Misconceptions and Unmet Need for Modern Contraception among Cambodian Females: A Mix Methods Study


Abstract
:1. Introduction
Aim
2. Materials and Methods
2.1. Ethics
2.2. Quantitative Methods
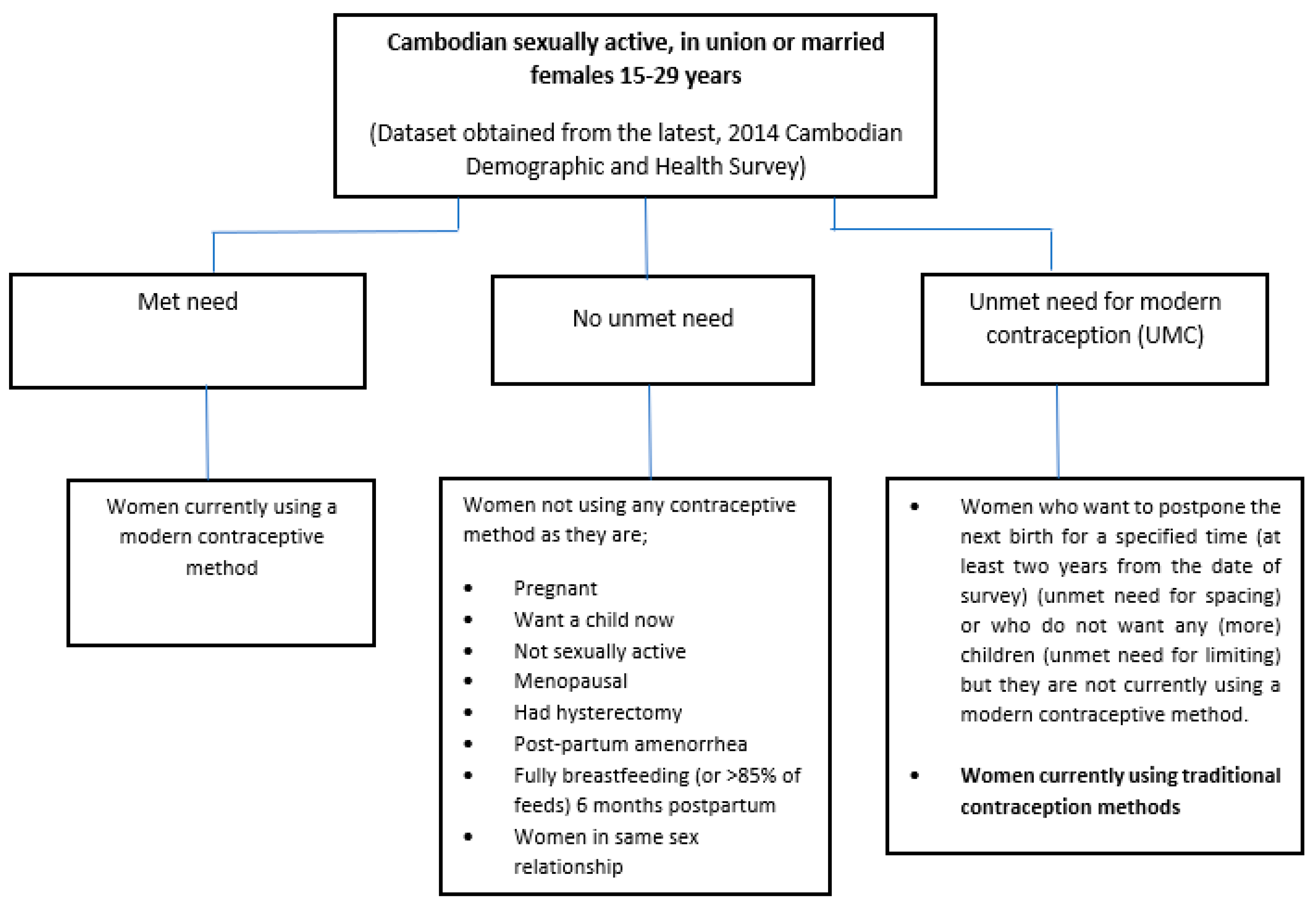
2.3. Standard DHS Approach for Calculating Unmet Need for Contraception
2.4. Rationale for Including Cambodian Females Aged 15–29 Years
2.5. Summary of Our Proposed Categories for Unmet Need for Modern Contraception
3. Results
3.1. Quantitative Statistical Analyses
3.2. Multiple Independent Variables
3.3. Bivariate and Binary Logistic Regression Analyses
3.4. Knowledge of Contraception Methods and Menstrual Cycle
3.5. Contraceptive Prevalence Rate (CPR)
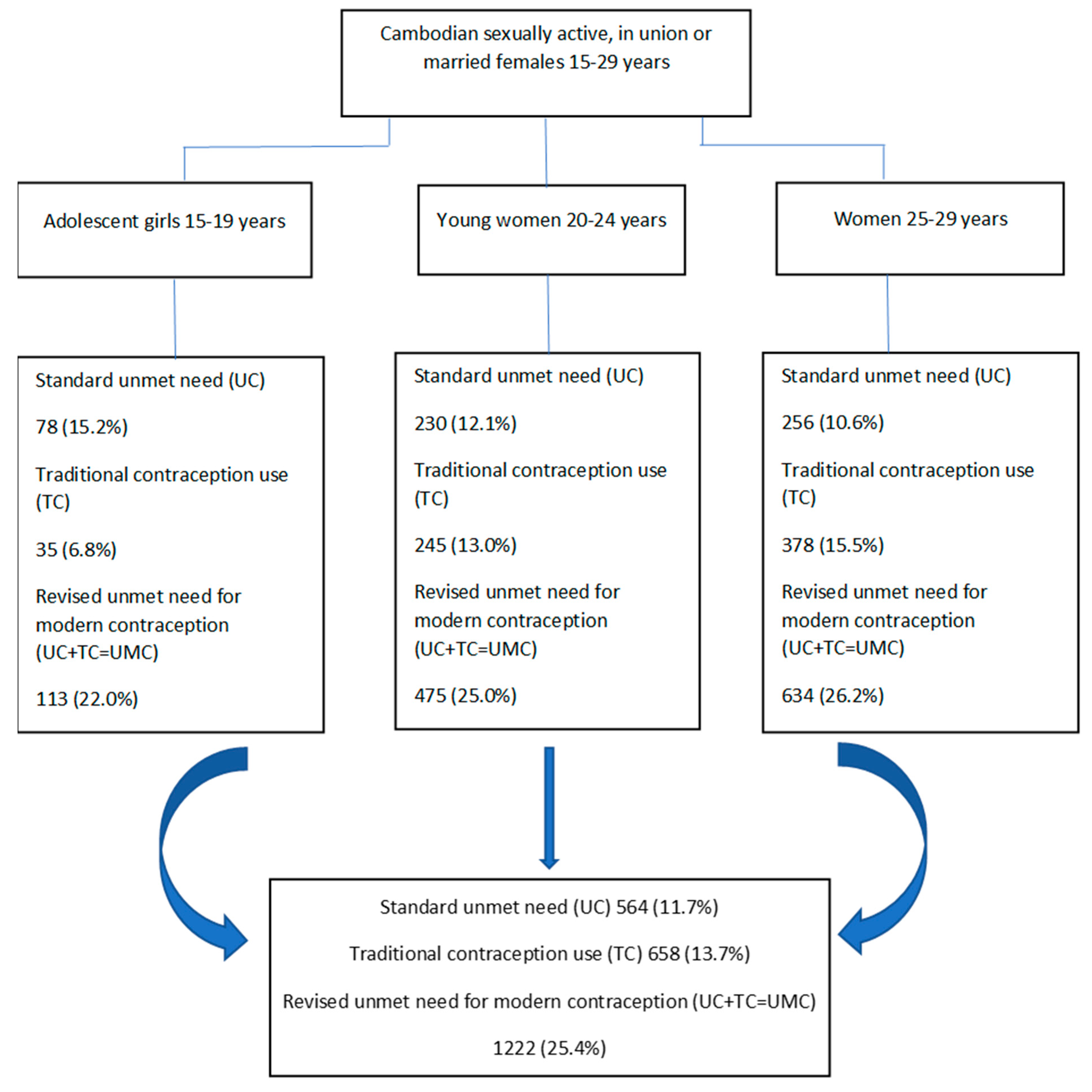
3.6. Revised Calculation of Unmet Need for Modern Contraception
3.7. Demand Satisfied for Modern Contraception (DSMC)
3.8. Qualitative Methods
3.9. Qualitative Data Analysis
3.10. Qualitative Results
4. Major and Minor Themes
4.1. Lack of Knowledge about Menstrual Cycle
“Yes, if the woman sleeps with a man, she is safe after the periods, umm…from day eight”.(P9, 25 years, married)
“She is not safe during these days (she can become pregnant) …the 5 days before the bleeding and during the bleeding days”.(P12, 20 years, sexually active)
4.2. Misconceptions about Modern Contraception
4.2.1. Fear of Health Side-Effects with Oral Pills
