholar] [CrossRef]
- Drahota, A.; Beller, E. RevMan Calculator for Microsoft Excel [Computer Software]; Cochrane: London, UK, 2020. [Google Scholar]
- Deeks, J.J.; Higgins, J.P.; Altman, D.G. Analysing data and undertaking meta-analyses. In Cochrane Handbook for Systematic Reviews of Interventions: The Cochrane Collaboration; Higgins, J.P., Green, S., Eds.; The Cochrane Collaboration: London, UK, 2008; pp. 243–296. [Google Scholar]
- Kontopantelis, E.; Springate, D.A.; Reeves, D. A re-analysis of the Cochrane Library data: The dangers of unobserved heterogeneity in meta-analyses. PLoS ONE 2013, 8, e69930. [Google Scholar] [CrossRef]
- Hopkins, W.G.; Marshall, S.W.; Batterham, A.M.; Hanin, J. Progressive statistics for studies in sports medicine and exercise science. Med. Sci. Sports Exerc. 2009, 41, 3–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.P.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef]
- Moran, J.; Clark, C.C.T.; Ramirez-Campillo, R.; Davies, M.J.; Drury, B. A meta-analysis of plyometric training in female youth: Its efficacy and shortcomings in the literature. J. Strength Cond. Res. 2019, 33, 1996–2008. [Google Scholar] [CrossRef] [PubMed]
- Moran, J.; Sandercock, G.R.; Ramírez-Campillo, R.; Meylan, C.; Collison, J.; Parry, D.A. A meta-analysis of maturation-related variation in adolescent boy athletes’ adaptations to short-term resistance training. J. Sports Sci. 2017, 35, 1041–1051. [Google Scholar] [CrossRef]
- Egger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [Green Version]
- Duval, S.; Tweedie, R. Trim and fill: A simple funnel-plot-based method of testing and adjusting for publication bias in meta-analysis. Biometrics 2000, 56, 455–463. [Google Scholar] [CrossRef] [PubMed]
- Shi, L.; Lin, L. The trim-and-fill method for publication bias: Practical guidelines and recommendations based on a large database of meta-analyses. Medicine 2019, 98, e15987. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Alonso-Coello, P.; Guyatt, G.H.; Yepes-Nuñez, J.J.; Akl, E.A.; Hazlewood, G.; Pardo-Hernandez, H.; Etxeandia-Ikobaltzeta, I.; Qaseem, A.; Williams, J.W., Jr.; et al. GRADE Guidelines: 19. Assessing the certainty of evidence in the importance of outcomes or values and preferences—Risk of bias and indirectness. J. Clin. Epidemiol. 2019, 111, 94–104. [Google Scholar] [CrossRef] [PubMed]
- Schünemann, H.J.; Mustafa, R.A.; Brozek, J.; Steingart, K.R.; Leeflang, M.; Murad, M.H.; Bossuyt, P.; Glasziou, P.; Jaeschke, R.; Lange, S.; et al. GRADE guidelines: 21 part 1. Study design, risk of bias, and indirectness in rating the certainty across a body of evidence for test accuracy. J. Clin. Epidemiol. 2020, 122, 129–141. [Google Scholar] [CrossRef]
- Schünemann, H.J.; Mustafa, R.A.; Brozek, J.; Steingart, K.R.; Leeflang, M.; Murad, M.H.; Bossuyt, P.; Glasziou, P.; Jaeschke, R.; Lange, S.; et al. GRADE guidelines: 21 part 2. Test accuracy: Inconsistency, imprecision, publication bias, and other domains for rating the certainty of evidence and presenting it in evidence profiles and summary of findings tables. J. Clin. Epidemiol. 2020, 122, 142–152. [Google Scholar] [CrossRef] [PubMed]
- Bali, S.; Guru, K. Comparative Effect of Static Stretching and Mulligan Stretching on Hip Adductor Flexibility in Footballers—A Two Group Trial. JK Sci. 2020, 22, 96–100. [Google Scholar]
