
Successful Implementation of Newborn Screening for Hemoglobin Disorders in the Philippines


 , ,
, ,
Abstract
1. Introduction
1.1. Evolution of Newborn Screening in the Philippines
1.2. Hemoglobin Disorders
2. Methodology
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| α | Alpha |
| β | Beta |
| CAH | Congenital adrenal hyperplasia |
| CDC | Centers for Disease Control and Prevention (U.S.) |
| CE | Capillary electrophoresis |
| CH | Congenital hypothyroidism |
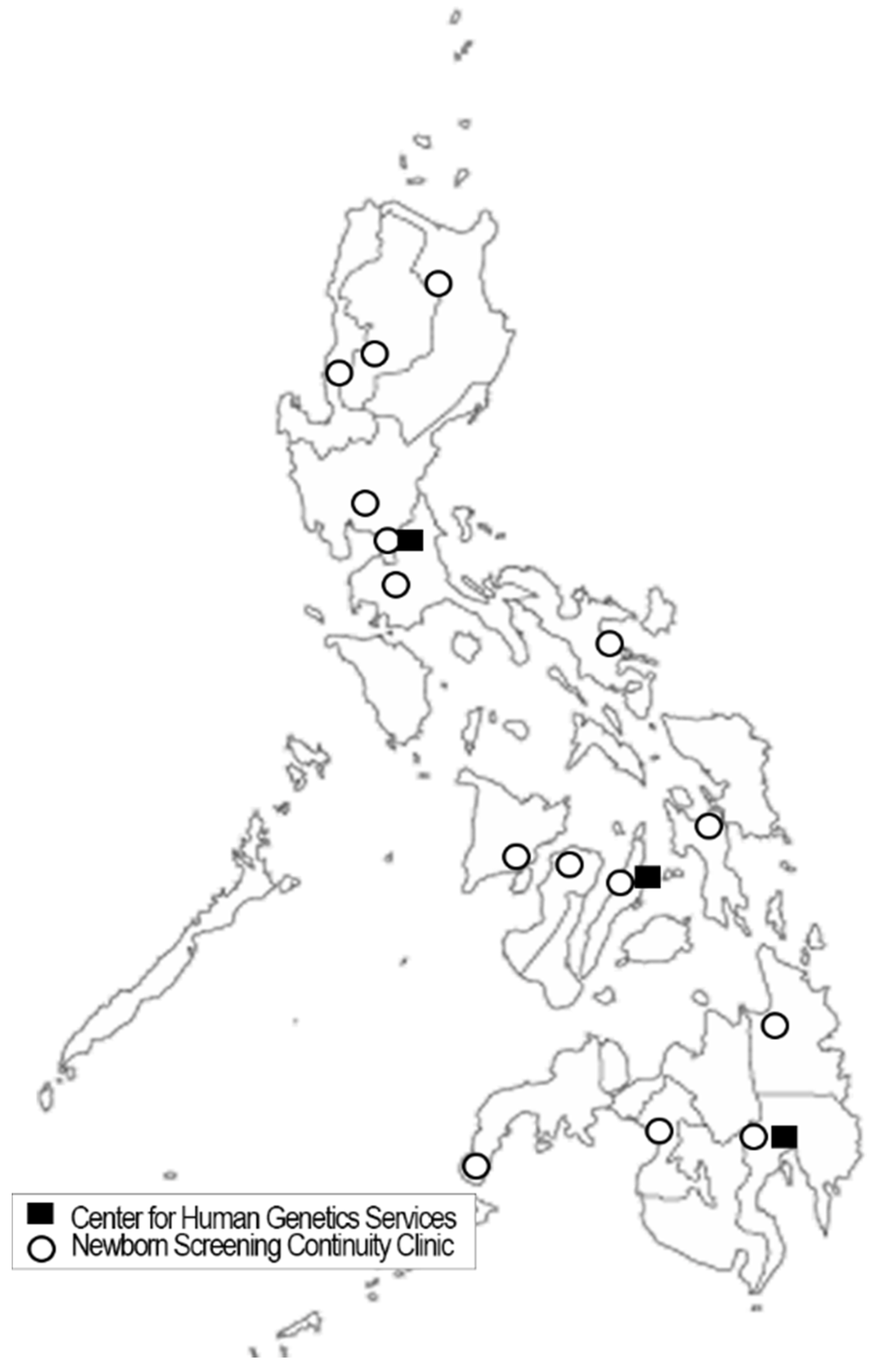
| CHGS | Center for Human Genetic Services |
| CNSP | California Newborn Screening Program (U.S.) |
| DOH | Department of Health (national health agency - Philippines) |
| G6PD | Glucose-6-phosphate dehydrogenase |
| GAL | Galactosemia |
| Hb | Hemoglobin |
| HCY | Homocystinuria |
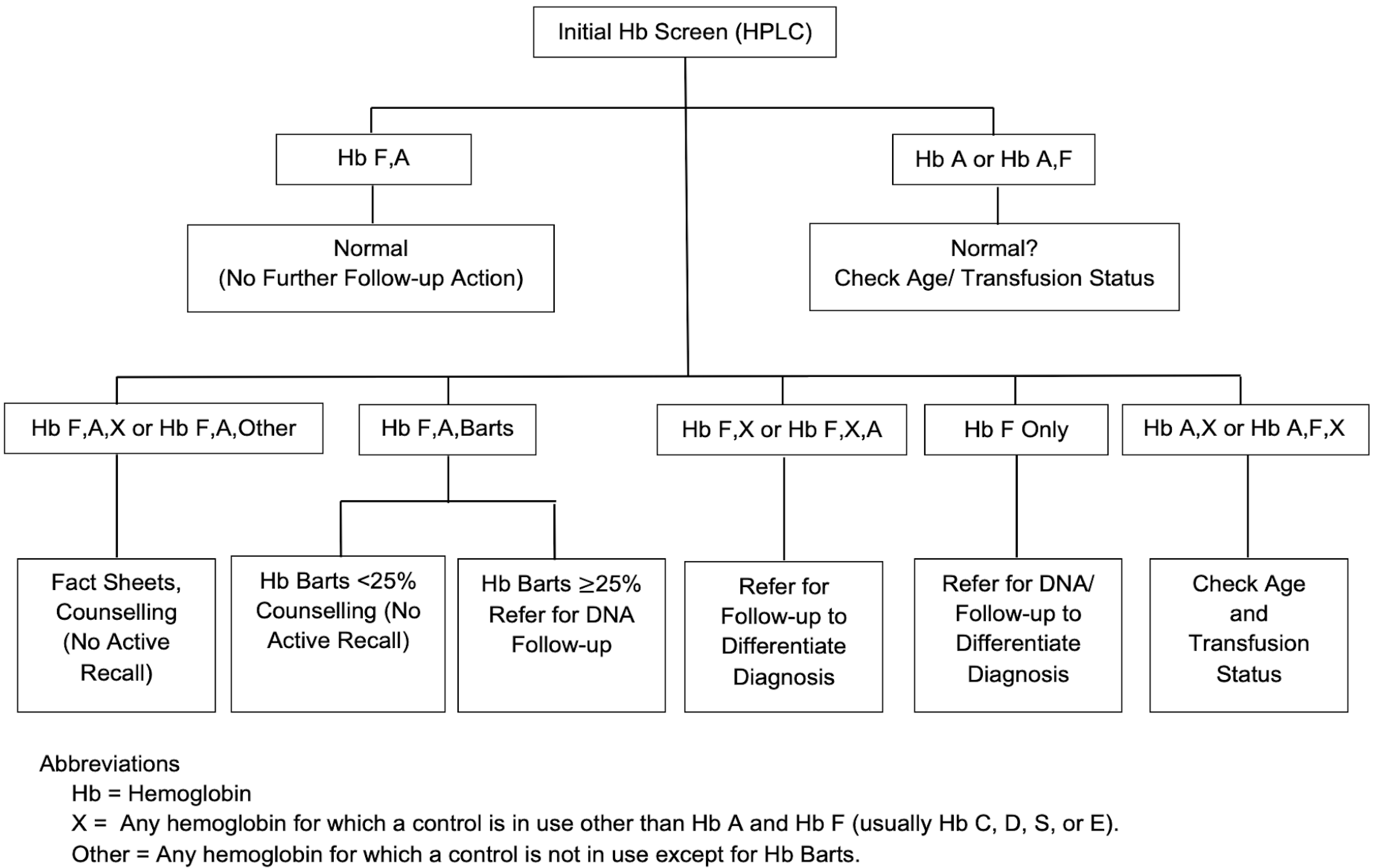
| HPLC | High performance liquid chromatography |
| MSUD | Maple syrup urine disease |
| NBS | Newborn bloodspot screening |
| NBSCC | Newborn screening continuity clinic (long-term follow-up - Philippines) |
| NNSGRC | National Newborn Screening and Global Resource Center (U.S.) |
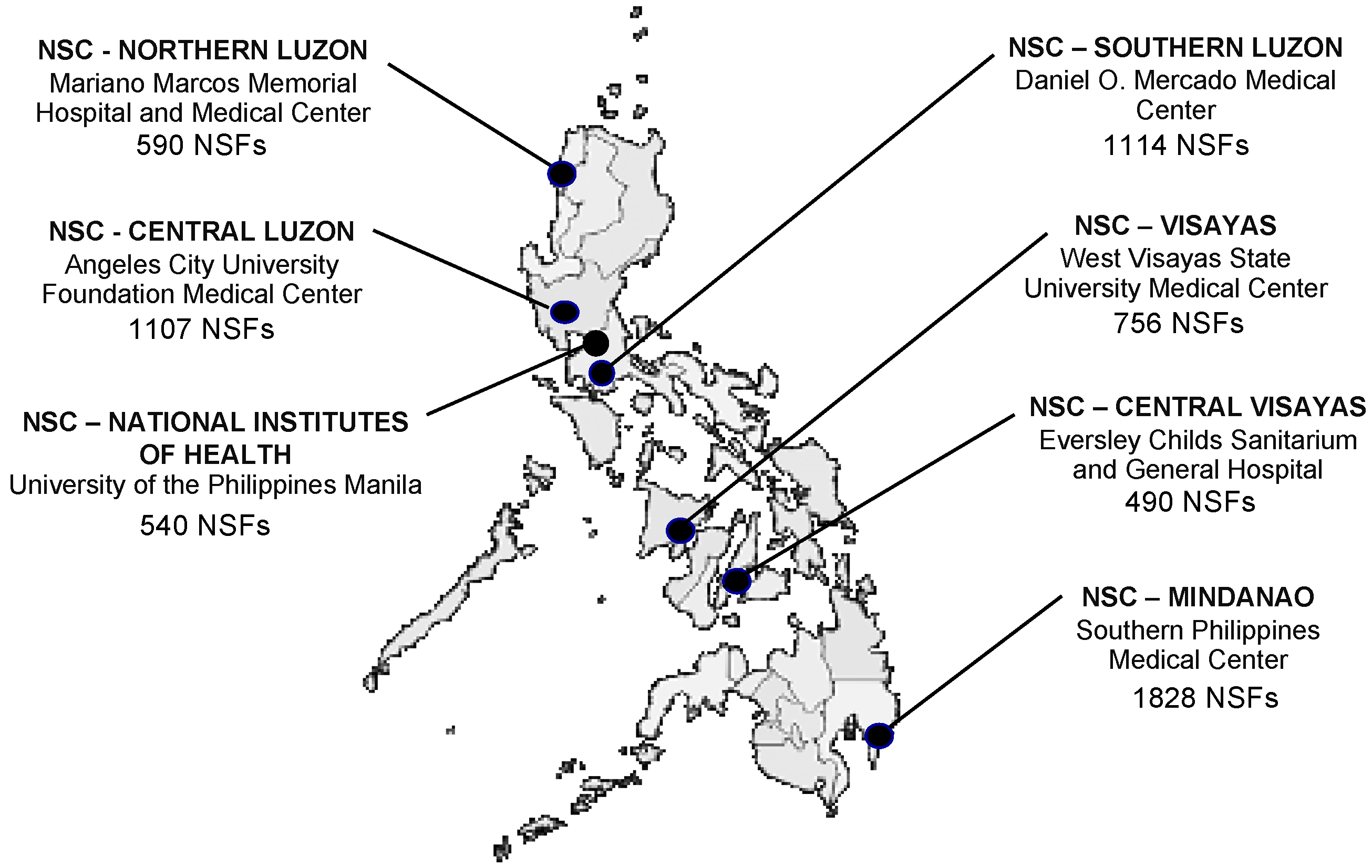
| NSC | Newborn Screening Center (screening laboratory - Philippines) |
| NSF | Newborn Screening Facility (screening specimen collection site - Philippines) |
| NSQAP | Newborn Screening Quality Assurance Program (U.S.) |
| NSRC | Newborn Screening Reference Center (Philippines) |
| PhilHealth | Philippine Health Insurance Corporation (national health insurance) |
| PKU | Phenylketonuria |
| POGS | Philippine Obstetrical and Gynecological Society |
| PPS | Philippine Pediatric Society |
| PT | Proficiency testing |
| QC | Quality control |
| SCD | Sickle cell disease |
References
