
Effect of the Intake of Brown Rice for Six Months on the Cognitive Function in Healthy Elderly Persons: A Study Protocol for a Pilot, Non-Randomized Controlled Trial


Abstract
:1. Introduction
2. Methods and Analysis
2.1. Study Design and Objectives
2.2. Criteria for Inclusion/Exclusion
2.3. Rice Used for the Intervention
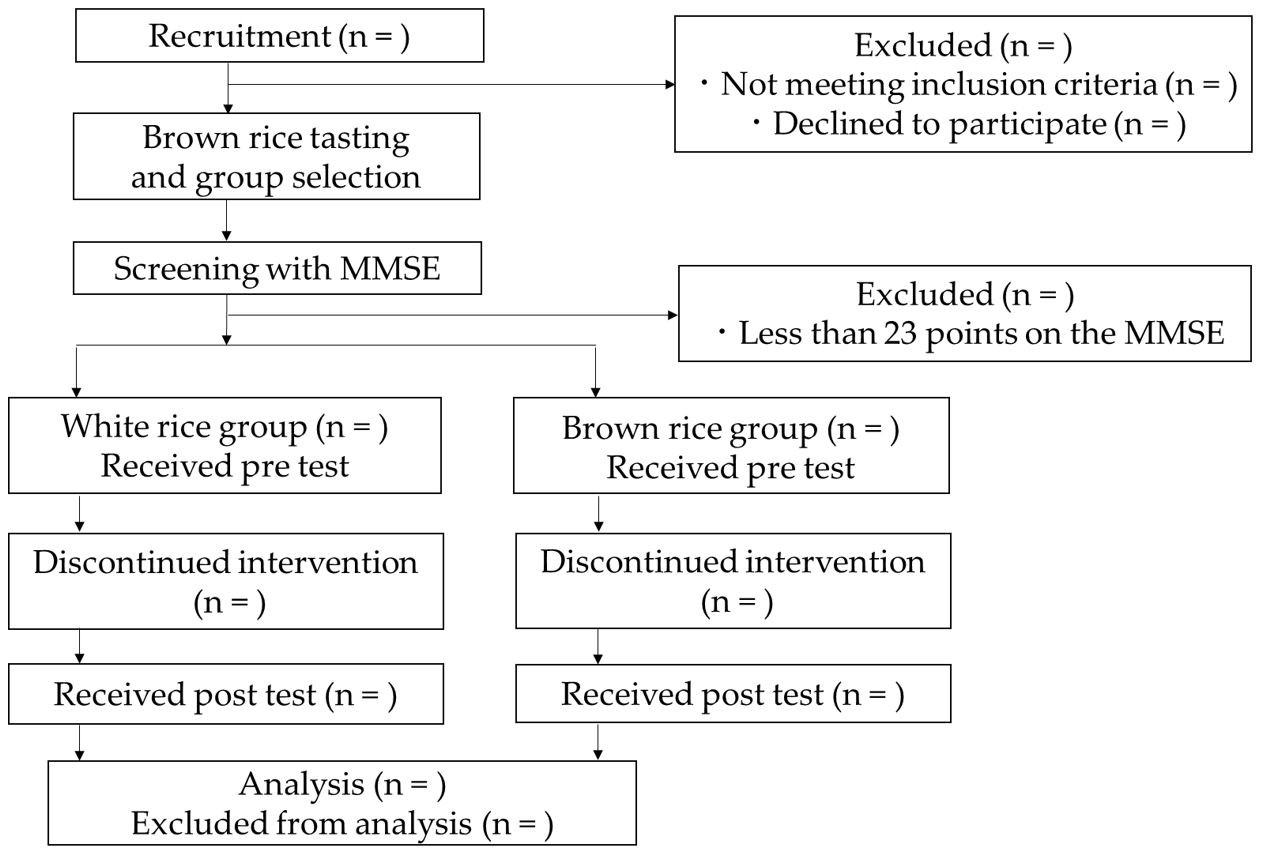
3. Protocol
4. Measurement Items
4.1. Mini-Mental State Examination (MMSE)
4.2. Frontal Assessment Battery (FAB)
4.3. S-A Creativity Test
4.4. Conversational Assessment of Neurocognitive Dysfunction (CANDy)
4.5. General Health Questionnaire 12 (GHQ12)
4.6. Visual Analog Scale (VAS) on Happiness, Health, and Sleep
4.7. Fingertip Volume Pulse Wave
4.8. Questionnaire on Specific Health Examination (QSHE) and Dietary Variety Score (DVS)
5. Sample Size
6. Statistical Considerations
7. Discussions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Ciulu, M.; Cádiz-Gurrea, M.L.; Segura-Carretero, A. Extraction and analysis of phenolic compounds in rice: A review. Molecules 2018, 23, 2890. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bandumula, N. Rice production in Asia: Key to global food security. Proc. Natl. Acad. Sci. USA 2018, 88, 1323–1328. [Google Scholar] [CrossRef]
- Monika, B.D. Food Security in Asia: Challenges, Policies and Implications; International Institute for Strategic Studies (IISS): London, UK, 2013. [Google Scholar]
- Liu, Q.; Zhou, X.; Sun, Z. Application of silicon fertilizer affects nutritional quality of rice. Chil. J. Agric. Res. 2017, 77, 163–170. [Google Scholar] [CrossRef] [Green Version]
- Mirtaleb, S.H.; Niknejad, Y.; Fallah, H. Foliar spray of amino acids and potassic fertilizer improves the nutritional quality of rice. J. Plant. Nutr. 2021, 2029–2041. [Google Scholar] [CrossRef]
- Kozuka, C.; Sunagawa, S.; Ueda, R.; Higa, M.; Tanaka, H.; Shimizu-Okabe, C.; Ishiuchi, S.; Takayama, C.; Matsushita, M.; Tsutsui, M.; et al. γ-Oryzanol protects pancreatic β-cells against endoplasmic reticulum stress in male mice. Endocrinology 2015, 156, 1242–1250. [Google Scholar] [CrossRef] [Green Version]
- Wang, L.; Lin, Q.; Yang, T.; Liang, Y.; Nie, Y.; Luo, Y.; Shen, J.; Fu, X.; Tang, Y.; Luo, F. Oryzanol modifies high fat diet-induced obesity, liver gene expression profile, and inflammation response in mice. J. Agric. Food Chem. 2017, 65, 8374–8385. [Google Scholar] [CrossRef]
- Kozuka, C.; Sunagawa, S.; Ueda, R.; Higa, M.; Ohshiro, Y.; Tanaka, H.; Shimizu-Okabe, C.; Takayama, C.; Matsushita, M.; Tsutsui, M.; et al. A novel insulinotropic mechanism of whole grain-derived γ-oryzanol via the suppression of local dopamine D2 receptor signalling in mouse islet. Br. J. Pharmacol. 2015, 172, 4519–4534. [Google Scholar] [CrossRef] [Green Version]
