Neonatal Urine Screening Program in the Province of Quebec: Technological Upgrade from Thin Layer Chromatography to Tandem Mass Spectrometry


Abstract
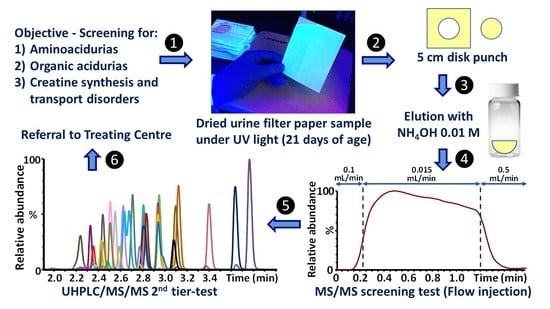
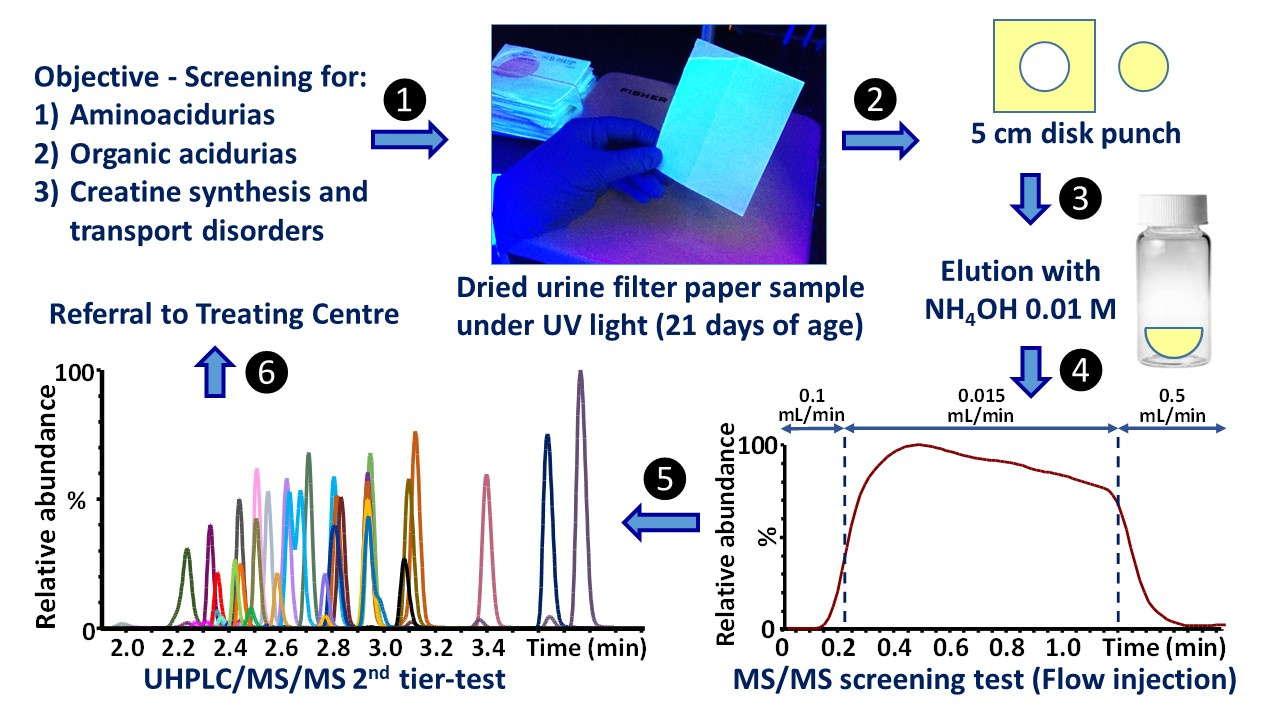
1. Introduction
2. Materials and Methods
2.1. Ethics Approval
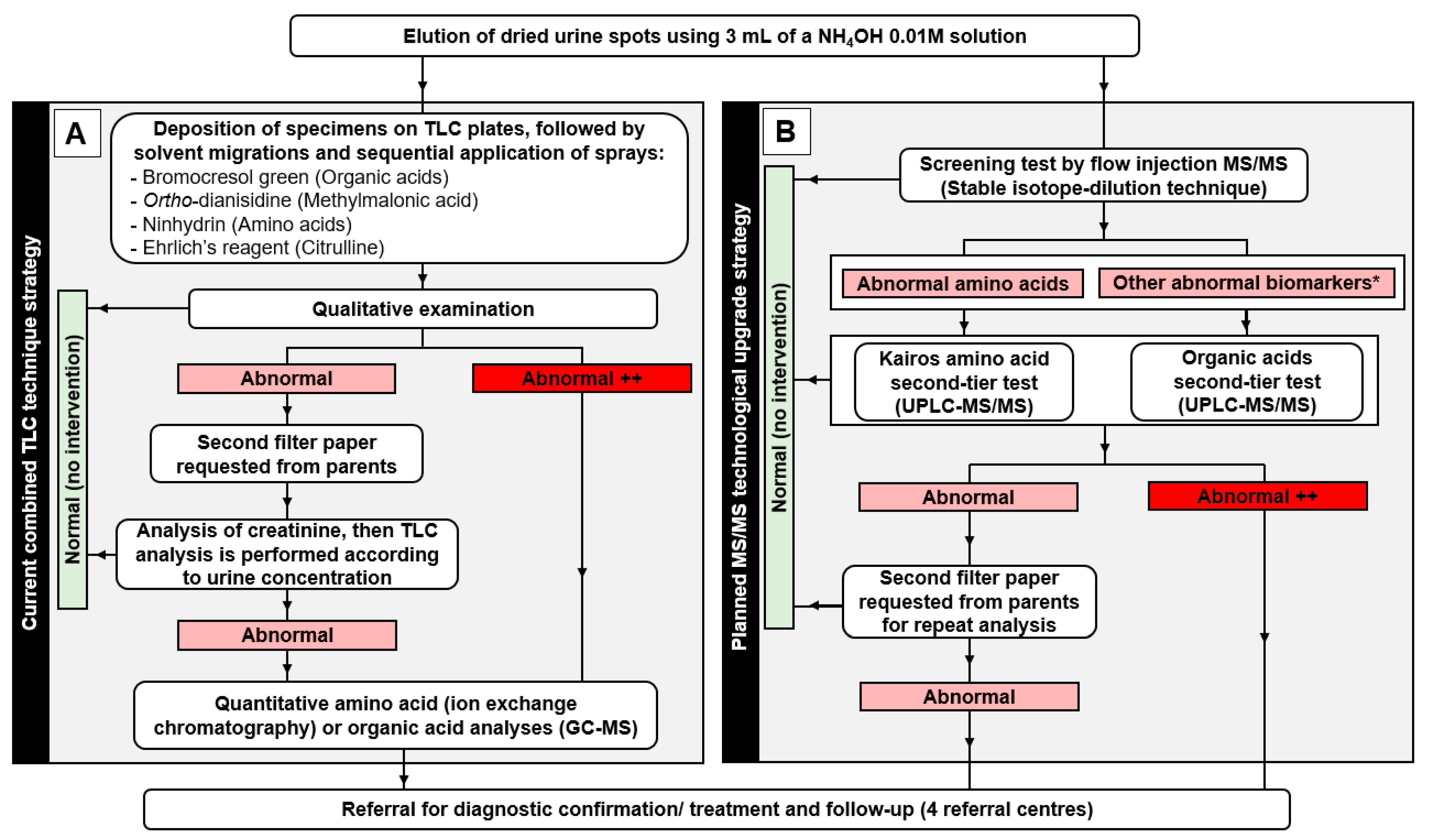
2.2. Overview of Current and Future Sample Processing and Interventions
2.3. Urine Specimens Collected on Filter Paper
2.4. Reagents
2.5. Preparation of Solutions
2.5.1. Standard Stock Solutions
2.5.2. Standard Working Solutions
Kairos Amino Acid Second-Tier Test
Organic Acids Second-Tier Test
2.5.3. Internal Standard Solutions
Screening Test
Kairos Amino Acid Second-Tier Test
Organic Acids Second-Tier Test
2.5.4. Quality Controls
Screening Test
Kairos Amino Acid Second-Tier Test
Organic Acids Second-Tier Test
2.6. Sample Preparation
2.6.1. Screening Test
2.6.2. Kairos Amino Acid Second-Tier Test
2.6.3. Organic Acids Second-Tier Test
2.7. Instrumentation and Parameters
2.7.1. Screening Test
2.7.2. Kairos Amino Acid Second-Tier Test
2.7.3. Organic Acids Second-Tier Test
2.8. Data Analysis
2.8.1. Screening Test
- A = (mcreat/m(IS-creat))*IScreat
- B = (1000*(mbiomarker/m(IS-biomarker))*ISbiomarker)/A
- C = (1000*(marginino/m(IS-cystine))*IScystine/RRF(arginino/cystine))/A
- D = ((m(creat-confirmation)/m(IS-creat-confirmation)*IScreat)/A
- E = ((mguanidine/m(IS-guanidine))*ISguanidine)/((mcreatine/m(IS-creatine))*IScreatine)
- A = Creatinine concentration (µM)
- mcreat = Signal of creatinine
- m(IS-creat) = Signal of creatinine internal standard
- IScreat = Creatinine internal standard concentration (µM)
- B = Biomarker concentration normalized with creatinine (µmol/mmol creatinine)
- mbiomarker = Signal of the biomarker analyzed
- m(IS-biomarker) = Signal of the internal standard of the biomarker
- C = Argininosuccinic acid concentration normalized with creatinine (µmol/mmol creatinine)
