
Reference Gene Validation for RT–qPCR in PBMCs from Asthmatic Patients with or without Obesity

 , ,
, ,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Control Subjects
2.2. Blood Collection and PBMCs Isolation
2.3. Cell Culture Conditions
2.4. RNA Extraction and cDNA Synthesis
2.5. Real-Time qPCR
2.6. Statistical Analysis
3. Results
3.1. Quantification Cycle (Cq) Characterization of Candidate RGs
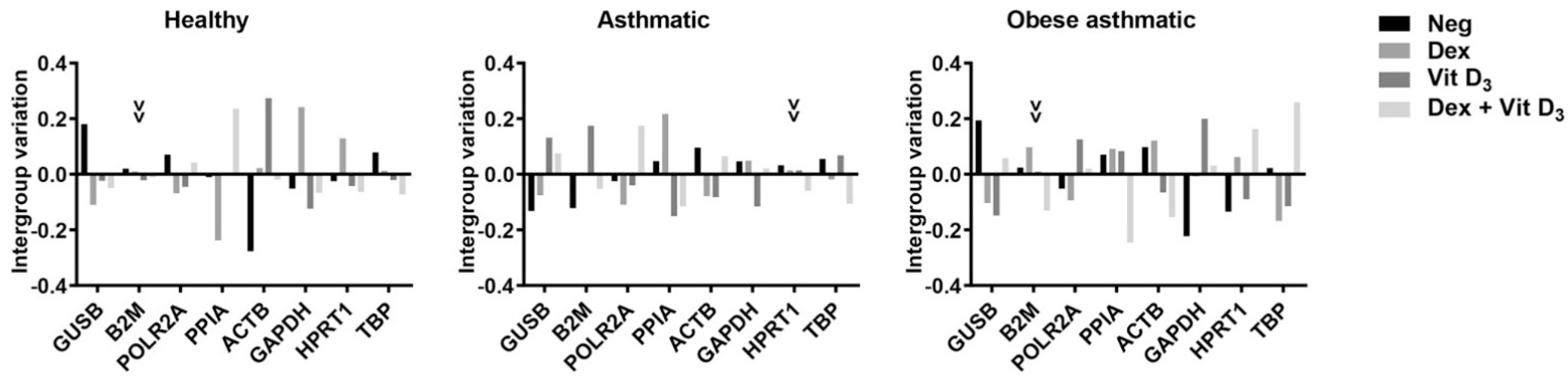
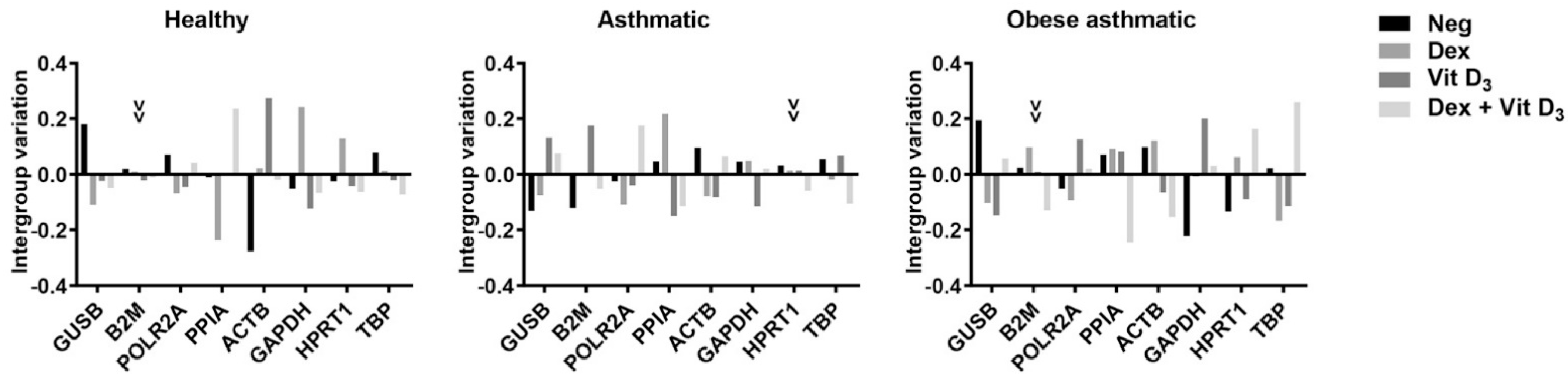
3.2. Influence of Experimental Conditions
3.3. Analyses of Gene Expression Stability
3.3.1. BestKeeper Analysis
3.3.2. ΔCt Analysis
3.3.3. geNorm Analysis
3.3.4. NormFinder
3.4. Comprehensive Ranking
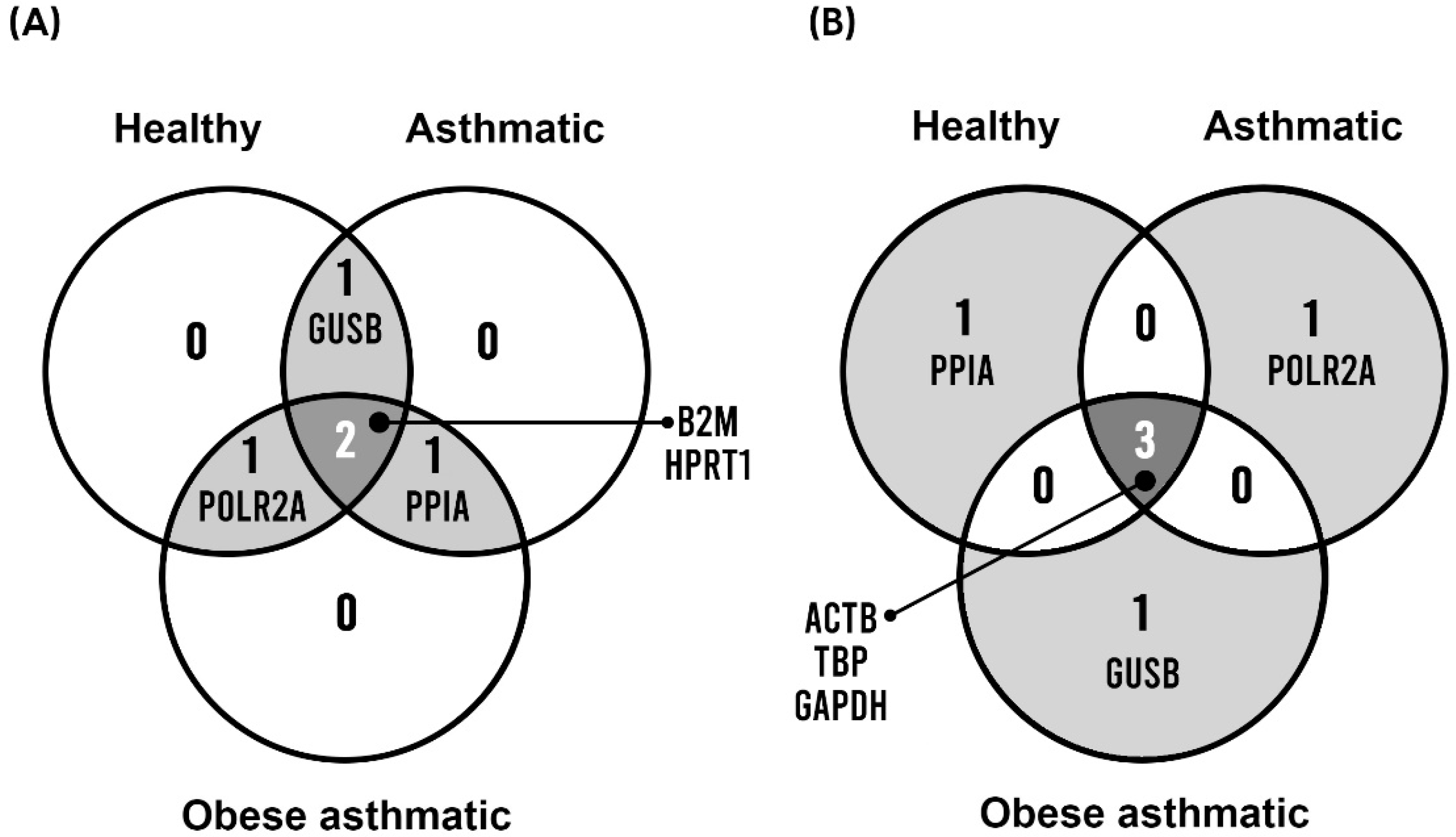
