Hamstrings and Quadriceps Muscles Function in Subjects with Prior ACL Reconstruction Surgery



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Experimental Protocol
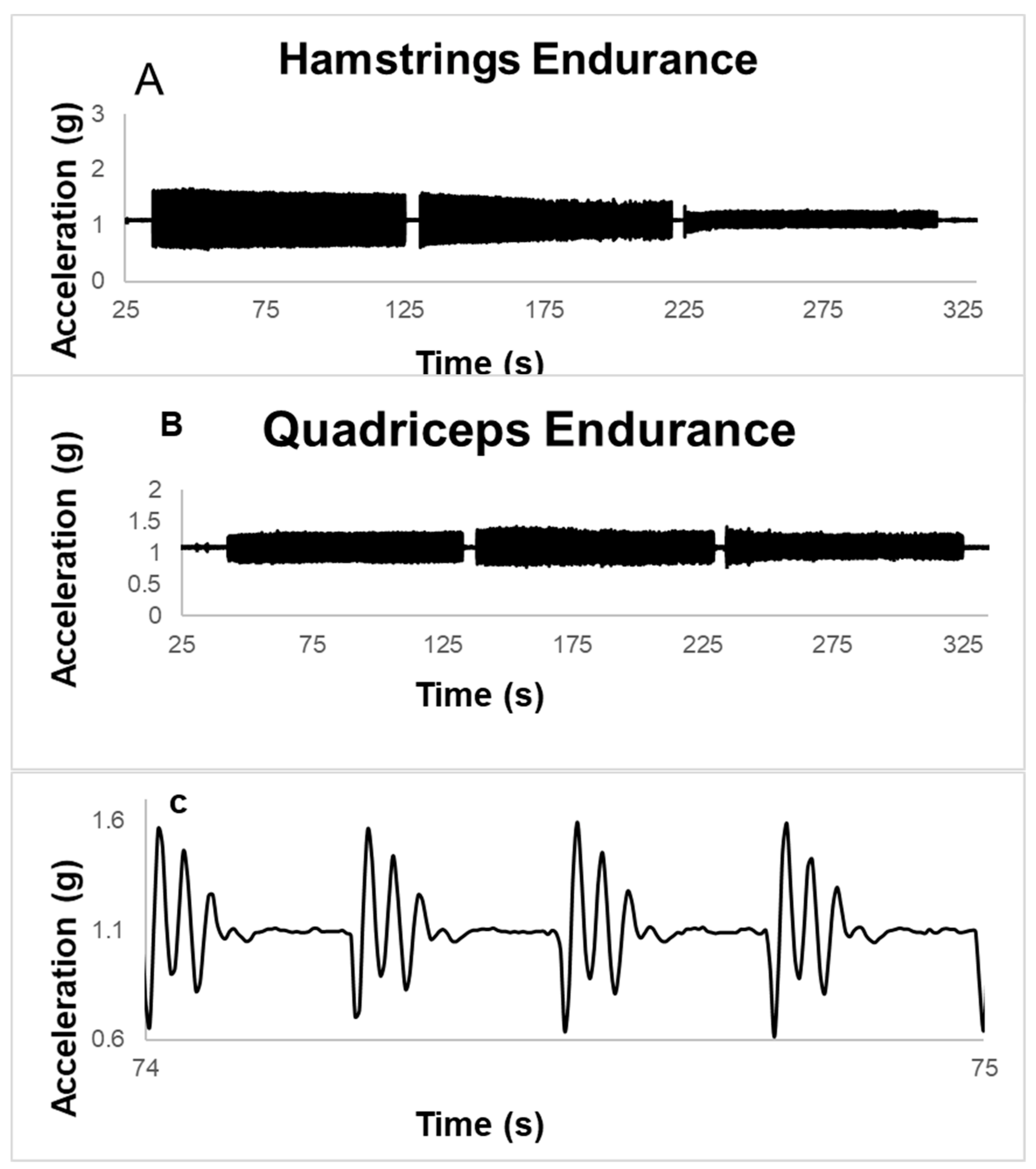
2.3. Endurance Test
2.4. Muscle Strength
2.5. Data Analysis
2.6. Statistical Analysis
3. Results
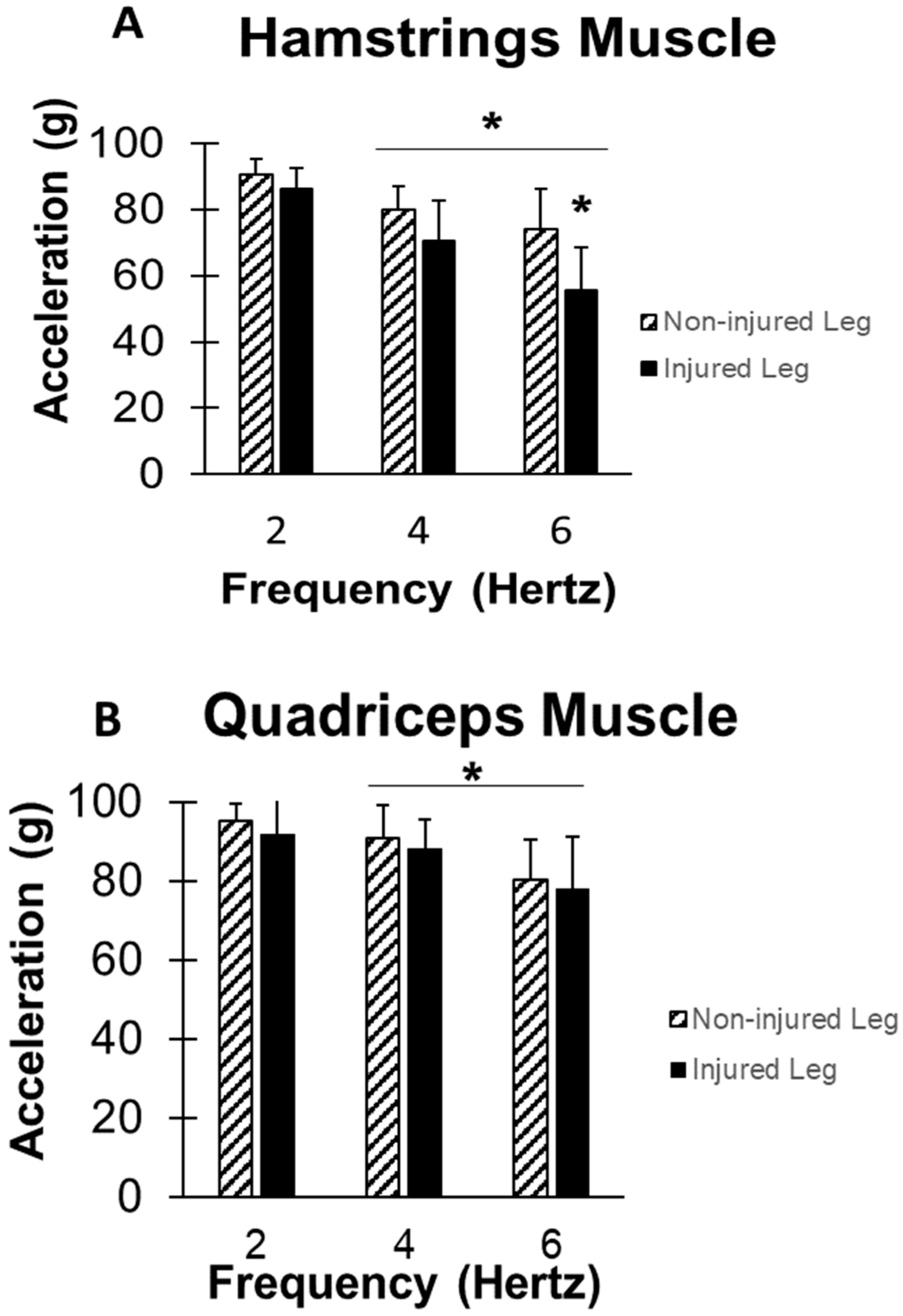
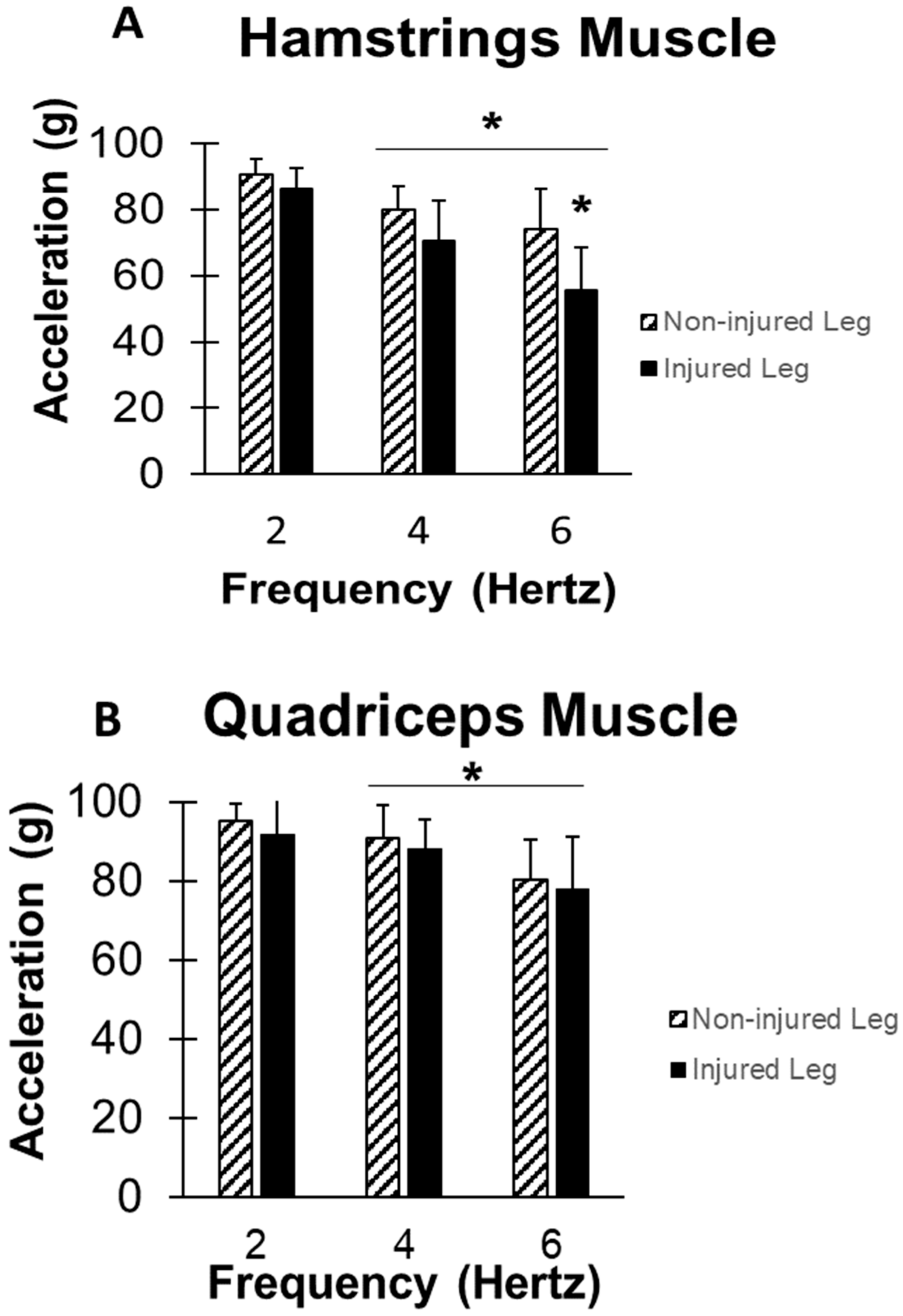
3.1. Hamstring Endurance
3.2. Quadriceps Endurance
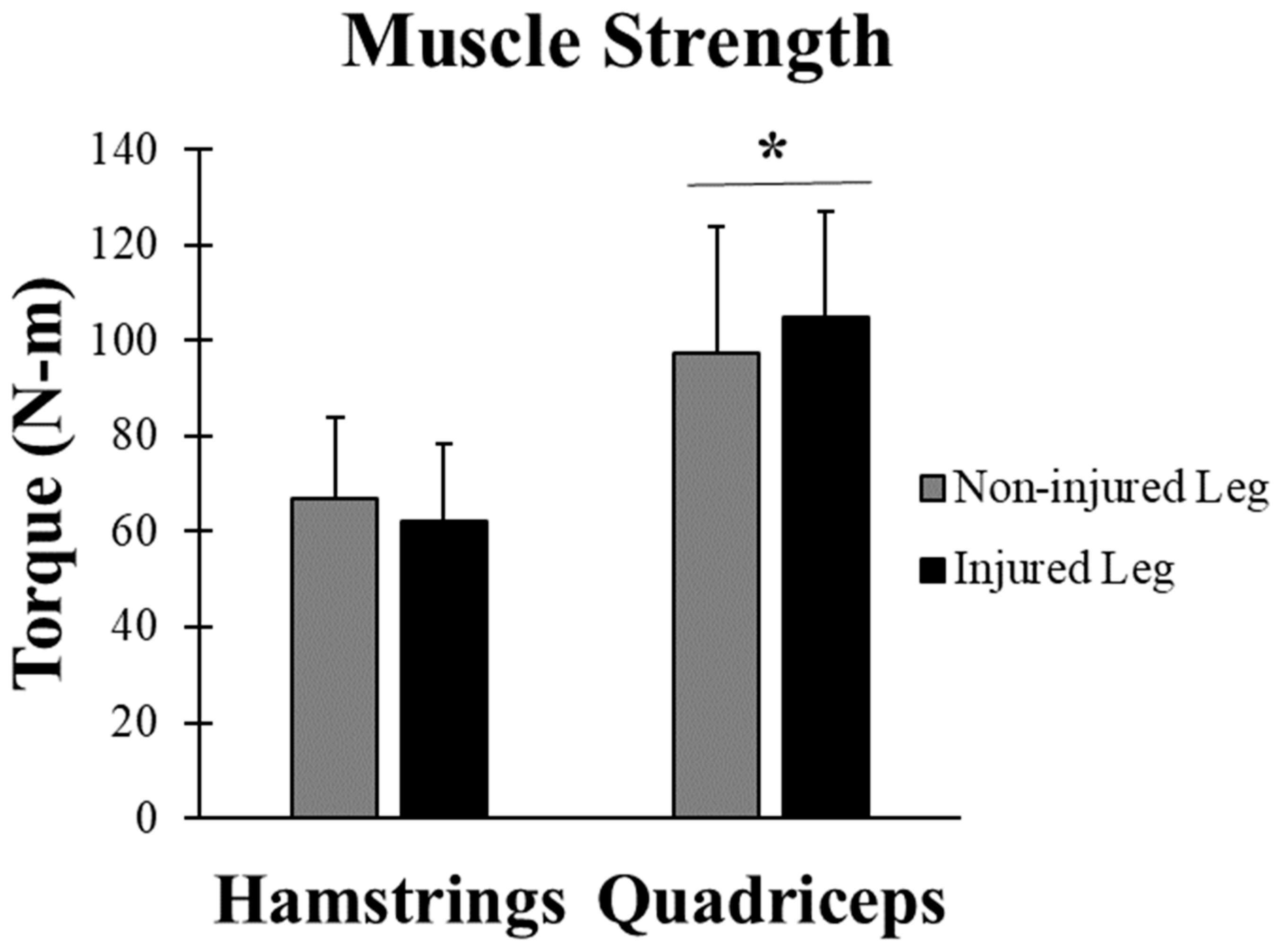
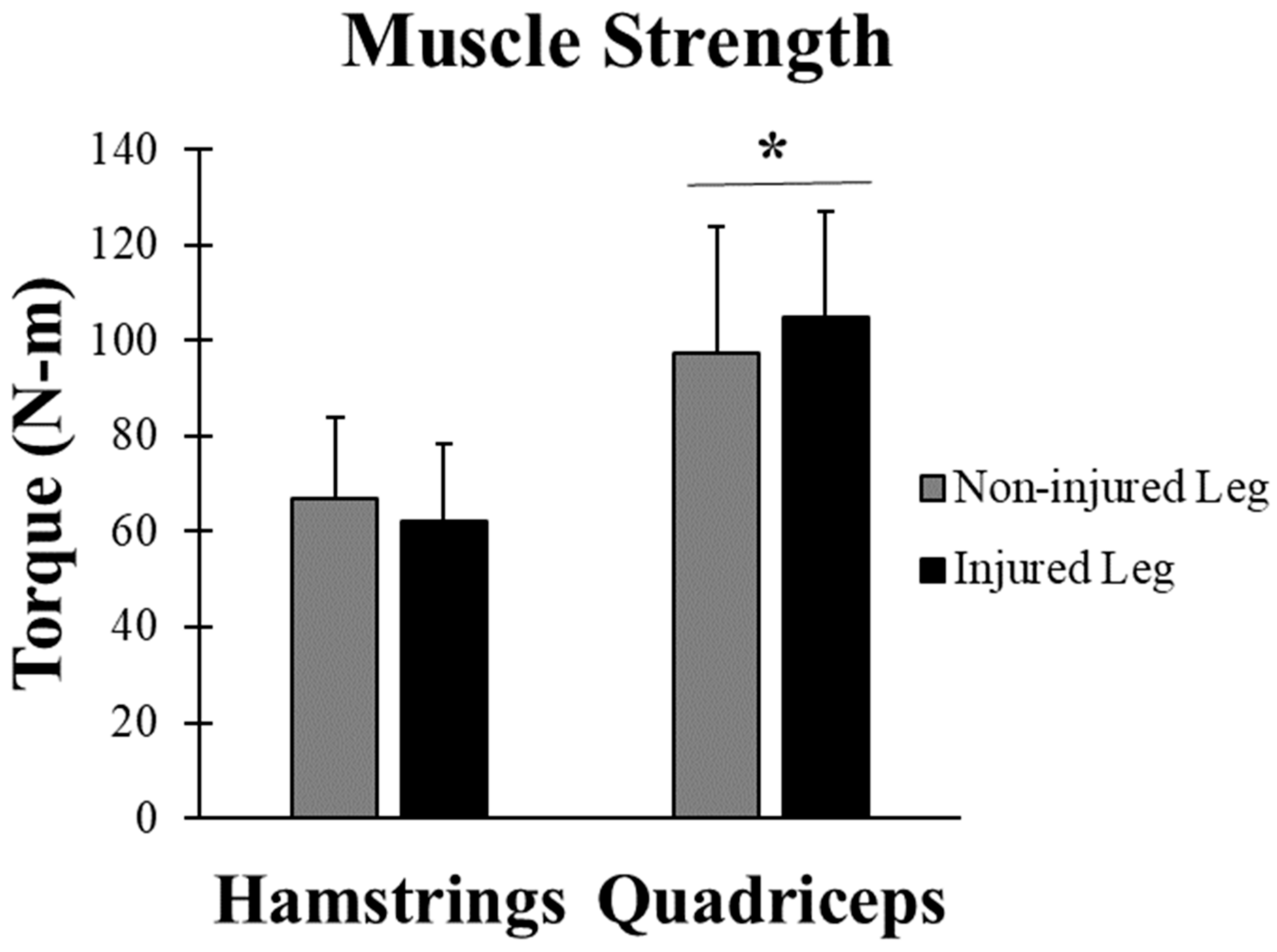
3.3. Muscle Strength
4. Discussion
5. Conclusion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Parkkari, J.; Pasanen, K.; Mattila, V.M.; Kannus, P.; Rimpela, A. The risk for a cruciate ligament injury of the knee in adolescents and young adults: A population-based cohort study of 46 500 people with a 9 year follow-up. Br. J. Sports Med. 2008, 6, 422–426. [Google Scholar] [CrossRef] [PubMed]
- Thomas, A.C.; Villwock, M.; Wojtys, E.M.; Palmieri-Smith, R.M. Lower Extremity Muscle Strength after Anterior Cruciate Ligament Injury and Reconstruction. J. Athl. Train. 2013, 48, 610–620. [Google Scholar] [CrossRef] [PubMed]
- Majewski, M.; Susanne, H.; Klaus, S. Epidemiology of athletic knee injuries: A 10-year study. Knee 2006, 3, 184–188. [Google Scholar] [CrossRef] [PubMed]
