
Prospective Outcomes of Injury Study 10 Years on (POIS-10): An Observational Cohort Study

 , , , and
, , , and 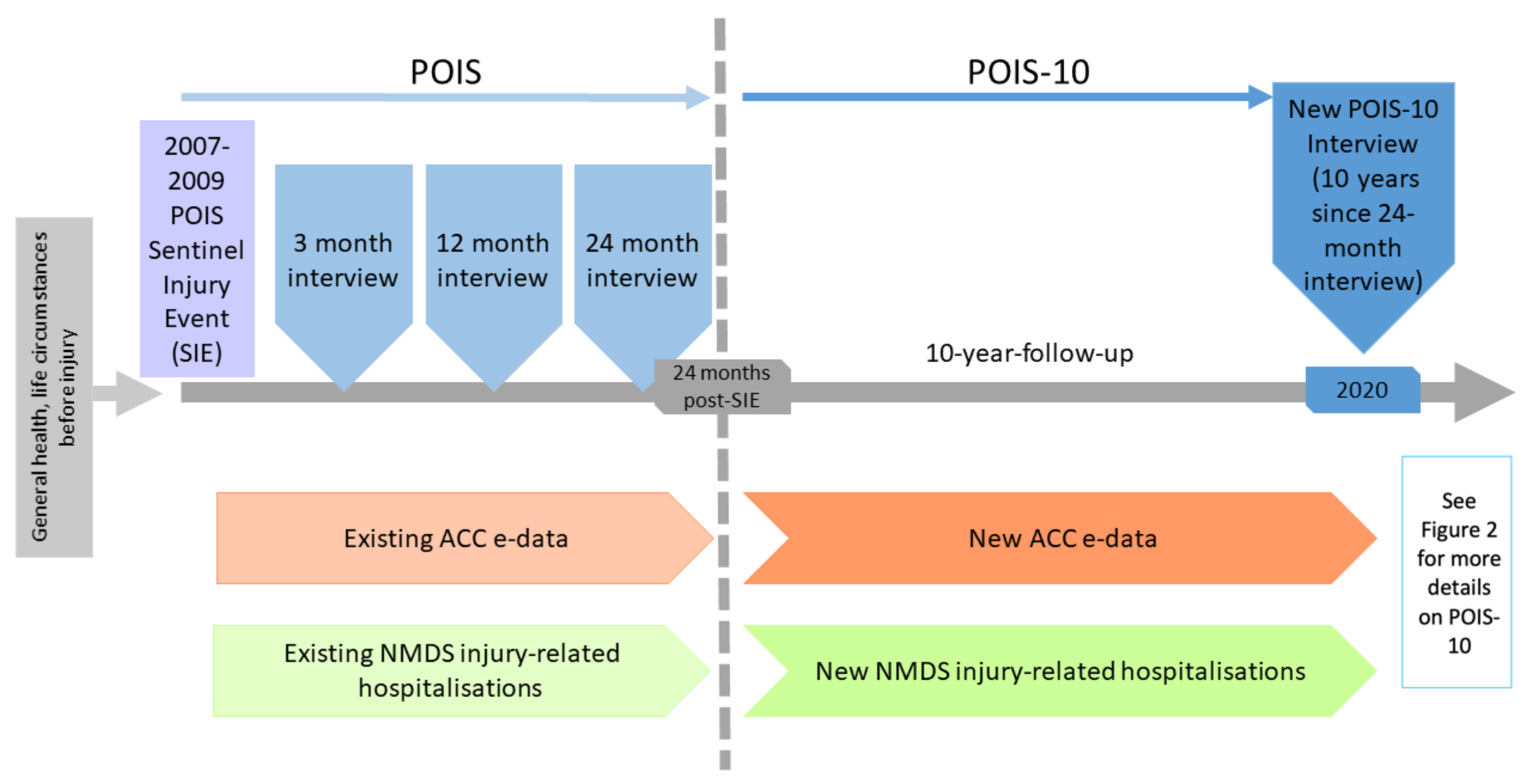{kind=link}
{kind=link}
Abstract
1. Introduction
1.1. Long-Term Outcomes of Injury Internationally
1.2. Long-Term Outcomes of Injury in New Zealand
1.3. Limitations of Existing Research
1.4. Contribution of POIS
1.5. Benefits of Additional POIS Follow-Up
1.6. POIS-10 Aims and Objectives
- Describe significant life events, employment, comorbidities, injuries and injury-related hospitalisations experienced by POIS-10 participants over the past 10 years, as people were last interviewed 24 months after the injury, which led to their recruitment to POIS (referred to as the ‘sentinel injury event’ (SIE)), including specifically for Māori;
- Investigate 12-year SIE outcomes (disability, health, and wellbeing) experienced by all POIS-10 participants and for key subgroups;
- Determine which characteristics (including baseline sociodemographic and health related, SIE related, and post-SIE related) predict outcomes for POIS-10 participants at 12 years post-SIE;
- Analyse key outcome trajectories over time;
- Develop a POIS-10 Injury Early Care (prediction) Tool (INJECT) for long-term outcomes, informed by predictors found to be of importance.
