
Effects of 12 Weeks of Interval Block Resistance Training Versus Circuit Resistance Training on Body Composition, Performance, and Autonomic Recovery in Adults: Randomized Controlled Trial

 , , , , , , , , , ,
, , , , , , , , , , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Design
2.2. Eligibility
2.2.1. Inclusion Criteria
- Aged between 18 and 30 years and classified as a physically active adult.
- Refrain from engaging in moderate or intense physical activity during the 48 h prior to each session to prevent interference with acute training responses.
- Attend all scheduled training sessions punctually throughout the 12-week intervention.
- Read, understand, and sign the informed consent form before undergoing evaluations.
2.2.2. Exclusion Criteria
- Diagnosis of conditions such as hypertension, type 2 diabetes, coronary artery disease, or other cardiovascular, metabolic disorders, or inability to exercise due to injury.
- Body mass index within the overweight or obese range, along with a waist circumference exceeding the high cardiometabolic risk threshold of 88 cm for the Chilean adult population.
- Hand grip strength below the threshold 50 kg was considered a risk of muscle weakness in the classification for the Chilean adult population
- Performance below the 644 m reference threshold for reduced functional capacity in the Chilean adult population.
- Participation in another training program during the intervention, which could interfere with the study protocol response.
2.3. Training Protocols
- The experimental group followed an IBRT protocol, where each set consisted of a different exercise in the session (Set 1: Push-up, Set 2: Mountain climber, Set 3: Squat, Set 4: Jumping Jack, Set 5: Burpees, Set 6: Skipping).
- The control group followed a CRT protocol, in which all six exercises were performed sequentially within each set, and this same circuit was repeated across all sets.
2.3.1. Level of Physical Activity
2.3.2. Body Composition
2.3.3. Hand Grip Strength
2.3.4. Running Anaerobic Sprint Test
2.3.5. Six Min Walking Test
2.3.6. Autonomic Recovery
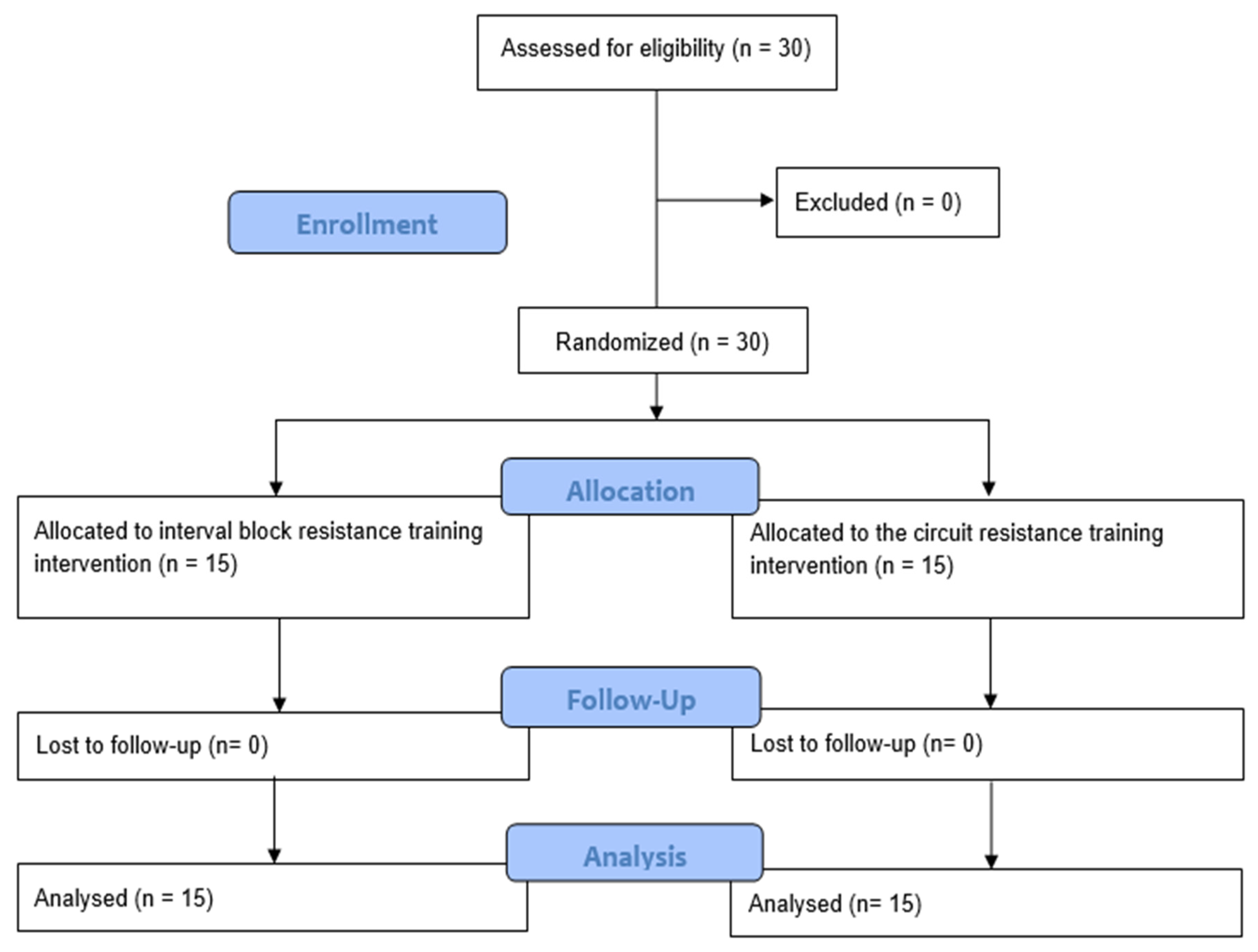
2.4. Randomization
2.5. Blinding
2.6. Sample Size and Statistical Power
2.7. Data Analysis
3. Results
4. Discussion
5. Clinical and Practical Implications
6. Limitations and Future Directions
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Buckner, S.L.; Jessee, M.B.; Mouser, J.G.; Dankel, S.J.; Mattocks, K.T.; Bell, Z.W.; Abe, T.; Loenneke, J.P. The Basics of Training for Muscle Size and Strength: A Brief Review on the Theory. Med. Sci. Sports Exerc. 2020, 52, 645–653. [Google Scholar] [CrossRef] [PubMed]
- Issurin, V. Block periodization versus traditional training theory: A review. J. Sports Med. Phys. Fit. 2008, 48, 65–75. [Google Scholar]
- Issurin, V.B. Biological Background of Block Periodized Endurance Training: A Review. Sports Med. 2019, 49, 31–39. [Google Scholar] [CrossRef]
- Issurin, V.B. Benefits and Limitations of Block Periodized Training Approaches to Athletes’ Preparation: A Review. Sports Med. 2016, 46, 329–338. [Google Scholar] [CrossRef]
- Zaryski, C.; Smith, D.J. Training principles and issues for ultra-endurance athletes. Curr. Sports Med. Rep. 2005, 4, 165–170. [Google Scholar] [CrossRef] [PubMed]
- Granacher, U.; Behm, D.G. Relevance and Effectiveness of Combined Resistance and Balance Training to Improve Balance and Muscular Fitness in Healthy Youth and Youth Athletes: A Scoping Review. Sports Med. 2023, 53, 349–370. [Google Scholar] [CrossRef]
- Moquin, P.A.; Wetmore, A.B.; Carroll, K.M.; Fry, A.C.; Hornsby, W.G.; Stone, M.H. Lean Body Mass and Muscle Cross-Sectional Area Adaptations Among College Age Males with Different Strength Levels across 11 Weeks of Block Periodized Programmed Resistance Training. Int. J. Environ. Res. Public Health 2021, 18, 4735. [Google Scholar] [CrossRef] [PubMed]
- Stone, M.H.; Hornsby, W.G.; Haff, G.G.; Fry, A.C.; Suarez, D.G.; Liu, J.; Gonzalez-Rave, J.M.; Pierce, K.C. Periodization and Block Periodization in Sports: Emphasis on Strength-Power Training-A Provocative and Challenging Narrative. J. Strength Cond. Res. 2021, 35, 2351–2371. [Google Scholar] [CrossRef]
- Mølmen, K.S.; Øfsteng, S.J.; Rønnestad, B.R. Block periodization of endurance training—a systematic review and meta-analysis. Open Access J. Sports Med. 2019, 10, 145–160. [Google Scholar] [CrossRef]
- Gavanda, S.; Geisler, S.; Quitmann, O.J.; Bauhaus, H.; Schiffer, T. Three Weeks of Detraining Does Not Decrease Muscle Thickness, Strength or Sport Performance in Adolescent Athletes. Int. J. Exerc. Sci. 2020, 13, 633–644. [Google Scholar]
- Chen, H.; Xu, K.; Sun, C.; Gui, S.; Wu, J.; Wang, S. Inhibition of ANGPT2 activates autophagy during hypertrophic scar formation via PI3K/AKT/mTOR pathway. An. Bras. Dermatol. 2023, 98, 26–35. [Google Scholar] [CrossRef] [PubMed]
- Kuikman, M.A.; Coates, A.M.; Burr, J.F. Markers of Low Energy Availability in Overreached Athletes: A Systematic Review and Meta-analysis. Sports Med. 2022, 52, 2925–2941. [Google Scholar] [CrossRef] [PubMed]
- Pliauga, V.; Lukonaitiene, I.; Kamandulis, S.; Skurvydas, A.; Sakalauskas, R.; Scanlan, A.T.; Stanislovaitiene, J.; Conte, D. The effect of block and traditional periodization training models on jump and sprint performance in collegiate basketball players. Biol. Sport. 2018, 35, 373–382. [Google Scholar] [CrossRef] [PubMed]