- Hewett, T.E.; Myer, G.D.; Ford, K.R.; Heidt, R.S., Jr.; Colosimo, A.J.; McLean, S.G.; van den Bogert, A.J.; Paterno, M.V.; Succop, p. Biomechanical measures of neuromuscular control and valgus loading of the knee predict anterior cruciate ligament injury risk in female athletes: A prospective study. Am. J. Sports Med. 2005, 4, 492–501. [Google Scholar] [CrossRef] [PubMed]
- Behrens, M.; Mau-Moeller, A.; Wassermann, F.; Bruhn, S. Effect of Fatigue on Hamstring Reflex Responses and Posterior-Anterior Tibial Translation in Men and Women. PLoS ONE 2013, 8, e56988. [Google Scholar] [CrossRef] [PubMed]
- Thomee, R.; Kaplan, Y.; Kvist, J.; Myklebust, G.; Risberg, M.A.; Theisen, D.; Tsepis, E.; Werner, s.; Wondrasch, B.; Witvrouw, E. Muscle strength and hop performance criteria prior to return to sports after ACL reconstruction. Knee Surg. Sports Traumatol. Arthrosc. 2011, 11, 1798–1805. [Google Scholar] [CrossRef] [PubMed]
- Kruse, L.M.; Gray, B.; Wright, R.W. Rehabilitation after anterior cruciate ligament reconstruction: A systematic review. J. Bone Joint Surg. Am. 2012, 19, 1737–1748. [Google Scholar] [CrossRef] [PubMed]
