Is Newborn Screening the Ultimate Strategy to Reduce Diagnostic Delays in Pompe Disease? The Parent and Patient Perspective

Abstract
:1. Introduction
2. Diagnostic Delay
- Classic IOPD patients—cardiac function, hearing, muscle strength and motor development were all impaired, one in three (36%) required supplemental oxygen and two in three (64%) required nasogastric tube feeding;
- LOPD patients—advanced muscle weakness and impaired respiratory function were present, causing varying degrees of handicap, and respiratory support (14% of adults) and use of a wheelchair (7% of adults) were required.
2.1. Barriers to Timely Diagnosis—Australian Perspectives
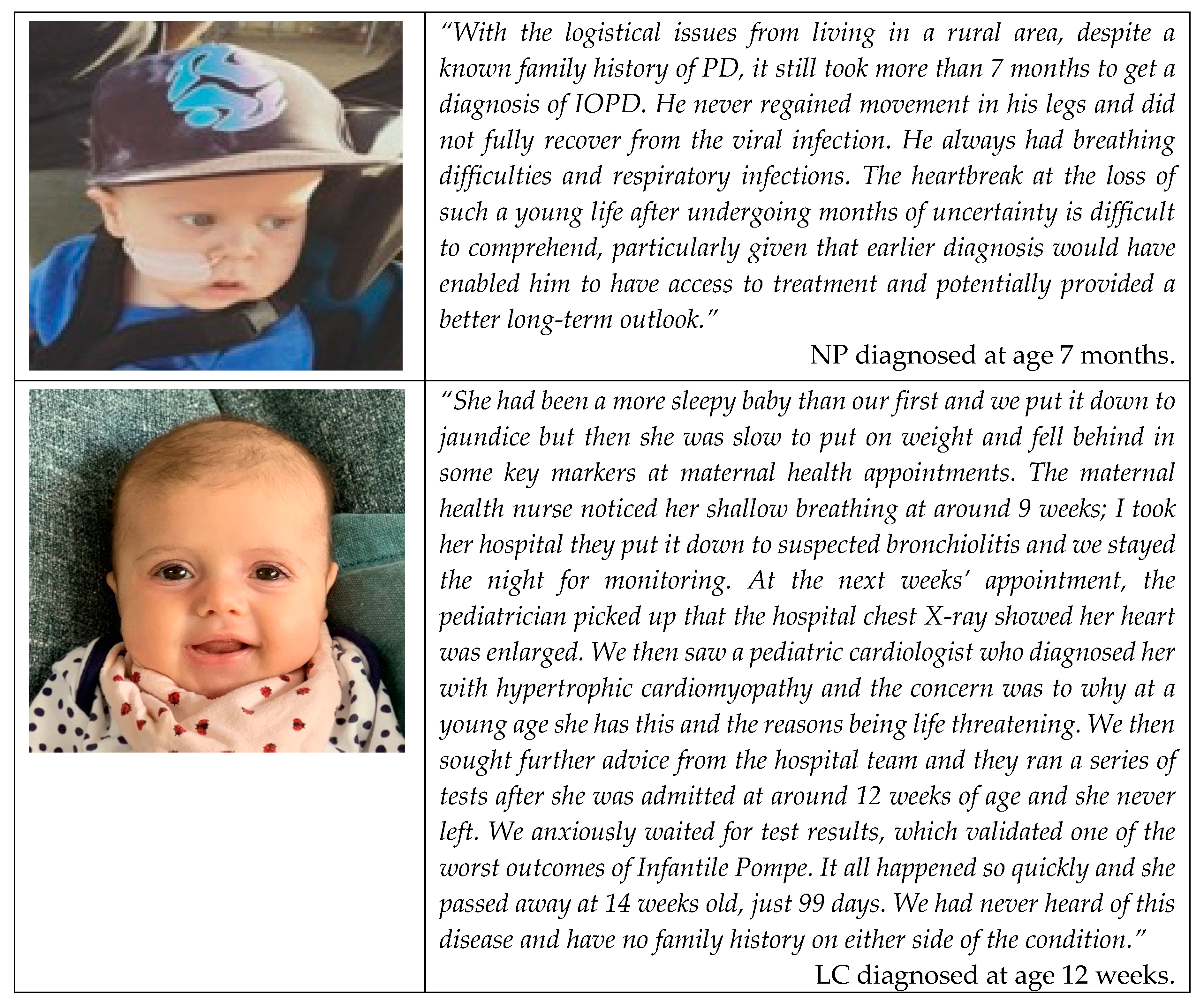
2.2. Diagnostic Delays—Australian IOPD Experiences
3. What Do We Know about NBS for PD?
- The development of promising new treatment options;
- Advances in screening technology;
- Advocacy by special interest groups.
3.1. Benefits of NBS for PD
3.1.1. Reduced Diagnostic Odyssey in IOPD
3.1.2. Greater Knowledge of Reproductive Risk
3.1.3. Improved Understanding of the True Prevalence of PD
3.2. What Have We Learnt from Current PD NBS Programs?
3.3. Impact on Immunomodulation Protocols
3.4. Weighing Prognostic Uncertainty against Informed Decision Making
3.4.1. False Positives
3.4.2. Early Identification of LOPD
“There is much that needs to be done to help people with rare diseases, particularly around raising awareness to the public and also medical professionals in order for early diagnosis and also correcting misdiagnosis to occur. Had I been diagnosed even in 1997 when I was 17 and received treatment as soon as it became available perhaps my life would be very different today.”