- Kozuka, C.; Yabiku, K.; Sunagawa, S.; Ueda, R.; Taira, S.; Ohshiro, H.; Ikema, T.; Yamakawa, K.; Higa, M.; Tanaka, H.; et al. Brown rice and its component, γ-oryzanol, attenuate the preference for high-fat diet by decreasing hypothalamic endoplasmic reticulum stress in mice. Diabetes 2012, 61, 3084–3093. [Google Scholar] [CrossRef] [Green Version]
- Masuzaki, H.; Kozuka, C.; Okamoto, S.; Yonamine, M.; Tanaka, H.; Shimabukuro, M. Brown rice-specific γ-oryzanol as a promising prophylactic avenue to protect against diabetes mellitus and obesity in humans. J. Diabetes Investig. 2019, 10, 18–25. [Google Scholar] [CrossRef] [Green Version]
- Kondo, K.; Morino, K.; Nishio, Y.; Ishikado, A.; Arima, H.; Nakao, K.; Nakagawa, F.; Nikami, F.; Sekine, O.; Nemoto, K.; et al. Fiber-rich diet with brown rice improves endothelial function in type 2 diabetes mellitus: A randomized controlled trial. PLoS ONE 2017, 12, e0179869. [Google Scholar] [CrossRef]
- Shimabukuro, M.; Higa, M.; Kinjo, R.; Yamakawa, K.; Tanaka, H.; Kozuka, C.; Yabiku, K.; Taira, S.; Sata, M.; Masuzaki, H. Effects of the brown rice diet on visceral obesity and endothelial function: The BRAVO study. Br. J. Nutr. 2014, 111, 310–320. [Google Scholar] [CrossRef] [Green Version]
- Mellen, P.B.; Walsh, T.F.; Herrington, D.M. Whole grain intake and cardiovascular disease: A meta-analysis. Nutr. Metab. Cardiovasc. Dis. 2008, 18, 283–290. [Google Scholar] [CrossRef]
- Shao, Y.; Bao, J. Polyphenols in whole rice grain: Genetic diversity and health benefits. Food Chem. 2015, 180, 86–97. [Google Scholar] [CrossRef]
- Kesse-Guyot, E.; Fezeu, L.; Andreeva, V.A.; Touvier, M.; Scalbert, A.; Hercberg, S.; Galan, P. Total and specific polyphenol intakes in midlife are associated with cognitive function measured 13 years later. J. Nutr. 2012, 142, 76–83. [Google Scholar] [CrossRef]
- Lamport, D.; Dye, L.; Wightman, J.D.; Lawton, C.L. The effects of flavonoid and other polyphenol consumption on cognitive performance: A systematic research review of human experimental and epidemiological studies. Nutr. Aging 2012, 1, 5–25. [Google Scholar] [CrossRef] [Green Version]
- Keane, K. Polyphenol Pharmacokinetics and Cardiovascular, Cognitive and Exercise Pharmacodynamics Following Montmorency Tart Cherry Intake in Humans. Ph.D. Thesis, Northumbria University, Newcastle upon Tyne, UK, 2017; p. 231. Available online: http://nrl.northumbria.ac.uk/31599 (accessed on 2 August 2021).
- Godos, J.; Caraci, F.; Castellano, S.; Currenti, W.; Galvano, F.; Ferri, R.; Grosso, G. Association between dietary flavonoids Intake and cognitive function in an Italian cohort. Biomolecules 2020, 10, 1300. [Google Scholar] [CrossRef]