2. Experimental Design
3. Procedure
3.1. Participants
3.2. POIS-10 Recruitment
3.3. Data Collection
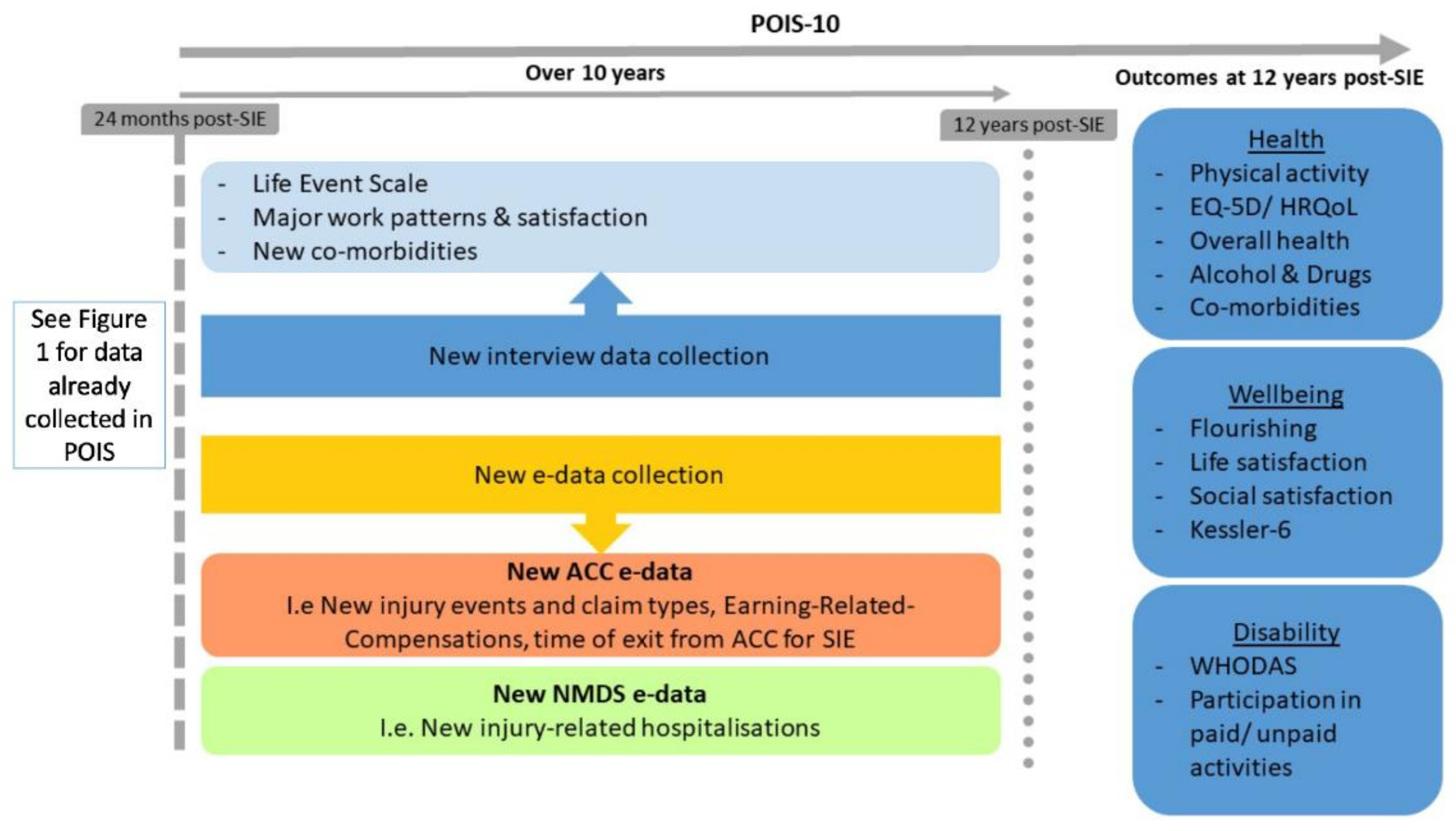
- Interviews to 10 years since last POIS data collection: Interviewer-administered computer-assisted telephone interviews (CATIs) will be conducted by a team of highly trained interviewers. Based on our earlier POIS interviews, each interview is expected to be up to 1 h in duration. Interview questions include a range of sociodemographic characteristics [50,51,52], new major life events [53], and comorbidities [54] occurring over the 10 years since the last POIS data collection (24 months post-SIE); and key disability [55], health [56,57], and wellbeing [58,59,60] outcomes at 12 years post-SIE. Interview questions will, as for POIS, align with the World Health Organization International Classification of Functioning, Disability, and Health framework [61].
- E-data between 24-month and 10-year follow-up: We will also obtain administrative e-data from ACC about new injuries occurring during the past 10 years (e.g., funded health services, support and claims processes, and earnings-related compensation) and also about ongoing claim entitlements from the original SIE. From the NMDS, we will collect administrative data about any injury-related hospitalisations occurring over the past 10 years.
3.4. Types of Data Collected
3.4.1. Sociodemographic Characteristics
3.4.2. Major Life Events and Comorbidities over the 10 years since Last Interview
3.5. Key Outcomes
3.5.1. Disability
3.5.2. Health
3.5.3. Wellbeing
3.6. Ethical Approval and Data
4. Expected Result
4.1. Analyses
4.2. Dissemination
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Haagsma, J.A.; Graetz, N.; Bolliger, I.; Naghavi, M.; Higashi, H.; Mullany, E.C.; Abera, S.F.; Abraham, J.P.; Adofo, K.; Alsharif, U.; et al. The global burden of injury: Incidence, mortality, disability-adjusted life years and time trends from the Global Burden of Disease study 2013. Inj. Prev. 2015. [Google Scholar] [CrossRef] [PubMed]
- Statistics New Zealand. Key Findings from the 2013 New Zealand Disability Survey. Available online: https://www.stats.govt.nz/assets/Uploads/Disability-survey/Disability-survey-2013/Disability-survey-2013-additional-documents/Key-findings-from-the-2013-New-Zealand-Disability-Survey-A4-brochure.pdf (accessed on 13 May 2021).