- Padilla, C.; Domingo, C.F. Implementation of newborn screening in the Philippines. Phil. J. Pediatr. 2002, 51, 2–10. [Google Scholar]
- David-Padilla, C.; Basilio, J.A.; Oliveros, Y.E. Newborn Screening: Research to Policy. Acta Med. Philipp. 2009, 43, 6–14. [Google Scholar]
- Padilla, C. Newborn screening in the Philippines. Southeast Asia J. Trop. Med. Pub. Health 2003, 34 (Suppl. S3), 87–88. [Google Scholar]
- Department of Health Memorandum No. 2012-0154. Inclusion of MSUD in the Newborn Screening Panel of Disorders. Available online: https://www.newbornscreening.ph/images/stories/ResourcesDOHPolicies/doh-2012-0154.pdf (accessed on 17 February 2021).
- Presidential Proclamation No. 540. Declaring the 1st Week of October of Each Year as “National Newborn Screening Week”. Available online: https://www.newbornscreening.ph/images/stories/ResourcesDOHPolicies/Presidential%20Proclamation%20No.%20540.pdf (accessed on 5 April 2021).
- Republic Act 9288—Newborn Screening Act of 2004. Available online: https://www.doh.gov.ph/sites/default/files/policies_and_laws/RA09288.pdf (accessed on 17 February 2021).
- PhilHealth Circular, No. 34, s-2006. PhilHealth Newborn Care Package. Available online: https://www.philhealth.gov.ph/circulars/2006/circ34_2006.pdf (accessed on 17 February 2021).
- American Academy of Pediatrics, Newborn Screening Task Force. Serving the family from birth to the medical home—Newborn screening: A blueprint for the future. Pediatrics 2000, 106, 383–427. [Google Scholar]
- American College of Medical Genetics, Newborn Screening Expert Group. Newborn screening: Toward a uniform screening panel and system. Genet. Med. 2006, 8 (Suppl. S1), 1S–252S. [Google Scholar]
- Feuchtbaum, L.; Carter, J.; Dowray, S.; Currier, R.J.; Lorey, F. Birth prevalence of disorders detectable through newborn screening by race/ethnicity. Genet. Med. 2012, 14, 937–945. [Google Scholar] [CrossRef]