- Arden, C.L.; Webster, K.E.; Taylor, N.F.; Feller, J.A. Return to sports following anterior cruciate ligament reconstruction surgery: A systematic review an meta-analysis of the state of play. Br. J. Sports Med. 2011, 45, 596–606. [Google Scholar] [CrossRef] [PubMed]
- Biggs, A.; Jenkins, W.L.; Urch, S.E.; Shelbourne, K.D. Rehabilitation for Patients Following ACL Reconstruction: A Knee Symmetry Model. N. Am. J. Sports Phys. Ther. 2009, 1, 2–12. [Google Scholar]
- Decarlo, M.S.; Shelbourne, K.D.; McCarroll, J.R.; Rettig, A.C. Traditional versus Accelerated Rehabilitation following ACL Reconstruction: A One-Year Follow-Up. J. Orthop. Sports Phys. Ther. 1992, 6, 309–316. [Google Scholar] [CrossRef] [PubMed]
- Liu-Ambrose, T.; Taunton, J.E.; MacIntyre, D.; McConkey, P.; Khan, K.M. The effects of proprioceptive or strength training on the neuromuscular function of the ACL reconstructed knee: A randomized clinical trial. Scand. J. Med. Sci. Sports 2003, 2, 115–123. [Google Scholar] [CrossRef]
- Willingham, T.B.; McCully, K.K. Assessment of Skeletal Muscle Endurance Using Twitch Electrical Stimulation and Accelerometer-Based Mechanomyography. Adv. Skelet. Muscle Funct. Assess. 2017, 2, 9–15. [Google Scholar]
- Kent-Braun, J.A.; Sharma, K.R.; Miller, R.G.; Weiner, M.W. Postexercise phosphocreatine resynthesis is slowed in multiple sclerosis. Muscle Nerve 1994, 8, 835–841. [Google Scholar] [CrossRef] [PubMed]
