Effect of Kinesio® Taping on Ankle Complex Motion and Stiffness and Jump Landing Time to Stabilization in Female Ballet Dancers

 ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.3. Instrumentation
2.4. Data Collection
2.4.1. Taping Procedure
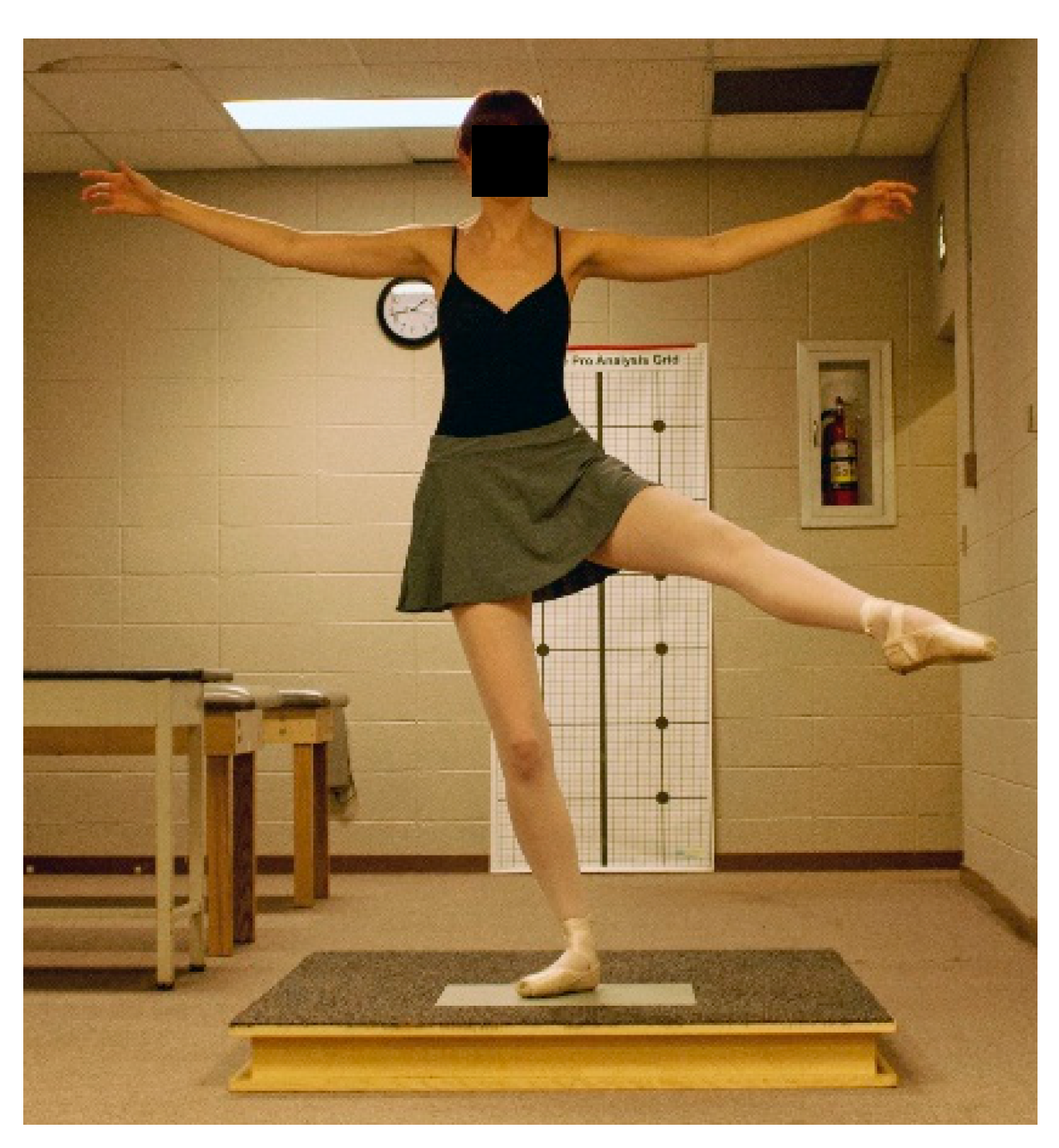
2.4.2. Ballet Jump Procedures
2.4.3. Ankle Arthrometric Procedures
2.4.4. Data Reduction and Statistical Analysis
3. Results
3.1. Ankle Complex Stability
3.2. Ankle Joint Range of Motion
3.3. Time to Stabilization
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Leanderson, J.; Eriksson, E.; Nilsson, C.; Wykman, A. Proprioception in classical ballet dancers: A prospective study of the influence of an ankle sprain on proprioception in the ankle joint. Am. J. Sports Med. 2016, 24, 370–374. [Google Scholar] [CrossRef]
- Wiesler, E.R.; Hunter, D.M.; Martin, D.F.; Curl, W.W.; Hoen, H. Ankle flexibility and injury patterns in dancers. Am. J. Sports Med. 1996, 24, 754–757. [Google Scholar] [CrossRef]
- Ahonen, J. Biomechanics of the foot in dance: A literature review. J. Dance Med. Sci. 2008, 12, 99–108. [Google Scholar] [PubMed]
- Bowling, A. Injuries to dancers: Prevalence, treatment, and perceptions of causes. Br. Med. J. 1989, 298, 731–734. [Google Scholar] [CrossRef]
- Byhring, S.; Bo, K. Musculoskeletal injuries in the Norwegian National Ballet: A prospective cohort study. Scand. J. Med. Sci. Sports 2002, 12, 365–370. [Google Scholar] [CrossRef]
- Ritter, S.; Moore, M. The relationship between lateral ankle sprain and ankle tendonitis in ballet dancers. J. Dance Med. Sci. 2008, 12, 23–31. [Google Scholar] [PubMed]
- Ewalt, K.L. Bandaging and taping considerations for the dancer. J. Dance Med. Sci. 2010, 14, 103–113. [Google Scholar]
- Lee, S.M.; Lee, J.H. The immediate effects of ankle balance taping with kinesiology tape on ankle active range of motion and performance in the Balance Error Scoring System. Phys. Ther. Sport 2017, 25, 99–105. [Google Scholar] [CrossRef]
- Ohman, A.M. Kinesiology taping a therapeutic tool in the paediatric population. J. Nov. Physiother. 2013, 3, 173–174. [Google Scholar] [CrossRef]
- Fayson, S.D.; Needle, A.R.; Kaminski, T.W. The effects of Kinesio taping on ankle stiffness and dynamic balance. Res. Sports Med. 2013, 21, 204–216. [Google Scholar] [CrossRef] [PubMed]
- Halseth, T.; McChesney, J.W.; DeBeliso, M.; Vaughn, R.; Lien, J. The effects of Kinesio taping on proprioception at the ankle. J. Sports Sci. Med. 2004, 3, 1–7. [Google Scholar]
