
Flow Cytometry Confirmation Post Newborn Screening for SCID in England


Abstract
:1. Introduction
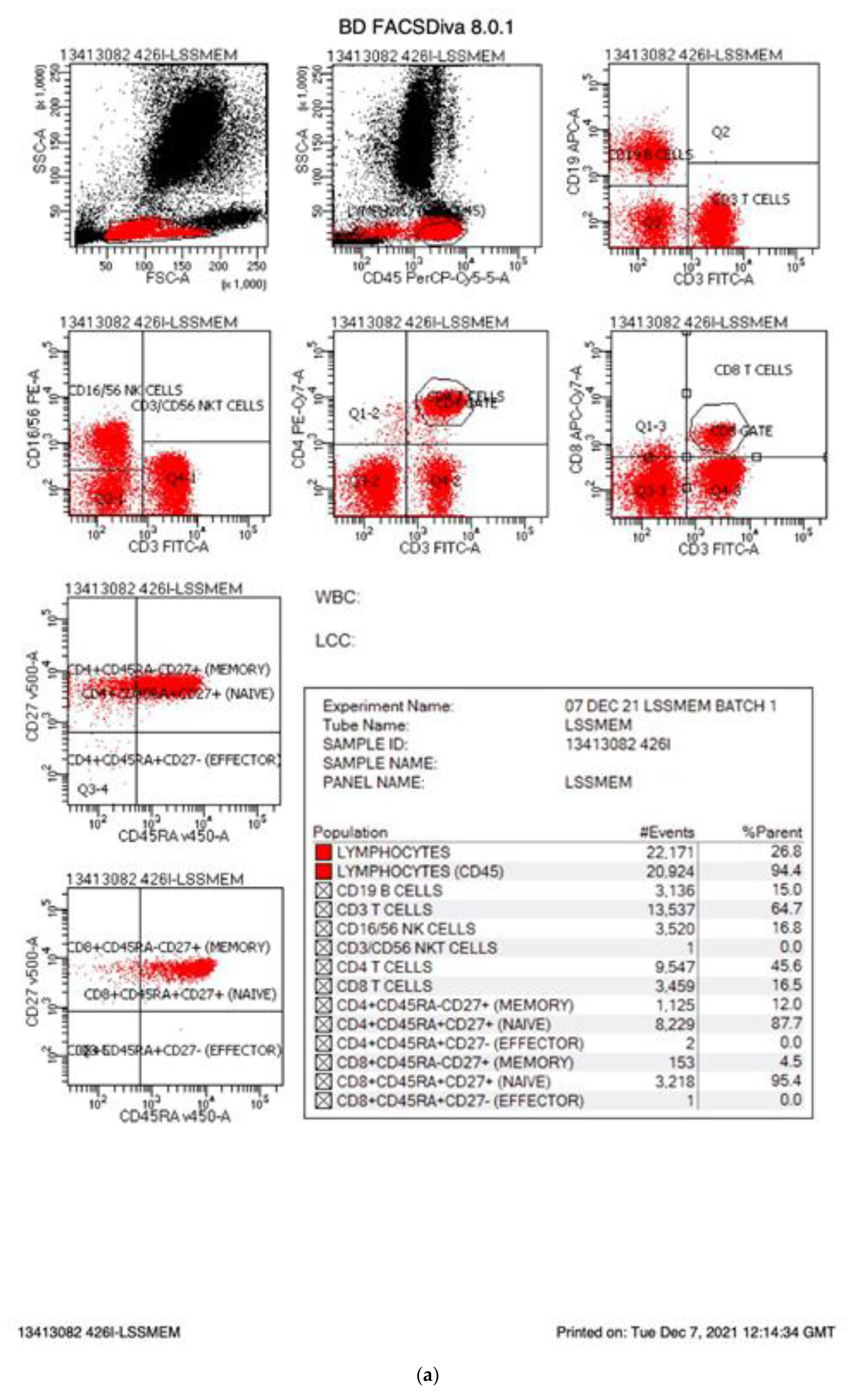
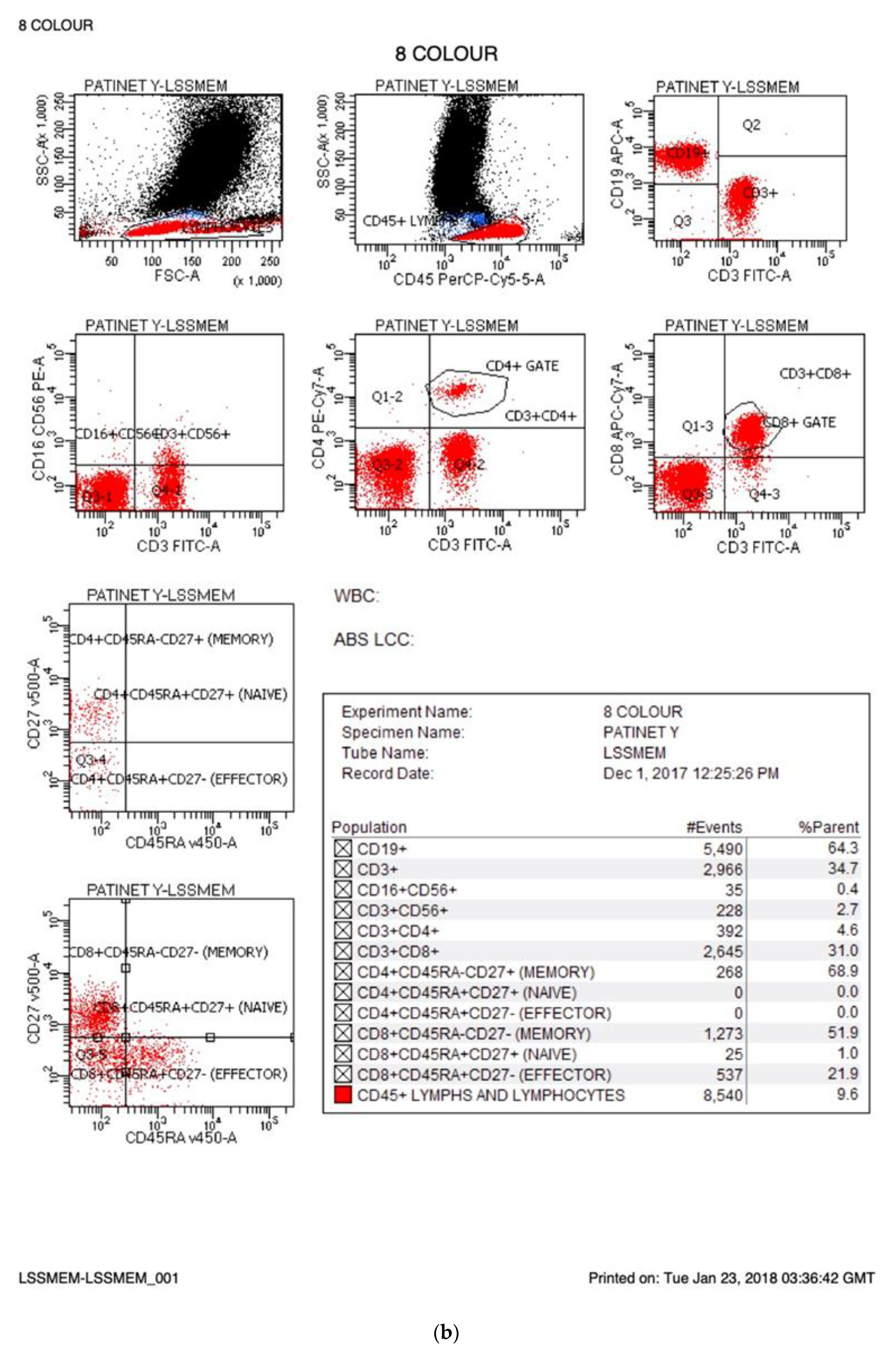
2. Flow Cytometry for SCID in England
3. Comparison of English Values with Other SCID Screening Programs
4. Summary
Funding
Conflicts of Interest
References
- Brown, L.; Xu-Bayford, J.; Allwood, Z.; Slatter, M.; Cant, A.; Davies, E.G.; Veys, P.; Gennery, A.R.; Gaspar, H.B. Neonatal diagnossi of severe combined immunodefricney leads to significantly improved survival outcome: The case for newbron screening. Blood 2011, 17, 3243–3246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kwan, A.; Abraham, R.S.; Currier, R.; Brower, A.; Andruszewski, K.; Abbott, J.; Baker, M.; Ballow, M.; Bartoshesky, L.E.; Bonilla, F.A.; et al. Newborn screening for severe combined immunodeficiency in 11 screening programs in the United States. JAMA 2014, 312, 729–738. [Google Scholar] [CrossRef] [PubMed]
- Knight, V.; Heimall, J.R.; Wright, N.; Dutmer, C.M.; Boyce, T.G.; Torgerson, T.R.; Abraham, R.S. Follow-up for an abnormal newborn screen for severe combined immunodeficiencies (nbs scid): A clinical immunology society (CIS) Survey of Cur/1 rent Practices. Int. J. Neonatal Screen. 2020, 6, 52. [Google Scholar] [CrossRef] [PubMed]