- Accident Compensation Corporation. Annual Report 2019; Accident Compensation Corporation: Wellington, New Zealand, 2019. [Google Scholar]
- Derrett, S.; Langley, J.; Hokowhitu, B.; Ameratunga, S.; Hansen, P.; Davie, G.; Wyeth, E.; Lilley, R. Prospective Outcomes of Injury Study. Inj. Prev. 2009, 15, 351. [Google Scholar] [CrossRef]
- Derrett, S.; Davie, G.; Ameratunga, S.; Wyeth, E.; Colhoun, S.; Wilson, S.; Samaranayaka, A.; Lilley, R.; Hokowhitu, B.; Hansen, P.; et al. Prospective Outcomes of Injury Study: Recruitment, and participant characteristics, health and disability status. Inj. Prev. 2011, 17, 415. [Google Scholar] [CrossRef] [PubMed]
- Wyeth, E.; Lambert, M.; Tapsell, M.; Samaranayaka, A.; Anselm, D.; Ellison, P.; Harwood, M.; Metzger, B.; Wright-Tawha, T.; Derrett, S. Understanding longer-term disability outcomes for Māori and non-Māori after hospitalisation for injury: Results from a longitudinal cohort study. Public Health 2019, 176, 118–127. [Google Scholar] [CrossRef]
- Harcombe, H.; Langley, J.; Davie, G.; Derrett, S. Functional status following injury: What recovery pathways do people follow? Injury 2015, 46, 1275–1280. [Google Scholar] [CrossRef]
- Geraerds, A.; Richardson, A.; Haagsma, J.; Derrett, S.; Polinder, S. A systematic review of studies measuring health-related quality of life of general injury populations: Update 2010–2018. Health Qual. Life Outcomes 2020, 18, 160. [Google Scholar] [CrossRef] [PubMed]
- Falkenberg, L.; Zeckey, C.; Mommsen, P.; Winkelmann, M.; Zelle, B.A.; Panzica, M.; Pape, H.-C.; Krettek, C.; Probst, C. Long-term outcome in 324 polytrauma patients: What factors are associated with posttraumatic stress disorder and depressive disorder symptoms? Eur. J. Med Res. 2017, 22, 44. [Google Scholar] [CrossRef] [PubMed]
- Spittal, M.J.; Grant, G.; O’Donnell, M.; McFarlane, A.C.; Studdert, D.M. Development of prediction models of stress and long-term disability among claimants to injury compensation systems: A cohort study. BMJ Open 2018, 8, e020803. [Google Scholar] [CrossRef] [PubMed]
- Gabbe, B.J.; Simpson, P.M.; Cameron, P.A.; Ponsford, J.; Lyons, R.A.; Collie, A.; Fitzgerald, M.; Judson, R.; Teague, W.J.; Braaf, S. Long-term health status and trajectories of seriously injured patients: A population-based longitudinal study. PLoS Med. 2017, 14, e1002322. [Google Scholar] [CrossRef]
- O’Hagan, F.T.; Ballantyne, P.J.; Vienneau, P. Mental health status of Ontario injured workers with permanent impairments. Can. J. Public Health 2012, 103, e303–e308. [Google Scholar] [CrossRef]
- Casey, R.; Ballantyne, P.J. Diagnosed chronic health conditions among injured workers with permanent impairments and the general population. J. Occup. Environ. Med. 2017, 59, 486–496. [Google Scholar] [CrossRef]
- Ballantyne, P.J.; Casey, R.; O’Hagan, F.T.; Vienneau, P. Poverty status of worker compensation claimants with permanent impairments. Crit. Public Health 2016, 26, 173–190. [Google Scholar] [CrossRef]