- Bossie, H.M.; Willingham, T.B.; Schoick, R.A.V.; O’Connor, P.J.; McCully, K.K. Mitochondrial capacity, muscle endurance, and low energy in friedreich ataxia. Muscle Nerve 2017, 4, 773–779. [Google Scholar] [CrossRef] [PubMed]
- Pincivero, D.M.; Lephart, S.M.; Karunakara, R.A. Reliability and precision of isokinetic strength and muscular endurance for the quadriceps and hamstrings. Int. J. Sports Med. 1997, 2, 113–117. [Google Scholar] [CrossRef] [PubMed]
- Lowe, T.; Dong, X.N. The Use of Hamstring Fatigue to Reduce Quadriceps Inhibition after Anterior Cruciate Ligament Reconstruction. Percept. Motor Skills 2018, 125, 81–92. [Google Scholar] [CrossRef] [PubMed]
- Wojtys, E.M.; Huston, L.J. Longitudinal effects of anterior cruciate ligament injury and patellar tendon autograft reconstruction on neuromuscular performance. Am. J. Sports Med. 2000, 3, 336–344. [Google Scholar] [CrossRef] [PubMed]
- Vairo, G.L. Knee flexor strength and endurance profiles after ipsilateral hamstring tendons anterior cruciate ligament reconstruction. Arch. Phys. Med. Rehabil. 2014, 3, 552–561. [Google Scholar] [CrossRef] [PubMed]