- Wright, A.A.; Hegedus, E.J.; Taylor, J.B.; Dischiavi, S.L.; Stubbs, A.J. Non-operative management of femoroacetabular impingement: A prospective, randomized controlled clinical trial pilot study. J. Sci. Med. Sport 2016, 19, 716–721. [Google Scholar] [CrossRef] [PubMed]
- Squires, J.E.; Sullivan, K.; Eccles, M.P.; Worswick, J.; Grimshaw, J.M. Are multifaceted interventions more effective than single-component interventions in changing health-care professionals’ behaviours? An overview of systematic reviews. Implement Sci. 2014, 9, 152. [Google Scholar] [CrossRef] [Green Version]
- Gardner, M.M.; Robertson, M.C.; Campbell, A.J. Exercise in preventing falls and fall related injuries in older people: A review of randomised controlled trials. Br. J. Sports Med. 2000, 34, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tavoian, D.; Russ, D.W.; Consitt, L.A.; Clark, B.C. Perspective: Pragmatic exercise recommendations for older adults: The case for emphasizing resistance training. Front. Physiol. 2020, 11, 799. [Google Scholar] [CrossRef]
- Medina-Mirapeix, F.; Escolar-Reina, P.; Gascón-Cánovas, J.J.; Montilla-Herrador, J.; Jimeno-Serrano, F.J.; Collins, S.M. Predictive factors of adherence to frequency and duration components in home exercise programs for neck and low back pain: An observational study. BMC Musculoskelet. Disord. 2009, 10, 155. [Google Scholar] [CrossRef] [Green Version]
- Kim, G.; Kim, H.; Kim, W.K.; Kim, J. Effect of stretching-based rehabilitation on pain, flexibility and muscle strength in dancers with hamstring injury: A single-blind, prospective, randomized clinical trial. J. Sports Med. Phys. Fit. 2018, 58, 1287–1295. [Google Scholar] [CrossRef]
- Sawle, L.; Freeman, J.; Marsden, J. A Pilot RCT investigating the effects of targeted compression on athletes with pelvic/groin pain. J. Sport Rehabil. 2019, 28, 133–143. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pae, C.-U. Why systematic review rather than narrative review? Psychiatry Investig 2015, 12, 417–419. [Google Scholar] [CrossRef] [Green Version]
- Jarosz, B.S. Individualized multi-modal management of osteitis pubis in an Australian Rules footballer. J. Chiropr. Med. 2011, 10, 105–110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nissen, T.; Wynn, R. The clinical case report: A review of its merits and limitations. BMC Res. Notes 2014, 7, 264. [Google Scholar] [CrossRef] [Green Version]
- Bruchmann, K. Compared to What? The importance of control groups in social comparison research. Basic Appl. Soc. Psychol. 2017, 39, 91–100. [Google Scholar] [CrossRef]
- Pithon, M.M. Importance of the control group in scientific research. Dent. Press J. Orthod. 2013, 18, 13–14. [Google Scholar] [CrossRef] [Green Version]
- Malay, S.; Chung, K.C. The choice of controls for providing validity and evidence in clinical research. Plast. Reconstr. Surg. 2012, 130, 959–965. [Google Scholar] [CrossRef]
- Lang, A.; Edwards, N.; Fleiszer, A. Empty systematic reviews: Hidden perils and lessons learned. J. Clin. Epidemiol. 2007, 60, 595–597. [Google Scholar] [CrossRef] [PubMed]
- Yaffe, J.; Montgomery, P.; Hopewell, S.; Shepard, L.D. Empty reviews: A description and consideration of cochrane systematic reviews with no included studies. PLoS ONE 2012, 7, e36626. [Google Scholar] [CrossRef]
- Weintraub, P.G. The importance of publishing negative results. J. Insect. Sci. 2016, 16, 109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nimpf, S.; Keays, D.A. Why (and how) we should publish negative data. EMBO Rep. 2020, 21, e49775. [Google Scholar] [CrossRef] [PubMed]