- Rønnestad, B.R.; Øfsteng, S.J.; Ellefsen, S. Block periodization of strength and endurance training is superior to traditional periodization in ice hockey players. Scand. J. Med. Sci. Sports 2019, 29, 180–188. [Google Scholar] [CrossRef]
- Suchomel, T.J.; Nimphius, S.; Bellon, C.R.; Stone, M.H. The Importance of Muscular Strength: Training Considerations. Sports Med. 2018, 48, 765–785. [Google Scholar] [CrossRef]
- Taber, C.; Carroll, K.; DeWeese, B.; Sato, K.; Stuart, C.; Howell, M.; Hall, K.; Bazyler, C.; Stone, M. Neuromuscular Adaptations Following Training and Protein Supplementation in a Group of Trained Weightlifters. Sports 2018, 6, 37. [Google Scholar] [CrossRef]
- McGawley, K.; Juudas, E.; Kazior, Z.; Ström, K.; Blomstrand, E.; Hansson, O.; Holmberg, H.C. No Additional Benefits of Block- Over Evenly-Distributed High-Intensity Interval Training within a Polarized Microcycle. Front. Physiol. 2017, 8, 413. [Google Scholar] [CrossRef]
- Vissing, K.; McGee, S.; Farup, J.; Kjølhede, T.; Vendelbo, M.; Jessen, N. Differentiated mTOR but not AMPK signaling after strength vs endurance exercise in training-accustomed individuals. Scand. J. Med. Sci. Sports 2013, 23, 355–366. [Google Scholar] [CrossRef]
- Abt, J.P.; Oliver, J.M.; Nagai, T.; Sell, T.C.; Lovalekar, M.T.; Beals, K.; Wood, D.E.; Lephart, S.M. Block-Periodized Training Improves Physiological and Tactically Relevant Performance in Naval Special Warfare Operators. J. Strength Cond. Res. 2016, 30, 39–52. [Google Scholar] [CrossRef]
- Moesgaard, L.; Beck, M.M.; Christiansen, L.; Aagaard, P.; Lundbye-Jensen, J. Effects of Periodization on Strength and Muscle Hypertrophy in Volume-Equated Resistance Training Programs: A Systematic Review and Meta-analysis. Sports Med. 2022, 52, 1647–1666. [Google Scholar] [CrossRef]
- Vargas-Molina, S.; García-Sillero, M.; Romance, R.; Petro, J.L.; Jiménez-García, J.D.; Bonilla, D.A.; Kreider, R.B.; Benítez-Porres, J. Traditional and Undulating Periodization on Body Composition, Strength Levels and Physical Fitness in Older Adults. Int. J. Environ. Res. Public Health 2022, 19, 4522. [Google Scholar] [CrossRef] [PubMed]
- Soares, V.L.; Soares, W.F.; Zanetti, H.R.; Neves, F.F.; Silva-Vergara, M.L.; Mendes, E.L. Daily Undulating Periodization Is More Effective Than Nonperiodized Training on Maximal Strength, Aerobic Capacity, and TCD4+ Cell Count in People Living with HIV. J. Strength Cond. Res. 2022, 36, 1738–1748. [Google Scholar] [CrossRef] [PubMed]
- Szymanek-Pilarczyk, M.; Nowak, M.J.; Góra, T.; Oleksy, Ł.; Drozd, M.; Wąsik, J. The Evaluation of the Modified Wave Periodization Model Efficiency on the Example of Young Soccer Players’ Sprint Tests. J. Hum. Kinet. 2024, 94, 215–226. [Google Scholar] [CrossRef]
- Amaro-Gahete, F.J.; De-la-O, A.; Sanchez-Delgado, G.; Robles-Gonzalez, L.; Jurado-Fasoli, L.; Ruiz, J.R.; Gutiérrez, A. Functional Exercise Training and Undulating Periodization Enhances the Effect of Whole-Body Electromyostimulation Training on Running Performance. Front. Physiol. 2018, 9, 720. [Google Scholar] [CrossRef]
- Coelho-Júnior, H.J.; de Oliveira Gonçalvez, I.; Sampaio, R.A.C.; Sewo Sampaio, P.Y.; Cadore, E.L.; Izquierdo, M.; Marzetti, E.; Uchida, M.C. Periodized and non-periodized resistance training programs on body composition and physical function of older women. Exp. Gerontol. 2019, 121, 10–18. [Google Scholar] [CrossRef]
- Evans, J.W. Periodized Resistance Training for Enhancing Skeletal Muscle Hypertrophy and Strength: A Mini-Review. Front. Physiol. 2019, 10, 13. [Google Scholar] [CrossRef]
- Williams, T.D.; Tolusso, D.V.; Fedewa, M.V.; Esco, M.R. Comparison of Periodized and Non-Periodized Resistance Training on Maximal Strength: A Meta-Analysis. Sports Med. 2017, 47, 2083–2100. [Google Scholar] [CrossRef]
- Moraes, E.; Fleck, S.J.; Ricardo Dias, M.; Simão, R. Effects on strength, power, and flexibility in adolescents of nonperiodized vs. daily nonlinear periodized weight training. J. Strength Cond. Res. 2013, 27, 3310–3321. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Rosell, D.; Martínez-Cava, A.; Yáñez-García, J.M.; Hernández-Belmonte, A.; Mora-Custodio, R.; Morán-Navarro, R.; Pallarés, J.G.; González-Badillo, J.J. Linear programming produces greater, earlier and uninterrupted neuromuscular and functional adaptations than daily-undulating programming after velocity-based resistance training. Physiol. Behav. 2021, 233, 113337. [Google Scholar] [CrossRef]
- Turri-Silva, N.; Vale-Lira, A.; Verboven, K.; Quaglioti Durigan, J.L.; Hansen, D.; Cipriano, G., Jr. High-intensity interval training versus progressive high-intensity circuit resistance training on endothelial function and cardiorespiratory fitness in heart failure: A preliminary randomized controlled trial. PLoS ONE 2021, 16, e0257607. [Google Scholar] [CrossRef]
- Buch, A.; Kis, O.; Carmeli, E.; Keinan-Boker, L.; Berner, Y.; Barer, Y.; Shefer, G.; Marcus, Y.; Stern, N. Circuit resistance training is an effective means to enhance muscle strength in older and middle aged adults: A systematic review and meta-analysis. Ageing Res. Rev. 2017, 37, 16–27. [Google Scholar] [CrossRef] [PubMed]
