
Sexual Compulsivity and Gender Stereotypes in Men Who Have Sex with Men: A Cross-Sectional Study in Spain


Abstract
1. Introduction
2. Materials and Methods
2.1. Sociodemographic Variables, Behavioral Characteristics, and Unsafe Sexual Practices
2.2. Sexual Compulsivity Scale
2.3. Gender Stereotype Self-Identification: The Bem Sex Role Inventory
3. Statistical Analysis
Ethical Considerations
4. Results
4.1. Participants
4.2. Behavioral Characteristics, Unsafe Sexual Practices, and SCS
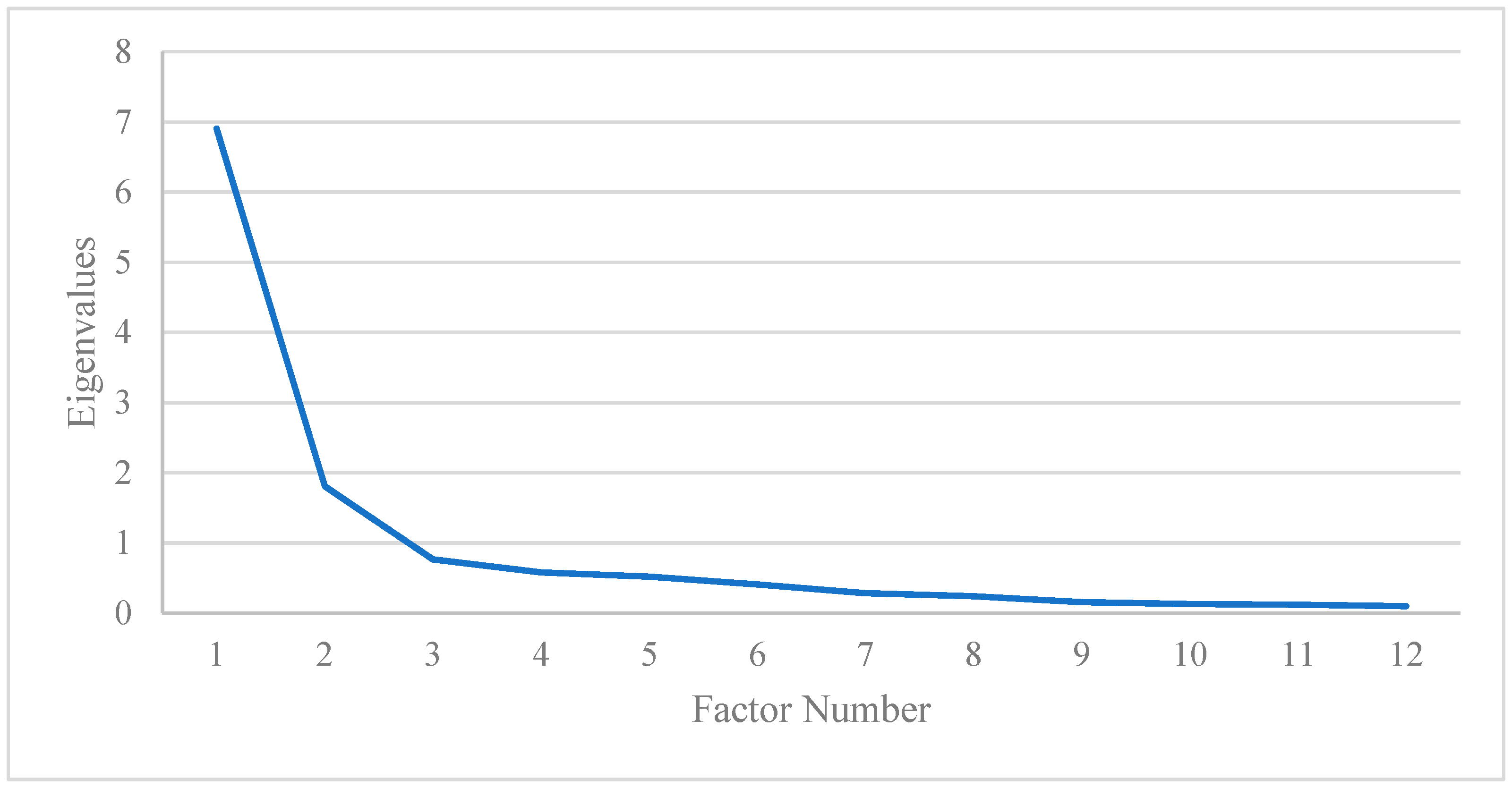
4.3. Psychometric Properties of BSRI-12
4.4. Gender Stereotypes and Sexual Compulsivity
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Glick, S.N.; Morris, M.; Foxman, B.; Aral, S.O.; Manhart, L.E.; Holmes, K.K.; Golden, M.R. Sex with Men and Heterosexual Men and Women. J. Acquir. Immune Defic. Syndr. 2013, 60, 83–90. [Google Scholar]
- McKirnan, D.J.; Du Bois, S.N.; Alvy, L.M.; Jones, K. Health Care Access and Health Behaviors Among Men Who Have Sex With Men: The Cost of Health Disparities. Health Educ. Behav. 2013, 40, 32–41. [Google Scholar] [CrossRef] [PubMed]
- Zhang Kudon, H.; Mulatu, M.S.; Song, W.; Heitgerd, J.; Rao, S. Trends in Condomless Sex among MSM Who Participated in CDC-Funded HIV Risk-Reduction Interventions in the United States, 2012–2017. J. Public Health Manag. Pract. 2022, 28, 170–173. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Hepatitis A Outbreaks Mostly Affecting Men Who Have Sex with Men—European Region and the Americas. 2017. Available online: https://www.who.int/news/item/07-06-2017-hepatitis-a-outbreaks-mostly-affecting-men-who-have-sex-with-men-european-region-and-the-americas (accessed on 23 May 2024).