- Grauwmeijer, E.; Heijenbrok-Kal, M.H.; Haitsma, I.K.; Ribbers, G.M. Employment outcome ten years after moderate to severe traumatic brain injury: A prospective cohort study. J. Neurotrauma 2017, 34, 2575–2581. [Google Scholar] [CrossRef]
- Dowd, M.D.; Langley, J.; Koepsell, T.; Soderberg, R.; Rivara, F.P. Hospitalizations for injury in New Zealand: Prior injury as a risk factor for assaultive injury. Am. J. Public Health 1996, 86, 929–934. [Google Scholar] [CrossRef]
- Kieser, J.; Stephenson, S.; Liston, P.; Tong, D.; Langley, J.D. Serious facial fractures in New Zealand from 1979 to 1998. Int. J. Oral Maxillofac. Surg. 2002, 31, 206–209. [Google Scholar] [CrossRef]
- Feigin, V.L.; Theadom, A.; Barker-Collo, S.; Starkey, N.J.; McPherson, K.; Kahan, M.; Dowell, A.; Brown, P.; Parag, V.; Kydd, R. Incidence of traumatic brain injury in New Zealand: A population-based study. Lancet Neurol. 2013, 12, 53–64. [Google Scholar] [CrossRef]
- Bird, Y.; Waller, A.E.; Marshall, S.W.; Alsop, J.; Chalmers, D.; Gerrard, D. The New Zealand Rugby injury and Performance Project: V. Epidemiology of a season of rugby injury. Br. J. Sports Med. 1998, 32, 319–325. [Google Scholar] [CrossRef]
- Scuffham, P.A.; Langley, J.D. Trends in cycle injury in New Zealand under voluntary helmet use. Accid. Anal. Prev. 1997, 29, 1–9. [Google Scholar] [CrossRef]
- Fransen, M.; Wilsmore, B.; Winstanley, J.; Woodward, M.; Grunstein, R.; Ameratunga, S.; Norton, R. Shift work and work injury in the New Zealand blood donors’ health study. Occup. Environ. Med. 2006, 63, 352–358. [Google Scholar] [CrossRef]
- Humphrey, G.; Casswell, S.; Han, D.Y. Alcohol and injury among attendees at a New Zealand emergency department. N. Z. Med. J. Online 2003, 116, 1168. [Google Scholar]
- Derrett, S.; Beaver, C.; Sullivan, M.J.; Herbison, G.P.; Acland, R.; Paul, C. Traumatic and non-traumatic spinal cord impairment in New Zealand: Incidence and characteristics of people admitted to spinal units. Inj. Prev. 2012, 18, 343–346. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, M.; Paul, C.E.; Herbison, G.P.; Tamou, P.; Derrett, S.; Crawford, M. A longitudinal study of the life histories of people with spinal cord injury. Inj. Prev. 2010, 16, e3. [Google Scholar] [CrossRef] [PubMed]
- Theadom, A.; Parag, V.; Dowell, T.; McPherson, K.; Starkey, N.; Barker-Collo, S.; Jones, K.; Ameratunga, S.; Feigin, V.L.; BIONIC Research Group. Persistent problems 1 year after mild traumatic brain injury: A longitudinal population study in New Zealand. Br. J. Gen. Pr. 2016, 66, e16–e23. [Google Scholar] [CrossRef]
- Theadom, A.; Starkey, N.; Barker-Collo, S.; Jones, K.; Ameratunga, S.; Feigin, V.; BIONIC4you Research Group. Population-based cohort study of the impacts of mild traumatic brain injury in adults four years post-injury. PLoS ONE 2018, 13, e0191655. [Google Scholar] [CrossRef] [PubMed]
- Polinder, S.; Haagsma, J.A.; Toet, H.; van Beeck, E.F. Epidemiological burden of minor, major and fatal trauma in a national injury pyramid. Br. J. Surg. 2012, 99, 114–120. [Google Scholar] [CrossRef] [PubMed]