4. Specific Considerations for NBS in the Australian Setting
4.1. Current NBS Policies and Processes
4.2. Application to Include PD in the NBS
4.3. Access to Current Therapies in Australia
4.4. Potential Impact of Future Therapies
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Pompe, J.C. Over idiopatische hypertrophie van het hart. Ned. Tijdschr. Geneeskd. 1932, 76, 304. [Google Scholar]
- Angelini, C.; Nascimbeni, A.C.; Semplicini, C. Therapeutic advances in the management of Pompe disease and other metabolic myopathies. Ther. Adv. Neurol. Disord. 2013, 6, 311–321. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lim, J.A.; Li, L.; Raben, N. Pompe disease: From pathophysiology to therapy and back again. Front. Aging Neurosci. 2014, 6, 177. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herzog, A.; Hartung, R.; Reuser, A.J.; Hermanns, P.; Runz, H.; Karabul, N.; Gökce, S.; Pohlenz, J.; Kampmann, C.; Lampe, C.; et al. A cross-sectional single-centre study on the spectrum of Pompe disease, German patients: Molecular analysis of the GAA gene, manifestation and genotype-phenotype correlations. Orphanet J. Rare Dis. 2012, 7, 35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kemper, A.R.; Comeau, A.M.; Green, N.S.; Goldenberg, A.; Ojodu, J.; Prosser, L.A.; Tanksley, S.; Weinreich, S.; Lam, K.K. The Condition Review Workgroup. Evidence Report: Newborn Screening for Pompe Disease; US Department of Health and Human Services: Rockville, MD, USA, 2013. Available online: http://www.hrsa.gov/advisorycommittees/mchbadvisory/heritabledisorders/nominatecondition/reviews/pompereport2013.pdf (accessed on 18 November 2019).