- European Center for Disease Prevention and Control. Epidemiological Update: Hepatitis A Outbreak in the EU/EEA Mostly Affecting Men Who Have Sex with Men. 2018. Available online: https://www.ecdc.europa.eu/en/news-events/epidemiological-update-hepatitis-outbreak-eueea-mostly-affecting-men-who-have-sex-men-1 (accessed on 23 May 2024).
- World Health Organization. 2022–2024 Mpox (Momkeypox) Outbreak: Global Trends. 2022. Available online: https://worldhealthorg.shinyapps.io/mpx_global/ (accessed on 23 May 2024).
- European Centre for Disease Prevention and Control. Monkeypox Multi-Country Outbreak, First Update–8 July 2022. ECDC: Stockholm. 2022. Available online: https://www.ecdc.europa.eu/sites/default/files/documents/Monkeypox-multi-country-outbreak-first-update-8-July-FINAL3.pdf (accessed on 23 May 2024).
- Geretti, A.M.; Mardh, O.; de Vries, H.J.C.; Winter, A.; McSorley, J.; Seguy, N.; Vuylsteke, B.; Gokengin, D. Sexual Transmission of Infections across Europe: Appraising the Present, Scoping the Future. Sex. Transm. Infect. 2022, 98, 451–457. [Google Scholar] [CrossRef] [PubMed]
- Rooney, B.M.; Tulloch, T.G.; Blashill, A.J. Psychosocial Syndemic Correlates of Sexual Compulsivity Among Men Who Have Sex with Men: A Meta-Analysis. Arch. Sex. Behav. 2018, 47, 75–93. [Google Scholar] [CrossRef] [PubMed]
- Cheng, P.J. Sexual Dysfunction in Men Who Have Sex with Men. Sex. Med. Rev. 2022, 10, 130–141. [Google Scholar] [CrossRef] [PubMed]
- Kalichman, S.C.; Cain, D. The Relationship between Indicators of Sexual Compulsivity and High Risk Sexual Practices among Men and Women Receiving Services from a Sexually Transmitted Infection Clinic. J. Sex. Res. 2004, 41, 235–241. [Google Scholar] [CrossRef] [PubMed]
- Quadland, M.C. Compulsive Sexual Behavior: Definition of a Problem and an Approach to Treatment. J. Sex. Marital. Ther. 1985, 11, 121–132. [Google Scholar] [CrossRef] [PubMed]
- Parsons, J.T.; Kelly, B.C.; Bimbi, D.S.; DiMaria, L.; Wainberg, M.L.; Morgenstern, J. Explanations for the Origins of Sexual Compulsivity among Gay and Bisexual Men. Arch. Sex. Behav. 2008, 37, 817–826. [Google Scholar] [CrossRef]
- Ni, Y.; Liu, H.; Gong, R.; Shi, M.; Zhang, S.; Wang, S.; Cai, Y. The Role of Sexual Compulsivity in Unprotected Intercourse among STI Patients in Shanghai, China. BMC Public Health 2021, 21, 141. [Google Scholar] [CrossRef]
- Garner, A.R.; Shorey, R.C.; Anderson, S.; Stuart, G.L. Risky Sexual Behaviors among Men in Residential Treatment for Substance Misuse: The Role of Compulsive Sexual Behavior. Sex. Addict. Compulsivity 2020, 27, 135–148. [Google Scholar] [CrossRef]
- Achterbergh, R.C.A.; van Rooijen, M.S.; van den Brink, W.; Boyd, A.; de Vries, H.J.C. Enhancing Help-Seeking Behaviour among Men Who Have Sex with Men at Risk for Sexually Transmitted Infections: The Syn.Bas.in Randomised Controlled Trial. Sex. Transm. Infect. 2020, 97, 11–17. [Google Scholar] [CrossRef] [PubMed]
- Janssen, E.; Prause, N.; Swinburne Romine, R.; Raymond, N.; MacDonald, A.; Coleman, E.; Miner, M.H. Sexual Responsivity and the Effects of Negative Mood on Sexual Arousal in Hypersexual Men Who Have Sex with Men (MSM). J. Sex. Med. 2020, 17, 1751–1760. [Google Scholar] [CrossRef] [PubMed]
- Hergenrather, K.C.; Emmanuel, D.; Zeglin, R.J.; Ruda, D.J.; Rhodes, S.D. Men Who Have Sex with Men and HIV Risk Behavior: Exploring the Influence of Masculinity within the Social Ecological Model. AIDS Educ. Prev. 2021, 33, 511–533. [Google Scholar] [CrossRef] [PubMed]
- Woodhill, B.M.; Samuels, C.A. Positive and Negative Androgyny and Their Relationship with Psychological Health and Well-Being. Sex Roles 2003, 48, 555–565. [Google Scholar] [CrossRef]
- Mayer, K.H.; Bekker, L.G.; Stall, R.; Grulich, A.E.; Colfax, G.; Lama, J.R. Comprehensive Clinical Care for Men Who Have Sex with Men: An Integrated Approach. Lancet 2012, 380, 378–387. [Google Scholar] [CrossRef]
- Concannon, L. Proving Manhood: Gay Culture, Competitiveness, Risk, and Mental Wellbeing. Competitiveness, Risk, and Mental Wellbeing. SocArXir Papers 2022. [Google Scholar] [CrossRef]