- Werner, D.M.; Barrios, J.A. Trunk Muscle Endurance in Individuals with and Without a History of Anterior Cruciate Ligament Reconstruction. J. Strength Cond. Res. 2018. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.J.; Lee, J.H.; Ahn, S.E.; Park, M.J.; Lee, D.H. Influence of Anterior Cruciate Ligament Tear on Thigh Muscle Strength and Hamstring-to-Quadriceps Ratio: A Meta-Analysis. PLoS ONE 2016, 1, e0146234. [Google Scholar] [CrossRef] [PubMed]
- Chung, K.S.; Ha, J.K.; Yeom, C.H.; Ra, H.J.; Lim, J.W.; Kwon, M.S.; Kim, J.G. Are Muscle Strength and Function of the Uninjured Lower Limb Weakened After Anterior Cruciate Ligament Injury? Two-Year Follow-up after Reconstruction. Am. J. Sports Med. 2015, 12, 3013–3021. [Google Scholar] [CrossRef] [PubMed]
- Rosene, J.M.; Fogarty, T.D.; Mahaffey, B.L. Isokinetic Hamstrings: Quadriceps Ratio in Intercollegiate Athletes. J. Athl. Train. 2001, 4, 378–383. [Google Scholar]
- Paterno, M.V.; Rauh, M.J.; Schmitt, L.C.; Ford, K.R.; Hewett, T.E. Incidence of Second ACL Injuries 2 Years After Primary ACL Reconstruction and Return to Sport. Am. J. Sports Med. 2014, 7, 1567–1573. [Google Scholar] [CrossRef] [PubMed]
- Dhammi, I.K.; Rehan-UI-Haq Kumar, S. Graft choices for anterior cruciate ligament reconstruction. Indian J. Orthop. 2015, 2, 127–128. [Google Scholar] [CrossRef] [PubMed]