- Lyons, R.; Kendrick, D.; Towner, E.; Christie, N.; Macey, S.; Coupland, C.; Gabbe, B.; UK Burden of Injuries Study Group. Measuring the population burden of injuries—implications for global and national estimates: A multi-centre prospective UK longitudinal study. PLoS Med. 2011, 8, e1001140. [Google Scholar] [CrossRef]
- Hepp, U.; Moergeli, H.; Buchi, S.; Bruchhaus-Steinert, H.; Sensky, T.; Schnyder, U. The long-term prediction of return to work following serious accidental injuries: A follow up study. BMC Psychiatry 2011, 11, 53. [Google Scholar] [CrossRef]
- Derrett, S.; Samaranayaka, A.; Wilson, S.; Langley, J.; Ameratunga, S.; Cameron, I.D.; Lilley, R.; Wyeth, E.; Davie, G. Prevalence and predictors of sub-acute phase disability after injury among hospitalised and non-hospitalised groups: A longitudinal cohort study. PLoS ONE 2012, 7, e44909. [Google Scholar] [CrossRef]
- Derrett, S.; Wilson, S.; Samaranayaka, A.; Langley, J.; Wyeth, E.; Ameratunga, S.; Lilley, R.; Davie, G.; Mauiliu, M. Prevalence and predictors of disability 24-months after injury for hospitalised and non-hospitalised participants: Results from a longitudinal cohort study in New Zealand. PLoS ONE 2013, 8, e80194. [Google Scholar] [CrossRef]
- Wyeth, E.; Derrett, S.; Hokowhitu, B.; Hall, C.; Langley, J. Rangatiratanga and Ōritetanga: Responses to the Treaty of Waitangi in a New Zealand study. Ethn. Health 2010, 15, 303–316. [Google Scholar] [CrossRef]
- Wyeth, E.; Derrett, S.; Hokowhitu, B.; Samaranayaka, A. Indigenous injury outcomes: Life satisfaction among injured Māori in New Zealand three months after injury. Health Qual. Life Outcomes 2013, 11, 120. [Google Scholar] [CrossRef]
- Maclennan, B.; Wyeth, E.; Davie, G.; Wilson, S.; Derrett, S. Twelve-month post-injury outcomes for Māori and non-Māori: Findings from a New Zealand cohort study. Aust. N. Z. J. Public Health 2014, 38, 227–233. [Google Scholar] [CrossRef]
- Maclennan, B.; Wyeth, E.; Hokowhitu, B.; Wilson, S.; Derrett, S. Injury severity and 3-month outcomes among Māori: Results from a New Zealand prospective cohort study. N. Z. Med. J. 2013, 126, 39–49. [Google Scholar]
- Wyeth, E.H.; Maclennan, B.; Lambert, M.; Davie, G.; Lilley, R.; Derrett, S. Predictors of Work Participation for Māori Three Months After Injury. Arch. Environ. Occup. Health 2017, 73, 79–89. [Google Scholar] [CrossRef]
- Wyeth, E.H.; Samaranayaka, A.; Davie, G.; Derrett, S. Prevalence and predictors of disability for Māori 24 months after injury. Aust. N. Z. J. Public Health 2017, 41, 262–268. [Google Scholar] [CrossRef]
- Wilson, S.J.; Davie, G.; Derrett, S. Two years after injury: Prevalence and early post-injury predictors of ongoing injury-related problems. Qual. Life Res. 2017, 26, 1831–1838. [Google Scholar] [CrossRef]
- Derrett, S.; Harcombe, H.; Wyeth, E.; Davie, G.; Samaranayaka, A.; Hansen, P.; Hall, G.; Cameron, I.D.; Gabbe, B.; Powell, D.; et al. Subsequent Injury Study (SInS): Improving outcomes for injured New Zealanders. Inj. Prev. 2017, 23, 429. [Google Scholar] [CrossRef]