“I can see how the body changes (weight loss) and headaches…Some of my friends gave me information and told me what is inside of the prescription for oral pills, and I have already decided not to use it”.(P6, 23 years, sexually active)
4.2.2. Fear of IUCD as Foreign Object
“For coil (IUCD), some people (women) will lose weight or get sick, too much bleeding. The coil is not safe, it can get out in my body and maybe badly affect my stomach, I will get sick and thin”.(P09, 25 years, married with one child)
4.2.3. Fear of Infertility with Hormone-Based Modern Methods
“After they (women) use it (oral pills) for a long time and when they want to have a baby, they cannot have it”.(P12, 20 years, sexually active)
“Pills can cause a woman not to have a baby forever, so not good for her”.(P1, 19 years, single and not sexually active)
“I will wait to use the injection or (oral) pills once I get one baby. Afterwards, I will use the pills, because if we use it right before having baby, then baby is delayed. However, if we use it after we had a baby, it is ok”.(P14, 20 years, not sexually active)
4.3. Use of Withdrawal Method by Partners and Husbands
“My boyfriend is using natural method (withdrawal). He wants it this way as he says it is safe”.(P10, 19 years, sexually active)
5. Discussion
6. Limitations
7. Conclusions
7.1. Recommendations
7.1.1. Sexual and Reproductive Health Literacy Program