- Kishnani, P.S.; Steiner, R.D.; Bali, D.; Berger, K.; Byrne, B.J.; Case, L.E. Pompe disease diagnosis and management guideline. Genet. Med. 2006, 8, 267–288. [Google Scholar] [CrossRef] [Green Version]
- Toscano, A.; Montagnese, F.; Musumeci, O. Early is better? A new algorithm for early diagnosis in late onset Pompe disease (LOPD). Acta Myol. 2013, 32, 78–81. [Google Scholar]
- Kishnani, P.S.; Amartino, H.M.; Lindberg, C.; Miller, T.M.; Wilson, A.; Keutzer, J. Timing of diagnosis of patients with Pompe disease: Data from the Pompe registry. Am. J. Med. Genet. A 2013, 161A, 2431–2443. [Google Scholar] [CrossRef]
- Prosser, L.A.; Lam, K.K.; Grosse, S.D.; Casale, M.; Kemper, A.R. Using Decision Analysis to Support Newborn Screening Policy Decisions: A Case Study for Pompe Disease. MDM Policy Pract. 2018, 3. [Google Scholar] [CrossRef] [Green Version]
- Owens, P.; Wong, M.; Bhattacharya, K.; Ellaway, C. Infantile-onset Pompe disease: A case series highlighting early clinical features, spectrum of disease severity and treatment response. J. Paediatr. Child Health 2018, 54, 1255–1261. [Google Scholar] [CrossRef]
- Rigter, T.; Weinreich, S.S.; van El, C.G.; de Vries, J.M.; van Gelder, C.M.; Gungor, D.; Reuser, A.J.J.; Hagemans, M.L.C.; Cornel, M.C.; van der Ploeg, A.T.; et al. Severely impaired health status at diagnosis of Pompe disease: A cross-sectional analysis to explore the potential utility of neonatal screening. Mol. Genet. Metab. 2012, 107, 448–455. [Google Scholar] [CrossRef]
- Zurynski, Y.; Deverell, M.; Dalkeith, T.; Johnson, S.; Christodoulou, J.; Leonard, H.; Elliott, E.J. Australian children living with rare diseases: Experiences of diagnosis and perceived consequences of diagnostic delays. Orphanet J. Rare Dis. 2017, 12, 68. [Google Scholar] [CrossRef] [PubMed]
- Molster, C.; Urwin, D.; Di Pietro, L.; Fookes, M.; Petrie, D.; van der Laan, S.; Dawkins, H. Survey of healthcare experiences of Australian adults living with rare diseases. Orphanet J. Rare Dis. 2016, 11, 30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lagler, F.B.; Moder, A.; Rohrbach, M.; Hennermann, J.; Mengel, E.; Gökce, S.; Hundsberger, T.; Rösler, K.M.; Karabul, N.; Huemer, M.; et al. Extent, impact, and predictors of diagnostic delay in Pompe disease: A combined survey approach to unveil the diagnostic odyssey. JIMD Rep. 2019, 49, 89–95. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Di Iorio, G.; Cipullo, F.; Stromillo, L.; Sodano, L.; Capone, E.; Farina, O. S1.3 Adult-onset Pompe disease. Acta Myol. 2011, 30, 200–202. [Google Scholar]
- Burton, B.K.; Kronn, D.F.; Hwu, W.-L.; Kishnani, P.S. The Initial Evaluation of Patients After Positive Newborn Screening: Recommended Algorithms Leading to a Confirmed Diagnosis of Pompe Disease. Pediatrics 2017, 140, S14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Millington, D.S.; Bali, D. Current state of the art of newborn screening for lysosomal storage disorders. Int. J. Neonatal Screen. 2018, 4, 24. [Google Scholar] [CrossRef] [Green Version]
- Millington, D.S. The Role of Technology in Newborn Screening. N. C. Med. J. 2019, 80, 49–53. [Google Scholar] [CrossRef]
- Baker, M.; Griggs, R.; Byrne, B.; Connolly, A.M.; Finkel, R.; Grajkowska, L.; Haidet-Phillips, A.; Hagerty, L.; Ostrander, R.; Orlando, L.; et al. Maximizing the Benefit of Life-Saving Treatments for Pompe Disease, Spinal Muscular Atrophy, and Duchenne Muscular Dystrophy Through Newborn Screening: Essential Steps. JAMA Neurol. 2019, 76, 978–983. [Google Scholar] [CrossRef]
- Newborn Screening Technical Assistance and Evaluation Program (NewSTEPs). Disorders Screening Status Map New Steps: US National Newborn Screening Resource Center; Association of Public Health Laboratories: Silver Spring, MD, USA. Available online: https://www.newsteps.org/resources/newborn-screening-status-all-disorders (accessed on 20 November 2019).