- Bacio, M.; Rinaldi, C. Becoming Male Sex Worker, Doing Masculinities. Socio-Sexual Interactions and Gender Production in Men Selling Sex to Men in Italy and Sweden. Ital. J. Sociol. Educ. 2022, 14, 7–30. [Google Scholar]
- Foster, J.; Baker, J. Muscles, Makeup, and Femboys: Analyzing TikTok’s “Radical” Masculinities. Soc. Media Soc. 2022, 8, 20563051221126040. [Google Scholar] [CrossRef]
- Jacques-Aviñó, C.; Garcia de Olalla, P.; Gonzalez Antelo, A.; Fernandez Quevedo, M.; Romaní, O.; Caylà, J.A. The Theory of Masculinity in Studies on HIV. A Systematic Review. Glob. Public Health 2019, 14, 601–620. [Google Scholar] [CrossRef]
- Holmes, D.; Gastaldo, D.; O’byrne, P.; Lombardo, A. Bareback Sex: A Conflation of Risk and Masculinity. Int. J. Mens. Health 2008, 7, 171. [Google Scholar] [CrossRef]
- Vosburgh, H.; Mansergh, G.; Sullivan, P.S.; Purcell, D.W. A Review of the Literature on Event-Level Substance Use and Sexual Risk Behavior among Men Who Have Sex with Men. AIDS Behav. 2012, 16, 1394–1410. [Google Scholar] [CrossRef] [PubMed]
- Berg, R.C. Barebacking: A Review of the Literature. Arch. Sex. Behav. 2009, 38, 754–764. [Google Scholar] [CrossRef] [PubMed]
- Malebranche, D.J.; Fields, E.L.; Bryant, L.O.; Harper, S.R. Masculine Socialization and Sexual Risk Behaviors among Black Men Who Have Sex with Men: A Qualitative Exploration. Men. Masc. 2009, 12, 90–112. [Google Scholar] [CrossRef]
- Fields, E.L.; Bogart, L.M.; Smith, K.C.; Malebranche, D.J.; Ellen, J.; Schuster, M.A. “I Always Felt I Had to Prove My Manhood”: Homosexuality, Masculinity, Gender Role Strain, and HIV Risk among Young Black Men Who Have Sex with Men. Am. J. Public Health 2015, 105, 122–131. [Google Scholar] [CrossRef]
- Perez-Brumer, A.; Konda, K.; Salvatierra, J.; Coates, T.; Hall, E.; Klausner, J.; Clark, J.; Caceres, C.; Segura, E.; Salazar, X. Moderno Love: Sexual Role-Based Identities and HIV/STI Prevention among Men Who Have Sex with Men in Lima, Peru. AIDS Behav. 2013, 17, 1313–1328. [Google Scholar]
- Connell, R.W. Masculinities, 2nd ed.; Polity Press: Cambrige, UK, 2005; ISBN 9781003116479. [Google Scholar]
- Kaplan, R.L.; Sevelius, J.; Ribeiro, K. In the Name of Brevity: The Problem with Binary HIV Risk Categories. Glob. Public Health 2016, 11, 824–834. [Google Scholar] [CrossRef] [PubMed]
- Schmitz, S. Sex, Gender, and the Brain—Biological Determinism versus Socio-Cultural Constructivism. Sex Gend. Biomed. Theor. Methodol. Results 2011, 57–76. [Google Scholar]
- Bem, S.L. The Measurement of Psychological Androgyny. J. Consult. Clin. Psychol. 1974, 42, 155–162. [Google Scholar] [CrossRef]
- Spence, J.T.; Helmreich, R.; Stapp, J. Ratings of Self and Peers on Sex Role Attributes and Their Relation to Self-Esteem and Conceptions of Masculinity and Femininity. J. Pers. Soc. Psychol. 1975, 32, 29–39. [Google Scholar] [CrossRef]
- Bem, S.L. On the Utility of Alternative Procedures for Assessing Psychological Androgyny. J. Consult. Clin. Psychol. 1977, 45, 196–205. [Google Scholar] [CrossRef] [PubMed]
- Matud, M.P.; López-Curbelo, M.; Fortes, D. Gender and Psychological Well-Being. Int. J. Environ. Res. Public Health 2019, 16, 3531. [Google Scholar] [CrossRef] [PubMed]
- Gasch Gallén, Á.; Tomás Aznar, C.; Rubio Aranda, E. Assessing Gender Stereotypes and Sexual Risk Practices in Men Who Have Sex with Men. Gac. Sanit. 2019, 32, 519–525. [Google Scholar] [CrossRef] [PubMed]
- Verhofstadt, L.L.; Weytens, F. Biological Sex and Gender Role Identity as Predictors of Spousal Support Provision: A Scenario-Based Study. J. Gend. Stud. 2013, 22, 166–177. [Google Scholar] [CrossRef]
- Gallén, À.G.; Tomás, C. The Gap of Masculinity in the Research on HIV among Men Who Have Sex with Men: A Review of Quantitative Literature and Theoretical Contributions on Gender and Masculinity Approaches. Soc. Theory Health 2015, 13, 202–218. [Google Scholar] [CrossRef]