- marginino = Signal of argininosuccinic acid
- m(IS-cystine) = Signal of the cystine internal standard
- IScystine = Cystine internal standard concentration (µM)
- RRF(arginino/cystine) = Relative response factor (argininosuccinic acid/cystine)
- D = Creatinine confirmation ratio (no unit)
- m(creat-confirmation) = Signal of creatinine confirmation ion
- m(IS-creat-confirmation) = Signal of creatinine internal standard confirmation ion
- E = Ratio guanidineacetic acid/creatine (no unit)
- mguanidine = Signal guanidineacetic acid
- m(IS-guanidine) = Signal guanidineacetic acid internal standard
- ISguanidine = Guanidineacetic acid internal standard concentration (µM)
- mcreatine = Signal of creatine
- m(IS-creatine) = Signal of creatine internal standard
- IScreatine = Creatine internal standard concentration (µM)
2.8.2. Kairos Amino Acid Second-Tier Test
2.8.3. Organic Acids Second-Tier Test
2.9. Validation
2.9.1. Screening Test
2.9.2. Kairos Amino Acid Second-Tier Test
2.9.3. Organic Acids Second-Tier Test
3. Results
3.1. Chromatograms
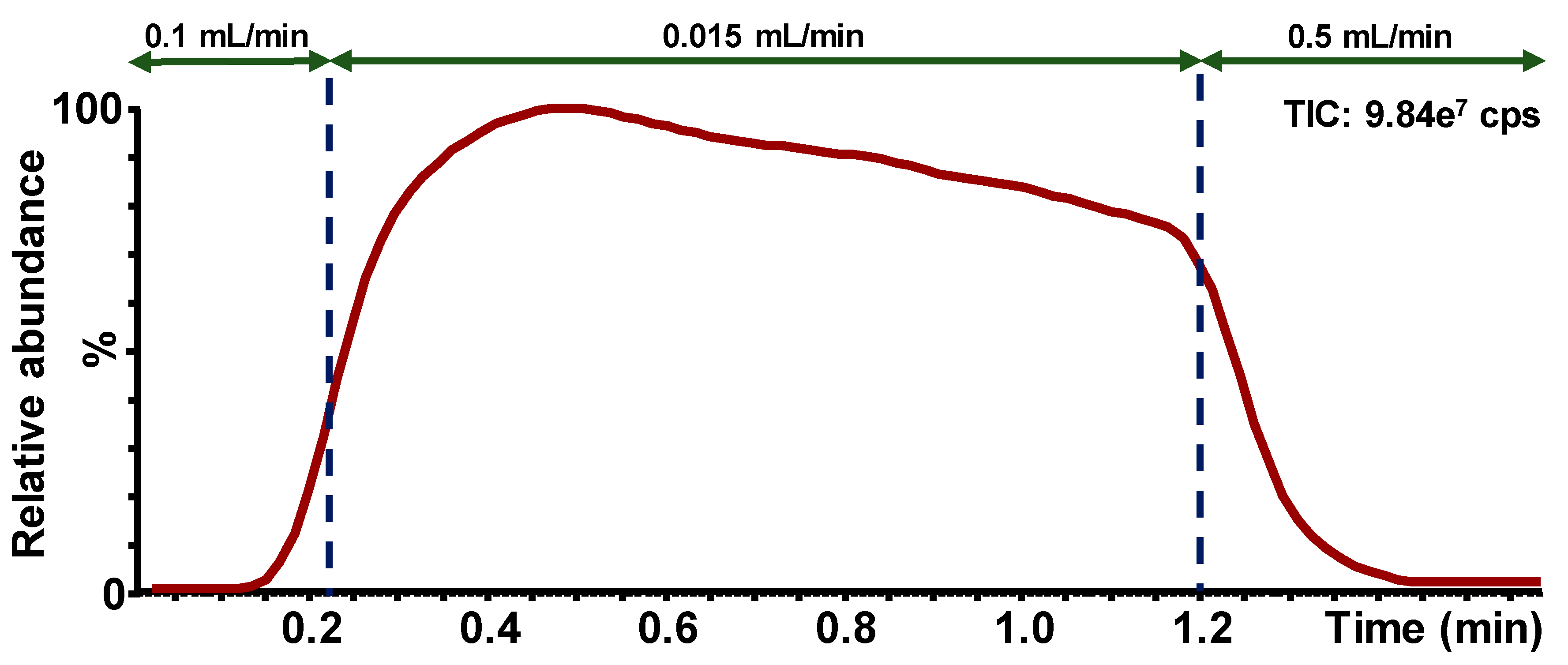
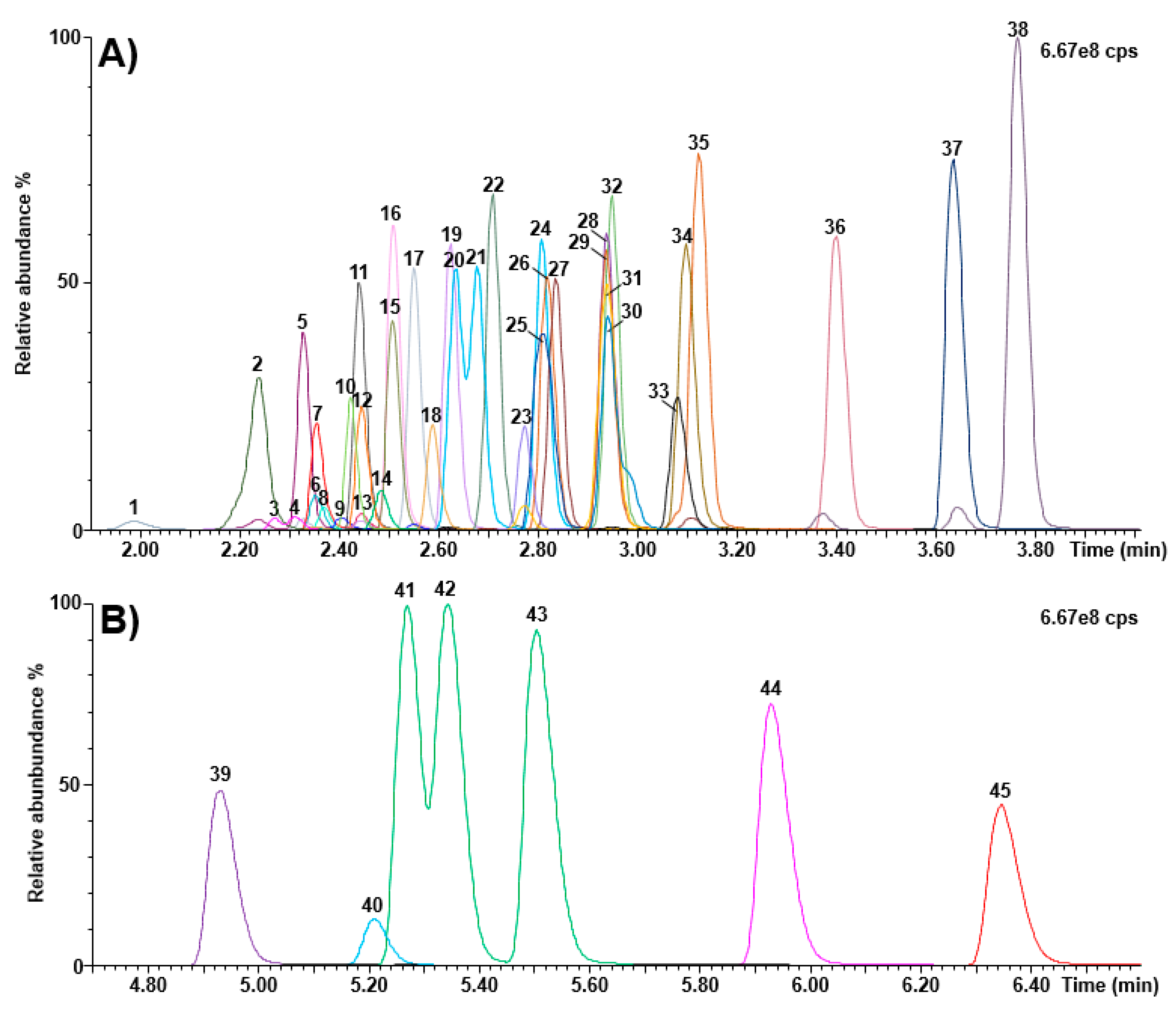
3.1.1. Screening Test
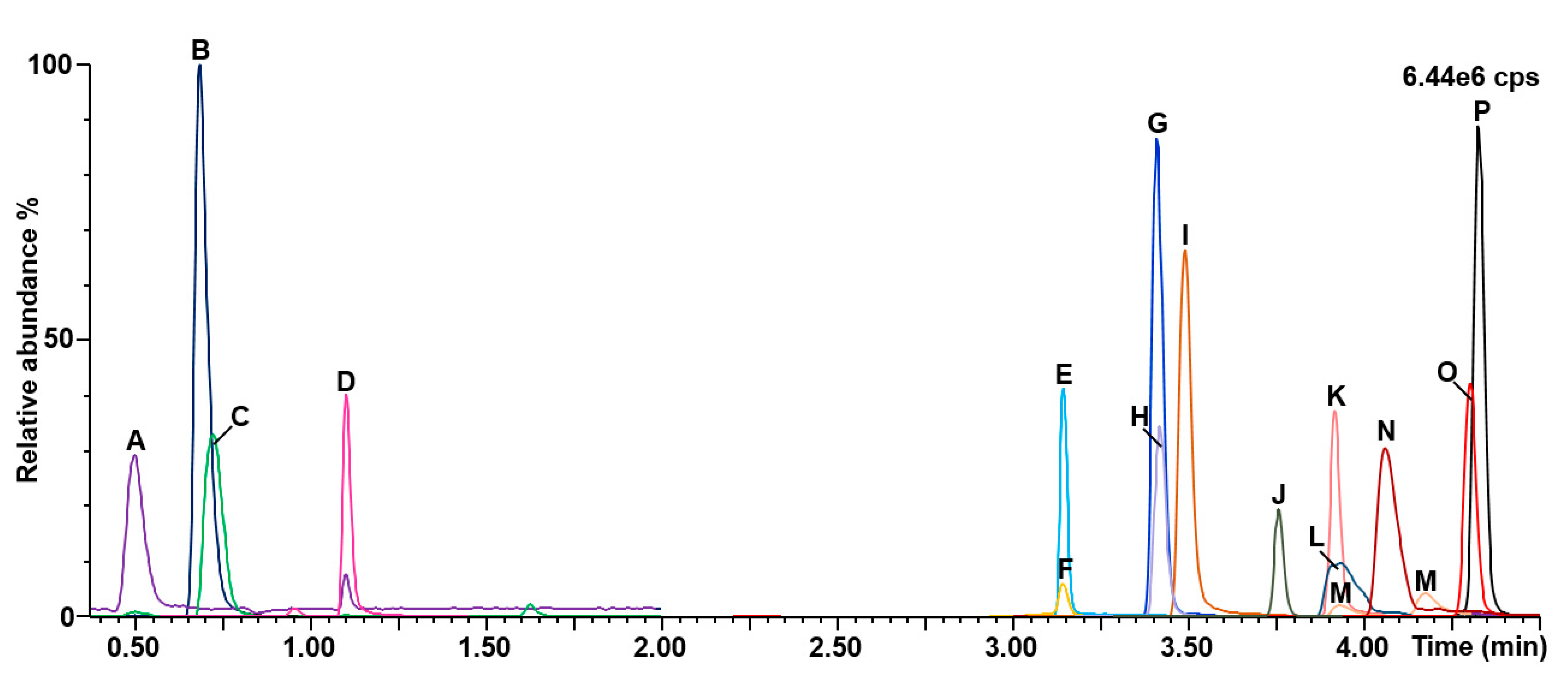
3.1.2. Kairos Amino Acids Second-Tier Test
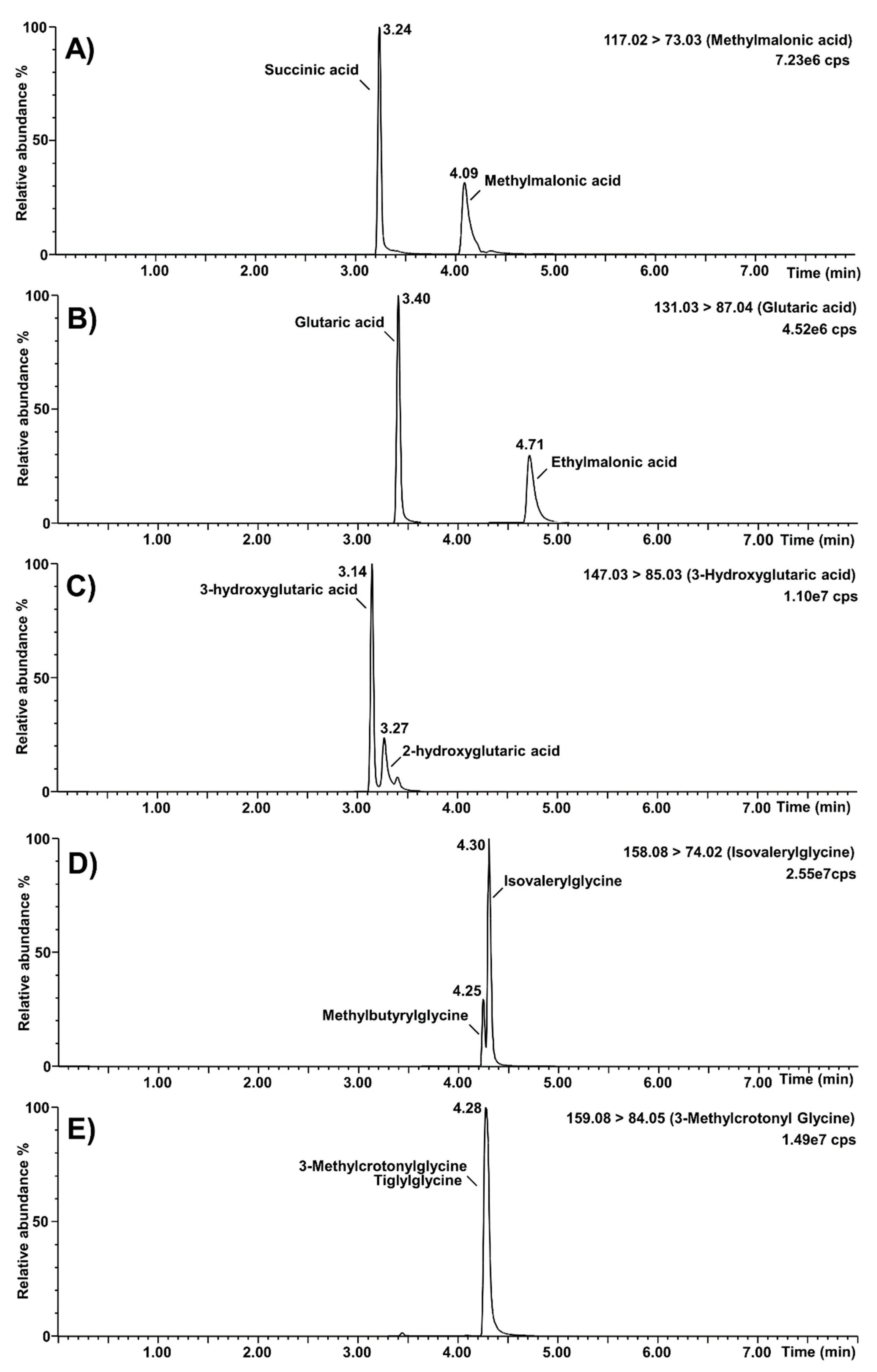
3.1.3. Organic Acids Second-Tier Test
3.2. Validation
3.2.1. Screening Test
3.2.2. Kairos Amino Acid Second-Tier Test
3.2.3. Organic Acids Second-Tier Test
3.3. Reference Values
3.3.1. Screening Test
3.3.2. Kairos Amino Acids Second-Tier Test
3.3.3. Organic Acids Second-Tier Test
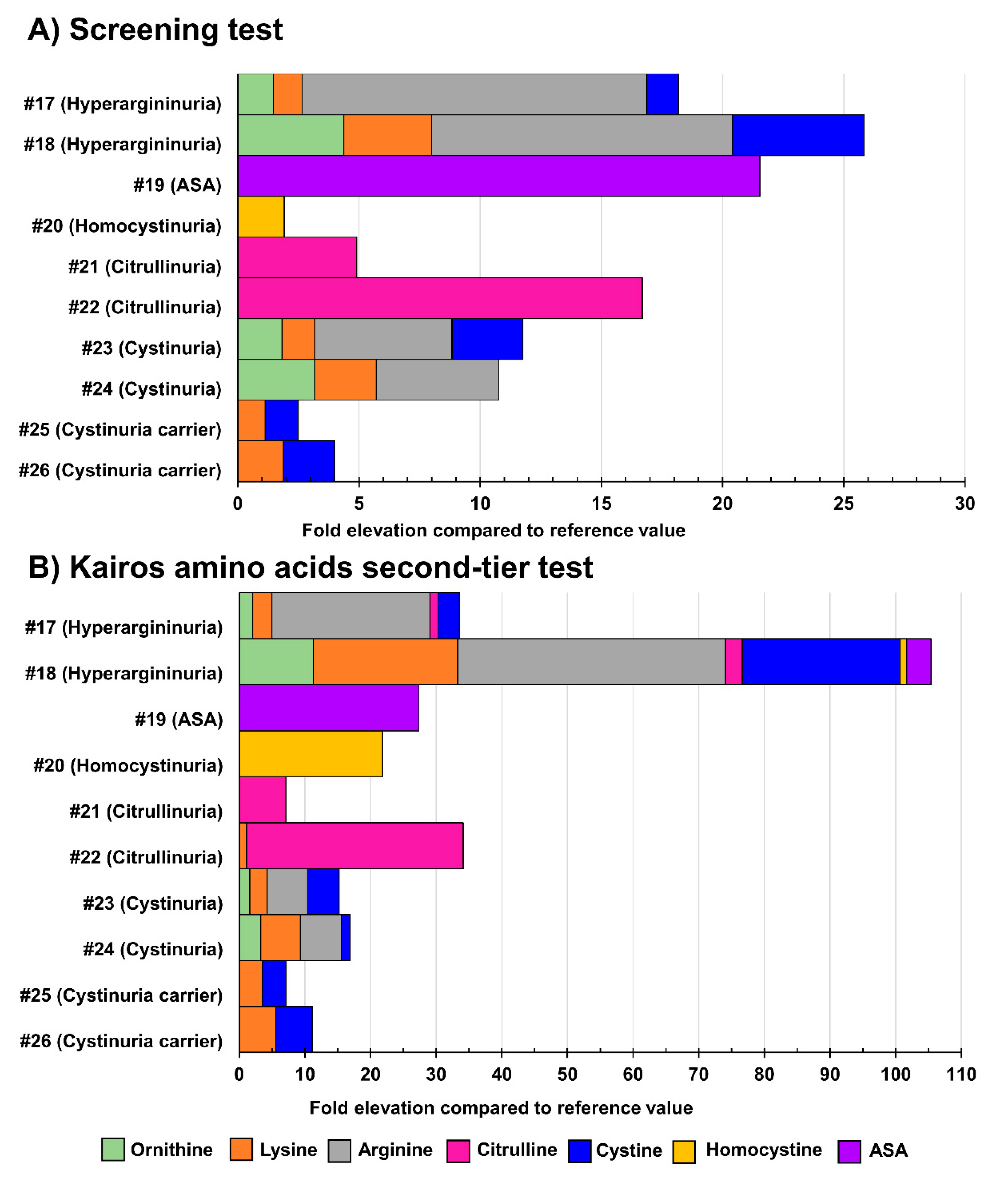
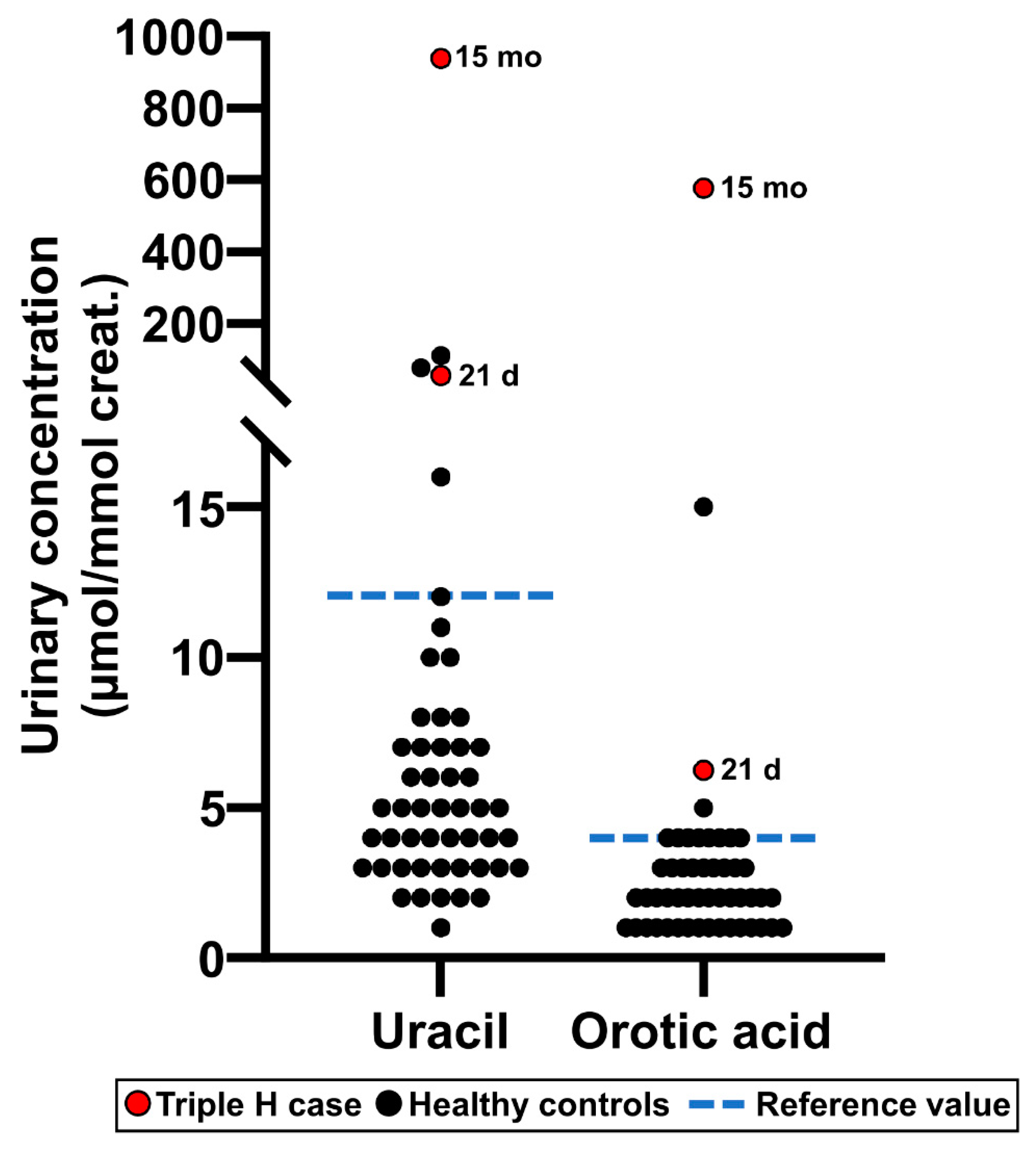
3.4. Analysis of Positive Cases
3.5. Comparison of Methods for Amino Acids and Organic Acids
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| NBS | Newborn screening |
| IEM | Inborn errors of metabolism |
| QNGM | Quebec Network of Genetic Medicine |