- Sutton, K.M.; Bullock, J.M. Anterior cruciate ligament rupture: Differences between males and females. J. Am. Acad. Orthop. Surg. 2013, 1, 41–50. [Google Scholar] [CrossRef] [PubMed]
- Cheung, E.C.; Boguszewski, D.V.; Joshi, N.B.; Wang, D.; McAllister, D.R. Anatomic Factors that May Predispose Female Athletes to Anterior Cruciate Ligament Injury. Curr. Sports Med. Rep. 2015, 5, 368–372. [Google Scholar] [CrossRef] [PubMed]
- Jenkins, W.L.; Killian, C.B.; Williams, D.S., 3rd; Loudon, J.; Raedeke, S.G. Anterior cruciate ligament injury in female and male athletes: The relationship between foot structure and injury. J. Am. Podiatr. Med. Assoc. 2007, 5, 371–376. [Google Scholar] [CrossRef]
- Stijak, L.; Blagojevic, Z.; Santrac-Stijak, G.; Spasojevic, G.; Herzog, R.; Filipovic, B. Predicting ACL rupture in the population actively engaged in sports activities based on anatomical risk factors. Orthopedics 2011, 6, 431. [Google Scholar] [CrossRef] [PubMed]
- Paterno, M.V.; Weed, A.M.; Hewett, T.E. A between sex comparison of anterior-posterior knee laxity after anterior cruciate ligament reconstruction with patellar tendon or hamstrings autograft: A systematic review. Sports Med 2012, 2, 135–152. [Google Scholar] [CrossRef] [PubMed]
- Devan, M.R.; Pescatello, L.S.; Faghri, P.; Anderson, J. A Prospective Study of Overuse Knee Injuries among Female Athletes with Muscle Imbalances and Structural Abnormalities. J. Athl. Train. 2004, 3, 263–267. [Google Scholar]