- Buchbinder, S.P.; Vittinghoff, E.; Heagerty, P.J.; Celum, C.L.; Seage, G.R.; Judson, F.N.; McKirnan, D.; Mayer, K.H.; Koblin, B.A. Sexual Risk, Nitrite Inhalant Use, and Lack of Circumcision Associated with HIV Seroconversion in Men Who Have Sex with Men in the United States. J. Acquir. Immune Defic. Syndr. (1988) 2005, 39, 82–89. [Google Scholar] [CrossRef] [PubMed]
- Paz-Bailey, G.; Mendoza, M.C.B.; Finlayson, T.; Wejnert, C.; Le, B.; Rose, C.; Raymond, H.F.; Prejean, J.; Taussig, J.; Gern, R.; et al. Trends in Condom Use among MSM in the United States: The Role of Antiretroviral Therapy and Seroadaptive Strategies. Aids 2016, 30, 1985–1990. [Google Scholar] [CrossRef]
- Chaney, M.P.; Burns-Wortham, C.M. Sexual Compulsivity and Men Who Have Sex with Men (MSM). In The Routledge International Handbook of Sexual Addiction; Routledge/Taylor & Francis Group: Montreal, QC, Canada, 2018; pp. 305–316. [Google Scholar] [CrossRef]
- Ballester-Arnal, R.; Gómez-Martínez, S.; Llario, M.D.G.; Salmerón-Sánchez, P. Sexual Compulsivity Scale: Adaptation and Validation in the Spanish Population. J. Sex. Marital. Ther. 2013, 39, 526–540. [Google Scholar]
- Ibáñez-Tomás, E.; Ballester-Arnal, R.; Elipe-Miravet, M.; Gasch-Gallén, Á. Psychometric Properties of the Sexual Compulsivity Scale in Men Who Have Sex with Men in Spanish Population. AIDS Behav. 2022, 27, 1211–1221. [Google Scholar] [CrossRef]
- Gómez Berrocal, C.; Cervilla, O.; Álvarez Muelas, A. The Bem Sex-Role Inventory: Propuesta de una Versión Corta en Español. Ann. Psychol. 2022, 38, 530–537. [Google Scholar]
- Mateo, M.A.; Fernández, J. La Dimensionalidad de Los Conceptos de Masculinidad y Feminidad. Investig. Psicológicas 1991, 9, 95–116. [Google Scholar]
- Rennie, K.M. Exploratory and Confirmatory Rotation Strategies in Exploratory Factor Analysis. In Proceedings of the Annual Meeting of the Southwest Educational Research Association, Austin, TX, USA, 23–25 January 1997; pp. 1–28. [Google Scholar]
- Cronbach, L.J. Coefficient Alpha and the Internal Structure of Tests. Psychometrika 1951, 16, 297–334. [Google Scholar] [CrossRef]
- Hair, J.F.; Anderson, R.E.; Tatham, R.L.; Black, W.C. Análisis Multivariante, 5th ed.; Pearson Prentice Hall: Madrid, Spain, 1999; ISBN 9788578110796. [Google Scholar]
- Blackman, S. Comment on Three Methods of Scoring Androgyny as a Continuous Variable. Pssichol. Rep. 1982, 51, 1100–1102. [Google Scholar] [CrossRef]
- Nebot Garcia, J.E. Estrés de Las Minorías Sexuales y Su Impacto En La Salud Mental de Las Personas LGB+. Ph.D. Dissertation/Tesis, Universidad Jaume I, Castellón de la Plana, Spain, 12 September 2022. [Google Scholar]
- Marcus, U.; Schink, S.B. The European MSM Internet Survey as a Basis for Prevention Work in Germany for Men Who Have Sex with Men. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz 2021, 64, 1430–1439. [Google Scholar] [CrossRef] [PubMed]
- Barreda, V.; Carballo-Dieguez, A.; Marone, R.; Balàn, I.C.; de los Pando, M.A.; àvila, M.M. Prevención Del VIH/SIDA En Los Circuitos de Levante HSH: Una Asignatura Pendiente. Sex. Salud Soc. 2010, 6, 41–62. [Google Scholar] [CrossRef] [PubMed]
- Obarska, K.; Szymczak, K.; Lewczuk, K.; Gola, M. Threats to Mental Health Facilitated by Dating Applications Use among Men Having Sex with Men. Front. Psychiatry 2020, 11, 584548. [Google Scholar] [CrossRef] [PubMed]
- Knoops, L.; van Amsterdam, J.; Albers, T.; Brunt, T.M.; van den Brink, W. Slamsex in The Netherlands among Men Who Have Sex with Men (MSM): Use Patterns, Motives, and Adverse Effects. Sex. Health 2022, 19, 566–573. [Google Scholar] [CrossRef] [PubMed]
- Rollet, D.; Clergue-Duval, V.; Fouere, S.; Segouin, C.; Simon, A.; Ohayon, M.; Aim-Eusebi, A. Chemgen Study: Assessing the Consumption of Care in General Practice of Men with Sexual Relationships with Men Users of Psychoactive Products in a Sexual Context. Sex. Res. Soc. Social. Policy 2022, 19, 1080–1089. [Google Scholar] [CrossRef]
- Numer, M.; Holmes, D.; Hammond, C.; Joy, P.; Sinno, J. Assemblages of Excess and Pleasures: The Sociosexual Uses of Online and Chemical Technologies among Men Who Have Sex with Men. Nurs. Philos. 2022, 23, e12370. [Google Scholar] [CrossRef] [PubMed]