- Ramos-Campo, D.J.; Andreu-Caravaca, L.; Carrasco-Poyatos, M.; Benito, P.J.; Rubio-Arias, J.Á. Effects of Circuit Resistance Training on Body Composition, Strength, and Cardiorespiratory Fitness in Middle-Aged and Older Women: A Systematic Review and Meta-Analysis. J. Aging Phys. Act. 2021, 30, 725–738. [Google Scholar] [CrossRef]
- Habani, R.; Nazari, M.; Dalili, S.; Rad, A.H. Effect of Circuit Resistance Training on Glycemic Control of Females with Diabetes Type II. Int. J. Prev. Med. 2015, 6, 34. [Google Scholar]
- Safarzade, A.; Alizadeh, H.; Bastani, Z. The effects of circuit resistance training on plasma progranulin level, insulin resistance and body composition in obese men. Horm. Mol. Biol. Clin. Investig. 2020, 41, 1–8. [Google Scholar] [CrossRef]
- Boidin, M.; David, L.P.; Trachsel, L.D.; Gayda, M.; Tremblay, J.; Lalongé, J.; Juneau, M.; Nigam, A.; Henri, C. Impact of 2 different aerobic periodization training protocols on left ventricular function in patients with stable coronary artery disease: An exploratory study. Appl. Physiol. Nutr. Metab. 2021, 46, 436–442. [Google Scholar] [CrossRef]
- Wu, C.; Bu, R.; Wang, Y.; Xu, C.; Chen, Y.; Che, L.; Wang, S. Rehabilitation effects of circuit resistance training in coronary heart disease patients: A systematic review and meta-analysis. Clin. Cardiol. 2022, 45, 821–830. [Google Scholar] [CrossRef] [PubMed]
- Debien, P.B.; Mancini, M.; Coimbra, D.R.; de Freitas, D.G.S.; Miranda, R.; Bara Filho, M.G. Monitoring Training Load, Recovery, and Performance of Brazilian Professional Volleyball Players During a Season. Int. J. Sports Physiol. Perform. 2018, 13, 1182–1189. [Google Scholar] [CrossRef]
- Debien, P.B.; Miloski, B.; Werneck, F.Z.; Timoteo, T.F.; Ferezin, C.; Filho, M.G.B.; Gabbett, T.J. Training Load and Recovery During a Pre-Olympic Season in Professional Rhythmic Gymnasts. J. Athl. Train. 2020, 55, 977–983. [Google Scholar] [CrossRef]
- Painter, K.B.; Haff, G.G.; Triplett, N.T.; Stuart, C.; Hornsby, G.; Ramsey, M.W.; Bazyler, C.D.; Stone, M.H. Resting Hormone Alterations and Injuries: Block vs. DUP Weight-Training among D-1 Track and Field Athletes. Sports 2018, 6, 3. [Google Scholar] [CrossRef]
- Roberson, K.B.; Chowdhari, S.S.; White, M.J.; Signorile, J.F. Loads and Movement Speeds Dictate Differences in Power Output During Circuit Training. J. Strength Cond. Res. 2017, 31, 2765–2776. [Google Scholar] [CrossRef]
- Kolahdouzi, S.; Baghadam, M.; Kani-Golzar, F.A.; Saeidi, A.; Jabbour, G.; Ayadi, A.; De Sousa, M.; Zouita, A.; Abderrahmane, A.B.; Zouhal, H. Progressive circuit resistance training improves inflammatory biomarkers and insulin resistance in obese men. Physiol. Behav. 2019, 205, 15–21. [Google Scholar] [CrossRef] [PubMed]
- Helms, E.R.; Fitschen, P.J.; Aragon, A.A.; Cronin, J.; Schoenfeld, B.J. Recommendations for natural bodybuilding contest preparation: Resistance and cardiovascular training. J. Sports Med. Phys. Fit. 2015, 55, 164–178. [Google Scholar]
- Gavanda, S.; Geisler, S.; Quittmann, O.J.; Schiffer, T. The Effect of Block Versus Daily Undulating Periodization on Strength and Performance in Adolescent Football Players. Int. J. Sports Physiol. Perform. 2019, 14, 814–821. [Google Scholar] [CrossRef] [PubMed]
- Painter, K.B.; Haff, G.G.; Ramsey, M.W.; McBride, J.; Triplett, T.; Sands, W.A.; Lamont, H.S.; Stone, M.E.; Stone, M.H. Strength gains: Block versus daily undulating periodization weight training among track and field athletes. Int. J. Sports Physiol. Perform. 2012, 7, 161–169. [Google Scholar] [CrossRef] [PubMed]
- Conlon, J.A.; Newton, R.U.; Tufano, J.J.; Banyard, H.G.; Hopper, A.J.; Ridge, A.J.; Haff, G.G. Periodization Strategies in Older Adults: Impact on Physical Function and Health. Med. Sci. Sports Exerc. 2016, 48, 2426–2436. [Google Scholar] [CrossRef]
- Conlon, J.A.; Haff, G.G.; Tufano, J.J.; Newton, R.U. Application of Session Rating of Perceived Exertion Among Different Models of Resistance Training in Older Adults. J. Strength Cond. Res. 2015, 29, 3439–3446. [Google Scholar] [CrossRef]
- Butcher, N.J.; Monsour, A.; Mew, E.J.; Chan, A.W.; Moher, D.; Mayo-Wilson, E.; Terwee, C.B.; Chee-A-Tow, A.; Baba, A.; Gavin, F.; et al. Guidelines for Reporting Outcomes in Trial Reports: The CONSORT-Outcomes 2022 Extension. JAMA 2022, 328, 2252–2264. [Google Scholar] [CrossRef]
- World Medical Association. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef]
- Fuentes-Barría, H.; Aguilera Eguia, R.; Polevoy, G. High intensity interval training based on parasympathetic activity and its impact on the cardiorespiratory capacity of university students. Randomized Controlled Trial. Retos 2024, 55, 513–519. [Google Scholar] [CrossRef]
- Fuentes-Barría, H.; Aguilera-Eguía, R.; Polevoy, G.G.; Maureira-Sánchez, J.; Angarita-Dávila, L. Effects of High-Intensity Interval Training on Aerobic Capacity and Heart Rate Variability in University Students: A Quasi-Experimental Study. J. Sport. Health Res. 2024, 16, 58–66. [Google Scholar]
- Fuentes-Barría, H.; Urbano-Cerda, S.; Aguilera-Eguía, R.; Vera-Aguirre, V.; González-Wong, C. Effects of 4 weeks of high intensity interval training on autonomic balance in adults confined by COVID-19. J. Sport. Health Res. 2022, 16, 58–66. [Google Scholar]