- Joseph, A.M.; Collins, C.L.; Henke, N.M.; Yard, E.E.; Fields, S.K.; Comstock, R.D. A multisport epidemiologic comparison of anterior cruciate ligament injuries in high school athletics. J. Athl. Train. 2013, 6, 810–817. [Google Scholar] [CrossRef] [PubMed]
- Van Grinsven, S.; van Cingel, R.E.; Holla, C.J.; van Loon, C.J. Evidence-based rehabilitation following anterior cruciate ligament reconstruction. Knee Surg. Sports Traumatol. Arthrosc. 2010, 8, 1128–1144. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Subject | Gender | Age (yr) | Weight (kg) | Height (cm) | BMI (kg·m−2) | Time After Surgery (months) | Graft Type | Previous Physical Activity |
|---|---|---|---|---|---|---|---|---|
| 1 | F | 19 | 61.2 | 162.6 | 23.2 | 29 | Quadriceps | Occasional rock climbing |
| 2 | F | 21 | 65.8 | 167.6 | 23.4 | 59 | Hamstrings | Running 4×/week + weights |
| 3 | F | 21 | 65.8 | 160.0 | 25.7 | 39 | Cadaver | Running 4×/week + weights |
| 4 | F | 21 | 63.5 | 167.6 | 22.6 | 36 | Patella Tendon | Elliptical 4×/week + weights |
| 5 | F | 21 | 55.3 | 170.2 | 19.1 | 48 | Hamstrings | Running 4×/week + weights |
| 6 | F | 22 | 56.7 | 154.9 | 23.6 | 94 | Hamstrings | Running 5×/week + weights |