- Danko, M.; Buzwell, S.; Earle, M. Men at Risk of HIV: Sexual Sensation Seeking, Sexual Compulsivity and Sexual Risk Behavior among Australian MSM Who Frequently Present for Post-Exposure Prophylaxis. Sex. Addict. Compulsivity 2016, 23, 324–341. [Google Scholar] [CrossRef]
- Edeza, A.; Galarraga, O.; Novak, D.; Mayer, K.; Rosenberger, J.; Mimiaga, M.; Biello, K. The Role of Sexual Risk Behaviors on PrEP Awareness and Interest among Men Who Have Sex with Men in Latin America. Int. J. STD AIDS 2019, 30, 542–549. [Google Scholar] [CrossRef] [PubMed]
- Dodge, B.; Reece, M.; Herbenick, D.; Fisher, C.; Satinsky, S.; Stupiansky, N. Relations between Sexually Transmitted Infection Diagnosis and Sexual Compulsivity in a Community-Based Sample of Men Who Have Sex with Men. Sex. Transm. Infect. 2008, 84, 324–327. [Google Scholar] [CrossRef] [PubMed]
- Gaissad, L.; Velter, A. “Getting High to Get Laid”. Drugs and Gay Sex under Influence. Sexologies 2019, 28, e48–e53. [Google Scholar] [CrossRef]
- Daroya, E. Online ‘Barebacking’ Community and the Creation of ‘Sex Pig’Identities: Exploring Affordances of a Web Forum in Celebrating Sexual Excess. First Monday 2020, 25, 1–10. [Google Scholar]
- Bowen, A. Internet Sexuality Research with Rural Men Who Have Sex with Men: Can We Recruit and Retain Them? J. Sex Res. 2005, 42, 317–323. [Google Scholar] [CrossRef] [PubMed]
- Geibel, S.; Tun, W.; Tapsoba, P.; Kellerman, S. HIV Vulnerability of Men Who Have Sex with Men in Developing Countries: Horizons Studies, 2001–2008. Public Health Rep. 2010, 125, 316–324. [Google Scholar] [CrossRef] [PubMed]
- Huebner, D.M.; Kegeles, S.M.; Rebchook, G.M.; Peterson, J.L.; Neilands, T.B.; Johnson, W.D.; Eke, A.N. Social Oppression, Psychological Vulnerability, and Unprotected Intercourse among Young Black Men Who Have Sex with Men. Health Psychol. 2014, 33, 1568. [Google Scholar] [CrossRef]
- Mayer, K.H.; Wheeler, D.P.; Bekker, L.-G.; Grinsztejn, B.; Remien, R.H.; Sandfort, T.G.M.; Beyrer, C. Overcoming Biological, Behavioral and Structural Vulnerabilities: New Directions in Research to Decrease HIV Transmission in Men Who Have Sex with Men. J. Acquir. Immune Defic. Syndr. 2013, 63, S161. [Google Scholar] [CrossRef] [PubMed]
- Silva, T. Bud-Sex: Constructing Normative Masculinity among Rural Straight Men That Have Sex with Men. Gend. Soc. 2017, 31, 51–73. [Google Scholar] [CrossRef]
- Szpitalak, M.; Polska, K.P.-P. Psychological gender in clinical depression. Preliminary study. Psychiatria Polska 2013, 47, 53–56. [Google Scholar]
- Eliason, M.J. The Gender Binary in Nursing. Nurs. Inq. 2017, 24, e12176. [Google Scholar] [CrossRef] [PubMed]
- León, S.P.; Sánchez, C.A.; Augusto-Landa, J.M.; García-Martínez, I. Analysis of Sexual Inhibition and Satisfaction from a Gender Perspective among University Students. Int. J. Environ. Res. Public Health 2021, 18, 7994. [Google Scholar] [CrossRef] [PubMed]
- Carver, L.F.; Vafaei, A.; Guerra, R.; Freire, A.; Phillips, S.P. Gender Differences: Examination of the 12-Item Bem Sex Role Inventory (BSRI-12) in an Older Brazilian Population. PLoS ONE 2013, 8, e76356. [Google Scholar] [CrossRef] [PubMed]
- Donnelly, K.; Twenge, J.M. Masculine and Feminine Traits on the Bem Sex-Role Inventory, 1993–2012: A Cross-Temporal Meta-Analysis. Sex Roles 2017, 76, 556–565. [Google Scholar] [CrossRef]
- Vafaei, A.; Alvarado, B.; Tomás, C.; Muro, C.; Martinez, B.; Zunzunegui, M.V. The Validity of the 12-Item Bem Sex Role Inventory in Older Spanish Population: An Examination of the Androgyny Model. Arch. Gerontol. Geriatr. 2014, 59, 257–263. [Google Scholar] [CrossRef] [PubMed]
- Johnson, J.L.; Repta, R. Sex and Gender. Designing and conducting gender, sex, and health research. CJNR 2012, 1737. [Google Scholar]
- Ahmed, T.; Vafaei, A.; Auais, M.; Phillips, S.P.; Guralnik, J.; Zunzunegui, M. V Health Behaviors and Chronic Conditions Mediate the Protective Effects of Masculinity for Physical Performance in Older Adults. J. Aging Health 2018, 30, 1062–1083. [Google Scholar] [CrossRef] [PubMed]