- Bodamer, O.A.; Scott, C.R.; Giugliani, R. Newborn Screening for Pompe Disease. Pediatrics 2017, 140, S4. [Google Scholar] [CrossRef] [Green Version]
- Bombard, Y.; Miller, F.A.; Hayeems, R.Z.; Avard, D.; Knoppers, B.M. Reconsidering reproductive benefit through newborn screening: A systematic review of guidelines on preconception, prenatal and newborn screening. Eur. J. Hum. Genet. 2010, 18, 751–760. [Google Scholar] [CrossRef] [Green Version]
- Meikle, P.J.; Hopwood, J.J.; Clague, A.E.; Carey, W.F. Prevalence of lysosomal storage disorders. JAMA 1999, 281, 249–254. [Google Scholar] [CrossRef] [PubMed]
- Health Consult. Review of Life Saving Drugs Program Medicines: Pompe Disease. In Final Review Protocol; Australian Government Department of Health: Canberra, Australia, 2019. Available online: https://www1.health.gov.au/internet/main/publishing.nsf/Content/E959F2C329B6255ACA258308001F0EE1/$File/Review-Protocol-for-Pompe-disease.pdf (accessed on 20 November 2019).
- Chien, Y.H.; Hwu, W.L.; Lee, N.C. Newborn screening: Taiwanese experience. Ann. Transl. Med. 2019, 7, 281. [Google Scholar] [CrossRef] [PubMed]
- Desai, A.K.; Kazi, Z.B.; Bali, D.S.; Kishnani, P.S. Characterization of immune response in Cross-Reactive Immunological Material (CRIM)-positive infantile Pompe disease patients treated with enzyme replacement therapy. Mol. Genet. Metab. Rep. 2019, 20, 100475. [Google Scholar] [CrossRef] [PubMed]
- Chien, Y.H.; Hwu, W.L.; Lee, N.C. Pompe disease: Early diagnosis and early treatment make a difference. Pediatr. Neonatol. 2013, 54, 219–227. [Google Scholar] [CrossRef] [Green Version]
- Yang, C.F.; Yang, C.C.; Liao, H.C.; Huang, L.Y.; Chiang, C.C.; Ho, H.C.; Lai, C.J.; Chu, T.H.; Yang, T.F.; Hsu, T.R.; et al. Very Early Treatment for Infantile-Onset Pompe Disease Contributes to Better Outcomes. J. Pediatr. 2016, 169, 174–180. [Google Scholar] [CrossRef]
- Chien, Y.H.; Lee, N.C.; Chen, C.A.; Tsai, F.J.; Tsai, W.H.; Shieh, J.Y.; Huang, H.J.; Hsu, W.C.; Tsai, T.H.; Hwu, W.L.; et al. Long-term prognosis of patients with infantile-onset Pompe disease diagnosed by newborn screening and treated since birth. J. Pediatr. 2015, 166, 985–991. [Google Scholar] [CrossRef]
- Hahn, A.; Schänzer, A. Long-term outcome and unmet needs in infantile-onset Pompe disease. Ann. Transl. Med. 2019, 7, 283. [Google Scholar] [CrossRef]
- Desai, A.K.; Li, C.; Rosenberg, A.S.; Kishnani, P.S. Immunological challenges and approaches to immunomodulation in Pompe disease: A literature review. Ann. Transl. Med. 2019, 7, 285. [Google Scholar] [CrossRef]
- Poelman, E.; Hoogeveen-Westerveld, M.; van den Hout, J.M.P.; Bredius, R.G.M.; Lankester, A.C.; Driessen, G.J.A.; Kamphuis, S.S.M.; Pijnappel, W.W.M.; van der Ploeg, A.T. Effects of immunomodulation in classic infantile Pompe patients with high antibody titers. Orphanet J. Rare Dis. 2019, 14, 71. [Google Scholar] [CrossRef]
- Matsuoka, T.; Miwa, Y.; Tajika, M.; Sawada, M.; Fujimaki, K.; Soga, T.; Tomita, H.; Uemura, S.; Nishino, I.; Fukuda, T.; et al. Divergent clinical outcomes of alpha-glucosidase enzyme replacement therapy in two siblings with infantile-onset Pompe disease treated in the symptomatic or pre-symptomatic state. Mol. Genet. Metab. Rep. 2016, 9, 98–105. [Google Scholar] [CrossRef]