- Godos, J.; Caraci, F.; Micek, A.; Castellano, S.; D’Amico, E.; Paladino, N.; Ferri, R.; Galvano, F.; Grosso, G. Dietary phenolic acids and their major food sources are associated with cognitive status in older Italian adults. Antioxidants 2021, 10, 700. [Google Scholar] [CrossRef]
- Goni, L.; Fernández-Matarrubia, M.; Romanos-Nanclares, A.; Razquin, C.; Ruiz-Canela, M.; Martínez-González, M.Á.; Toledo, E. Polyphenol intake and cognitive decline in the Seguimiento Universidad de Navarra (SUN) Project. Br. J. Nutr. 2021, 126, 43–52. [Google Scholar] [CrossRef]
- Surh, Y.J.; Chun, K.S.; Cha, H.H.; Han, S.S.; Keum, Y.S.; Park, K.K.; Lee, S.S. Molecular mechanisms underlying chemopreventive activities of anti-inflammatory phytochemicals: Down-regulation of COX-2 and iNOS through suppression of NF-κB activation. Mutat. Res.-Fund. Mol. Mech. Mutagenesis 2001, 480, 243–268. [Google Scholar] [CrossRef]
- Scott, B.C.; Butler, J.; Halliwell, B.; Aruoma, O.I. Evaluation of the antioxidant actions of ferulic acid and catechins. Free Radic. Res. Commun. 1993, 19, 241–253. [Google Scholar] [CrossRef]
- Narasimhan, A.; Chinnaiyan, M.; Karundevi, B. Ferulic acid exerts its antidiabetic effect by modulating insulin-signalling molecules in the liver of high-fat diet and fructose-induced type-2 diabetic adult male rat. Appl. Physiol. Nutr. Metab. 2015, 40, 769–781. [Google Scholar] [CrossRef] [PubMed]
- Mori, T.; Koyama, N.; Guillot-Sestier, M.V.; Tan, J.; Town, T. Ferulic acid is a nutraceutical β-secretase modulator that improves behavioral impairMent. and alzheimer-like pathology in transgenic mice. PLoS ONE 2013, 8, e55774. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fukagawa, N.K.; Ziska, L.H. Rice: Importance for global nutrition. J. Nutr. Sci. Vitam. 2019, 65, S2–S3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Swaminathan, A.; Jicha, G.A. Nutrition and prevention of Alzheimer’s dementia. Front. Aging NeuroSci. 2014, 6, 282. [Google Scholar] [CrossRef] [Green Version]
- Lourida, I.; Hannon, E.; Littlejohns, T.J.; Langa, K.M.; Hyppönen, E.; Kuzma, E.; Llewellyn, D.J. Association of lifestyle and genetic risk with incidence of dementia. JAMA 2019, 322, 430–437. [Google Scholar] [CrossRef]
- Okuda, M.; Fujita, Y.; Katsube, T.; Tabata, H.; Yoshino, K.; Hashimoto, M.; Sugimoto, H. Highly water pressurized brown rice improves cognitive dysfunction in senescence-accelerated mouse prone 8 and reduces amyloid beta in the brain. BMC Complement. Altern. Med. 2018, 18, 110. [Google Scholar] [CrossRef]