| 7 | F | 21 | 69.9 | 170.2 | 24.1 | 84 | Hamstrings | Cycle 2×/week, soccer 1×/week. + weights |
| 8 | F | 31 | 64.4 | 167.6 | 22.9 | 43 | Cadaver | 2mi 2×/week + weights |
| Mean ± SD | 22.1 ± 3.7 | 62.8 ± 4.9 | 165. ± 5.4 | 22.1 ± 3.7 | 54 ± 23.5 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Faxon, J.L.; Sanni, A.A.; McCully, K.K. Hamstrings and Quadriceps Muscles Function in Subjects with Prior ACL Reconstruction Surgery. J. Funct. Morphol. Kinesiol. 2018, 3, 56. https://doi.org/10.3390/jfmk3040056
Faxon JL, Sanni AA, McCully KK. Hamstrings and Quadriceps Muscles Function in Subjects with Prior ACL Reconstruction Surgery. Journal of Functional Morphology and Kinesiology. 2018; 3(4):56. https://doi.org/10.3390/jfmk3040056
Chicago/Turabian StyleFaxon, Jamie L., Adeola A. Sanni, and Kevin K. McCully. 2018. "Hamstrings and Quadriceps Muscles Function in Subjects with Prior ACL Reconstruction Surgery" Journal of Functional Morphology and Kinesiology 3, no. 4: 56. https://doi.org/10.3390/jfmk3040056
APA StyleFaxon, J. L., Sanni, A. A., & McCully, K. K. (2018). Hamstrings and Quadriceps Muscles Function in Subjects with Prior ACL Reconstruction Surgery. Journal of Functional Morphology and Kinesiology, 3(4), 56. https://doi.org/10.3390/jfmk3040056