- Amatuni, G.S.; Currier, R.J.; Church, J.A.; Bishop, T.; Grimbacher, E.; Nguyen, A.; Agarwal-Hashmi, R.; Aznar, C.P.; Butte, M.J.; Cowan, M.J.; et al. Newborn screening for severe combined immunodeficiency and T-cell Lymphopenia in California, 2010–2017. Pediatrics 2019, 143, e20182300. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Comans-Bitter, W.M.; de Groot, R.; van den Beemd, R.; Neijens, H.J.; Hop, W.C.; Groeneveld, K.; Hooijkaas, H.; van Dongen, J.J. Immunophneotyping of blood lymphocytes in childhood. Reference values for lymphocyte subpopulations. J. Pediatr. 1997, 130, 388–393. [Google Scholar] [CrossRef] [Green Version]
- Shearer, W.T.; Dunn, E.; Notarangelo, L.D.; Dvorak, C.C.; Puck, J.M.; Logan, B.R.; Griffith, L.M.; Kohn, D.B.; O’Reilly, R.J.; Fleisher, T.A.; et al. Establishing diagnostic criteria for severe combined immunodeficiency disease (SCID), leaky SCID, and Omenn syndrome: The primary immune deficiency treatment consortium experience. J. Allergy Clin. Immunol. 2014, 133, 1092–1098. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Argudo-Remirez, A.; Martin-Nalda, A.; Marin-Sori, J.L.; Lopez-Galera, R.M.; Pajares-Garcia, S.; Gonzolez de Aledo-Castillo, J.M.; Martínez-Gallo, M.; García-Prat, M.; Colobran, R.; Riviere, J.G. First Universal Screening Program for Severe Combined Immunodeficiency in Europe. Two years’ experience in Catalonia (Spain). Front. Immunol. 2019, 10, 2406. [Google Scholar] [CrossRef] [PubMed]