- Padilla, C.D. Enhancing Case Detection of Selected Inherited Disorders through Expanded Newborn Screening in the Philippines. Acta Med. Philipp. 2013, 47, 1–6. [Google Scholar] [CrossRef]
- Therrell, B.L.; Hoppe, C.; Mann, M.Y.; Azimi, M.; Brants, A.; Brown, S.E.; Carte, L.S.; Dorle, M.C.; Eckman, J.R.; Flamini, M. Newborn Screening for Hemoglobinopathies, 1st ed.; CLSI Guideline NBS08; Clinical Laboratory Standards Institute: Wayne, PA, USA, 2019. [Google Scholar]
- Lorey, F.; Cunningham, G.; Vichinsky, E.P.; Lubin, B.H.; Witkowska, H.E.; Matsunaga, A.; Azimi, M.; Sherwin, J.; Eastman, J.; Farina, F.; et al. Universal Newborn Screening for Hb H Disease in California. Genet. Test. 2001, 5, 93–100. [Google Scholar] [CrossRef]
- Michlitsch, J.; Azimi, M.; Hoppe, C.; Walters, M.C.; Lubin, B.; Lorey, F.; Vichinsky, E. Newborn screening for hemoglobinopathies in California. Pediatr. Blood Cancer 2009, 52, 486–490. [Google Scholar] [CrossRef]
- Hoppe, C.C. Newborn Screening for Hemoglobin Disorders. Hemoglobin 2011, 35, 556–564. [Google Scholar] [CrossRef]
- Therrell, B.; Pass, K. Hemoglobinopathy screening laboratory techniques for newborns. In Laboratory Methods for Neonatal Screening; Therrell, B., Ed.; American Public Health Association: Washington, DC, USA, 1993; pp. 169–189. [Google Scholar]
- Lal, A.; Goldrich, M.L.; Haines, D.A.; Azimi, M.; Singer, S.T.; Vichinsky, E.P. Heterogeneity of Hemoglobin H Disease in Childhood. N. Engl. J. Med. 2011, 364, 710–718. [Google Scholar] [CrossRef]
- Piel, F.B.; Weatherall, D.J. The α-thalassemias. N. Engl. J. Med. 2014, 371, 1908–1916. [Google Scholar] [CrossRef] [PubMed]