- Uenobe, M.; Saika, T.; Waku, N.; Ohno, M.; Inagawa, H. Efficacy of continuous ingestion of dewaxed brown rice on the cognitive functions of the residents of elderly welfare facilities: A pilot test using crossover trial. Food Sci. Nutr. 2019, 7, 3520–3526. [Google Scholar] [CrossRef] [Green Version]
- Kuroda, Y.; Matsuzaki, K.; Wakatsuki, H.; Shido, O.; Harauma, A.; Moriguchi, T.; Sugimoto, H.; Yamaguchi, S.; Yoshino, O.; Hashimoto, M. Influence of ultra-high hydrostatic pressurizing brown rice on cognitive functions and mental health of elderly Japanese individuals: A 2-year randomized and controlled trial. J. Nutr. Sci. Vitaminol. 2019, 65, S80–S87. [Google Scholar] [CrossRef] [Green Version]
- Saika, K.; Yonei, Y. Reduction of medical expenses by ingesting processed brown rice (sub-aleurone layer residual rinse-free rice, dewaxed brown rice). Glycative Stress Res. 2021, 8, 115–122. [Google Scholar] [CrossRef]
- Sun, Q.; Spiegelman, D.; van Dam, R.M.; Holmes, M.D.; Malik, V.S.; Willett, W.C.; Hu, F.B. White rice, brown rice, and risk of type 2 diabetes in US men and women. Arch. Intern. Med. 2010, 170, 961–969. [Google Scholar] [CrossRef]
- Villegas, R.; Liu, S.; Gao, Y.T.; Yang, G.; Li, H.; Zheng, W.; Shu, X.O. Prospective study of dietary carbohydrates, glycemic index, glycemic load, and incidence of type 2 diabetes mellitus in middle-aged Chinese women. Arch. Intern. Med. 2007, 167, 2310–2316. [Google Scholar] [CrossRef] [Green Version]
- Okubo, H.; Inagaki, H.; Gondo, Y.; Kamide, K.; Ikebe, K.; Masui, Y.; Arai, Y.; Ishizaki, T.; Sasaki, S.; Nakagawa, T.; et al. Association between dietary patterns and cognitive function among 70-year-old Japanese elderly: A cross-sectional analysis of the SONIC study. Nutr. J. 2017, 16, 56. [Google Scholar] [CrossRef] [Green Version]
- Koga, M.; Toyomaki, A.; Miyazaki, A.; Nakai, Y.; Yamaguchi, A.; Kubo, C.; Suzuki, J.; Ohkubo, I.; Shimizu, M.; Musashi, M.; et al. Mediators of the effects of rice intake on health in individuals consuming a traditional Japanese diet centered on rice. PLoS ONE 2017, 12, e0185816. [Google Scholar] [CrossRef] [Green Version]
- Sharif, M.K.; Butt, M.S.; Anjum, F.M.; Khan, S.H. Rice bran: A novel functional ingredient. Crit. Rev. Food Sci. Nutr. 2014, 54, 807–816. [Google Scholar] [CrossRef]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Faxen-Irving, G.; Andren-Olsson, B.; Af Geijerstam, A.; Basun, H.; Cederholm, T. The effect of nutritional intervention in elderly subjects residing in group-living for the demented. Eur. J. Clin. Nutr. 2002, 56, 221–227. [Google Scholar] [CrossRef]
- Salva, A.; Andrieu, S.; Fernandez, E.; Schiffrin, E.J.; Moulin, J.; Decarli, B.; Rojano-I-Luque, X.; Guigoz, Y.; Vellas, B.; The Nutrialz Group. Health and nutrition promotion program for patients with dementia (NutriAlz): Cluster randomized trial. J. Nutr. Health Aging 2011, 15, 822–830. [Google Scholar] [CrossRef]