- Mlinarić, A.; Horvat, M.; Šupak Smolčić, V. Dealing with the positive publication bias: Why you should really publish your negative results. Biochem. Med. 2017, 27, 030201. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schlosser, R.W.; Hemsley, B.; Shane, H.; Todd, J.; Lang, R.; Lilienfeld, S.O.; Trembath, D.; Mostert, M.; Fong, S.; Odom, S. Rapid prompting method and autism spectrum disorder: Systematic review exposes lack of evidence. Rev. J. Autism Dev. Disord. 2019, 6, 403–412. [Google Scholar] [CrossRef] [Green Version]
- Slyer, J.T. Unanswered questions: Implications of an empty review. JBI Evid. Synth. 2016, 14, 1–2. [Google Scholar] [CrossRef]
- Green, S.; Higgins, J.P.; Schünemann, H.J.; Becker, L. Response to paper by Lang A, Edwards N, and Fleiszer, A. J. Clin. Epidemiol. 2007, 60, 598–599. [Google Scholar] [CrossRef] [PubMed]
- Faggion, C.M.; Bakas, N.P.; Wasiak, J. A survey of prevalence of narrative and systematic reviews in five major medical journals. BMC Med. Res. Methodol. 2017, 17, 176. [Google Scholar] [CrossRef] [Green Version]
- Lunny, C.; Ramasubbu, C.; Puil, L.; Liu, T.; Gerrish, S.; Salzwedel, D.M.; Mintzes, B.; Wright, J.M. Over half of clinical practice guidelines use non-systematic methods to inform recommendations: A methods study. PLoS ONE 2021, 16, e0250356. [Google Scholar] [CrossRef]
- Greenhalgh, T.; Thorne, S.; Malterud, K. Time to challenge the spurious hierarchy of systematic over narrative reviews? Eur. J. Clin. Investig. 2018, 48, e12931. [Google Scholar] [CrossRef]
- Afonso, J.; Bessa, C.; Nikolaidis, P.T.; Teoldo, I.; Clemente, F. A systematic review of research on Tactical Periodization: Absence of empirical data, burden of proof, and benefit of doubt. Hum. Mov. 2020, 21, 37–43. [Google Scholar] [CrossRef]
- Pigliucci, M.; Boudry, M. Prove it! The burden of proof game in science vs. pseudoscience disputes. Philosophia 2014, 42, 487–502. [Google Scholar] [CrossRef]
- Hamilton, B.; Best, T.M. Platelet-enriched plasma and muscle strain injuries: Challenges imposed by the burden of proof. Clin. J. Sport Med. 2011, 21, 31–36. [Google Scholar] [CrossRef] [PubMed]
- Koplin, J.J.; Selgelid, M.J. Burden of proof in bioethics. Bioethics 2015, 29, 597–603. [Google Scholar] [CrossRef] [PubMed]
- Windhaber, T.; Koula, M.L.; Ntzani, E.; Velivasi, A.; Rizos, E.; Doumas, M.T.; Pappas, E.E.; Onder, G.; Vetrano, D.L.; Roudriguez Laso, A.; et al. Educational strategies to train health care professionals across the education continuum on the process of frailty prevention and frailty management: A systematic review. Aging Clin. Exp. Res. 2018, 30, 1409–1415. [Google Scholar] [CrossRef] [Green Version]
- Laake-Geelen, C.C.M.v.; Smeets, R.J.E.M.; Quadflieg, S.P.A.B.; Kleijnen, J.; Verbunt, J.A. The effect of exercise therapy combined with psychological therapy on physical activity and quality of life in patients with painful diabetic neuropathy: A systematic review. Scand. J. Pain 2019, 19, 433–439. [Google Scholar] [CrossRef] [PubMed]
- Moyo, N.; Jones, M.; Kushemererwa, D.; Pantha, S.; Gilbert, S.; Romero, L.; Gray, R. The Association between the mental health nurse-to-registered nurse ratio and patient outcomes in psychiatric inpatient wards: A systematic review. Int. J. Environ. Res. Public Health 2020, 17, 6890. [Google Scholar] [CrossRef] [PubMed]
- Brukner, P.; Bradshaw, C.; McCrory, P. Obturator neuropathy: A cause of exercise-related groin pain. Phys. Sportsmed. 1999, 27, 62–73. [Google Scholar] [CrossRef]