| DBS | Dried blood spot |
| DUS | Dried urine spot |
| TLC | Thin layer chromatography |
| Triple H | Hyperornithinemia-hyperammonemia-homocitrullinuria |
| QNSP | Quebec Neuroblastoma Screening Project |
| NIH | National Institutes of Health |
| HVA | Homovanillic acid |
| VMA | Vanillylmandelic acid |
| QCs | Quality controls |
| MS/MS | Tandem mass spectrometry |
| LC-MS/MS | Liquid chromatography-tandem mass spectrometry |
| CID | Collision-induced dissociation |
| IS | Internal standard |
| REB | Research Ethics Board |
| CIUSSSE-CHUS | Centre intégré universitaire de santé et de services sociaux de l’Estrie-Centre hospitalier universitaire de Sherbrooke |
| CMMA | Combined malonic and methylmalonic aciduria |
| ASA | Argininosuccinic aciduria |
| HCl | Hydrochloric acid |
| IQA | Internal quality assurance |
| ERNDIM | European Research Network for Evaluation and Improvement of Screening, Diagnosis, and Treatment of Inborn Errors of Metabolism |
| LOQ | Limit of quantitation |
| UHPLC-MS/MS | Ultra-high performance liquid chromatography tandem mass spectrometry |
| MRM | Multiple reaction monitoring |
| RRF | Relative Response Factor |
| LOD | Limits of detection |
| BSTFA | N,O-Bis(trimethylsilyl)trifluoroacetamide |
References
- Scriver, C.R. Community Genetics and Dignity in Diversity in the Quebec Network of Genetic Medicine. Public Heal. Genom. 2006, 9, 142–152. [Google Scholar] [CrossRef] [PubMed]
- Lemieux, B.; Auray-Blais, C.; Giguère, R.; Shapcott, D.; Scriver, C.R. Newborn Urine Screening Experience with over one Million Infants in the Quebec Network of Genetic Medicine. J. Inherit. Metab. Dis. 1988, 11, 45–55. [Google Scholar] [CrossRef] [PubMed]
- Auray-Blais, C.; Cyr, D.; Drouin, R. Quebec neonatal mass urinary screening programme: From micromolecules to macromolecules. J. Inherit. Metab. Dis. 2007, 30, 515–521. [Google Scholar] [CrossRef]