- Harcombe, H.; Davie, G.; Wyeth, E.; Samaranayaka, A.; Derrett, S. Injury upon injury: A prospective cohort study examining subsequent injury claims in the 24 months following a substantial injury. Inj. Prev. J. Int. Soc. Child Adolesc. Inj. Prev. 2017. [Google Scholar] [CrossRef] [PubMed]
- Davie, G.; Samaranayaka, A.; Derrett, S. The role of pre-existing comorbidity on the rate of recovery following injury: A longitudinal cohort study. PLoS ONE 2018, 13, e0193019. [Google Scholar] [CrossRef]
- Langley, J.; Lilley, R.; Samaranayaka, A.; Derrett, S. Work status and disability trajectories over 12 months after injury among workers in New Zealand. N. Z. Med. J. 2014, 127, 1–8. [Google Scholar]
- Lilley, R.; Davie, G.; Ameratunga, S.; Derrett, S. Factors predicting work status three months after injury: Results from the Prospective Outcome of Injury Study. BMJ Open 2012, 2, e000400. [Google Scholar] [CrossRef] [PubMed]
- Lilley, R.; Davie, G.; Langley, J.; Ameratunga, S.; Derrett, S. Do outcomes differ between work and non-work-related injury in a universal injury compensation system? Findings from the New Zealand Prospective Outcomes of Injury Study. BMC Public Health 2013, 13, 995. [Google Scholar] [CrossRef] [PubMed]
- Lilley, R.; Davie, G.; Derrett, S. Are the early predictors of long-term work absence following injury time dependent? Results from the Prospective Outcomes of Injury Study. BMJ Open 2017, 7, e017390. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Wilson, S.J.; Davie, G.; Harcombe, H.; Wyeth, E.H.; Cameron, I.D.; Derrett, S. Impact of further injury on participation in work and activities among those previously injured: Results from a New Zealand prospective cohort study. Qual. Life Res. 2018. [Google Scholar] [CrossRef]
- Harcombe, H.; Derrett, S.; Langley, J.; Davie, G. Individual EQ-5D trajectories: An alternative approach to understanding recovery pathways. In Proceedings of the EuroQol Group’s 31st Scientific Meeting, Stockholm, Sweden, 25–26 September 2014. [Google Scholar]
- McAllister, S.; Derrett, S.; Davie, G.; McGee, R. Injury characteristics and EQ-5D as predictors of personal wellbeing after injury. Int. J. Wellbeing 2014, 4, 19–31. [Google Scholar] [CrossRef]
- Gabbe, B.; Lyons, R.A.; Simpson, P.M.; Rivara, F.P.; Ameratunga, S.; Polinder, S.; Derrett, S.; Harrison, J.E. Disability weights for injury burden: Person-reported results from the prospective, multi-national, injury-vibes cohort. Bull. World Health Organ. 2016, 94, 806C–816C. [Google Scholar] [CrossRef]
- Statistics New Zealand. New Zealand Standard Classification of Occupations; Statistics New Zealand: Willington, New Zealand, 2001. [Google Scholar]
- Statistics New Zealand. 2006 Census Questionnaires. Available online: http://www.stats.govt.nz/Census/about-2006-census/2006-census-questionnaires.aspx (accessed on 12 August 2011).