7.1.2. Focus on Acceptability, Affordability and Availability of Modern Contraceptives
7.1.3. Modern Contraception Information via the Internet and Social Media
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Razavi, S. The 2030 Agenda: Challenges of implementation to attain gender equality and women’s rights. Gend. Dev. 2016, 24, 25–41. [Google Scholar] [CrossRef]
- UN. Sustainable Development Goals (SDGs) Knowledge Platform. United Nations-Department of Economic and Social Affairs. 2015. Available online: https://sustainabledevelopment.un.org/sdgs (accessed on 12 August 2020).
- WHO. Health in 2015: From MDGs, Millennium Development Goals to Sdgs, Sustainable Development Goals. 2015. Available online: https://www.who.int/gho/publications/mdgs-sdgs/en/ (accessed on 15 July 2020).
- Starrs, A.M.; Ezeh, A.; Barker, G.; Basu, A.; Bertrand, J.T.; Blum, R.; Coll-Seck, A.M.; Grover, A.; Laski, L.; Roa, M.; et al. Accelerate progress—sexual and reproductive health and rights for all: Report of the Guttmacher– Lancet Commission. Lancet 2018, 391, 2642–2692. [Google Scholar] [CrossRef]
- Bradley, S.E.; Croft, T.N.; Fishel, J.D.; Westoff, C.F. Revising Unmet Need for Family Planning; United States Agency for International Development; ICF International: Calverton, MD, USA, 2012; Available online: https://dhsprogram.com/pubs/pdf/AS25/AS25[12June2012].pdf (accessed on 2 February 2020).