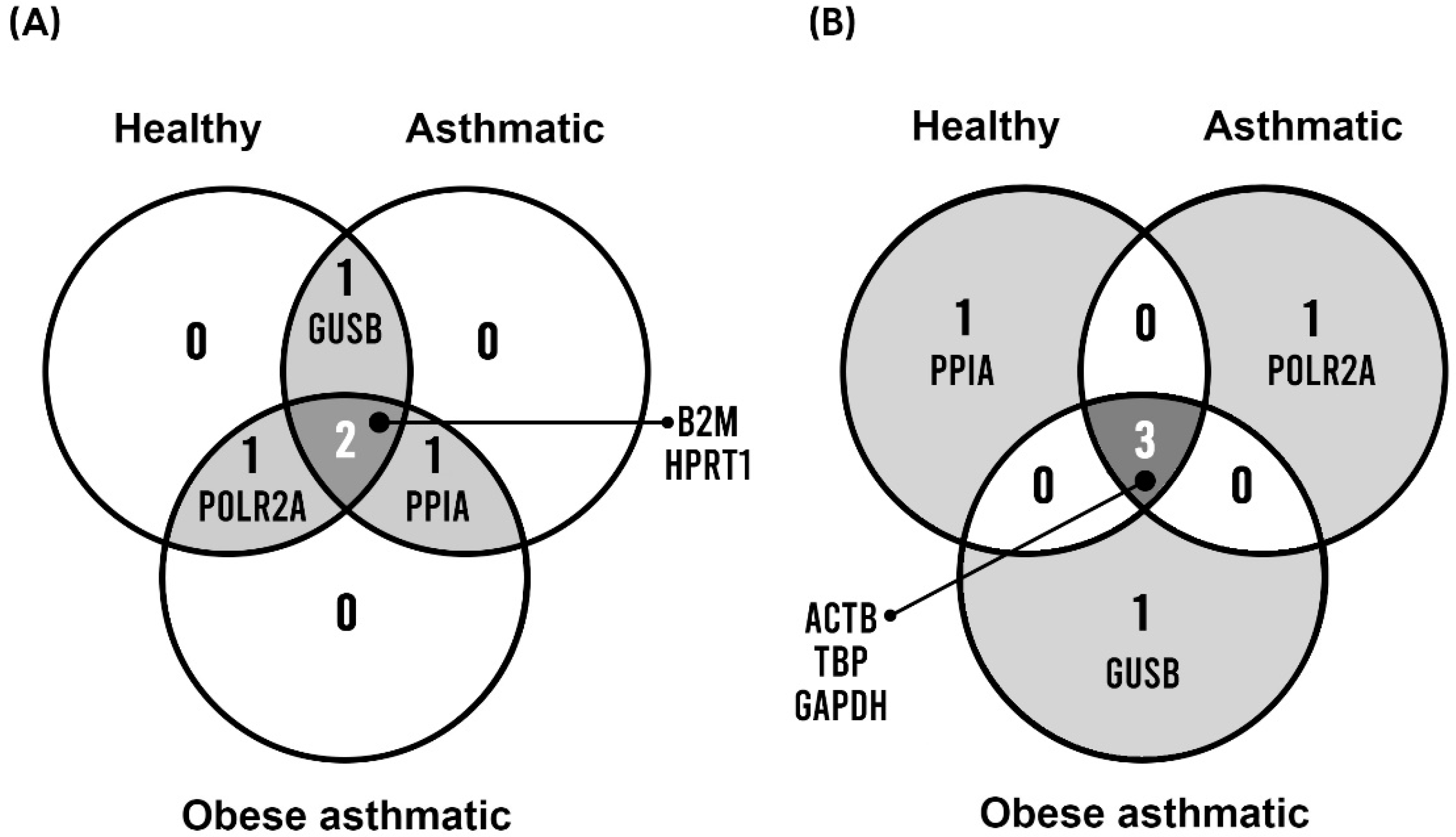
3.5. Identification of the Best and Worst Shared Scored Genes
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Global Initiative for Asthma. 2021 GINA Report, Global Strategy for Asthma Management and Prevention (2021). Available online: https://ginasthma.org/ (accessed on 15 February 2022).