- Adams, S.P.; Kricke, S.; Ralph, E.; Gilmour, N.; Gilmour, K.C. A comparison of TRECs and flow cytometry for naïve T cell quantification. Clin. Exp. Immunol. 2018, 191, 198–202. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Lymphocyte Population | FACs/CD Marker | Normal Range for 1–4 Weeks [5] Percentage Absolute Counts (Cells/μL) | Range for SCID Percentage Absolute Counts (Cells/μL) | Range for Abnormal/T Lymphopaenia Percentage Absolute Counts (Cells/μL) |
|---|---|---|---|---|
| T cells | CD3+ | 60–85% 2300–7000 | <300 | <30% T cells < 1500 |
| B cells | CD19+ | 4–26% 600–1900 | ||
| NK | CD16+/56+ | 3–23% 200–1400 | ||
| CD4 T cells | CD3+CD4+ | 41–68% 1700–3500 | ||
| CD8 T cells | CD3+CD8+ | 9–23% 400–1700 | ||
| Naïve T cells | CD45RA+/CD27+_ | 80–100% | <25% | <70% |
| MHC II expression on APCs (B cells or monocytes | DR+ | 100% | <10% | <90% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gilmour, K.C. Flow Cytometry Confirmation Post Newborn Screening for SCID in England. Int. J. Neonatal Screen. 2022, 8, 1. https://doi.org/10.3390/ijns8010001
Gilmour KC. Flow Cytometry Confirmation Post Newborn Screening for SCID in England. International Journal of Neonatal Screening. 2022; 8(1):1. https://doi.org/10.3390/ijns8010001
Chicago/Turabian StyleGilmour, Kimberly C. 2022. "Flow Cytometry Confirmation Post Newborn Screening for SCID in England" International Journal of Neonatal Screening 8, no. 1: 1. https://doi.org/10.3390/ijns8010001
APA StyleGilmour, K. C. (2022). Flow Cytometry Confirmation Post Newborn Screening for SCID in England. International Journal of Neonatal Screening, 8(1), 1. https://doi.org/10.3390/ijns8010001