- Cahill, N.; Sonneveldt, E.; Stover, J.; Weinberger, M.; Williamson, J.; Wei, C.; Brown, W.; Alkema, L. Modern contraceptive use, unmet need, and demand satisfied among women of reproductive age who are married or in a union in the focus countries of the Family Planning 2020 initiative: A systematic analysis using the Family Planning Estimation Tool. Lancet 2018, 391, 870–882. [Google Scholar] [CrossRef] [Green Version]
- DHS; CNIS; ICF. Cambodia Demographic and Health Survey 2014; National Institute of Statistics/Cambodia, Directorate General for Health/Cambodia, ICF International, The DHS Program; ICF International: Rockville, MD, USA, 2015; Available online: http://dhsprogram.com/pubs/pdf/FR312/FR312.pdf (accessed on 20 February 2020).
- Audu, B.M.; Yahya, S.J.; Bassi, A. Knowledge, Attitude and Practice of Natural Family Planning Methods in A Population with Poor Utilisation of Modern Contraceptives. J. Obstet. Gynaecol. 2006, 26, 555–560. [Google Scholar] [CrossRef]
- Rizvi, F.; Williams, J.; Hoban, E. Factors Influencing Unintended Pregnancies amongst Adolescent Girls and Young Women in Cambodia. Int. J. Environ. Res. Public Heal. 2019, 16, 4006. [Google Scholar] [CrossRef] [Green Version]
- Rizvi, F.; Williams, J.; Bowe, S.; Hoban, E. Factors influencing unmet need for contraception amongst adolescent girls and women in Cambodia. PeerJ 2020, 8, e10065. [Google Scholar] [CrossRef]
- Rizvi, F.; Williams, J.; Maheen, H.; Hoban, E. Using Social Ecological Theory to Identify Factors Associated With Risky Sexual Behavior in Cambodian Adolescent Girls and Young Women Aged 10 to 24 Years: A Systematic Review. Asia Pac. J. Public Heal. 2020, 32, 71–80. [Google Scholar] [CrossRef]
- Metheny, N.; Stephenson, R. How the Community Shapes Unmet Need for Modern Contraception: An Analysis of 44 Demographic and Health Surveys. Stud. Fam. Plan. 2017, 48, 235–251. [Google Scholar] [CrossRef]
- Creswell, J.W.; Hirose, M. Mixed methods and survey research in family medicine and community health. Fam. Med. Community Heal. 2019, 7, e000086. [Google Scholar] [CrossRef] [Green Version]
- USAID. The DHS Program—Demographic and Health Surveys Available Datasets. Available online: https://dhsprogram.com/data/available-datasets.cfm (accessed on 23 July 2020).
- CNIS. 2017 National Institute of Statistics. Ministry of Planning, Phnom Penh. National Institute of Statistics Cambodia. Available online: http://www.nis.gov.kh/index.php/en/about (accessed on 10 June 2020).
- Vandenbroucke, J.P.; Von Elm, E.; Altman, D.G.; Gøtzsche, P.C.; Mulrow, C.D.; Pocock, S.J.; Poole, C.; Schlesselman, J.J.; Egger, M.; Initiative, S. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): Explanation and elaboration. PLoS Med. 2007, 4, e297. [Google Scholar] [CrossRef] [Green Version]
- USAID. Family Planning and Reproductive Health Indicators. MEASURE EVALUATION. 2015. Available online: https://www.measureevaluation.org/prh/rh_indicators (accessed on 19 May 2020).
- Peng, C.-Y.J.; Lee, K.L.; Ingersoll, G.M. An Introduction to Logistic Regression Analysis and Reporting. J. Educ. Res. 2002, 96, 3–14. [Google Scholar] [CrossRef]
- UNFPA; CNIS. Sexual and Reproductive Health of Adolescents and Youth in Cambodia. Analysis of 2000–2014 Cambodia Demographic and Health Survey Data. UNFPA and National Institute of Statistics Cambodia. 2016. Available online: https://cambodia.unfpa.org/sites/default/files/pub-pdf/UNFPA_Final_Report_10_October_2016_5pm%28NRT_reformated%29.pdf (accessed on 18 July 2020).