- Anderson, W.J.; Lipworth, B.J. Does body mass index influence responsiveness to inhaled corticosteroids in persistent asthma? Ann. Allergy Asthma Immunol. 2012, 108, 237–242. [Google Scholar] [CrossRef] [PubMed]
- Dixon, A.E.; Holguin, F.; Sood, A.; Salome, C.M.; Pratley, R.E.; Beuther, D.A.; Celedón, J.C.; Shore, S.A.; Boulet, L.P.; O’Donnell, C.; et al. An official American thoracic society workshop report: Obesity and asthma. Proc. Am. Thorac. Soc. 2010, 7, 325–335. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taylor, B.; Mannino, D.; Brown, C.; Crocker, D.; Twum-Baah, N.; Holguin, F. Body mass index and asthma severity in the National Asthma Survey. Thorax 2008, 63, 14–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sutherland, E.R.; Goleva, E.; Jackson, L.P.; Stevens, A.D.; Leung, D.Y.M. Vitamin D Levels, Lung Function, and Steroid Response in Adult Asthma. Am. J. Respir. Crit. Care Med. 2010, 181, 699–704. [Google Scholar] [CrossRef] [Green Version]
- Cassim, R.; Russell, M.A.; Lodge, C.J.; Lowe, A.J.; Koplin, J.J.; Dharmage, S.C. The role of circulating 25 hydroxyvitamin D in asthma: A systematic review. Allergy 2015, 70, 339–354. [Google Scholar] [CrossRef]
- Vo, P.; Bair-Merritt, M.; Camargo, C.A. The potential role of vitamin D in the link between obesity and asthma severity/control in children. Expert Rev. Respir. Med. 2015, 9, 309–325. [Google Scholar] [CrossRef]
- Goleva, E.; Jackson, L.P.; Gleason, M.; Leung, D.Y.M. Usefulness of PBMCs to predict clinical response to corticosteroids in asthmatic patients. J. Allergy Clin. Immunol. 2012, 129, 687–693. [Google Scholar] [CrossRef] [Green Version]
- Bustin, S.A.; Benes, V.; Garson, J.A.; Hellemans, J.; Huggett, J.; Kubista, M.; Mueller, R.; Nolan, T.; Pfaffl, M.W.; Shipley, G.L.; et al. The MIQE guidelines: Minimum information for publication of quantitative real-time PCR experiments. Clin. Chem. 2009, 55, 611–622. [Google Scholar] [CrossRef] [Green Version]
- Thellin, O.; ElMoualij, B.; Heinen, E.; Zorzi, W. A decade of improvements in quantification of gene expression and internal standard selection. Biotechnol. Adv. 2009, 27, 323–333. [Google Scholar] [CrossRef]
- Bustin, S.A. Absolute quantification of mrna using real-time reverse transcription polymerase chain reaction assays. J. Mol. Endocrinol. 2000, 25, 169–193. [Google Scholar] [CrossRef] [Green Version]
- de Jonge, H.J.M.; Fehrmann, R.S.N.; de Bont, E.S.J.M.; Hofstra, R.M.W.; Gerbens, F.; Kamps, W.A.; de Vries, E.G.E.; van der Zee, A.G.J.; te Meerman, G.J.; ter Elst, A. Evidence based selection of housekeeping genes. PLoS ONE 2007, 2, e898. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vandesompele, J.; De Preter, K.; Pattyn, F.; Poppe, B.; Van Roy, N.; De Paepe, A.; Speleman, F. Accurate normalization of real-time quantitative RT-PCR data by geometric averaging of multiple internal control genes. Genome Biol. 2002, 3, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andersen, C.L.; Jensen, J.L.; Ørntoft, T.F. Normalization of real-time quantitative reverse transcription-PCR data: A model-based variance estimation approach to identify genes suited for normalization, applied to bladder and colon cancer data sets. Cancer Res. 2004, 64, 5245–5250. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, T.; Liang, Z.A.; Sandford, A.J.; Xiong, X.Y.; Yang, Y.Y.; Ji, Y.L.; He, J.Q. Selection of Suitable Housekeeping Genes for Real-Time Quantitative PCR in CD4+ Lymphocytes from Asthmatics with or without Depression. PLoS ONE 2012, 7, e48367. [Google Scholar] [CrossRef] [PubMed]