- Stellingwerff, T.; Morton, J.P.; Burke, L.M. A Framework for Periodized Nutrition for Athletics. Int. J. Sport Nutr. Exerc. Metab. 2019, 29, 141–151. [Google Scholar] [CrossRef]
- Gao, J.; Yu, L. Effects of concurrent training sequence on VO2max and lower limb strength performance: A systematic review and meta-analysis. Front. Physiol. 2023, 14, 1072679. [Google Scholar] [CrossRef] [PubMed]
- Thompson, W.R. Worldwide survey of fitness trends for 2021. ACSM’s Health Fit. J. 2021, 25, 10–19. [Google Scholar] [CrossRef]
- Yabe, H.; Kono, K.; Onoyama, A.; Kiyota, A.; Moriyama, Y.; Okada, K.; Kasuga, H. Predicting a target exercise heart rate that reflects the anaerobic threshold in nonbeta-blocked hemodialysis patients: The Karvonen and heart rate reserve formulas. Ther. Apher. Dial. 2021, 25, 884–889. [Google Scholar] [CrossRef]
- Tanaka, H.; Monahan, K.D.; Seals, D.R. Age-predicted maximal heart rate revisited. J. Am. Coll. Cardiol. 2001, 37, 153–156. [Google Scholar] [CrossRef]
- Nuuttila, O.P.; Korhonen, E.; Laukkanen, J.; Kyröläinen, H. Validity of the Wrist-Worn Polar Vantage V2 to Measure Heart Rate and Heart Rate Variability at Rest. Sensors 2021, 22, 137. [Google Scholar] [CrossRef]
- Schaffarczyk, M.; Rogers, B.; Reer, R.; Gronwald, T. Validity of the Polar H10 Sensor for Heart Rate Variability Analysis during Resting State and Incremental Exercise in Recreational Men and Women. Sensors 2022, 22, 6536. [Google Scholar] [CrossRef]
- Coates, A.M.; Joyner, M.J.; Little, J.P.; Jones, A.M.; Gibala, M.J. A Perspective on High-Intensity Interval Training for Performance and Health. Sports Med. 2023, 53, 85–96. [Google Scholar] [CrossRef]
- Balboa-Castillo, T.; Muñoz, S.; Serón, P.; Andrade-Mayorga, O.; Lavados-Romo, P.; Aguilar-Farias, N. Validity and reliability of the international physical activity questionnaire short form in Chilean adults. PLoS ONE 2023, 18, e0291604. [Google Scholar] [CrossRef]
- Meh, K.; Jurak, G.; Sorić, M.; Rocha, P.; Sember, V. Validity and Reliability of IPAQ-SF and GPAQ for Assessing Sedentary Behaviour in Adults in the European Un-ion: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 4602. [Google Scholar] [CrossRef] [PubMed]
- Lee, P.H.; Macfarlane, D.J.; Lam, T.H.; Stewart, S.M. Validity of the International Physical Activity Questionnaire Short Form (IPAQ-SF): A systematic review. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 115. [Google Scholar] [CrossRef] [PubMed]
- Sember, V.; Meh, K.; Sorić, M.; Starc, G.; Rocha, P.; Jurak, G. Validity and Reliability of International Physical Activity Questionnaires for Adults across EU Countries: Sys-tematic Review and Meta Analysis. Int. J. Environ. Res. Public Health 2020, 17, 7161. [Google Scholar] [CrossRef] [PubMed]
- Giro, R.; Matias, C.N.; Campa, F.; Santos, D.A.; Cavaca, M.L.; Duque, P.; Oliveira, M.; Matos, N.; Vicente, F.; Pereira, P.; et al. Development and Validation of an Anthropometric Equation to Predict Fat Mass Percentage in Professional and Semi-Professional Male Futsal Players. Nutrients 2022, 14, 4514. [Google Scholar] [CrossRef]
- Silva, V.S.; Vieira, F. International Society for the Advancement of Kinanthropometry (ISAK) Global: International accreditation scheme of the competent anthropometrist. Rev. Bras. Cineantropom Desempenho Hum. 2020, 22, e70517. [Google Scholar] [CrossRef]
- Pacheco, L.S.; Blanco, E.; Burrows, R.; Correa-Burrows, P.; Santos, J.L.; Gahagan, S. Eating behavior and body composition in Chilean young adults. Appetite 2021, 156, 104857. [Google Scholar] [CrossRef]
- Labraña, A.M.; Durán, E.; Martínez, M.A.; Leiva, A.M.; Garrido-Méndez, A.; Díaz, X.; Salas, C.; Celis-Morales, C. Effects of a lower body weight or waist circumference on cardiovascular risk. Findings from the Chilean health survey. Rev. Méd. Chil. 2017, 145, 585–594. [Google Scholar]
- Romero-Dapueto, C.; Mahn, J.; Cavada, G.; Daza, R.; Ulloa, V.; Antúnez, M. Hand grip strength values in normal Chilean subjects. Rev. Med. Chil. 2019, 147, 741–750. [Google Scholar] [CrossRef]
- Lupton-Smith, A.; Fourie, K.; Mazinyo, A.; Mokone, M.; Nxaba, S.; Morrow, B. Measurement of hand grip strength: A cross-sectional study of two dynamometry devices. S. Afr. J. Physiother. 2022, 78, 1768. [Google Scholar] [CrossRef]
- Huang, L.; Liu, Y.; Lin, T.; Hou, L.; Song, Q.; Ge, N.; Yue, J. Reliability and validity of two hand dynamometers when used by community-dwelling adults aged over 50 years. BMC Geriatr. 2022, 22, 580. [Google Scholar] [CrossRef]
- Jiménez-Sánchez, A.; Pereira-Cunill, J.L.; Limón-Mirón, M.L.; López-Ladrón, A.; Salvador-Bofill, F.J.; García-Luna, P.P. A Cross-Sectional Validation Study of Camry EH101 versus JAMAR Plus Handheld Dynamometers in Colorectal Cancer Patients and Their Correlations with Bioelectrical Impedance and Nutritional Status. Nutrients 2024, 16, 1824. [Google Scholar] [CrossRef] [PubMed]
- Zagatto, A.M.; Beck, W.R.; Gobatto, C.A. Validity of the running anaerobic sprint test for assessing anaerobic power and predicting short-distance performances. J. Strength Cond. Res. 2009, 23, 1820–1827. [Google Scholar] [CrossRef]
- Osses, A.R.; Yáñez, V.J.; Barría, P.P.; Palacios, M.S.; Dreyse, D.J.; Díaz, P.O.; Lisboa, B.C. Reference values for the 6-minutes walking test in healthy subjects 20–80 years old. Rev. Med. Chil. 2010, 138, 1124–1130. [Google Scholar]