- Statistics New Zealand. Household Economic Survey 2006–2007 Printable Questionnaires. Available online: https://www.stats.govt.nz/about-us/stats-nz-archive-website/ (accessed on 14 May 2021).
- Holmes, T.H.; Rahe, R.H. The social readjustment rating scale. J. Psychosom. Res. 1967, 11, 213–218. [Google Scholar] [CrossRef]
- Ministry of Health. A Portrait of Health. Key Results from the 2006/07 New Zealand Health Survey; Ministry of Health: Wellington, New Zealand, 2008.
- Üstün, T.B.; Chatterji, S.; Kostanjsek, N.; Rehm, J.; Kennedy, C.; Epping-Jordan, J.; Saxena, S.; van Korff, M.; Pull, C. Developing the World Health Organization disability assessment schedule 2.0. Bull. World Health Organ. 2010, 88, 815–823. [Google Scholar] [CrossRef]
- Herdman, M.; Gudex, C.; Lloyd, A.; Janssen, M.F.; Kind, P.; Parkin, D.; Bonsel, G.; Badia, X. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual. Life Res. 2011, 20, 1727–1736. [Google Scholar] [CrossRef]
- Bush, K.; Kivlahan, D.R.; McDonell, M.B.; Fihn, S.D.; Bradley, K.A. The AUDIT alcohol consumption questions (AUDIT-C): An effective brief screening test for problem drinking. Arch. Intern. Med. 1998, 158, 1789–1795. [Google Scholar] [CrossRef]
- Fugl-Meyer, A.R.; Bränholm, I.-B.; Fugl-Meyer, K.S. Happiness and domain-specific life satisfaction in adult northern Swedes. Clin. Rehabil. 1991, 5, 25–33. [Google Scholar] [CrossRef]
- Kessler, R.C.; Andrews, G.; Colpe, L.J.; Hiripi, E.; Mroczek, D.K.; Normand, S.L.T.; Walters, E.E.; Zaslavsky, A.M. Short screening scales to monitor population prevalences and trends in non-specific psychological distress. Psychol. Med. 2002, 32, 959–976. [Google Scholar] [CrossRef]
- Diener, E.; Wirtz, D.; Tov, W.; Kim-Prieto, C.; Choi, D.-W.; Oishi, S.; Biswas-Diener, R. New well-being measures: Short scales to assess flourishing and positive and negative feelings. Soc. Indic. Res. 2010, 97, 143–156. [Google Scholar] [CrossRef]
- World Health Organisation. ICF: International Classification of Functioning, Disability and Health; World Health Organisation: Geneva, Switzerland, 2001. [Google Scholar]
- Ministry of Health. Content Guide 2016/17: New Zealand Health Survey; Ministry of Health: Wellington, New Zealand, 2017.