- Hölmich, P. Adductor-related groin pain in athletes. Sports Med. Arthrosc. Rev. 1997, 5, 285–291. [Google Scholar]
- Grant, M.J.; Booth, A. A typology of reviews: An analysis of 14 review types and associated methodologies. Health Inf. Libr. J. 2009, 26, 91–108. [Google Scholar] [CrossRef]

{kind=link}
| Rule | Inclusion Criteria | Exclusion Criteria |
|---|---|---|
| Article type | Original research in peer-reviewed journals. No constraints regarding language and publication date. | Conference abstracts, books and book chapters, book reviews, editorials, letters to the editor, feasibility and pilot studies, trial registrations, reviews, essays, original research in non-peer-reviewed journals. |
| Participants | Athletes of any age, sex, and training status, diagnosed with GPI (or any equivalent term). | Athletes not diagnosed with GPI. Non-athletes. Non-human animals (e.g., experimental animal models). |
| Interventions | Stretching (e.g., static passive, static active, dynamic, proprioceptive neuromuscular facilitation, other). * | Interventions without stretching. Multimodal interventions (e.g., stretching combined with strength training). † |
| Comparators | Non-exercise controls under conservative care. Controls performing alternative exercise protocols (e.g., balance, strength-training). Multimodal programs including stretching. | Absence of comparators. |
| Outcomes | Primary outcomes Symptom remission (e.g., pain, discomfort, functional limitations); return to sport; return to play. Secondary outcomes (optional) Recurrence of symptoms. Perceived quality of life, functional assessments, strength levels, range of motion. Adverse effects arising from the interventions. | Absence of the pre-defined primary outcomes. |
| Study design | Randomized controlled trials (cluster, parallel or crossover), with no limitation regarding timeframe for follow-up. | Non-randomized studies. Case reports, case series, observational studies and similar designs. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Afonso, J.; Claudino, J.G.; Fonseca, H.; Moreira-Gonçalves, D.; Ferreira, V.; Almeida, J.M.; Clemente, F.M.; Ramirez-Campillo, R. Stretching for Recovery from Groin Pain or Injury in Athletes: A Critical and Systematic Review. J. Funct. Morphol. Kinesiol. 2021, 6, 73. https://doi.org/10.3390/jfmk6030073
Afonso J, Claudino JG, Fonseca H, Moreira-Gonçalves D, Ferreira V, Almeida JM, Clemente FM, Ramirez-Campillo R. Stretching for Recovery from Groin Pain or Injury in Athletes: A Critical and Systematic Review. Journal of Functional Morphology and Kinesiology. 2021; 6(3):73. https://doi.org/10.3390/jfmk6030073
Chicago/Turabian StyleAfonso, José, João Gustavo Claudino, Hélder Fonseca, Daniel Moreira-Gonçalves, Victor Ferreira, José Marques Almeida, Filipe Manuel Clemente, and Rodrigo Ramirez-Campillo. 2021. "Stretching for Recovery from Groin Pain or Injury in Athletes: A Critical and Systematic Review" Journal of Functional Morphology and Kinesiology 6, no. 3: 73. https://doi.org/10.3390/jfmk6030073
APA StyleAfonso, J., Claudino, J. G., Fonseca, H., Moreira-Gonçalves, D., Ferreira, V., Almeida, J. M., Clemente, F. M., & Ramirez-Campillo, R. (2021). Stretching for Recovery from Groin Pain or Injury in Athletes: A Critical and Systematic Review. Journal of Functional Morphology and Kinesiology, 6(3), 73. https://doi.org/10.3390/jfmk6030073