- Sinai, I.; Igras, S.; Lundgren, R. A practical alternative to calculating unmet need for family planning. Open Access J. Contracept. 2017, 8, 53–59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Booth, A.; Hannes, K.; Harden, A.; Noyes, J.; Harris, J.; Tong, A. COREQ (Consolidated Criteria for Reporting Qualitative Studies); Wiley: Hoboken, NJ, USA, 2014; pp. 214–226. [Google Scholar]
- Webber, G.C.; Spitzer, D.L.; Somrongthong, R.; Dat, T.C.; Kounnavongsa, S. Facilitators and barriers to accessing reproductive health care for migrant beer promoters in Cambodia, Laos, Thailand and Vietnam: A mixed methods study. Glob. Heal. 2012, 8, 21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liamputtong, P.; Serry, T. Making Sense of Qualitative Data. Research Methods in Health: Foundations for Evidence-Based Practice; OUP: Oxford, UK, 2013; pp. 365–379. [Google Scholar]
- Rettke, H.; Pretto, M.; Spichiger, E.; Frei, I.A.; Spirig, R. Using Reflexive Thinking to Establish Rigor in Qualitative Research. Nurs. Res. 2018, 67, 490–497. [Google Scholar] [CrossRef] [PubMed]
- Belotto, M.J. Data analysis methods for qualitative research: Managing the challenges of coding, interrater reliability, and thematic analysis. Qual. Rep. 2018, 23, 2622–2633. [Google Scholar]
- Miles, M.; Huberman, M.; Saldana, J. Drawing and Verifying Conclusions. In Qualitative Data Analysis: A Methods Sourcebook; Sage Publications Inc.: Thousand Oaks, CA, USA, 2016; pp. 275–322. [Google Scholar]
- Cleland, J.; Harbison, S.; Shah, I.H. Unmet need for contraception: Issues and challenges. Stud. Fam. Plan. 2014, 45, 105–122. [Google Scholar] [CrossRef] [PubMed]
- Apter, D. Contraception Options: Aspects Unique to Adolescent and Young Adult. Best Pract. Res. Clin. Obstet. Gynaecol. 2018, 48, 115–127. [Google Scholar] [CrossRef]
- Duane, M.; Contreras, A.; Jensen, E.T.; White, A. The performance of fertility awareness-based method apps marketed to avoid pregnancy. J. Am. Board Fam. Med. 2016, 29, 508–511. [Google Scholar] [CrossRef] [Green Version]
- Samandari, G.; Speizer, I.S.; O’Connell, K. The role of social support and parity on contraceptive use in Cambodia. Int. Perspect. Sex. Reprod. Health 2010, 36, 122–131. [Google Scholar] [CrossRef]
- UNFPA. Sexual and Reproductive Health and Rights: An Essential Element of Universal Health Coverage. Background document for the Nairobi Summit on ICPD 25—Accelerating the Promise; UNFPA: New York, NY, USA, 2019; p. 44. Available online: https://www.unfpa.org/featured-publication/sexual-and-reproductive-health-and-rights-essential-element-universal-health (accessed on 14 August 2020).
- Webber, G.; Edwards, N.; Amaratunga, C.; Graham, I.D.; Keane, V.; Ros, S. Knowledge and views regarding condom use among female garment factory workers in Cambodia. Southeast Asian J. Trop. Med. Public Health 2010, 41, 685–695. [Google Scholar]
- Webber, G.C.; Spitzer, D.L.; Somrongthong, R.; Dat, T.C.; Kounnavongsa, S. Migrant Beer Promoters’ Experiences Accessing Reproductive Health Care in Cambodia, Laos, Thailand, and Vietnam: Lessons for Planners and Providers. Asia Pac. J. Public Health 2015, 27, NP1228–NP1240. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- UNFPA. Program of Cooperation between The Royal Government of Cambodia and the United Nations Population Fund 2016–2018. Country Program Action Plan (CPAP). Available online: http://www.cdc-crdb.gov.kh/cdc/Donor_Development_Cooperation_Programs/undaf/cpap_meeting_2015/download/Draft_Cambodia_CPAP_2016_2018.pdf (accessed on 25 August 2020).