- Oda, E.; Tanaka, T.; Migita, O.; Kosuga, M.; Fukushi, M.; Okumiya, T.; Osawa, M. Newborn screening for Pompe disease in Japan. Mol. Genet. Metab. 2011, 104, 560–565. [Google Scholar] [CrossRef] [PubMed]
- Goldenberg, A.J.; Comeau, A.M.; Grosse, S.D.; Tanksley, S.; Prosser, L.A.; Ojodu, J.; Botkin, J.R.; Kemper, A.R.; Green, N.S. Evaluating Harms in the Assessment of Net Benefit: A Framework for Newborn Screening Condition Review. Matern. Child Health J. 2016, 20, 693–700. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Minter Baerg, M.M.; Stoway, S.D.; Hart, J.; Mott, L.; Peck, D.S.; Nett, S.L.; Eckerman, J.S.; Lacey, J.M.; Turgeon, C.T.; Gavrilov, D.; et al. Precision newborn screening for lysosomal disorders. Genet. Med. 2018, 20, 847–854. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wasserstein, M.P.; Caggana, M.; Bailey, S.M.; Desnick, R.J.; Edelmann, L.; Estrella, L.; Holzman, I.; Kelly, N.R.; Kornreich, R.; Kupchik, S.G.; et al. The New York pilot newborn screening program for lysosomal storage diseases: Report of the First 65,000 Infants. Genet. Med. 2019, 21, 631–640. [Google Scholar] [CrossRef] [PubMed]
- Chiang, S.C.; Chen, P.W.; Hwu, W.L.; Lee, A.J.; Chen, L.C.; Lee, N.C.; Chiou, L.Y.; Chien, Y.H. Performance of the Four-Plex Tandem Mass Spectrometry Lysosomal Storage Disease Newborn Screening Test: The Necessity of Adding a 2nd Tier Test for Pompe Disease. Int. J. Neonatal Screen. 2018, 4, 41. [Google Scholar] [CrossRef] [Green Version]
- Van El, C.G.; Rigter, T.; Reuser, A.J.; van der Ploeg, A.T.; Weinreich, S.S.; Cornel, M.C. Newborn screening for pompe disease? A qualitative study exploring professional views. BMC Pediatr. 2014, 14, 203. [Google Scholar] [CrossRef] [Green Version]
- Wilcken, B. Newborn Screening for Lysosomal Disease: Mission Creep and a Taste of Things to Come? Int. J. Neonatal Screen. 2018, 4. [Google Scholar] [CrossRef] [Green Version]
- Schoser, B.; Bilder, D.A.; Dimmock, D.; Gupta, D.; James, E.S.; Prasad, S. The humanistic burden of Pompe disease: Are there still unmet needs? A systematic review. BMC Neurol. 2017, 17, 202. [Google Scholar] [CrossRef] [Green Version]
- Reardon, K.; McKelvie, P. 090 The expanding clinical phenotype of late onset pompe disease: A multi-system disorder. JNNP 2018, 89. [Google Scholar] [CrossRef]
- Royal Australian Collge of General Practitioners. Genomics in General Practice; RACGP: East Melbourne, Australia, 2018; Available online: https://www.racgp.org.au/download/Documents/Guidelines/Genomics-in-general-practice.pdf (accessed on 20 November 2019).
- O’Leary, P.; Maxwell, S. Newborn bloodspot screening policy framework for Australia. Australas. Med. J. 2015, 8, 292–298. [Google Scholar] [CrossRef]
- White, C. Newborn Bloodspot Screening Working Group: Newborn Bloodspot Screening National Policy Framework; Australian Government Department of Health: Canberra, Australia, 2018. Available online: http://www.cancerscreening.gov.au/internet/screening/publishing.nsf/Content/newborn-bloodspot-screening (accessed on 5 December 2019).