- Hall, J.G.; Yuen, J.; Hunt, J.A.; Chu, B.M.; Hsia, Y.E. Gene frequencies for the alpha-globin variants among Chinese, Laotians and Filipinos. Am. J. Hum. Genet. 1991, 49, 470, Abstract 2679. [Google Scholar]
- Ko, T.M.; Hwa, H.L.; Liu, C.W.; Li, S.F.; Chu, J.Y.; Cheung, Y.P. Prevalence study and molecular characterization of alpha-thalassemia in Filipinos. Ann. Hematol. 1999, 78, 355–357. [Google Scholar] [CrossRef] [PubMed]
- Ko, T.M.; Caviles, A.P., Jr.; Hwa, H.L.; Liu, C.W.; Hsu, P.M.; Chung, Y.P. Prevalence and molecular characterization of beta-thalassemia in Filipinos. Ann. Hematol. 1998, 77, 257–260. [Google Scholar] [CrossRef]
- Loeber, J.G.; Burgard, P.; Cornel, M.C.; Rigter, T.; Weinreich, S.S.; Rupp, K.; Hoffmann, G.F.; Vittozzi, L. Newborn screening programmes in Europe; arguments and efforts regarding harmonization. Part 1—From blood spot to screening result. J. Inherit. Metab. Dis. 2012, 35, 603–611. [Google Scholar] [CrossRef] [PubMed]
- Burgard, P.; Rupp, K.; Lindner, M.; Haege, G.; Rigter, T.; Weinreich, S.S.; Loeber, J.G.; Taruscio, D.; Vittozzi, L.; Cornel, M.C.; et al. Newborn screening programmes in Europe; arguments and efforts regarding harmonization. Part 2—From screening laboratory results to treatment, follow-up and quality assurance. J. Inherit. Metab. Dis. 2012, 35, 613–625. [Google Scholar] [CrossRef]
- Benson, J.M.; Therrell, B.L., Jr. History and current status of newborn screening for hemoglobinopathies. Semin Perinatol. 2010, 34, 134–144. [Google Scholar] [CrossRef]
- Hoppe, C.C. Newborn screening for non-sickling hemoglobinopathies. Hematology 2009, 2009, 19–25. [Google Scholar] [CrossRef]
- Shafer, F.E.; Lorey, F.; Cunningham, G.C.; Klumpp, C.; Vichinsky, E.; Lubin, B. Newborn screening for sickle cell disease: 4 years of experience from California’s newborn screening program. J. Pediatr Hematol Oncol. 1996, 18, 36–41. [Google Scholar] [CrossRef]