- Chiang, J.K.; Lin, Y.C.; Hung, T.Y.; Kao, H.H.; Kao, Y.H. The Impact on Autonomic Nervous System Activity during and Following Exercise in Adults: A Meta-Regression Study and Trial Sequential Analysis. Medicina 2024, 60, 1223. [Google Scholar] [CrossRef]
- Vondrasek, J.D.; Riemann, B.L.; Grosicki, G.J.; Flatt, A.A. Validity and Efficacy of the Elite HRV Smartphone Application during Slow-Paced Breathing. Sensors 2023, 23, 9496. [Google Scholar] [CrossRef]
- Rogers, B.; Schaffarczyk, M.; Gronwald, T. Estimation of Respiratory Frequency in Women and Men by Kubios HRV Software Using the Polar H10 or Movesense Medical ECG Sensor during an Exercise Ramp. Sensors 2022, 22, 7156. [Google Scholar] [CrossRef] [PubMed]
- Shaffer, F.; Ginsberg, J.P. An Overview of Heart Rate Variability Metrics and Norms. Front. Public Health 2017, 5, 258. [Google Scholar]
- Ernst, G. Hidden Signals—The History and Methods of Heart Rate Variability. Front. Public Health 2017, 5, 265. [Google Scholar] [CrossRef]
- Yang, F.; Ma, Y.; Liang, S.; Shi, Y.; Wang, C. Effect of Exercise Modality on Heart Rate Variability in Adults: A Systematic Review and Network Meta-Analysis. Rev. Cardiovasc. Med. 2024, 25, 9. [Google Scholar] [CrossRef]
- Serdar, C.C.; Cihan, M.; Yücel, D.; Serdar, M.A. Sample size, power and effect size revisited: Simplified and practical approaches in pre-clinical, clinical and laboratory studies. Biochem. Med. 2021, 31, 010502. [Google Scholar] [CrossRef]
- Shieh, G. Effect size, statistical power, and sample size for assessing interactions between categorical and continuous variables. Br. J. Math. Stat. Psychol. 2019, 72, 136–154. [Google Scholar] [CrossRef] [PubMed]
- Ross, R.; Neeland, I.J.; Yamashita, S.; Shai, I.; Seidell, J.; Magni, P.; Santos, R.D.; Arsenault, B.; Cuevas, A.; Hu, F.B.; et al. Waist circumference as a vital sign in clinical practice: A Consensus Statement from the IAS and ICCR Working Group on Visceral Obesity. Nat. Rev. Endocrinol. 2020, 16, 177–189. [Google Scholar] [CrossRef] [PubMed]
- Mezghani, N.; Ammar, A.; Boukhris, O.; Abid, R.; Hadadi, A.; Alzahrani, T.M.; Trabelsi, O.; Boujelbane, M.A.; Masmoudi, L.; Ouergui, I.; et al. The Impact of Exercise Training Intensity on Physiological Adaptations and Insulin Resistance in Women with Abdominal Obesity. Healthcare 2022, 10, 2533. [Google Scholar] [CrossRef]
- Moon, J.; Oh, M.; Kim, S.; Lee, K.; Lee, J.; Song, Y.; Jeon, J.Y. Intelligent Estimation of Exercise Induced Energy Expenditure Including Excess Post-Exercise Oxygen Consumption (EPOC) with Different Exercise Intensity. Sensors 2023, 23, 9235. [Google Scholar] [CrossRef]
- Higashida, K.; Takeuchi, N.; Inoue, S.; Hashimoto, T.; Nakai, N. Iron deficiency attenuates catecholamine-stimulated lipolysis via downregulation of lipolysis-related proteins and glucose utilization in 3T3-L1 adipocytes. Mol. Med. Rep. 2020, 21, 1383–1389. [Google Scholar] [CrossRef]
- Hwaung, P.; Heo, M.; Kennedy, S.; Hong, S.; Thomas, D.M.; Shepherd, J.; Heymsfield, S.B. Optimum waist circumference-height indices for evaluating adult adiposity: An analytic review. Obes. Rev. 2020, 21, e12947. [Google Scholar] [CrossRef] [PubMed]
- Heymsfield, S.B.; Peterson, C.M.; Thomas, D.M.; Heo, M.; Schuna, J.M., Jr. Why are there race/ethnic differences in adult body mass index-adiposity relationships? A quantitative critical review. Obes. Rev. 2016, 17, 262–275. [Google Scholar] [CrossRef]
- Kapsis, D.P.; Tsoukos, A.; Psarraki, M.P.; Douda, H.T.; Smilios, I.; Bogdanis, G.C. Changes in Body Composition and Strength after 12 Weeks of High-Intensity Functional Training with Two Different Loads in Physically Active Men and Women: A Randomized Controlled Study. Sports 2022, 10, 7. [Google Scholar] [CrossRef]
- Jacko, D.; Schaaf, K.; Masur, L.; Windoffer, H.; Aussieker, T.; Schiffer, T.; Zacher, J.; Bloch, W.; Gehlert, S. Repeated and Interrupted Resistance Exercise Induces the Desensitization and Re-Sensitization of mTOR-Related Signaling in Human Skeletal Muscle Fibers. Int. J. Mol. Sci. 2022, 23, 5431. [Google Scholar] [CrossRef]
- Pérez-Castilla, A.; García-Ramos, A.; Redondo, B.; Andrés, F.R.; Jiménez, R.; Vera, J. Determinant Factors of Intraocular Pressure Responses to a Maximal Isometric Handgrip Test: Hand Dominance, Handgrip Strength and Sex. Curr. Eye Res. 2021, 46, 64–70. [Google Scholar] [CrossRef]
- Martin, J.A.; Ramsay, J.; Hughes, C.; Peters, D.M.; Edwards, M.G. Age and grip strength predict hand dexterity in adults. PLoS ONE 2015, 10, e0117598. [Google Scholar] [CrossRef] [PubMed]
- Oka, N.; Sakoh, M.; Hirayama, M.; Niiyama, M.; Gjedde, A. Relationship between manual dexterity and left-right asymmetry of anatomical and functional properties of corticofugal tracts revealed by T2-weighted brain images. Sci. Rep. 2023, 13, 2738. [Google Scholar] [CrossRef] [PubMed]
- Bellosta-López, P.; Blasco-Abadía, J.; Andersen, L.L.; Vinstrup, J.; Skovlund, S.V.; Doménech-García, V. Multimodal sensorimotor assessment of hand and forearm asymmetries: A reliability and correlational study. PeerJ 2024, 12, e17403. [Google Scholar] [CrossRef]
- Ishida, A.; Travis, S.K.; Stone, M.H. Short-Term Periodized Programming May Improve Strength, Power, Jump Kinetics, and Sprint Efficiency in Soccer. J. Funct. Morphol. Kinesiol. 2021, 6, 45. [Google Scholar] [CrossRef] [PubMed]