- Ulrich, A.K.; Sanchez, J.; Lama, J.R.; Manhart, L.E.; Goodreau, S.M.; Duerr, A.C. Correlates of Concurrent Partnerships and Patterns of Condom Use among Men Who Have Sex with Men and Transgender Women in Peru. PLoS ONE 2019, 14, e0222114. [Google Scholar] [CrossRef] [PubMed]
- Mayer, K.H.; Nelson, L.; Hightow-Weidman, L.; Mimiaga, M.J.; Mena, L.; Reisner, S.; Daskalakis, D.; Safren, S.A.; Beyrer, C.; Sullivan, P.S. The Persistent and Evolving HIV Epidemic in American Men Who Have Sex with Men. Lancet 2021, 397, 1116–1126. [Google Scholar] [CrossRef]
- Safren, S.A.; Blashill, A.J.; Lee, J.S.; O’Cleirigh, C.; Tomassili, J.; Biello, K.B.; Mimiaga, M.J.; Mayer, K.H. Condom-Use Self-Efficacy as a Mediator between Syndemics and Condomless Sex in Men Who Have Sex with Men (MSM). Health Psychol. 2018, 37, 820. [Google Scholar] [CrossRef]
- Ševčíková, A.; Blinka, L.; Škařupová, K.; Vašek, D. Online Sex Addiction after 50: An Exploratory Study of Age-Related Vulnerability. Int. J. Ment. Health Addict. 2021, 19, 850–864. [Google Scholar] [CrossRef]
- Miller, B. Textually Presenting Masculinity and the Body on Mobile Dating Apps for Men Who Have Sex with Men. J. Mens. Stud. 2018, 26, 305–326. [Google Scholar] [CrossRef]
- Miller, B. A Picture Is Worth 1000 Messages: Investigating Face and Body Photos on Mobile Dating Apps for Men Who Have Sex with Men. J. Homosex. 2020, 67, 1798–1822. [Google Scholar] [CrossRef] [PubMed]
- Parmenter, J.; Crowell, K.; Roles, R.G.-S. Subjective Importance of Masculinity as a Factor in Understanding Risky Sexual Attitudes and Behaviors among Sexual Minority Men. Springer 2020, 82, 463–472. [Google Scholar] [CrossRef]
- Nimbi, F.M.; Ciocca, G.; Limoncin, E.; Fontanesi, L.; Uysal, Ü.B.; Flinchum, M.; Tambelli, R.; Jannini, E.A.; Simonelli, C. Sexual Desire and Fantasies in the LGBT+ Community: Focus on Lesbian Women and Gay Men. Curr. Sex. Health Rep. 2020, 12, 153–161. [Google Scholar] [CrossRef]
- Štulhofer, A.; Jurin, T.; Briken, P. Is High Sexual Desire a Facet of Male Hypersexuality? Results from an Online Study. J. Sex. Marital. Ther. 2016, 42, 665–680. [Google Scholar]
- Peixoto, M.; Nobre, P. Dysfunctional Sexual Beliefs: A Comparative Study of Heterosexual Men and Women, Gay Men, and Lesbian Women with and without Sexual Problems. J. Sex. Med 2014, 11, 2690–2700. [Google Scholar] [CrossRef]

{kind=link}
| n | % | |
|---|---|---|
| Age (years), median [IQR] | 32 [25–40] | |
| <35 | 458 | 52 |
| 35–44 | 209 | 23.7 |
| ≥45 | 108 | 12.3 |
| Place of birth | ||
| Other | 240 | 27 |
| Spain | 641 | 73 |
| Education level | ||
| Secondary school and below | 56 | 6.4 |
| Vocational training | 186 | 21.1 |
| College degree and above | 639 | 72.5 |
| Employment | ||
| Employed | 682 | 77.4 |
| Unemployed | 47 | 5.3 |
| Student | 145 | 16.5 |
| Retired | 7 | 0.8 |
| Monthly income | ||
| ≥€ 1200 | 481 | 54.6 |
| € 700–1200 | 219 | 24.9 |
| ≤€ 700 | 181 | 20.5 |
| Cohabitation Situation | ||
| Stable partner | 196 | 22.2 |
| Alone | 308 | 35 |
| Others (family, shared apartment] | 377 | 42.8 |
| Sexual Compulsivity Scale | Interference of Sexual Behavior Domain | Failure to Control Sexual Impulses Domain | ||||||
|---|---|---|---|---|---|---|---|---|
| Score | Score | Score | ||||||
| n | % | MED [IQR] | p | MED [IQR] | p | MED [IQR] | p | |
| Sexual Orientation | ||||||||
| Heterosexual | 9 | 1 | 18 [15–35] | 0.046 | 7 [5–15] | 0.023 | 13 [8–19.5] | 0.123 |
| Bisexual | 110 | 12.5 | 15 [12–21] | 5 [4–8] | 9 [7–13] | |||
| Gay/homosexual | 755 | 85.7 | 14 [11–18] | 5 [4–7] | 9 [7–12] | |||
| Others | 7 | 0.8 | 18 [11–21] | 6 [5–8] | 11 [6–13] | |||
| Sexual Role | ||||||||
| Active/insertive | 224 | 27.7 | 13 [11–18] | 0.056 | 5 [4–6] | 0.057 | 8 [7–11] | 0.100 |
| Versatile | 433 | 49.1 | 15 [12–20] | 5 [4–7] | 9 [7–12] | |||
| Passive/receptive | 204 | 23.2 | 14 [12–18.75] | 5 [4–7] | 9 [7–12] | |||
| Sexual Partners (past 12 months) | ||||||||
| Regular sexual partners | 73 | 8.3 | 14 [10–17.50] | 0.183 | 5 [4–5.50] | 0.062 | 8 [7–11] | 0.474 |