- Auray-Blais, C.; Giguère, R.; Lemieux, B. Newborn urine screening programme in the province of Quebec: An update of 30 years’ experience. J. Inherit. Metab. Dis. 2003, 26, 393–402. [Google Scholar] [CrossRef]
- Auray-Blais, C.; Giguère, R.; Draper, P.; Shapcott, D.; Lemieux, B. Simple and Rapid System for Screening and Identification of Reducing Sugars in Urine. Clin. Biochem. 1978, 11, 235–237. [Google Scholar] [CrossRef]
- Auray-Blais, C.; Giguère, R.; Paradis, D.; Lemieux, B. Rapid Thin-Layer Chromatographic Method for the Detection of Urinary Methylmalonic Acid. Clin. Biochem. 1979, 12, 43–45. [Google Scholar] [CrossRef]
- Paradis, D.; Giguère, R.; Auray-Blais, C.; Draper, P.; Lemieux, B. An Automated Method for the Determination of Orotic Acid in the Urine of Children Being Screened for Metabolic disorders. Clin. Biochem. 1980, 13, 160–163. [Google Scholar] [CrossRef]
- Debray, F.-G.; Lambert, M.; Lemieux, B.; Soucy, J.F.; Drouin, R.; Fenyves, D.; Dubé, J.; Maranda, B.; Laframboise, R.; Mitchell, G.A. Phenotypic variability among patients with hyperornithinaemia-hyperammonaemia-homocitrullinuria syndrome homozygous for the delF188 mutation in SLC25A15. J. Med. Genet. 2008, 45, 759–764. [Google Scholar] [CrossRef]
- Sokoro, A.A.; Lepage, J.; Antonishyn, N.; McDonald, R.; Rockman-Greenberg, C.; Irvine, J.; Lehotay, D.C. Diagnosis and high incidence of hyperornithinaemia-hyperammonaemia-homocitrullinuria (HHH) syndrome in northern Saskatchewan. J. Inherit. Metab. Dis. 2010, 33, S275–S281. [Google Scholar] [CrossRef] [PubMed]
- Häberle, J.; Burlina, A.; Chakrapani, A.; Dixon, M.; Karall, D.; Lindner, M.; Mandel, H.; Martinelli, D.; Pintos-Morell, G.; Santer, R.; et al. Suggested guidelines for the diagnosis and management of urea cycle disorders: First revision. J. Inherit. Metab. Dis. 2019, 42, 1192–1230. [Google Scholar] [CrossRef] [PubMed]