- Harries, S.K.; Lubans, D.R.; Buxton, A.; MacDougall, T.H.J.; Callister, R. Effects of 12-Week Resistance Training on Sprint and Jump Performances in Competitive Adolescent Rugby Union Players. J. Strength Cond. Res. 2018, 32, 2762–2769. [Google Scholar] [CrossRef]
- Riscart-López, J.; Sánchez-Valdepeñas, J.; Mora-Vela, R.; Caro-Ávalos, J.; Sánchez-González, L.; Sánchez-Moreno, M.; León-Prados, J.A.; Pareja-Blanco, F. Effects of 4 Different Velocity-Based Resistance-Training Programming Models on Physical Performance. Int. J. Sports Physiol. Perform. 2024, 19, 271–279. [Google Scholar] [CrossRef]
- Valamatos, M.J.; Abrantes, J.M.; Carnide, F.; Valamatos, M.J.; Monteiro, C.P. Biomechanical Performance Factors in the Track and Field Sprint Start: A Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 4074. [Google Scholar] [CrossRef]
- Batra, A.; Wetmore, A.B.; Hornsby, W.G.; Lipinska, P.; Staniak, Z.; Surala, O.; Stone, M.H. Strength, Endocrine, and Body Composition Alterations across Four Blocks of Training in an Elite 400 m Sprinter. J. Funct. Morphol. Kinesiol. 2021, 6, 25. [Google Scholar] [CrossRef]
- Mangine, G.T.; Huet, K.; Williamson, C.; Bechke, E.; Serafini, P.; Bender, D.; Hudy, J.; Townsend, J. A Resisted Sprint Improves Rate of Force Development During a 20-m Sprint in Athletes. J. Strength Cond. Res. 2018, 32, 1531–1537. [Google Scholar] [CrossRef]
- Bouguetoch, A.; Martin, A.; Grosprêtre, S. Insights into the combination of neuromuscular electrical stimulation and motor imagery in a training-based approach. Eur. J. Appl. Physiol. 2021, 121, 941–955. [Google Scholar] [CrossRef]
- Borzuola, R.; Nuccio, S.; Scalia, M.; Parrella, M.; Del Vecchio, A.; Bazzucchi, I.; Felici, F.; Macaluso, A. Adjustments in the motor unit discharge behavior following neuromuscular electrical stimulation compared to voluntary contractions. Front. Physiol. 2023, 14, 1212453. [Google Scholar] [CrossRef] [PubMed]
- Santinelli, F.B.; Abasıyanık, Z.; Ramari, C.; Gysemberg, G.; Kos, D.; Pau, M.; Kalron, A.; Meyns, P.; Ozakbas, S.; Feys, P. Manifestations of walking fatigability in people with multiple sclerosis based on gait quality and distance walked during the six minutes walking test. Mult. Scler. Relat. Disord. 2024, 91, 105909. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Guo, C.; Liu, S.; Zhang, S.; Mao, Y.; Fang, L. Eight Weeks of High-Intensity Interval Static Strength Training Improves Skeletal Muscle Atrophy and Motor Function in Aged Rats via the PGC-1α/FNDC5/UCP1 Pathway. Clin. Interv. Aging 2021, 16, 811–821. [Google Scholar] [CrossRef]
- Helgerud, J.; Hov, H.; Mehus, H.; Balto, B.; Boye, A.; Finsås, L.; Hoff, J.; Wang, E. Aerobic high-intensity intervals improve VO2max more than supramaximal sprint intervals in females, similar to males. Scand. J. Med. Sci. Sports 2023, 33, 2193–2207. [Google Scholar] [CrossRef] [PubMed]
- Atakan, M.M.; Li, Y.; Koşar, Ş.N.; Turnagöl, H.H.; Yan, X. Evidence-Based Effects of High-Intensity Interval Training on Exercise Capacity and Health: A Review with Historical Perspective. Int. J. Environ. Res. Public Health 2021, 18, 7201. [Google Scholar] [CrossRef]
- Rønnestad, B.R.; Rømer, T.; Hansen, J. Increasing Oxygen Uptake in Well-Trained Cross-Country Skiers During Work Intervals With a Fast Start. Int. J. Sports Physiol. Perform. 2020, 15, 383–389. [Google Scholar] [CrossRef]
- Romero-Arenas, S.; Martínez-Pascual, M.; Alcaraz, P.E. Impact of resistance circuit training on neuromuscular, cardiorespiratory and body composition adaptations in the elderly. Aging Dis. 2013, 4, 256–263. [Google Scholar] [CrossRef]
- Zhang, Q.; Lu, H.; Pan, S.; Lin, Y.; Zhou, K.; Wang, L. 6MWT Performance and its Correlations with VO2 and Handgrip Strength in Home-Dwelling Mid-Aged and Older Chinese. Int. J. Environ. Res. Public Health 2017, 14, 473. [Google Scholar] [CrossRef]
- Llanos-Lagos, C.; Ramirez-Campillo, R.; Moran, J.; Sáez de Villarreal, E. Effect of Strength Training Programs in Middle- and Long-Distance Runners’ Economy at Different Running Speeds: A Systematic Review with Meta-analysis. Sports Med. 2024, 54, 895–932. [Google Scholar] [CrossRef]
- Llanos-Lagos, C.; Ramirez-Campillo, R.; Moran, J.; Sáez de Villarreal, E. The Effect of Strength Training Methods on Middle-Distance and Long-Distance Runners’ Athletic Performance: A Systematic Review with Meta-analysis. Sports Med. 2024, 54, 1801–1833. [Google Scholar] [CrossRef]
- Davies, T.B.; Tran, D.L.; Hogan, C.M.; Haff, G.G.; Latella, C. Chronic Effects of Altering Resistance Training Set Configurations Using Cluster Sets: A Systematic Review and Meta-Analysis. Sports Med. 2021, 51, 707–736. [Google Scholar] [CrossRef] [PubMed]
- Bhati, P.; Moiz, J.A.; Menon, G.R.; Hussain, M.E. Does resistance training modulate cardiac autonomic control? A systematic review and meta-analysis. Clin. Auton. Res. 2019, 29, 75–103. [Google Scholar] [CrossRef] [PubMed]
- Farah, B.Q.; Christofaro, D.G.D.; Correia, M.A.; Oliveira, C.B.; Parmenter, B.J.; Ritti-Dias, R.M. Effects of isometric handgrip training on cardiac autonomic profile: A systematic review and meta-analysis study. Clin. Physiol. Funct. Imaging 2020, 40, 141–147. [Google Scholar] [CrossRef] [PubMed]