- Ewerling, F.; Victora, C.G.; Raj, A.; Coll, C.V.; Hellwig, F.; Barros, A.J. Demand for family planning satisfied with modern methods among sexually active women in low-and middle-income countries: Who is lagging behind? BMC Reprod. Health 2018, 15, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dude, A.; Neustadt, A.; Martins, S.; Gilliam, M. Use of withdrawal and unintended pregnancy among females 15–24 years of age. Obstet. Gynecol. 2013, 122, 595–600. [Google Scholar] [CrossRef] [PubMed]
- Johnson, R. Young Adult Males’ Attitudes, Perceptions and Behaviours in Regards to Male Condoms in Cambodia. Major Project HSH733/734, Deakin University. 2019. Available online: https://www.classrank.com.au/courses/deakin/HSH734 (accessed on 8 November 2020).



{kind=link}
{kind=link}
| Variable | Frequency (N) | Percentage (%) |
|---|---|---|
| Age | ||
| 15–19 years | 512 | 10.6 |
| 20–24 years | 1893 | 39.2 |
| 25–29 years | 2418 | 50.1 |
| Marital status | ||
| Single | 47 | 0.9 |
| Married | 4401 | 91.2 |
| Living with partner | 49 | 1.0 |
| Widowed | 74 | 1.5 |
| Divorced | 218 | 4.5 |
| Separated (No longer living together) | 34 | 0.7 |
| Educational level | ||
| Higher | 230 | 4.8 |
| Secondary | 1950 | 40.4 |
| Primary | 2154 | 44.6 |
| No education | 489 | 10.1 |
| Wealth status | ||
| Richest | 1224 | 25.4 |
| Richer | 917 | 19.0 |
| Middle | 815 | 16.9 |
| Poorer | 910 | 18.9 |
| Poorest | 957 | 19.8 |
| Current employment | ||
| Yes | 3231 | 67.0 |
| No | 1592 | 33.0 |
| Current contraception use | ||
| Modern methods | 1706 | 35.4 |
| Traditional methods | 658 | 13.6 |
| No contraception use | 2459 | 51.0 |
| Traditional method use | ||
| Withdrawal method | 561 | 11.7 |
| Periodic abstinence | 84 | 1.8 |
| Other traditional/folk methods | 13 | 0.3 |
| Modern methods use | ||
| Oral pills | 824 | 17.1 |
| Injections | 429 | 8.9 |
| IUCD | 190 | 3.9 |
| Norplant | 129 | 2.6 |
| Condoms | 110 | 2.3 |
| Female sterilisation (tubal ligation) | 24 | 0.5 |
| Non-use of contraception methods | 2459 | 50.9 |
| Reason of last contraceptive discontinuation n = 1654 (34.3%) | ||
| Became pregnant | 217 | 4.5 |
| Wanted to become pregnant | 790 | 16.4 |
| Husband disapproved | 16 | 0.3 |
| Health concerns/side-effects | 292 | 6.1 |
| Issues of accessibility or availability | 13 | 0.3 |
| Wanted more effective method | 82 | 1.7 |
| Inconvenient to use | 127 | 2.6 |
| Infrequent sex, or difficult to get pregnant or marital dissolution | 61 | 1.3 |
| Other | 52 | 1.1 |
| Missing | 3173 | 65.7 |
| Total | 4823 | 100 |
| Ever told about family planning at the health facility | ||
| Yes | 1230 | 25.5 |
| No | 1379 | 28.5 |
| Total | 2609 | 54.1 |
| Ever had a terminated pregnancy | ||
| Yes | 1037 | 21.5 |
| No | 3786 | 78.5 |
| Total | 4823 | 100 |
| Ever heard about HIV and sexually transmitted infections | ||
| Yes | 4699 | 97.4 |
| No | 124 | 2.6 |
| Person to decide for respondent’s healthcare | ||
| Respondent alone | 1816 | 37.6 |
| Together | 2240 | 46.4 |
| Husband alone | 355 | 7.4 |
| Someone else in the household (mother-in-law or parents-in-law) | 37 | 0.8 |
| Total | 4448 | 92.2 |
| Missing | 375 | 7.8 |
| Difficulty in getting to the health facility | ||
| Yes | 1663 | 34.5 |
| No | 3160 | 65.5 |
| Participant heard family planning on radio in the last few months | ||
| Yes | 1775 | 36.8 |
| No | 3048 | 63.2 |
| Participant heard family planning on television in the last few months | ||
| Yes | 2378 | 49.3 |
| No | 2445 | 50.7 |
| Factors Influencing Unmet Need for Modern Contraception | Unmet Need for Modern Contraception | Unmet Need for Modern Contraception (Binary Logistic Regression Analyses) |
|---|---|---|
| (Chi-Square) | ||