- Scriver, C.R.; Gregory, D.; Bernstein, M.; Clow, C.L.; Weisdorf, T.; Dougherty, G.E.; Auray-Blais, C.; Giguère, R.; Lemieux, B.; Laberge, C. Feasibility of chemical screening of urine for neuroblastoma case finding in infancy in Quebec. CMAJ 1987, 136, 952–956. [Google Scholar] [PubMed]
- Tuchman, M.; Auray-Blais, C.; Ramnaraine, M.L.; Neglia, J.; Krivit, W.; Lemieux, B. Determination of urinary homovanillic and vanillylmandelic acids from dried filter paper samples: Assessment of potential methods for neuroblastoma screening. Clin. Biochem. 1987, 20, 173–177. [Google Scholar] [CrossRef]
- Woods, W.G.; Gao, R.-N.; Shuster, J.J.; Robison, L.L.; Bernstein, M.; Weitzman, S.; Bunin, G.; Levy, I.; Brossard, J.; Dougherty, G.; et al. Screening of Infants and Mortality Due to Neuroblastoma. New Engl. J. Med. 2002, 346, 1041–1046. [Google Scholar] [CrossRef] [PubMed]
- Soderstrom, L.; Woods, W.G.; Bernstein, M.; Robison, L.L.; Tuchman, M.; Lemieux, B. Health and Economic Benefits of Well-Designed Evaluations: Some Lessons From Evaluating Neuroblastoma Screening. J. Natl. Cancer Inst. 2005, 97, 1118–1124. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Woods, W.G.; Tuchman, M.; Robison, L.L.; Bernstein, M.; Leclerc, J.-M.; Brisson, L.C.; Brossard, J.; Hill, G.; Shuster, J.; Luepker, R.; et al. A population-based study of the usefulness of screening for neuroblastoma. Lancet 1996, 348, 1682–1687. [Google Scholar] [CrossRef]
- Barrette, S.; Bernstein, M.L.; Leclerc, J.-M.; Champagne, M.A.; Samson, Y.; Brossard, J.; Woods, W.G. Treatment Complications in Children Diagnosed With Neuroblastoma During a Screening Program. J. Clin. Oncol. 2006, 24, 1542–1545. [Google Scholar] [CrossRef]
- Giguère, R.; Auray-Blais, C.; Draper, P.; Lemieux, B. Diet and medications giving positive ninhydrin reactions on TLC in a newborn urinary screening program. Clin. Biochem. 1980, 13, 103–105. [Google Scholar] [CrossRef]