- Padilla, C.P.; Therrell, B.L.; Panol, K.A.R.; Concordia, R.N.; Reyes, M.E.L.; Jomento, C.M.; Maceda, E.B.G.; Lising, J.A.C.; Beltran, F.D.E.; Orbillo, L.L. Philippine Performance Evaluation and Assessment Scheme (PPEAS): Experiences in newborn screening system quality control. Int. J. Neonatal Screen. 2020, 6, 95. [Google Scholar] [CrossRef] [PubMed]
- Lorey, F.; Cunningham, G.; Shafer, F.; Lubin, B.; Vichinsky, E. Universal Screening for Hemoglobinopathies Using High-Performance Liquid Chromatography: Clinical Results of 2.2 Million Screens. Eur. J. Hum. Genet. 1994, 2, 262–271. [Google Scholar] [CrossRef]
- Liao, C.; Zhou, J.-Y.; Xie, X.-M.; Tang, H.-S.; Li, R.; Li, D.-Z. Newborn Screening for Hb H Disease by Determination of Hb Bart’s Using the Sebia Capillary Electrophoresis System in Southern China. Hemoglobin 2013, 38, 73–75. [Google Scholar] [CrossRef]
- De Jesus, V.R.; Mei, J.V.; Bell, C.J.; Hannon, W.H. Improving and assuring newborn screening laboratory quality worldwide: 30-year experience at the Centers for Disease Control and Prevention. Semin. Perinatol. 2010, 34, 125–133. [Google Scholar] [CrossRef] [PubMed]
- Lorey, F. Asian Immigration and Public Health in California: Thalassemia in Newborns in California. J. Pediatr. Hematol. 2000, 22, 564–566. [Google Scholar] [CrossRef] [PubMed]
- Vichinsky, E.P.; Macklin, E.A.; Waye, J.S.; Lorey, F.; Olivieri, N.F. Changes in the Epidemiology of Thalassemia in North America: A New Minority Disease. Pediatrics 2005, 116, e818–e825. [Google Scholar] [CrossRef]
- Benz, E.J., Jr. Newborn screening for α-thalassemia–keeping up with globalization. N. Engl. J. Med. 2011, 364, 770–771. [Google Scholar] [CrossRef] [PubMed]