- Schmittgen, T.D.; Zakrajsek, B.A. Effect of experimental treatmentfile on housekeeping gene expression: Validation by real-time, quantitative RT-PCR. J. Biochem. Biophys. Methods 2000, 46, 69–81. [Google Scholar] [CrossRef]
- Radonić, A.; Thulke, S.; Mackay, I.M.; Landt, O.; Siegert, W.; Nitsche, A. Guideline to reference gene selection for quantitative real-time PCR. Biochem. Biophys. Res. Commun. 2004. [Google Scholar] [CrossRef]
- Schmid, H.; Cohen, C.D.; Henger, A.; Irrgang, S.; Schlöndorff, D.; Kretzler, M. Validation of endogenous controls for gene expression analysis in microdissected human renal biopsies. Kidney Int. 2003, 64, 356–360. [Google Scholar] [CrossRef] [Green Version]
- Ledderose, C.; Heyn, J.; Limbeck, E.; Kreth, S. Selection of reliable reference genes for quantitative real-time PCR in human T cells and neutrophils. BMC Res. Notes 2011, 4, 427. [Google Scholar] [CrossRef] [Green Version]
- Pfaffl, M.W.; Tichopad, A.; Prgomet, C.; Neuvians, T.P. Determination of stable housekeeping genes, differentially regulated target genes and sample integrity: BestKeeper—Excel-based tool using pair-wise correlations. Biotechnol. Lett. 2004, 26, 509–515. [Google Scholar] [CrossRef]
- Silver, N.; Best, S.; Jiang, J.; Thein, S.L. Selection of housekeeping genes for gene expression studies in human reticulocytes using real-time PCR. BMC Mol. Biol. 2006, 7, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.; Wang, Y.; Wang, H.; Hao, X.; Wu, Y.; Guo, J. Selection of reference genes for gene expression studies in porcine whole blood and peripheral blood mononuclear cells under polyinosinic:Polycytidylic acid stimulation. Asian-Australas. J. Anim. Sci. 2014, 27, 471–478. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Müller, G.C.; Pitrez, P.M.; Lopes, R.F.M.; Souza Pires, P.; Correa, B.L.; Pillat, M.M.; Teixeira, A.L.; Jones, M.H.; Stein, R.T.; Bauer, M.E. Peripheral glucocorticoid sensitivity in children with controlled persistent asthma. Neuroimmunomodulation 2010, 18, 98–102. [Google Scholar] [CrossRef] [PubMed]
- Vazquez-Tello, A.; Halwani, R.; Hamid, Q.; Al-Muhsen, S. Glucocorticoid receptor-beta up-regulation and steroid resistance induction by IL-17 and IL-23 cytokine stimulation in peripheral mononuclear cells. J. Clin. Immunol. 2013, 33, 466–478. [Google Scholar] [CrossRef] [PubMed]
- Oturai, D.B.; Søndergaard, H.B.; Börnsen, L.; Sellebjerg, F.; Romme Christensen, J. Identification of Suitable Reference Genes for Peripheral Blood Mononuclear Cell Subset Studies in Multiple Sclerosis. Scand. J. Immunol. 2016, 83, 72–80. [Google Scholar] [CrossRef] [Green Version]
- Barnes, M.G.; Grom, A.A.; Griffin, T.A.; Colbert, R.A.; Thompson, S.D. Gene expression profiles from peripheral blood mononuclear cells are sensitive to short processing delays. Biopreserv. Biobank. 2010, 8, 153–162. [Google Scholar] [CrossRef]
- Usarek, E.; Barańczyk-Kuźma, A.; Kaźmierczak, B.; Gajewska, B.; Kuźma-Kozakiewicz, M. Validation of qPCR reference genes in lymphocytes from patients with amyotrophic lateral sclerosis. PLoS ONE 2017, 12, e0174317. [Google Scholar] [CrossRef]