- Seger, C.; Salzmann, L. After another decade: LC–MS/MS became routine in clinical diagnostics. Clin. Biochem. 2020, 82, 2–11. [Google Scholar] [CrossRef]
- Millington, D.S. The Role of Technology in Newborn Screening. North Carol. Med. J. 2019, 80, 49–53. [Google Scholar] [CrossRef]
- Thompson, J.W.; Zhang, H.; Smith, P.; Hillman, S.; Moseley, M.A.; Millington, D.S. Extraction and analysis of carnitine and acylcarnitines by electrospray ionization tandem mass spectrometry directly from dried blood and plasma spots using a novel autosampler. Rapid Commun. Mass 2012, 26, 2548–2554. [Google Scholar] [CrossRef] [PubMed]
- Chace, D.H.; Kalas, T.A.; Naylor, E.W. Use of Tandem Mass Spectrometry for Multianalyte Screening of Dried Blood Specimens from Newborns. Clin. Chem. 2003, 49, 1797–1817. [Google Scholar] [CrossRef] [PubMed]
- Auray-Blais, C.; Maranda, B.; Lavoie, P. High-throughput tandem mass spectrometry multiplex analysis for newborn urinary screening of creatine synthesis and transport disorders, Triple H syndrome and OTC deficiency. Clin. Chim. Acta 2014, 436, 249–255. [Google Scholar] [CrossRef] [PubMed]
- Rossiter, P.; Dominguez, J.S.; Warren, J.; Breen, N.; Carlton, L. UPLC-MS/MS Analysis of 45 Amino Acids using the Kairos Amino Acid Kit for Biomedical Research, Waters application note. Available online: https://www.waters.com/webassets/cms/library/docs/720006487en.pdf (accessed on 19 March 2021).
- Boutin, M.; Presse, N.; Martineau, T.; Perreault, A.; Gaudreau, P.; Auray-Blais, C. Mass spectrometry analysis of urinary methylmalonic acid to screen for metabolic vitamin B12 deficiency in older adults. Bioanal. 2020, 12, 693–705. [Google Scholar]
- Bioanalytical Method Validation Guidance for Industry from the U.S. Food and Drug Administration (FDA), May 2018. Available online: www.fda.gov/regulatory-information/search-fda-guidance-documents/bioanalytical-method-validation-guidance-industry (accessed on 19 March 2021).