| Casual sexual partners | 357 | 40.5 | 14 [12–18] | 5 [4–7] | 9 [7–12] | |||
| Both regular/casual | 316 | 35.9 | 15 [11–20] | 5 [4–7] | 9 [7–13] | |||
| Dating apps | ||||||||
| Never | 54 | 6.1 | 13 [11–16] | 0.046 | 4 [4–6] | 0.007 | 8 [6.75–11.25] | 0.175 |
| Sometimes/usually | 827 | 93.9 | 14 [11–19] | 5 [4–7] | 9 [7–16] | |||
| Chemsex participation | ||||||||
| Never | 793 | 90 | 14 [11–18] | <0.001 | 5 [4–7] | <0.001 | 9 [7–12] | 0.004 |
| Sometimes/usually | 88 | 10 | 17 [13–23.75] | 7 [4.25–8] | 10.5 [7–14] | |||
| Sex while under the influence of drugs | ||||||||
| No | 654 | 74.2 | 14 [11–18] | <0.001 | 5 [4–6] | <0.001 | 9 [7–12] | 0.031 |
| Yes | 227 | 25.8 | 15 [12–21] | 6 [4–8] | 9 [7–13] | |||
| PrEP use | ||||||||
| Never | 813 | 92.3 | 14 [11–19] | 0.202 | 5 [4–7] | 0.156 | 9 [7–12] | 0.503 |
| Sometimes/usually | 68 | 7.7 | 15.50 [12–20] | 5 [4–8] | 9 [7–12] | |||
| Previous diagnosis of STIs | ||||||||
| No | 449 | 51 | 14 [11–19] | 0.865 | 5 [4–6] | 0.074 | 9 [7–12] | 0.251 |
| Yes | 432 | 49 | 14 [11–19] | 5 [4–7] | 9 [7–12] | |||
| Black-kissing | ||||||||
| Never | 274 | 31.1 | 14 [11–18.25] | 0.148 | 5 [4–6] | 0.002 | 9 [7–12] | 0.697 |
| Sometimes/usually | 607 | 68.9 | 14 [12–19] | 5 [4–7] | 9 [7–12] | |||
| Face-sitting | ||||||||
| Never | 679 | 77.1 | 14 [11–18] | <0.001 | 5 [4–7] | <0.001 | 9 [7–12] | <0.001 |
| Sometimes/usually | 202 | 22.9 | 16 [12–21] | 6 [4–8] | 10 [7–14] | |||
| Felching | ||||||||
| Never | 823 | 93.4 | 14 [11–19] | 0.105 | 5 [4–7] | 0.297 | 9 [7–12] | 0.054 |
| Sometimes/usually | 58 | 6.6 | 15 [12–20.25] | 5 [4–7] | 10 [7.75–13] | |||
| Introduction of fingers | ||||||||
| Never | 185 | 21 | 14 [11–19] | 0.546 | 5 [4–7] | 0.102 | 9 [7–12] | 0.870 |
| Sometimes/usually | 696 | 79 | 14 [12–19] | 5 [4–7] | 9 [7–12] | |||
| Introduction of objects | ||||||||
| Never | 546 | 62 | 14 [11–18] | 0.040 | 5 [4–7] | 0.195 | 9 [7–12] | 0.034 |
| Sometimes/usually | 335 | 38 | 14 [12–20] | 5 [4–7] | 9 [7–12] | |||
| Fisting | ||||||||
| Never | 758 | 86 | 14 [11–18] | <0.001 | 5 [4–7] | <0.001 | 9 [7–12] | 0.007 |
| Sometimes/usually | 123 | 14 | 16 [13–22] | 6 [4–8] | 10 [7–14] | |||
| Factor 1 | Factor 2 | |
|---|---|---|
| Items BSRI-12 | Feminine: Expressive Characteristics | Masculine: Instrumental Characteristics |
| BSRI_1: Gentle | 0.850 | |
| BSRI_2: Compressive | 0.872 | |
| BSRI_3: Has leadership abilities | 0.833 | |
| BSRI_4: Acts as a leader | 0.878 | |
| BSRI_5: Dominant | 0.787 | |
| BSRI_6: Tender | 0.849 | |
| BSRI_7: Warm | 0.867 | |
| BSRI_8: Affectionate | 0.883 | |
| BSRI_9: Strong personality | 0.656 | |
| BSRI_10: Defender of own beliefs | 0.678 | |
| BSRI_11: Sensitive to others’ needs | 0.814 | |
| BSRI_12: Makes decisions easily | 0.615 | |
| Cronbach’s Alpha | 0.947 | 0.857 |
| % Explained variance | 57.56 | 15.07 |
| Gender Role Categories | Sexual Compulsivity Scale Scores | ||||||
|---|---|---|---|---|---|---|---|
| Median < 14 | Median ≥ 14 | ||||||
| n | % | n | % | n | % | p | |
| Feminine | 120 | 13.6 | 57 | 14.7 | 63 | 12.8 | 0.007 |
| Masculine | 153 | 17.4 | 66 | 17 | 87 | 17.7 | |
| Androgynous | 283 | 32.1 | 103 | 26.5 | 180 | 36.6 | |
| Undifferentiated | 325 | 36.9 | 163 | 41.9 | 162 | 32.9 | |
| Overall participants | 881 | 100 | 389 | 44.2 | 492 | 55.8 | |
| Overall Participants (n = 881) | Androgynous (n = 283; 32.1%) | Feminine (n = 120; 13.6%) | Masculine (n = 153; 17.4%) | Undifferentiated (n = 325; 36.9%) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Items | Range | MED | [IQR] | MED | [IQR] | MED | [IQR] | MED | [IQR] | MED | [IQR] | p | |||
| Sexual Compulsivity Scale | 10 | 10–40 | 14 | [11–19] | 15 | [12–20] | 14 | [11–19] | 15 | [12–20] | 13 | [11–17] | <0.001 | ||
| Interference of sexual behavior | 4 | 4–16 | 5 | [4–7] | 5 | [4–7] | 5 | [4–7] | 5 | [4–7] | 5 | [4–6] | <0.001 | ||
| Failure to control sexual impulses | 6 | 6–24 | 9 | [7–12] | 9 | [7–12] | 9 | [7–12.7] | 10 | [7–13] | 8 | [7–11] | 0.015 | ||
| Gender Stereotypes and Sexual Compulsivity Dimensions | Wald | df | Sig. | OR | 95% C.I. | |