- Dubois, B.; Slachevsky, A.; Litvan, I.; Pillon, B. The FAB: A Frontal assessment battery at bedside. Neurology 2000, 55, 1621–1626. [Google Scholar] [CrossRef] [Green Version]
- Guilford, J.P. Creativity. Am. Psychol. 1950, 5, 444–454. [Google Scholar] [CrossRef]
- Goldberg, D.; Williams, P. A Users Guide to the General Health Questionnaire; nferNelson: London, UK, 1988. [Google Scholar]
- Oba, H.; Sato, S.; Kazui, H.; Nitta, Y.; Nashitani, T.; Kamiyama, A. Conversational assessment of cognitive dysfunction among residents living in long-term care facilities. Int. Psychogeriatr. 2018, 30, 87–94. [Google Scholar] [CrossRef] [Green Version]
- Abete, P.; Della-Morte, D.; Gargiulo, G.; Basile, C.; Langellotto, A.; Galizia, G.; Testa, G.; Canonico, V.; Bonaduce, D.; Cacciatore, F. Cognitive impairMent. and cardiovascular diseases in the elderly. A heart–brain continuum hypothesis. Aging Res. Rev. 2014, 18, 41–52. [Google Scholar] [CrossRef]
- Foltynie, T.; Brayne, C.E.; Robbins, T.W.; Barker, R.A. The cognitive ability of an incident cohort of Parkinson’s patients in the UK. The CamPaIGN study. Brain 2004, 127, 550–560. [Google Scholar] [CrossRef] [Green Version]
- Varadaraj, V.; Munoz, B.; Deal, J.A.; An, Y.; Albert, M.S.; Resnick, S.M.; Ferrucci, L.; Swenor, B.K. Association of vision impairMent. with cognitive decline across multiple domains in older adults. JAMA Netw. Open 2021, 4, e2117416. [Google Scholar] [CrossRef]
- Dahl, A.; Hassing, L.B.; Fransson, E.; Berg, S.; Gatz, M.; Reynolds, C.A.; Pedersen, N.L. Being overweight in midlife is associated with lower cognitive ability and steeper cognitive decline in late life. J. Gerontol. A Biol. Sci. Med. Sci. 2010, 65, 57–62. [Google Scholar] [CrossRef] [Green Version]
- Bherer, L.; Erickson, K.I.; Liu-Ambrose, T. A review of the effects of physical activity and exercise on cognitive and brain functions in older adults. J. Aging Res. 2013, 2013, 657508. [Google Scholar] [CrossRef] [Green Version]
- Stubbs, B.; Chen, L.J.; Chang, C.Y.; Sun, W.J.; Ku, P.W. Accelerometer-assessed light physical activity is protective of future cognitive ability: A longitudinal study among community dwelling older adults. Exp. Gerontol. 2017, 91, 104–109. [Google Scholar] [CrossRef]
- Wayne, P.M.; Walsh, J.N.; Taylor-Piliae, R.E.; Wells, R.E.; Papp, K.V.; Donovan, N.J.; Yeh, G.Y. Effect of Tai Chi on cognitive performance in older adults: Systematic review and meta-Analysis. J. Am. Geriatr. Soc. 2014, 62, 25–39. [Google Scholar] [CrossRef]