- Bain, B.J. Neonatal/newborn haemoglobinopathy screening in Europe and Africa. J. Clin. Pathol. 2009, 62, 53–56. [Google Scholar] [CrossRef]
- Therrell, B.L.; Padilla, C.D.; Loeber, J.G.; Kneisser, I.; Saadallah, A.; Borrajo, G.J.; Adams, J. Current status of newborn screening worldwide: 2015. Semin. Perinatol. 2015, 39, 171–187. [Google Scholar] [CrossRef]
- Therrell, B.L., Jr.; Lloyd-Puryear, M.A.; Ohene-Frempong, K.; Ware, R.E., Jr.; Padilla, C.D.; Ambrose, E.E.; Barkat, A.; Ghazal, H.; Kiyaga, C.; Mvalo, T.; et al. Empowering newborn screening programs in African countries through establishment of an international collaborative effort. J. Community Genet. 2020, 11, 253–268. [Google Scholar] [CrossRef]
- Chui, D.; Fucharoen, S.; Chan, V. Hemoglobin H disease: Not necessarily a benign disorder. Blood 2003, 101, 791–800. [Google Scholar] [CrossRef]
- Fucharoen, S.; Viprakasit, V. Hb H disease: Clinical course and disease modifiers. Hematology 2009, 2009, 26–34. [Google Scholar] [CrossRef]
- Fucharoen, S.; Winichagoon, P. Hemoglobinopathies in southeast Asia. Indian J. Med. Res. 2011, 134, 498–506. [Google Scholar] [CrossRef] [PubMed]
- Vichinsky, E. Advances in the treatment of alpha-thalassemia. Blood Rev. 2012, 26, S31–S34. [Google Scholar] [CrossRef]
- Fucharoen, S.; Weatherall, D.J. The Hemoglobin E Thalassemias. Cold Spring Harb. Perspect. Med. 2012, 2, a011734. [Google Scholar] [CrossRef] [PubMed]
- Laurino, M.Y.; Padilla, C.D. Genetic Counseling Training in the Philippines. J. Genet. Couns. 2013, 22, 865–868. [Google Scholar] [CrossRef] [PubMed]
- PhilHealth Circular, No. 2018-0021. Enhancement of PhilHealth Newborn Care Package. Available online: https://www.philhealth.gov.ph/circulars/2018/circ2018-0021.pdf (accessed on 13 April 2021).