|---|---|---|---|---|---|---|
| Lower | Higher | |||||
| FEMININE COMPULSIVITY (GLOBAL) | ||||||
| UNPROTECTED SEXUAL PRACTICES | ||||||
| Face-sitting | 4.286 | 1 | 0.038 | 5.749 | 1.098 | 30.109 |
| FEMININE INTERFERENCE | ||||||
| COHABITATION SITUATION | ||||||
| Stable partner | 4.348 | 2 | 0.114 | Reference | ||
| Alone | 3.639 | 1 | 0.056 | 0.250 | 0.060 | 1.039 |
| Others (family, shared apartment] | 3.211 | 1 | 0.073 | 0.239 | 0.050 | 1.144 |
| SEXUAL ROLE | ||||||
| Active/insertive | 5.834 | 2 | 0.054 | Reference | ||
| Versartile | 4.485 | 1 | 0.034 | 5.261 | 1.132 | 24.459 |
| Passive/receptive | 5.339 | 1 | 0.021 | 8.123 | 1.374 | 48.011 |
| MASCULINE COMPULSIVITY (GLOBAL) | ||||||
| EDUCATION LEVEL | ||||||
| Secondary school and below | 5.727 | 2 | 0.057 | Reference | ||
| Vocational training | 0.038 | 1 | 0.845 | 0.866 | 0.204 | 3.673 |
| College degree and above | 5.315 | 1 | 0.021 | 9.014 | 1.390 | 58.434 |
| MASCULINE INTERFERENCE | ||||||
| EDUCATION LEVEL | ||||||
| Secondary school and below | 4.053 | 2 | 0.132 | Reference | ||
| Vocational training | 3.985 | 1 | 0.046 | 0.313 | 0.100 | 0.979 |
| College degree and above | 0.279 | 1 | 0.597 | 0.609 | 0.097 | 3.836 |
| SEXUAL ROLE | ||||||
| Active/insertive | 3.746 | 2 | 0.154 | Reference | ||
| Versatile | 2.056 | 1 | 0.152 | 2.365 | 0.729 | 7.668 |
| Passive/receptive | 3.705 | 1 | 0.054 | 3.652 | 0.977 | 13.657 |
| SEXUAL ORIENTATION | ||||||
| Heterosexual | 10.287 | 3 | 0.016 | Reference | ||
| Bisexual | 0.044 | 1 | 0.835 | 1.429 | 0.050 | 40.855 |
| Gay/homosexual | 1.305 | 1 | 0.253 | 0.147 | 0.006 | 40.855 |
| Others | 0 | 1 | 1.000 | 0 | 0 | - |
| UNPROTECTED SEXUAL PRACTICES | ||||||
| Fisting | 3.856 | 1 | 0.050 | 3.435 | 1.002 | 11.771 |
| ANDROGYNOUS COMPULSIVITY (GLOBAL) | ||||||
| COHABITATION SITUATION | ||||||
| Stable partner | 8.960 | 2 | 0.011 | Reference | ||
| Alone | 4.773 | 1 | 0.029 | 0.310 | 0.108 | 0.888 |
| Others (family, shared apartment] | 8.326 | 1 | 0.004 | 0.215 | 0.076 | 0.611 |
| SEXUAL ORIENTATION | ||||||
| Heterosexual | 5.750 | 3 | 0.124 | Reference | ||
| Bisexual | 3.170 | 1 | 0.075 | 0.003 | 0.008 | 1.258 |
| Gay/homosexual | 5.404 | 1 | 0.020 | 0.061 | 0.006 | 0.645 |
| Others | 0 | 1 | 0.999 | 0 | 0 | - |
| ANDROGYNOUS INTERFERENCE | ||||||
| UNPROTECTED SEXUAL PRACTICES | ||||||
| Chemsex | 3.912 | 1 | 0.048 | 2.708 | 1.009 | 7.266 |
| UNDIFFERENTIATED COMPULSIVITY (GLOBAL) | ||||||
| UNPROTECTED SEXUAL PRACTICES | ||||||
| Face-sitting | 7.442 | 1 | 0.006 | 3.611 | 1.435 | 9.083 |
| UNDIFFERENTIATED INTERFERENCE | ||||||
| UNPROTECTED SEXUAL PRACTICES | ||||||
| Sex under the influence of drugs | 3.675 | 1 | 0.055 | 2.200 | 0.983 | 4.927 |
| Face-sitting | 4.968 | 1 | 0.026 | 2.119 | 1.095 | 4.103 |
| UNDIFFERENTIATED FAILURE OF CONTROL | ||||||
| SEXUAL ROLE | ||||||
| Active/insertive | 4.316 | 2 | 0.116 | Reference | ||
| Versartile | 3.928 | 1 | 0.047 | 2.028 | 1.008 | 4.081 |
| Passive/receptive | 0.244 | 1 | 0.622 | 1.267 | 0.495 | 3.238 |
| UNPROTECTED SEXUAL PRACTICES | ||||||
| Face-sitting | 8.433 | 1 | 0.004 | 2.696 | 1.380 | 5.265 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ibáñez-Tomás, E.; Gasch-Gallén, Á. Sexual Compulsivity and Gender Stereotypes in Men Who Have Sex with Men: A Cross-Sectional Study in Spain. Sexes 2024, 5, 85-100. https://doi.org/10.3390/sexes5020007
Ibáñez-Tomás E, Gasch-Gallén Á. Sexual Compulsivity and Gender Stereotypes in Men Who Have Sex with Men: A Cross-Sectional Study in Spain. Sexes. 2024; 5(2):85-100. https://doi.org/10.3390/sexes5020007
Chicago/Turabian StyleIbáñez-Tomás, Eduardo, and Ángel Gasch-Gallén. 2024. "Sexual Compulsivity and Gender Stereotypes in Men Who Have Sex with Men: A Cross-Sectional Study in Spain" Sexes 5, no. 2: 85-100. https://doi.org/10.3390/sexes5020007
APA StyleIbáñez-Tomás, E., & Gasch-Gallén, Á. (2024). Sexual Compulsivity and Gender Stereotypes in Men Who Have Sex with Men: A Cross-Sectional Study in Spain. Sexes, 5(2), 85-100. https://doi.org/10.3390/sexes5020007