- Wang, Y.; Gu, Y.; Chen, J.; Luo, W.; He, W.; Han, Z.; Tian, J. Kinesio taping is superior to other taping methods in ankle functional performance improvement: A systematic review and meta-analysis. Clin. Rehabil. 2018, 32, 1472–1481. [Google Scholar] [CrossRef]
- Huang, C.Y.; Hsieh, T.H.; Lu, S.C.; Su, F.C. Effect of Kinesio tape to muscle activity and vertical jump performance in healthy inactive people. BioMed Eng. OnLine 2010, 10, 70–80. [Google Scholar] [CrossRef]
- Nakajima, M.; Baldridge, C. The effect of Kinesio Tape on vertical jump and dynamic postural control. Int. J. Sports Phys. Ther. 2013, 8, 393–406. [Google Scholar]
- Costa de Mello, M.; de Sá Ferreira, A.; Felicio, L.R. Postural control during different unipodal positions in professional ballet dancers. J. Dance Med. Sci. 2017, 21, 151–155. [Google Scholar] [CrossRef]
- da Costa, P.H.L.; Nora, F.G.S.A.; Vieira, M.F.; Bosch, K.; Rosenbaum, D. Single-leg balancing in ballet: Effects of shoe conditions and poses. Gait Posture 2013, 27, 419–423. [Google Scholar] [CrossRef]
- Lin, C.; Lee, I.; Liao, J.; Wu, H.; Su, G. Comparison of postural stability between injured and uninjured ballet dancers. Am. J. Sports Med. 2011, 36, 1324–1331. [Google Scholar] [CrossRef]
- Hubbard, T.J.; Kovaleski, J.E.; Kaminski, T.W. Reliability of intratester and intertester measurement derived from an instrumented ankle arthrometer. J. Sport Rehabil. 2003, 12, 208–220. [Google Scholar] [CrossRef]
- Kovaleski, J.E.; Hollis, J.M.; Heitman, R.J.; Gurchiek, L.R.; Pearsall, A.W. Assessment of ankle-subtalar-joint-complex laxity using an instrumented ankle arthrometer: An experimental cadaveric investigation. J. Athl. Train. 2002, 37, 467–474. [Google Scholar]
- Kovaleski, J.E.; Gurchiek, L.R.; Heitman, R.J.; Hollis, J.M.; Pearsall, A.W. Instrumented measurement of anteroposterior and inversion-eversion laxity of the normal ankle joint complex. Foot Ankle Int. 1999, 20, 808–814. [Google Scholar] [CrossRef]
- Kovaleski, J.E.; Norrell, P.M.; Heitman, R.J.; Hollis, J.M.; Pearsall, A.W. Knee and ankle position, anterior drawer laxity, and stiffness of the ankle complex. J. Athl. Train. 2008, 43, 242–248. [Google Scholar] [CrossRef]
- Bruyneel, A.V.; Mesure, S.; Pare, J.C.; Bertrand, M. Organization of postural equilibrium in several planes in ballet dancers. Neurosci. Lett. 2010, 485, 228–232. [Google Scholar] [CrossRef]
- Kovaleski, J.E.; Heitman, R.J.; Gurchiek, L.R.; Hollis, J.M.; Liu, W.; Pearsall, A.W. Joint stability characteristics of the ankle complex after lateral ligamentous injury, part I: A laboratory comparison using arthrometric measurement. J. Athl. Train. 2014, 49, 192–197. [Google Scholar] [CrossRef]