- Nakayama, T.; Okada, N.; Yoshikawa, M.; Asaka, D.; Kuboki, A.; Kojima, H.; Tanaka, Y.; Haruna, S.I. Assessment of suitable reference genes for RT-qPCR studies in chronic rhinosinusitis. Sci. Rep. 2018, 8, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Bas, A.; Forsberg, G.; Hammarström, S.; Hammarström, M.L. Utility of the housekeeping genes 18S rRNA, β-actin and glyceraldehyde-3-phosphate-dehydrogenase for normalization in real-time quantitative reverse transcriptase-polymerase chain reaction analysis of gene expression in human T lymphocytes. Scand. J. Immunol. 2004, 59, 566–573. [Google Scholar] [CrossRef]
- Glare, E.M.; Divjak, M.; Bailey, M.J. β-Actin and GAPDH housekeeping gene expression in asthmatic airways is variable and not suitable for normalising mRNA levels. Thorax 2002, 57, 765–770. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
{kind=link}
| Group | Reference Genes | Stability Value | Comprehensive Ranking | ||||
|---|---|---|---|---|---|---|---|
| BestKeeper | ΔCt | geNorm | NormFinder | ||||
| SD | r | SD | M | S | |||
| Healthy | HPRT1 | 0.50 | 0.89 | 0.58 | 0.58 | 0.08 | 1.32 |
| GUSB | 0.45 | 0.76 | 0.63 | 0.63 | 0.11 | 2.06 | |
| B2M | 0.54 | 0.83 | 0.63 | 0.63 | 0.11 | 2.63 | |
| POLR2A | 0.47 | 0.75 | 0.64 | 0.64 | 0.12 | 3.36 | |
| ACTB | 0.55 | 0.76 | 0.69 | 0.69 | 0.15 | 5.48 | |
| TBP | 0.75 | 0.89 | 0.68 | 0.68 | 0.16 | 5.69 | |
| PPIA | 0.67 | 0.74 | 0.78 | 0.78 | 0.19 | 6.74 | |
| GAPDH | 0.85 | 0.82 | 0.87 | 0.87 | 0.19 | 8.00 | |
| Asthmatic | GUSB | 0.76 | 0.91 | 0.67 | 0.67 | 0.09 | 1.32 |
| HPRT1 | 0.80 | 0.91 | 0.70 | 0.70 | 0.13 | 3.16 | |
| PPIA | 0.75 | 0.90 | 0.72 | 0.72 | 0.22 | 3.46 | |
| B2M | 0.64 | 0.69 | 0.91 | 0.91 | 0.13 | 3.72 | |
| TBP | 0.78 | 0.84 | 0.76 | 0.76 | 0.13 | 4.47 | |
| POLR2A | 0.82 | 0.89 | 0.72 | 0.73 | 0.15 | 4.90 | |
| GAPDH | 1.00 | 0.92 | 0.81 | 0.81 | 0.12 | 5.29 | |
| ACTB | 0.84 | 0.91 | 0.77 | 0.77 | 0.18 | 6.48 | |
| Obese Asthmatic | B2M | 0.59 | 0.91 | 0.61 | 0.61 | 0.10 | 1.19 |
| PPIA | 0.57 | 0.86 | 0.66 | 0.66 | 0.15 | 2.11 | |
| POLR2A | 0.60 | 0.86 | 0.66 | 0.66 | 0.15 | 3.57 | |
| HPRT1 | 0.75 | 0.92 | 0.66 | 0.66 | 0.13 | 3.87 | |
| TBP | 0.65 | 0.85 | 0.70 | 0.70 | 0.13 | 4.16 | |
| ACTB | 0.73 | 0.91 | 0.70 | 0.70 | 0.14 | 5.42 | |
| GUSB | 0.71 | 0.79 | 0.76 | 0.76 | 0.20 | 6.44 | |
| GAPDH | 0.77 | 0.82 | 0.79 | 0.79 | 0.20 | 8.00 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bantulà, M.; Arismendi, E.; Picado, C.; Mullol, J.; Roca-Ferrer, J.; Tubita, V. Reference Gene Validation for RT–qPCR in PBMCs from Asthmatic Patients with or without Obesity. Methods Protoc. 2022, 5, 35. https://doi.org/10.3390/mps5030035
Bantulà M, Arismendi E, Picado C, Mullol J, Roca-Ferrer J, Tubita V. Reference Gene Validation for RT–qPCR in PBMCs from Asthmatic Patients with or without Obesity. Methods and Protocols. 2022; 5(3):35. https://doi.org/10.3390/mps5030035
Chicago/Turabian StyleBantulà, Marina, Ebymar Arismendi, César Picado, Joaquim Mullol, Jordi Roca-Ferrer, and Valeria Tubita. 2022. "Reference Gene Validation for RT–qPCR in PBMCs from Asthmatic Patients with or without Obesity" Methods and Protocols 5, no. 3: 35. https://doi.org/10.3390/mps5030035
APA StyleBantulà, M., Arismendi, E., Picado, C., Mullol, J., Roca-Ferrer, J., & Tubita, V. (2022). Reference Gene Validation for RT–qPCR in PBMCs from Asthmatic Patients with or without Obesity. Methods and Protocols, 5(3), 35. https://doi.org/10.3390/mps5030035