| p-Value (N = 4823) | Adjusted Odds Ratio (AOR), 95% Confidence Interval (CI) with p-Values (N = 4823) | |
| Age Group | ||
| 15–19 years | p = 0.1 | |
| 20–24 years | 1.1 (0.8–1.6), p = 0.300 | |
| 25–29 years (base) | 1.07 (0.9–1.2), p = 0.500 | |
| Region | ||
| Urban | p = 0.001 | 1.8 (1.5–2.2), p = 0.001 |
| Rural (base) | ||
| Parity | ||
| 1–2 children | p = 0.001 | |
| 3 or more children | 2.3 (1.7–2.7) p = 0.001 | |
| No children (base) | 3.0 (2.1–4.2) p = 0.001 |
| Id No | Age in Years | Education Status | Job Description | Place of Residence | Relationship Status | Current Contraception Method Used/Desire for Future Contraception |
|---|---|---|---|---|---|---|
| P01 | 19 | 1st year university | Student full time | Phnom Penh | Single (not sexually active) | - |
| P02 | 17 | Year 11 | Student full time | Phnom Penh | Single (not sexually active) | Interested in subdermal implant in future |
| P03 | 18 | Year 12 | Student and part time work at a beauty salon | Phnom Penh | Single (not sexually active) | Interested in subdermal implant if in a steady relationship |
| P04 | 16 | Year 10 | Student full time | Phnom Penh | Single (not sexually active) | Interested in subdermal implant in future |
| P05 | 18 | Year 11 | Student full time | Phnom Penh | Single (not sexually active) | Interested in subdermal implant in future |
| P06 | 23 | Bachelor Degree | Junior manager environment | Phnom Penh | Sexually active (has a partner currently) | Partner using withdrawal method |
| P07 | 26 | Year 6 | Garment factory worker | Phnom Penh | Married (1 month) | Not using any contraception as husband wants to have a baby |
| P08 | 24 | Year 5 | Shop keeper | Phnom Penh | Married (3 years)One child 2 years old | Initially, withdrawal method used, then switched to oral tablets after first child (unintended pregnancy) |
| P09 | 25 | Year 6 | Garment factory worker | Phnom Penh | Married (6 years)One child 5 years old | Initially, calendar method used for a few months, then withdrawal method used. After first child (unintended pregnancy), she switched to IUCD for 3 months, then switched to oral tablets |
| P10 | 19 | 1st year university | Student full time | Phnom Penh | Sexually active (has a partner for previous 4–6 months) | Partner using withdrawal method, she is interested in subdermal implant |
| P11 | 17 | 1st year university | Student full time | Phnom Penh | Single (not sexually active) | Interested in subdermal implant in future |
| P12 | 20 | 2nd year university | Student full time | Phnom Penh | Sexually active (has a partner for previous 3–4 months) | Initially, calendar method used for one month, then withdrawal method |
| P13 | 25 | Year 12 | Housewife | Phnom Penh | Married (7 years), Married at 18 years, One child 5 years | Husband using withdrawal method; she is interested in either IUCD or subdermal implant but not available at the health centre or pharmacies |
| P14 | 20 | 2nd year university | Part time cashier in a mini mart | Phnom Penh | Single (not sexually active) | - |
| P15 | 27 | Year 12 | Part time shop worker | Phnom Penh | Married 8 years 2 children; 6 years and 3.5 years | Initially, withdrawal method used, then switched to IUCD for 3 months but due to heavy bleeding in periods, shifted to oral tablets after second child (unintended pregnancy) |
| P16 | 22 | Bachelors in Information Technology | Administration and finance assistant | Phnom Penh | Married (1 month) | Husband sometimes uses withdrawal method and wife is using calendar method |
| P17 | 23 | Year 8 | Housewife | Siem Reap Province | Married 4 years 1 child 1 year old | Initially, calendar method for a few months, then withdrawal method |