- Colby, S.M.; Hintermeister, R.A.; Torry, M.R.; Steadman, J.R. Lower limb stability with ACL impairment. J. Orthop. Sports Phys. Ther. 1999, 29, 444–454. [Google Scholar] [CrossRef]
- Ross, S.E.; Guskiewicz, K.M. Time to stabilization: A method for analyzing dynamic postural stability. Athl. Ther. Today 2003, 8, 37–39. [Google Scholar]
- Wikstrom, E.; Tillman, M.; Borsa, P. Detection of dynamic stability deficits in subjects with functional ankle instability. Med. Sci. Sports Exerc. 2005, 37, 169–175. [Google Scholar] [CrossRef]
- Milan, K.B. Injury in ballet: A review of relevant topics for the physical therapist. J. Orthop. Sports Phys. Ther. 1994, 19, 121–129. [Google Scholar] [CrossRef][Green Version]
- Nilsson, C.; Leanderson, J.; Wykman, A.; Strender, L. The injury panorama in a Swedish professional ballet company. Knee Surg. Sports Traumatol. Arthrosc. 2001, 9, 242–246. [Google Scholar] [CrossRef]
- Quirk, R. Ballet injuries: The Australian experience. Clin. Sports Med. 1983, 2, 507–514. [Google Scholar]
- Leardini, A.; O’Connor, J.J.; Catani, F.; Giannini, S. The role of the passive structures in the mobility and stability of the human ankle joint: A literature review. Foot Ankle Int. 2000, 21, 602–615. [Google Scholar] [CrossRef]
- Tohyama, H.; Beynnon, B.D.; Renstrom, P.A.; Theis, M.J.; Fleming, B.C.; Pope, M.H. Biomechanical analysis of the ankle anterior drawer and talar tilt tests for anterior talofibular injuries. J. Orthop. Res. 1995, 13, 609–614. [Google Scholar] [CrossRef]
- Grigg, P. Peripheral neural mechanisms in proprioception. J. Sport Rehabil. 1994, 3, 2–17. [Google Scholar] [CrossRef]
- Stoffel, K.K.; Nicholls, R.L.; Winata, A.R.; Dempsey, A.R.; Boyle, J.J.; Lloyd, D.G. Effect of ankle taping on knee and ankle joint biomechanics in sporting tasks. Med. Sci. Sports Exerc. 2010, 42, 2089–2097. [Google Scholar] [CrossRef]
- Wikstrom, E.A.; Arrigenna, M.A.; Tillman, M.D.; Borsa, P.A. Dynamic postural stability in subjects with braced, functionally unstable ankles. J. Athl. Train. 2006, 41, 245–250. [Google Scholar]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Support Condition | Anterior Displacement (mm) | Posterior Displacement (mm) | Inversion (° ROM) | Eversion (° ROM) |
|---|---|---|---|---|
| Kinesio Tape | 10.00 ± 3.3 | 10.36 ± 3.2 | 28.17 ± 6.7 a | 23.37 ± 4.9 b |
| No Tape | 12.12 ± 3.5 | 11.64 ± 3.4 | 35.96 ± 9.1 | 28.14 ± 8.3 |