- Storniolo, J.L.; Esposti, R.; Cavallari, P. Heart Rate Kinetics and Sympatho-Vagal Balance Accompanying a Maximal Sprint Test. Front. Psychol. 2020, 10, 2950. [Google Scholar] [CrossRef]
- El-Malahi, O.; Mohajeri, D.; Mincu, R.; Bäuerle, A.; Rothenaicher, K.; Knuschke, R.; Rammos, C.; Rassaf, T.; Lortz, J. Beneficial impacts of physical activity on heart rate variability: A systematic review and meta-analysis. PLoS ONE 2024, 19, e0299793. [Google Scholar] [CrossRef]
- Medina Corrales, M.; Garrido Esquivel, A.; Flores Cruz, M.; Miranda Mendoza, F.J.; García Dávila, M.Z.; Hernández Cruz, G.; Naranjo Orellana, J. Utility of the RMSSD-Slope for internal training load quantification in elite badminton players. Case study. Retos 2021, 40, 60–66. [Google Scholar]
- Vreijling, S.R.; Troudart, Y.; Brosschot, J.F. Reduced Heart Rate Variability in Patients With Medically Unexplained Physical Symptoms: A Meta-Analysis of HF-HRV and RMSSD. Psychosom. Med. 2021, 83, 2–15. [Google Scholar] [CrossRef]
- Ramírez-Vélez, R.; Tordecilla-Sanders, A.; Téllez-T, L.A.; Camelo-Prieto, D.; Hernández-Quiñonez, P.A.; Correa-Bautista, J.E.; Garcia-Hermoso, A.; Ramírez-Campillo, R.; Izquierdo, M. Effect of Moderate- Versus High-Intensity Interval Exercise Training on Heart Rate Variability Parameters in Inactive Latin-American Adults: A Randomized Clinical Trial. J. Strength Cond. Res. 2020, 34, 3403–3415. [Google Scholar] [CrossRef]
- Amekran, Y.; El Hangouche, A.J. Effects of Exercise Training on Heart Rate Variability in Healthy Adults: A Systematic Review and Meta-analysis of Randomized Controlled Trials. Cureus 2024, 16, e62465. [Google Scholar] [CrossRef]
- Mustafa, G.; Kursat, F.M.; Ahmet, T.; Alparslan, G.F.; Omer, G.; Sertoglu, E.; Erkan, S.; Ediz, Y.; Turker, T.; Ayhan, K. The relationship between erythrocyte membrane fatty acid levels and cardiac autonomic function in obese children. Rev. Port. Cardiol. 2017, 36, 499–508. [Google Scholar] [CrossRef]
- Guo, Z.; Li, M.; Cai, J.; Gong, W.; Liu, Y.; Liu, Z. Effect of High-Intensity Interval Training vs. Moderate-Intensity Continuous Training on Fat Loss and Cardiorespiratory Fitness in the Young and Middle-Aged a Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2023, 20, 4741. [Google Scholar]
- Espinoza-Salinas, A.; González-Jurado, J.; Molina-Sotomayor, E.; Fuentes-Barría, H.; Farías-Valenzuela, C.; Arenas-Sánchez, G. Mobilization, transport and oxidation of fatty acids: Physiological mechanisms associated with weight loss. J. Sport. Health Res. 2020, 12, 303–312. [Google Scholar]

{kind=link}
| Phase | Duration | Type of Exercise |
|---|---|---|
| Warm-up | 5 min | Whole-body stretching. (flexion, extension, abduction, and adduction of the shoulders, hips, knees, and ankles). |
| Experimental group | 38–47 min | Interval block resistance training in the whole body (Push-up, Mountain climber, Squat, Jumping Jack, Burpees, and Skipping). |
| Control group | 38–47 min | Circuit resistance training in the whole body (Push-up, Mountain climber, Squat, Jumping Jack, Burpees, and Skipping). |
| Cool-down | 5 min | Whole-body stretching (flexion, extension, abduction, and adduction of the shoulders, hips, knees, and ankles). |
| Weeks | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | |
| Maximum heart rate (%) | 75 | 75 | 75 | 80 | 80 | 80 | 85 | 85 | 85 | 90 | 90 | 90 |
| Set (number) | 6 | 6 | 6 | 6 | 6 | 6 | 6 | 6 | 6 | 6 | 6 | 6 |
| Repetitions (number) | 6 | 6 | 6 | 6 | 6 | 6 | 6 | 6 | 6 | 6 | 6 | 6 |
| Time for repetition (s) | 30 | 30 | 30 | 35 | 35 | 35 | 40 | 40 | 40 | 45 | 45 | 45 |
| Total time of working (min) | 18 | 18 | 18 | 21 | 21 | 21 | 24 | 24 | 24 | 27 | 27 | 27 |
| Rest between repetitions (s) | 30 | 30 | 30 | 30 | 30 | 30 | 30 | 30 | 30 | 30 | 30 | 30 |
| Total rest between repetitions (min) | 15 | 15 | 15 | 15 | 15 | 15 | 15 | 15 | 15 | 15 | 15 | 15 |
| Rest between set (min) | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| Total rest between set (min) | 5 | 5 | 5 | 5 | 5 | 5 | 5 | 5 | 5 | 5 | 5 | 5 |
| Total time (min) | 38 | 38 | 38 | 41 | 41 | 41 | 44 | 44 | 44 | 47 | 47 | 47 |
| Indicators | Experimental Group (X ± SD) | Control Group (X ± SD) | Variation (%) | p-Value | Effect Size (d) |
|---|---|---|---|---|---|
| Age (years) | 25.2 ± 3.19 | 23.27 ± 3.69 | 8.29 | 0.14 | 0.56 |
| Metabolic Equivalent of Task | 2206.13 ± 397.91 | 2551.07 ± 386.48 | 15.63 | 0.08 | 0.88 |
| Weight (kg) | 63.47 ± 5.90 | 63.36 ± 5.54 | 0.17 | 0.96 | 0.02 |
| Height (cm) | 171.38 ± 5.43 | 168.37 ± 5.58 | 1.79 | 0.19 | 0.55 |
| Body mass index (kg/m2) | 21.56 ± 2.22 | 22.36 ± 1.70 | 3.72 | 0.30 | 0.40 |
| Waist circumference (cm) | 81.97 ± 5.07 | 79.25 ± 5.66 | 3.43 | 0.16 | 0.51 |
| Left-hand grip (kg) | 55.15 ± 4.52 | 56.83 ± 3.98 | 3.05 | 0.18 | 0.39 |
| Right-hand grip (kg) | 55.59 ± 2.91 | 58.04 ± 4.20 | 4.45 | 0.07 | 0.68 |
| Running anaerobic sprint test (s) | 4.87 ± 0.07 | 4.81 ± 0,10 | 1.23 | 0.09 | 0.67 |
| Six min walking test (m) | 697.77 ± 50.11 | 683.01 ± 25.78 | 2.17 | 0.25 | 0.37 |
| LF/HF ratio | 1.40 ± 0.18 | 1.37 ± 0.17 | 2.14 | 0.59 | 0.17 |
| RMSSD (m/s) | 49.47 ± 5.95 | 50.41 ± 2.90 | 1.90 | 0.52 | 0.20 |
| Indicators | Before (X ± SD) | After (X ± SD) | Variation (%) | p-Value | Effect Size (d) |
|---|---|---|---|---|---|