{kind=link}
{kind=link}
{kind=link}
| Hemoglobin Disorders | a Cases in Filipino Newborns Born in California 7 July 2005–6 July 2011 | a Prevalence in Filipino Newborns Born in California 7 July 2005–6 July 2011 | b Estimated Annual Cases of Filipino Newborns Born in Philippines |
|---|---|---|---|
| Hb H Disease | 93 | 1:1195 | 1860 |
| α Thalassemia Major | 5 | 1:22,225 | 100 |
| Homozygous E/E | 3 | 1:37,042 | 60 |
| Hb H/Constant Spring Disease | 2 | 1:55,564 | 40 |
| Hb SC Disease | 2 | 1:55,564 | 40 |
| Hb E/β+ Thalassemia | 1 | 1:111,127 | 20 |
| β Thalassemia major | 1 | 1:111,127 | 20 |
| Hb Variant/β+ Thalassemia | 1 | 1:111,127 | 20 |
| Hb SS Disease | 1 | 1:111,127 | 20 |
| Totals | 109 | 1:1020 | 2240 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Padilla, C.D.; Therrell, B.L., Jr.; Alcausin, M.M.L.B.; de Castro, R.C., Jr.; Gepte, M.B.P.; Reyes, M.E.L.; Jomento, C.M.; Suarez, R.C.N.; Maceda, E.B.G.; Abarquez, C.G.; et al. Successful Implementation of Newborn Screening for Hemoglobin Disorders in the Philippines. Int. J. Neonatal Screen. 2021, 7, 30. https://doi.org/10.3390/ijns7020030
Padilla CD, Therrell BL Jr., Alcausin MMLB, de Castro RC Jr., Gepte MBP, Reyes MEL, Jomento CM, Suarez RCN, Maceda EBG, Abarquez CG, et al. Successful Implementation of Newborn Screening for Hemoglobin Disorders in the Philippines. International Journal of Neonatal Screening. 2021; 7(2):30. https://doi.org/10.3390/ijns7020030
Chicago/Turabian StylePadilla, Carmencita D., Bradford L. Therrell, Jr., Maria Melanie Liberty B. Alcausin, Reynaldo C. de Castro, Jr., Maria Beatriz P. Gepte, Ma. Elouisa L. Reyes, Charity M. Jomento, Riza Concordia N. Suarez, Ebner Bon G. Maceda, Conchita G. Abarquez, and et al. 2021. "Successful Implementation of Newborn Screening for Hemoglobin Disorders in the Philippines" International Journal of Neonatal Screening 7, no. 2: 30. https://doi.org/10.3390/ijns7020030
APA StylePadilla, C. D., Therrell, B. L., Jr., Alcausin, M. M. L. B., de Castro, R. C., Jr., Gepte, M. B. P., Reyes, M. E. L., Jomento, C. M., Suarez, R. C. N., Maceda, E. B. G., Abarquez, C. G., Posecion, J. E. W. C., Andal, A. P., Elizaga, A. L. G., Halili-Mendoza, B. C., Otayza, M. P. V. K., & Hoppe, C. C. (2021). Successful Implementation of Newborn Screening for Hemoglobin Disorders in the Philippines. International Journal of Neonatal Screening, 7(2), 30. https://doi.org/10.3390/ijns7020030