| Sham-KT | 11.08 ± 3.4 | 11.48 ± 2.3 | 32.68 ± 5.7 | 26.05 ± 5.5 |
| Anterior (N·mm) | Posterior (N·mm) | Inversion (N·M/°) | Eversion (N·M/°) | |||||
|---|---|---|---|---|---|---|---|---|
| Low Load Range | High Load Range | Low Load Range | High Load Range | Low Load Range | High Load Range | Low Load Range | High Load Range | |
| KT | 10.91 ± 6.3 | 10.75 ± 4.7 | 14.12 ± 8.7 | 10.39 ± 4.5 | 0.167 ± 0.07 a | 0.157 ± 0.03 | 0.196 ± 0.08 | 0.191 ± 0.03 |
| NT | 9.03 ± 4.1 | 9.86 ± 2.5 | 10.90 ± 3.9 | 9.30 ± 4.7 | 0.102 ± 0.04 | 0.180 ± 0.05 | 0.165 ± 0.11 | 0.187 ± 0.04 |
| ST | 10.21 ± 4.2 | 10.82 ± 5.9 | 11.31 ± 3.6 | 8.71 ± 3.3 | 0.111 ± 0.04 b | 0.175 ± 0.02 | 0.176 ± 0.08 | 0.183 ± 0.04 |
| Support Condition | Jump Type | Time-to-Stabilization(s) |
|---|---|---|
| Kinesio Tape No Tape Sham-Kinesio Tape | JA | 0.583 ± 0.13 |
| JA | 0.651 ± 0.21 | |
| JA | 0.555 ± 0.15 | |
| Kinesio Tape No Tape Sham-Kinesio Tape | JF | 0.626 ± 0.13 |
| JF | 0.628 ± 0.12 | |
| JF | 0.634 ± 0.09 | |
| Kinesio Tape No Tape Sham-Kinesio Tape | JS | 0.585 ± 0.13 |
| JS | 0.592 ± 0.12 | |
| JS | 0.617 ± 0.33 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Botsis, A.E.; Schwarz, N.A.; Harper, M.E.; Liu, W.; Rooney, C.A.; Gurchiek, L.R.; Kovaleski, J.E. Effect of Kinesio® Taping on Ankle Complex Motion and Stiffness and Jump Landing Time to Stabilization in Female Ballet Dancers. J. Funct. Morphol. Kinesiol. 2019, 4, 19. https://doi.org/10.3390/jfmk4020019
Botsis AE, Schwarz NA, Harper ME, Liu W, Rooney CA, Gurchiek LR, Kovaleski JE. Effect of Kinesio® Taping on Ankle Complex Motion and Stiffness and Jump Landing Time to Stabilization in Female Ballet Dancers. Journal of Functional Morphology and Kinesiology. 2019; 4(2):19. https://doi.org/10.3390/jfmk4020019
Chicago/Turabian StyleBotsis, Aline E., Neil A. Schwarz, Megan E. Harper, Wei Liu, Collin A. Rooney, Larry R. Gurchiek, and John E. Kovaleski. 2019. "Effect of Kinesio® Taping on Ankle Complex Motion and Stiffness and Jump Landing Time to Stabilization in Female Ballet Dancers" Journal of Functional Morphology and Kinesiology 4, no. 2: 19. https://doi.org/10.3390/jfmk4020019
APA StyleBotsis, A. E., Schwarz, N. A., Harper, M. E., Liu, W., Rooney, C. A., Gurchiek, L. R., & Kovaleski, J. E. (2019). Effect of Kinesio® Taping on Ankle Complex Motion and Stiffness and Jump Landing Time to Stabilization in Female Ballet Dancers. Journal of Functional Morphology and Kinesiology, 4(2), 19. https://doi.org/10.3390/jfmk4020019