- Rebollido-Fernandez, M.M.; Castiñeiras, D.E.; Bóveda, M.D.; Couce, M.L.; Cocho, J.A.; Fraga, J.M. Development of electrospray ionization tandem mass spectrometry methods for the study of a high number of urine markers of inborn errors of metabolism. Rapid Commun. Mass Spectrom. 2012, 26, 2131–2144. [Google Scholar] [CrossRef]
- Goodman, S.I.; Markey, S.P. Diagnosis of organic acidemias by gas chromatography—mass spectrometry. Lab. Res. Methods Boil. Med. 1981, 6, 1–158. [Google Scholar]
- Chasson, A.L.; Grady, H.J.; Stanley, M.A. Determination of creatinine by means of automatic chemical analysis. Tech. Bull. Regist. Med. Technol. 1960, 30, 207–212. [Google Scholar] [CrossRef] [PubMed]
- Pitt, J.J.; Eggington, M.; Kahler, S.G. Comprehensive Screening of Urine Samples for Inborn Errors of Metabolism by Electrospray Tandem Mass Spectrometry. Clin. Chem. 2002, 48, 1970–1980. [Google Scholar] [CrossRef]
- Embade, N.; Cannet, C.; Diercks, T.; Gil-Redondo, R.; Bruzzone, C.; Ansó, S.; Echevarría, L.R.; Ayucar, M.M.M.; Collazos, L.; Lodoso, B.; et al. NMR-based newborn urine screening for optimized detection of inherited errors of metabolism. Sci. Rep. 2019, 9, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, A.D.; Miller, M.J.; Beebe, K.; Wulff, J.E.; Evans, A.M.; Miller, L.A.; Sutton, V.R.; Sun, Q.; Elsea, S.H. Metabolomic Profiling of Human Urine as a Screen for Multiple Inborn Errors of Metabolism. Genet. Test. Mol. Biomarkers 2016, 20, 485–495. [Google Scholar] [CrossRef] [PubMed]
- Couce, M.L.; Castiñeiras, D.E.; Bóveda, M.D.; Baña, A.; Cocho, J.A.; Iglesias, A.J.; Colón, C.; Alonso-Fernández, J.R.; Fraga, J.M. Evaluation and long-term follow-up of infants with inborn errors of metabolism identified in an expanded screening programme. Mol. Genet. Metab. 2011, 104, 470–475. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Disorders | OMIM No. | Targeted Biomarkers |
| Organic acidurias | ||
| Methylmalonic aciduria(s) | ||
| cblA type | 251,100 | Methylmalonic acid↑, 2-Methylcitric acid↑ |
| cblB type | 251,110 | Methylmalonic acid↑, 2-Methylcitric acid↑ |
| cblC type | 277,400 | Methylmalonic acid↑, 2-Methylcitric acid↑, Homocystine↑ |
| cblD type | 277,410 | Methylmalonic acid↑, 2-Methylcitric acid↑, Homocystine↑ |
| cblF type | 277,380 | Methylmalonic acid↑, 2-Methylcitric acid↑, Homocystine↑ |
| mut type | 251,000 | Methylmalonic acid↑, 2-Methylcitric acid↑ |
| Combined malonic and methylmalonic aciduria (CMAMMA) | 614,265 | Methylmalonic acid↑, 2-Methylcitric acid↑, Malonic acid↑ |
| Propionic aciduria | 606,054 | Propionylglycine↑, 2-Methylcitric acid↑, 3-Hydroxypropionic acid↑ |
| Isovaleric aciduria | 243,500 | Isovalerylglycine↑, 3-Hydroxyisovaleric acid↑ |
| Glutaric aciduria type 1 | 231,670 | Glutaric acid↑, 3-Hydroxyglutaric acid↑ |
| Alkaptonuria | 203,500 | Homogentisic acid↑ |
| 3-Methylcrotonylglycinuria type I | 210,200 | 3-Methylcrotonylglycine↑, 3-Hydroxyisovaleric acid↑ |
| Urea cycle disorders | ||
| Argininosuccinic aciduria | 207,900 | Argininosuccinic acid↑ |
| Hyperargininuria | 207,800 | Arginine↑ |
| Citrullinuria, classic | 215,700 | Citrulline↑ |
| Citrullinuria type II | 605,814 | Citrulline↑ |
| Triple H syndrome | 238,970 | Orotic acid↑, Uracil↑, |
| Disorders of amino acid transport | ||
| Cystinuria | 220,100 | Cystine↑, Ornithine↑, Lysine↑, Arginine↑ |
| Disorders of amino acid metabolism | ||
| Homocystinuria | 236,200 | Homocystine↑ |
| Creatine synthesis and transport disorders | ||
| Guanidinoacetate methyltransferase deficiency (GAMT) | 601,240 | Creatine↓, Guanidineacetic acid↑ |
| Arginine:glycine amidinotransferase deficiency (AGAT) | 602,360 | Creatine↓, Guanidineacetic acid↓ |
| Creatine transporter deficiency (CRTR) | 300,352 | Creatine↑ |
| UHPLC Parameters | |
| Analysis mode | Flow injection (no chromatography) |
| Mobile phase | 95:5 H2O:ACN + 0.1% F.A. (isocratic) |
| Weak wash solvent | H2O + 0.1% F.A. |
| Strong wash solvent | H2O + 0.1% F.A. |
| Injection volume | 10 µL |
| Injector type | Flow through needle |
| Flow rates | 0.00 → 0.22 min: 0.100 mL/min |
| 0.22 → 1.20 min: 0.015 mL/min | |
| 1.20 → 2.00 min: 0.500 mL/min | |
| MS Parameters | |
| Ionization mode | Electrospray (ESI) |
| Acquisition mode | Multiple reaction monitoring (MRM) |
| Capillary Voltage | ESI(−): 2.00 kV; ESI(+): 2.00 kV |
| Desolvation temperature | 200 °C |
| Desolvation gas flow | 1000 L/h |
| Cone gas flow | 10 L/h |
| Source temperature | 150 °C |
| Span | 0.1 Da |
| Dwell time | 14 ms |
| UHPLC Parameters | |
| Column | Atlantis PREMIER BEH C18 AX VanGuard FIT |
| ID x Length | 2.1 × 100 mm |
| Particle size | 1.7 µm |
| Column temperature | 30 °C |
| Mobile phase A | 40:60 ACN:H2O 30 mM Amm. Form. + 0.9% F.A. |
| Mobile phase B | 95:5 H2O:ACN |
| Gradient | |
| Flow rate (mL/min) | Mobile phase % |
| 0.350 | 0.00 → 1.50 min: 100%B |
| 0.350 | 1.50 → 5.00 min: 100 → 0%B (linear) |
| 0.350 | 5.00 → 7.00 min: 0%B |
| 0.350 | 7.00 → 7.10 min: 0 → 100%B (linear) |
| 0.350 | 7.10 → 8.00 min: 100%B |
| Weak wash solvent | H2O |
| Strong wash solvent | H2O |
| Injection volume | 10 µL |
| Injector type | Flow through needle |
| Autosampler temperature | 10 °C |
| MS Parameters | |
| Ionization mode | Electrospray (ESI) |
| Acquisition mode | Multiple reaction monitoring (MRM) |
| Capillary Voltage | ESI(+): 0.50 kV; ESI(−): 0.60 kV |
| Desolvation temperature | 500 °C |
| Desolvation gas flow | 750 L/h |
| Cone gas flow | 0 L/h |
| Source temperature | 150 °C |
| Span | 0.1 Da |
| Biomarker | Median | 1st Centile | 99th Centile | 99.9th Centile | Cut-Off Min. | Cut-Off Max. | Positive Rate |
|---|---|---|---|---|---|---|---|
| µmol/mmol Creat. | µM | µmol/mmol Creat. | µmol/mmol Creat. | µM | µmol/mmol Creat. | % | |
| Creatinine (µM) | 78.88 | 22.91 | -- | -- | 0.6 | -- | 0.08 |
| Creatinine ratio (no unit) | 1.28 | 1.19 | 1.39 | 1.42 | 1.15 | 1.51 | 0.46 |