- Langley, J.; Davie, G.; Wilson, S.; Lilley, R.; Ameratunga, S.; Wyeth, E.; Derrett, S. Difficulties in functioning 1 year after injury: The role of preinjury sociodemographic and health characteristics, health care and injury-related factors. Arch. Phys. Med. Rehabil. 2013, 94, 1277–1286. [Google Scholar] [CrossRef]
- Wilson, S.J.; Derrett, S.; Cameron, I.D.; Samaranayaka, A.; Davie, G.; Langley, J. Prevalence of poor outcomes soon after injury and their association with the severity of the injury. Inj. Prev. 2014, 20, 57. [Google Scholar] [CrossRef]
- SPARC. The New Zealand Physical Activity Questionnaires; SPARC (with support of the Ministry of Health, Wellington, New Zealand): Wellington, New Zealand, 2004.
- Langley, J.; Derrett, S.; Davie, G.; Ameratunga, S.; Wyeth, E. A cohort study of short-term functional outcomes following injury: The role of pre-injury socio-demographic and health characteristics, injury and injury-related healthcare. Health Qual. Life Outcomes 2011, 9, 68. [Google Scholar] [CrossRef]
- Ware, J.; Kosinski, M.; Gandek, B. SF-36® Health Survey: Manual and Interpretation Guide; QualityMetric Incorporated: Lincoln, RI, USA, 2000. [Google Scholar]
- Hone, L.; Jarden, A.; Schofield, G. Psychometric properties of the Flourishing Scale in a New Zealand sample. Soc. Indic. Res. 2014, 119, 1031–1045. [Google Scholar] [CrossRef]
- Wilson, R.; Hansen, P.; Langley, J.; Derrett, S. A comparison of injured patient and general population valuations of EQ-5D health states for New Zealand. Health Qual. Life Outcomes 2014, 12, 21. [Google Scholar] [CrossRef]
- Zou, G. A modified poisson regression approach to prospective studies with binary data. Am. J. Epidemiol. 2004, 159, 702–706. [Google Scholar] [CrossRef]
- Narduzzi, S.; Golini, M.N.; Porta, D.; Stafoggia, M.; Forastiere, F. Inverse probability weighting (IPW) for evaluating and “correcting” selection bias. Epidemiol. Prev. 2014, 38, 335–341. [Google Scholar]
- Sterne, J.A.; White, I.R.; Carlin, J.B.; Spratt, M.; Royston, P.; Kenward, M.G.; Wood, A.M.; Carpenter, J.R. Multiple imputation for missing data in epidemiological and clinical research: Potential and pitfalls. BMJ 2009, 338, b2393. [Google Scholar] [CrossRef] [PubMed]
- Lingsma, H.F.; Roozenbeek, B.; Steyerberg, E.W.; Murray, G.D.; Maas, A.I. Early prognosis in traumatic brain injury: From prophecies to predictions. Lancet Neurol. 2010, 9, 543–554. [Google Scholar] [CrossRef]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Derrett, S.; Wyeth, E.H.; Richardson, A.; Davie, G.; Samaranayaka, A.; Lilley, R.; Harcombe, H. Prospective Outcomes of Injury Study 10 Years on (POIS-10): An Observational Cohort Study. Methods Protoc. 2021, 4, 35. https://doi.org/10.3390/mps4020035
Derrett S, Wyeth EH, Richardson A, Davie G, Samaranayaka A, Lilley R, Harcombe H. Prospective Outcomes of Injury Study 10 Years on (POIS-10): An Observational Cohort Study. Methods and Protocols. 2021; 4(2):35. https://doi.org/10.3390/mps4020035
Chicago/Turabian StyleDerrett, Sarah, Emma H. Wyeth, Amy Richardson, Gabrielle Davie, Ari Samaranayaka, Rebbecca Lilley, and Helen Harcombe. 2021. "Prospective Outcomes of Injury Study 10 Years on (POIS-10): An Observational Cohort Study" Methods and Protocols 4, no. 2: 35. https://doi.org/10.3390/mps4020035
APA StyleDerrett, S., Wyeth, E. H., Richardson, A., Davie, G., Samaranayaka, A., Lilley, R., & Harcombe, H. (2021). Prospective Outcomes of Injury Study 10 Years on (POIS-10): An Observational Cohort Study. Methods and Protocols, 4(2), 35. https://doi.org/10.3390/mps4020035