- Yaffe, K.; Falvey, C.M.; Hoang, T. Connections between sleep and cognition in older adults. Lancet Neurol. 2014, 13, 1017–1028. [Google Scholar] [CrossRef]
- Féart, C.; Samieri, C.; Barberger-Gateau, P. Mediterranean diet and cognitive function in older adults. Curr. Opin. Clin. Nutr. Metab. Care 2010, 13, 14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shatenstein, B.; Ferland, G.; Belleville, S.; Gray-Donald, K.; Kergoat, M.J.; Morais, J.; Gaudreau, P.; Payette, H.; Greenwood, C. Diet quality and cognition among older adults from the NuAge study. Exp. Gerontol. 2012, 47, 353–360. [Google Scholar] [CrossRef]
- Akbari, E.; Asemi, Z.; Daneshvar Kakhaki, R.; Bahmani, F.; Kouchaki, E.; Tamtaji, O.R.; Hamidi, G.A.; Salami, M. Effect of probiotic supplementation on cognitive function and metabolic status in Alzheimer’s disease: A randomized, double-blind and controlled trial. Front. Aging NeuroSci. 2016, 8, 256. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sabia, S.; Elbaz, A.; Dugravot, A.; Head, J.; Shipley, M.; Hagger-Johnson, G.; Kivimaki, M.; Singh-Manoux, A. Impact of smoking on cognitive decline in early old age: The Whitehall II cohort study. Arch. Gen. Psychiatry 2012, 69, 627–635. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gross, A.L.; Rebok, G.W.; Ford, D.E.; Chu, A.Y.; Gallo, J.J.; Liang, K.Y.; Meoni, L.A.; Shihab, H.M.; Wang, N.Y.; Klag, M.J. Alcohol consumption and domain-specific cognitive function in older adults: Longitudinal data from the Johns Hopkins Precursors Study. J. Gerontol. B Psychol. Sci. Soc. Sci. 2011, 66, 39–47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zanjani, F.; Downer, B.G.; Kruger, T.M.; Willis, S.L.; Schaie, K.W. Alcohol effects on cognitive change in middle-aged and older adults. Aging Ment. Health 2013, 17, 12–23. [Google Scholar] [CrossRef] [Green Version]
- Corley, J.; Jia, X.; Kyle, J.A.; Gow, A.J.; Brett, C.E.; Starr, J.M.; McNeill, G.; Deary, I.J. Caffeine consumption and cognitive function at age 70: The Lothian Birth Cohort 1936 study. Psychosom. Med. 2010, 72, 206–214. [Google Scholar] [CrossRef] [Green Version]
- Ailshire, J.A.; Crimmins, E.M. Fine particulate matter air pollution and cognitive function among older US adults. Am. J. Epidemiol. 2014, 180, 359–366. [Google Scholar] [CrossRef] [Green Version]
- Tsakos, G.; Watt, R.G.; Rouxel, P.L.; de Oliveira, C.; Demakakos, P. Tooth loss associated with physical and cognitive decline in older adults. J. Am. Geriatr. Soc. 2015, 63, 91–99. [Google Scholar] [CrossRef]
- Japan Medical Association. Questionnaire on Specific Health Examination. Available online: http://amda-imic.com/oldpage/amdact/PDF/eng/spe-he-ex-e.pdf (accessed on 15 September 2021).