| P18 | 24 | Year 7 | Housewife | Siem Reap Province | Married 5 years 2 children 4 years and 1.5 years old | Initially, withdrawal method used, then switched to oral tablets after second child (unintended pregnancy) |
| P19 | 26 | Year 7 | Part time shop worker | Phnom Penh | Married 7 years 2 children 6 years and 2 years | Initially, withdrawal method used, then switched to oral tablets after second child (unintended pregnancy) |
| P20 | 25 | Bachelors Psychology | Govt officer (full time job) Ministry of Social Affairs | Phnom Penh | Married 2 months (Husband was boyfriend for 4–5 years) | Husband sometimes uses withdrawal method; she also uses calendar method |
| P21 | 24 | Bachelors Information Technology | Disability Action Council (Disability services officer) | Phnom Penh | Married 2 years (Husband was boyfriend) | Oral contraception pills |
| P22 | 23 | Bachelors (TESOL) | English teacher | Siem Reap | Married 1 month (Husband was boyfriend for 4 years) | Initially, calendar method for a few months, then withdrawal method |
| P23 | 22 | Year 5 | Garment factory worker | Phnom Penh | Widow Engaged now (sexually active with partner) | Initially, calendar method for a few months, then withdrawal method |
| P24 | 20 | Year 10 | Shop worker | Phnom Penh | Boyfriend and is sexually active Sexual debut at 19 years | Partner using withdrawal method |
| P25 | 21 | Year 12 diploma community college | Works in a family owned business and | Phnom Penh | Single (not sexually active) | - |
| P26 | 25 | Masters (USA) on scholarship | Product specialist at a telecom company | Phnom Penh | Sexually active (she has a partner for the past 2 years), Sexual debut at 21 years with 1st boyfriend. Second partner since age 22 | Partner using condoms She is interested in subdermal implant in future. |
| P27 | 25 | Bachelors (overseas) Currently doing Masters in Business administration | Program manager | Phnom Penh | Sexually active; she has had two boyfriends, the last one 6 months ago. | Second (current partner) using withdrawal method First partner used condoms Interested in subdermal implant in future and can not find any subdermal implants at the pharmacy |
| P28 | 18 | Year 2 | Helper in a beauty salon in Boeng Kang Kong 2 | Phnom Penh | Sexually active, and had sexual debut 3–4 months ago | Partner using withdrawal method |
| P29 | 19 | Year 5 | Cold drinks cart seller | Phnom Penh | Sexually active and has a boyfriend | Partner using withdrawal method |
| P30 | 19 | 1st year university | Student | Phnom Penh | Sexually active and she has a boyfriend | Initially, calendar method for few months, then withdrawal method used, then condom use and is interested in subdermal implant |
What we already know
|
What this paper adds
|
What are the policy implications?
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rizvi, F.; Williams, J.W.; Bowe, S.J.; Hoban, E. Misconceptions and Unmet Need for Modern Contraception among Cambodian Females: A Mix Methods Study. Sexes 2020, 1, 41-59. https://doi.org/10.3390/sexes1010005
Rizvi F, Williams JW, Bowe SJ, Hoban E. Misconceptions and Unmet Need for Modern Contraception among Cambodian Females: A Mix Methods Study. Sexes. 2020; 1(1):41-59. https://doi.org/10.3390/sexes1010005
Chicago/Turabian StyleRizvi, Farwa, Joanne W. Williams, Steven J. Bowe, and Elizabeth Hoban. 2020. "Misconceptions and Unmet Need for Modern Contraception among Cambodian Females: A Mix Methods Study" Sexes 1, no. 1: 41-59. https://doi.org/10.3390/sexes1010005
APA StyleRizvi, F., Williams, J. W., Bowe, S. J., & Hoban, E. (2020). Misconceptions and Unmet Need for Modern Contraception among Cambodian Females: A Mix Methods Study. Sexes, 1(1), 41-59. https://doi.org/10.3390/sexes1010005