- Schoser, B.; Hahn, A.; James, E.; Gupta, D.; Gitlin, M.; Prasad, S. A Systematic Review of the Health Economics of Pompe Disease. Pharm. Open 2019, 3, 479–493. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kishnani, P.S.; Beckemeyer, A.A. New therapeutic approaches for Pompe disease: Enzyme replacement therapy and beyond. Pediatr. Endocrinol. Rev. 2014, 12, 114–124. [Google Scholar] [PubMed]
- Ronzitti, G.; Collaud, F.; Laforet, P.; Mingozzi, F. Progress and challenges of gene therapy for Pompe disease. Ann. Transl. Med. 2019, 7, 287. [Google Scholar] [CrossRef] [PubMed]
- Salabarria, S.M.; Nair, J.; Clement, N.; Smith, B.K.; Raben, N.; Fuller, D.D.; Byrne, B.J.; Corti, M. Advancements in AAV-mediated Gene Therapy for Pompe Disease. J. Neuromuscul. Dis. 2019. [Google Scholar] [CrossRef] [Green Version]
- House, T.; O’Donnell, K.; Saich, R.; Di Pietro, F.; Broekgaarden, R.; Muir, A.; Schaller, T. The role of patient advocacy organizations in shaping medical research: The Pompe model. Ann. Transl. Med. 2019, 7, 293. [Google Scholar] [CrossRef]

{kind=link}
| Age Group | Results | Reference |
|---|---|---|
| Adults | Time to diagnosis:
| Molster, 2016 [13] |
| Children | Time to diagnosis:
| Zurynski, 2017 [12] |
Key Considerations:
| ||
| Country and Region | Sample Size | Total Cases of IOPD | Total Cases of LOPD | Prevalence |
|---|---|---|---|---|
| Taiwan | 473,738 | 9 | 19 | 1/16,919 |
| Austria * | 34,736 | 0 | 4 | 1/8684 |
| Italy * | 3403 | 0 | 0 | - |
| Hungary * | 40,024 | 7 | 2 | 1/4400 |
| USA (State): | ||||
| Illinois * | 166,463 | 2 | 9 | 1/15,133 |
| Missouri | 269,500 | 4 | 20 | 1/11,229 |
| Washington * | 154,544 | 0 | 5 | 1/31,000 |
| New York | 390,000 | 1 | 30 | 1/165,000 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Saich, R.; Brown, R.; Collicoat, M.; Jenner, C.; Primmer, J.; Clancy, B.; Holland, T.; Krinks, S. Is Newborn Screening the Ultimate Strategy to Reduce Diagnostic Delays in Pompe Disease? The Parent and Patient Perspective. Int. J. Neonatal Screen. 2020, 6, 1. https://doi.org/10.3390/ijns6010001
Saich R, Brown R, Collicoat M, Jenner C, Primmer J, Clancy B, Holland T, Krinks S. Is Newborn Screening the Ultimate Strategy to Reduce Diagnostic Delays in Pompe Disease? The Parent and Patient Perspective. International Journal of Neonatal Screening. 2020; 6(1):1. https://doi.org/10.3390/ijns6010001
Chicago/Turabian StyleSaich, Raymond, Renee Brown, Maddy Collicoat, Catherine Jenner, Jenna Primmer, Beverley Clancy, Tarryn Holland, and Steven Krinks. 2020. "Is Newborn Screening the Ultimate Strategy to Reduce Diagnostic Delays in Pompe Disease? The Parent and Patient Perspective" International Journal of Neonatal Screening 6, no. 1: 1. https://doi.org/10.3390/ijns6010001
APA StyleSaich, R., Brown, R., Collicoat, M., Jenner, C., Primmer, J., Clancy, B., Holland, T., & Krinks, S. (2020). Is Newborn Screening the Ultimate Strategy to Reduce Diagnostic Delays in Pompe Disease? The Parent and Patient Perspective. International Journal of Neonatal Screening, 6(1), 1. https://doi.org/10.3390/ijns6010001