- Kumagai, S.; Watanabe, S.; Shibata, H.; Amano, H.; Fujiwara, Y.; Shinkai, S.; Yoshida, H.; Suzuki, T.; Yukawa, H.; Yasumura, S.; et al. Effects of dietary variety on declines in high-level functional capacity in elderly people living in a community. JPN J. Public Health 2003, 50, 1117–1124. [Google Scholar]
- Cohen, S. Psychosocial models of the role of social support in the etiology of physical disease. Health Psychol. 1988, 7, 269. [Google Scholar] [CrossRef]


{kind=link}
| White Rice | Wax-Cut Brown Rice | Brown Rice | Method | |
|---|---|---|---|---|
| Protein (g) 1 | 5.1 | 5.8 | 6.1 | Combustion method |
| Lipids (g) | 0.8 | 2.6 | 2.9 | Acid decomposition method |
| Ash (g) | 0.3 | 1.1 | 1.2 | Direct ashing method |
| Carbohydrate (g) 2 | 78.5 | 75.3 | 74.8 | |
| Vitamin B1 (mg) 3 | 0.09 | 0.39 | 0.44 | High performance liquid chromatography |
| Vitamin B2 (mg) | 0.01 | 0.03 | 0.03 | High performance liquid chromatography |
| Vitamin B6 (mg) 4 | 0.058 | 0.410 | 0.517 | Microbioassay |
| Folic acid (μg) 5 | 18 | 30 | 29 | Microbioassay |
| Soluble fiber (g) | - | 0.2 | 0.2 | Enzymatic-gravimetric method |
| Insoluble fiber (g) | 0.3 | 2.3 | 2.5 | Enzymatic-gravimetric method |
| Monounsaturated fatty acid (g) | 0.14 | 0.76 | 0.90 | Gas chromatography |
| Polyunsaturated fatty acid (g) | 0.25 | 0.81 | 0.87 | Gas chromatography |
| Oryzanol (mg) | 1.2 | 30.1 | 41.4 | High performance liquid chromatography |
| Ferulic acid (mg) | 8.1 | 39 | 50 | High performance liquid chromatography |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Takano, Y.; Kokubun, K.; Saika, K.; Nishiyama, N.; Taki, Y. Effect of the Intake of Brown Rice for Six Months on the Cognitive Function in Healthy Elderly Persons: A Study Protocol for a Pilot, Non-Randomized Controlled Trial. Methods Protoc. 2021, 4, 78. https://doi.org/10.3390/mps4040078
Takano Y, Kokubun K, Saika K, Nishiyama N, Taki Y. Effect of the Intake of Brown Rice for Six Months on the Cognitive Function in Healthy Elderly Persons: A Study Protocol for a Pilot, Non-Randomized Controlled Trial. Methods and Protocols. 2021; 4(4):78. https://doi.org/10.3390/mps4040078
Chicago/Turabian StyleTakano, Yuji, Keisuke Kokubun, Keiji Saika, Naoki Nishiyama, and Yasuyuki Taki. 2021. "Effect of the Intake of Brown Rice for Six Months on the Cognitive Function in Healthy Elderly Persons: A Study Protocol for a Pilot, Non-Randomized Controlled Trial" Methods and Protocols 4, no. 4: 78. https://doi.org/10.3390/mps4040078
APA StyleTakano, Y., Kokubun, K., Saika, K., Nishiyama, N., & Taki, Y. (2021). Effect of the Intake of Brown Rice for Six Months on the Cognitive Function in Healthy Elderly Persons: A Study Protocol for a Pilot, Non-Randomized Controlled Trial. Methods and Protocols, 4(4), 78. https://doi.org/10.3390/mps4040078