| Creatine | 185.68 | -- | 800.49 | 1057.59 | -- | 1000 | 0.18 |
| Guanidineacetic acid | 127.03 | -- | 249.89 | 319.71 | -- | 290 | 0.30 |
| Guanidineacetic acid/creatine ratio (no unit) | 0.72 | -- | 3.53 | 4.47 | -- | 4.40 | 0.13 |
| 3-Methylcrotonylglycine | 7.68 | -- | 29.98 | 70.37 | -- | 60 | 0.18 |
| Uracil | 26.83 | -- | 78.36 | 150.68 | -- | 55 | 4.87 |
| Propionylglycine | 2.58 | -- | 13.20 | 31.00 | -- | 40 | 0.09 |
| Malonic acid | 32.81 | -- | 114.92 | 364.74 | -- | 200 | 0.22 |
| 3-Hydroxyglutaric acid | 20.34 | -- | 39.24 | 61.61 | -- | 60 | 0.15 |
| 3-Hydroxyisovaleric acid | 14.58 | -- | 59.50 | 113.48 | -- | 150 | 0.05 |
| Glutaric acid | 23.17 | -- | 58.38 | 109.90 | -- | 200 | 0.05 |
| Orotic acid | 11.20 | -- | 35.00 | 97.63 | -- | 43 | 0.63 |
| N-Isovalerylglycine | 1.52 | -- | 4.31 | 6.87 | -- | 15 | 0.05 |
| 2-Methylcitric acid | 6.56 | -- | 16.74 | 32.22 | -- | 38 | 0.09 |
| 3-Hydroxypropionic acid | 13.38 | -- | 89.30 | 259.18 | -- | 140 | 0.45 |
| Methylmalonic acid | 8.37 | -- | 104.29 | 250.78 | -- | 150 | 0.55 |
| Homogentisic acid | 2.87 | -- | 11.14 | 16.90 | -- | 100 | 0.00 |
| Ornithine | 43.42 | -- | 267.96 | 564.87 | -- | 350 | 0.49 |
| Lysine | 289.74 | -- | 873.09 | 1441.75 | -- | 1100 | 0.40 |
| Arginine | 25.71 | -- | 131.89 | 254.65 | -- | 200 | 0.33 |
| Argininosuccinic acid | 4.17 | -- | 11.82 | 18.54 | -- | 50 | 0.00 |
| Citrulline | 21.28 | -- | 172.08 | 391.92 | -- | 250 | 0.42 |
| Cystine | 27.15 | -- | 138.36 | 339.19 | -- | 200 | 0.43 |
| Homocystine | 2.02 | -- | 6.00 | 13.28 | -- | 14 | 0.12 |
| Biomarker | Minimum | Maximum | Median | 5th Percentile | 95th Percentile |
|---|---|---|---|---|---|
| µmol/mmol Creat. | µmol/mmol Creat. | µmol/mmol Creat. | µmol/mmol Creat. | µmol/mmol Creat. | |
| Taurine | 58 | 1362 | 645 | 181 | 1253 |
| Aspartic acid | 0 | 880 | 51 | 9 | 235 |
| Hydroxyproline | 65 | 1173 | 420 | 139 | 949 |
| Threonine | 28 | 741 | 160 | 54 | 549 |
| Serine | 0 | 1520 | 451 | 238 | 1145 |
| Asparagine | 0 | 237 | 67 | 0 | 170 |
| Glutamic acid | 11 | 275 | 46 | 15 | 193 |
| Glutamine | 103 | 691 | 301 | 144 | 533 |
| Sarcosine | 0 | 29 | 0 | 0 | 15 |
| Alpha Aminoadipic Acid | 0 | 104 | 13 | 0 | 57 |
| Proline | 47 | 773 | 210 | 56 | 643 |
| Glycine | 435 | 3366 | 1762 | 759 | 2781 |
| Alanine | 139 | 837 | 343 | 154 | 733 |
| Citrulline | 5 | 126 | 29 | 9 | 106 |
| Alpha Aminobutyric Acid | 0 | 0 | 0 | 0 | 0 |
| Valine | 3 | 220 | 33 | 12 | 137 |
| Cystine | 8 | 99 | 30 | 11 | 80 |
| Methionine | 0 | 52 | 0 | 0 | 15 |
| Homocitrulline | 0 | 93 | 0 | 0 | 52 |
| Allo-Isoleucine | 0 | 0 | 0 | 0 | 0 |
| Cystathionine | 0 | 21 | 0 | 0 | 10 |
| Isoleucine | 0 | 1075 | 10 | 0 | 66 |
| Leucine | 0 | 274 | 29 | 4 | 103 |
| Argininosuccinic Acid | 0 | 80 | 9 | 0 | 42 |
| Tyrosine | 0 | 150 | 58 | 24 | 104 |
| Beta Alanine | 0 | 105 | 27 | 3 | 85 |
| Phenylalanine | 0 | 103 | 21 | 3 | 53 |
| Beta Aminoisobutyric Acid | 0 | 943 | 8 | 0 | 226 |
| Homocystine | 0 | 0 | 0 | 0 | 0 |
| Gamma Aminobutyric Acid | 6 | 54 | 19 | 7 | 44 |
| L-Ornithine | 2 | 376 | 42 | 9 | 257 |
| Lysine | 11 | 505 | 121 | 37 | 282 |
| 1-Methyl Histidine | 0 | 156 | 0 | 0 | 96 |
| Histidine | 0 | 371 | 177 | 0 | 319 |
| 3-Methyl Histidine | 0 | 133 | 0 | 0 | 50 |
| Carnosine | 0 | 222 | 74 | 0 | 157 |
| Arginine | 25 | 210 | 49 | 27 | 110 |
| Ethanolamine | 55 | 983 | 208 | 89 | 566 |
| Phosphoethanolamine | 0 | 60 | 13 | 0 | 45 |
| Hydroxylysine | 0 | 40 | 10 | 0 | 26 |
| Glycyl proline | 0 | 51 | 19 | 0 | 36 |
| S-Sulfocysteine | 0 | 0 | 0 | 0 | 0 |
| Anserine | 0 | 80 | 30 | 0 | 66 |
| Kynurenine | 0 | 0 | 0 | 0 | 0 |
| Tryptophan | 10 | 66 | 30 | 15 | 53 |
| Biomarker | Minimum | Maximum | Median | 5th Percentile | 95th Percentile |
|---|---|---|---|---|---|
| µmol/mmol Creat. | µmol/mmol Creat. | µmol/mmol Creat. | µmol/mmol Creat. | µmol/mmol Creat. | |
| Guanidineacetic acid | 56 | 257 | 108 | 64 | 187 |
| Guanidineacetic acid/creatine ratio (no unit) | 0.23 | 3.74 | 0.88 | 0.25 | 3.18 |
| 3-Methylcrotonylglycine | 1 | 9 | 3 | 1 | 8 |
| Creatine | 23 | 755 | 144 | 26 | 581 |
| Creatinine | 44 | 270 | 127 | 51 | 228 |
| Orotic acid | 1 | 5 | 2 | 1 | 4 |
| Methylmalonic acid | 0 | 33 | 6 | 0 | 26 |
| Glutaric acid | 0 | 41 | 8 | 0 | 26 |
| 3-Hydroxyisovaleric acid | 1 | 52 | 10 | 2 | 29 |
| 3-Hydroxyglutaric acid | 0 | 12 | 2 | 0 | 9 |
| Malonic acid | 1 | 29 | 6 | 2 | 23 |
| Isovalerylglycine | 0 | 4 | 2 | 0 | 4 |
| 2-Methylcitric acid | 0 | 29 | 8 | 0 | 23 |
| Uracil | 1 | 16 | 5 | 2 | 12 |
| Propionylglycine | 0 | 1 | 0 | 0 | 1 |
| 3-Hydroxypropionic acid | 6 | 68 | 17 | 7 | 62 |
| Homogentisic acid | 0 | 2 | 0 | 0 | 2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Auray-Blais, C.; Boutin, M.; Lavoie, P.; Maranda, B. Neonatal Urine Screening Program in the Province of Quebec: Technological Upgrade from Thin Layer Chromatography to Tandem Mass Spectrometry. Int. J. Neonatal Screen. 2021, 7, 18. https://doi.org/10.3390/ijns7010018
Auray-Blais C, Boutin M, Lavoie P, Maranda B. Neonatal Urine Screening Program in the Province of Quebec: Technological Upgrade from Thin Layer Chromatography to Tandem Mass Spectrometry. International Journal of Neonatal Screening. 2021; 7(1):18. https://doi.org/10.3390/ijns7010018
Chicago/Turabian StyleAuray-Blais, Christiane, Michel Boutin, Pamela Lavoie, and Bruno Maranda. 2021. "Neonatal Urine Screening Program in the Province of Quebec: Technological Upgrade from Thin Layer Chromatography to Tandem Mass Spectrometry" International Journal of Neonatal Screening 7, no. 1: 18. https://doi.org/10.3390/ijns7010018
APA StyleAuray-Blais, C., Boutin, M., Lavoie, P., & Maranda, B. (2021). Neonatal Urine Screening Program in the Province of Quebec: Technological Upgrade from Thin Layer Chromatography to Tandem Mass Spectrometry. International Journal of Neonatal Screening, 7(1), 18. https://doi.org/10.3390/ijns7010018