| Metabolic Equivalent of Task | 2206.13 ± 397.91 | 2222.87 ± 429.26 | 0.76 | 0.41 | 0.04 |
| Weight (kg) | 63.47 ± 5.90 | 63.45 ± 5.76 | 0.03 | 0.98 | 0.003 |
| Height (cm) | 171.38 ± 5.43 | 171.38 ± 5.43 | N/A | N/A | N/A |
| Body mass index (kg/m2) | 21.56 ± 2.22 | 21.64 ± 1.97 | 0.37 | 0.71 | 0.04 |
| Waist circumference (cm) | 81.97 ± 5.07 | 80.45 ± 4.81 | 1.85 | ≤0.01 | 0.31 |
| Left-hand grip (kg) | 55.15 ± 4.52 | 56.0 ± 5.74 | 1.54 | 0.40 | 0.16 |
| Right-hand grip (kg) | 55.59 ± 2.91 | 58.63 ± 2.96 | 5.47 | ≤0.01 | 1.03 |
| Running anaerobic sprint test (s) | 4.87 ± 0.07 | 4.74 ± 0.12 | 2.67 | ≤0.01 | 1.30 |
| Six min walking test (m) | 697.77 ± 50.11 | 729.34 ± 46.85 | 4.53 | ≤0.01 | 0.65 |
| LF/HF ratio | 1.40 ± 0.18 | 1.24 ± 0.16 | 11.43 | ≤0.01 | 0.94 |
| RMSSD (m/s) | 49.47 ± 5.95 | 52.12 ± 5.71 | 5.36 | ≤0.01 | 0.45 |
| Indicators | Before (X ± SD) | After (X ± SD) | Variation (%) | p-Value | Effect Size (d) |
|---|---|---|---|---|---|
| Metabolic Equivalent of Task | 2551.07 ± 386.48 | 2566.33 ± 407.83 | 0.60 | 0.48 | 0.04 |
| Weight (kg) | 63.36 ± 5.54 | 63.65 ± 6.43 | 0.46 | 0.61 | 0.05 |
| Height (cm) | 168.37 ± 5.58 | 168.37 ± 5.58 | N/A | N/A | N/A |
| Body mass index (kg/m2) | 22.36 ± 1.70 | 22.46 ± 2.03 | 0.45 | 0.61 | 0.05 |
| Waist circumference (cm) | 79.25 ± 5.66 | 77.37 ± 5.51 | 2.37 | ≤0.01 | 0.34 |
| Left-hand grip (kg) | 56.83 ± 3.98 | 57.11 ± 3.87 | 0.49 | 0.32 | 0.07 |
| Right-hand grip (kg) | 58.04 ± 4.20 | 60.37 ± 4.22 | 4.02 | ≤0.01 | 0.55 |
| Running anaerobic sprint test (s) | 4.81 ± 0,10 | 4.76 ± 0.11 | 1.04 | ≤0.01 | 0.50 |
| Six min walking test (m) | 683.01 ± 25.78 | 697.80 ± 32.82 | 2.17 | ≤0.01 | 0.50 |
| LF/HF ratio | 1.37 ± 0.17 | 1.30 ± 0.17 | 5.11 | ≤0.01 | 0.41 |
| RMSSD (m/s) | 50.41 ± 2.90 | 52.33 ± 3.04 | 3.81 | ≤0.01 | 0.65 |
| Indicators | Experimental Group (X ± SD) | Control Group (X ± SD) | Variation (%) | p-Value | Effect Size (d) |
|---|---|---|---|---|---|
| Metabolic Equivalent of Task | 2222.87 ± 429.26 | 2566.33 ± 407.83 | 15.4 | 0.11 | 0.82 |
| Weight (kg) | 63.45 ± 5.76 | 63.65 ± 6.43 | 0.31 | 0.93 | 0.03 |
| Height (cm) | 171.38 ± 5.43 | 168.37 ± 5.58 | 1.79 | 0.19 | 0.55 |
| Body mass index (kg/m2) | 21.64 ± 1.97 | 22.46 ± 2.03 | 3.79 | 0.32 | 0.41 |
| Waist circumference (cm) | 80.45 ± 4.81 | 77.37 ± 5.51 | 3.95 | 0.10 | 0.60 |
| Left-hand grip (kg) | 56.0 ± 5.74 | 57.11 ± 3.87 | 1.98 | 0.51 | 0.23 |
| Right-hand grip (kg) | 58.63 ± 2.96 | 60.37 ± 4.22 | 2.97 | 0.15 | 0.48 |
| Running anaerobic sprint test (s) | 4.74 ± 0.12 | 4.76 ± 0.11 | 0.42 | 0.68 | 0.18 |
| Six min walking test (m) | 729.34 ± 46.85 | 697.80 ± 32.82 | 4.53 | 0.04 | 0.78 |
| LF/HF ratio | 1.24 ± 0.16 | 1.30 ± 0.17 | 4.84 | 0.37 | 0.36 |
| RMSSD (m/s) | 52.12 ± 5.71 | 52.33 ± 3.04 | 0.40 | 0.89 | 0.05 |
| Variable | Unstandardized Coefficient (B) | Standard Error | 95% CI | p-Value |
|---|---|---|---|---|
| Intercept | 141.11 | 79.75 | −22.51 to 304.73 | 0.09 |
| Predictive effects of pre-test on post-test | 0.81 | 0.12 | 0.58 to 1.05 | <0.001 |
| Adjusted difference between groups (IBRT vs. CRT) | 19.51 | 9.13 | 0.79 to 38.23 | 0.04 |
| R2 | 0.69 | |||
| Adjusted R2 | 0.67 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fuentes-Barría, H.; Aguilera-Eguía, R.; Maureira-Sánchez, J.; Alarcón-Rivera, M.; Garrido-Osorio, V.; López-Soto, O.P.; Aristizábal-Hoyos, J.A.; Angarita-Davila, L.; Rojas-Gómez, D.; Bermudez, V.; et al. Effects of 12 Weeks of Interval Block Resistance Training Versus Circuit Resistance Training on Body Composition, Performance, and Autonomic Recovery in Adults: Randomized Controlled Trial. J. Funct. Morphol. Kinesiol. 2025, 10, 195. https://doi.org/10.3390/jfmk10020195
Fuentes-Barría H, Aguilera-Eguía R, Maureira-Sánchez J, Alarcón-Rivera M, Garrido-Osorio V, López-Soto OP, Aristizábal-Hoyos JA, Angarita-Davila L, Rojas-Gómez D, Bermudez V, et al. Effects of 12 Weeks of Interval Block Resistance Training Versus Circuit Resistance Training on Body Composition, Performance, and Autonomic Recovery in Adults: Randomized Controlled Trial. Journal of Functional Morphology and Kinesiology. 2025; 10(2):195. https://doi.org/10.3390/jfmk10020195
Chicago/Turabian StyleFuentes-Barría, Héctor, Raúl Aguilera-Eguía, Juan Maureira-Sánchez, Miguel Alarcón-Rivera, Victor Garrido-Osorio, Olga Patrica López-Soto, Juan Alberto Aristizábal-Hoyos, Lissé Angarita-Davila, Diana Rojas-Gómez, Valmore Bermudez, and et al. 2025. "Effects of 12 Weeks of Interval Block Resistance Training Versus Circuit Resistance Training on Body Composition, Performance, and Autonomic Recovery in Adults: Randomized Controlled Trial" Journal of Functional Morphology and Kinesiology 10, no. 2: 195. https://doi.org/10.3390/jfmk10020195
APA StyleFuentes-Barría, H., Aguilera-Eguía, R., Maureira-Sánchez, J., Alarcón-Rivera, M., Garrido-Osorio, V., López-Soto, O. P., Aristizábal-Hoyos, J. A., Angarita-Davila, L., Rojas-Gómez, D., Bermudez, V., Flores-Fernández, C., Roco-Videla, Á., González-Casanova, J. E., Urbano-Cerda, S., & Iulian Alexe, D. (2025). Effects of 12 Weeks of Interval Block Resistance Training Versus Circuit Resistance Training on Body Composition, Performance, and Autonomic Recovery in Adults: Randomized Controlled Trial. Journal of Functional Morphology and Kinesiology, 10(2), 195. https://doi.org/10.3390/jfmk10020195