Highlights
- LARS-like symptoms (with important psycho-emotional impact on the affected persons) may also be present in normal healthy population.
- Clinicians should thus estimate to what extent the observed LARS-like symptoms affect the individual before and after treatment.
Highlights
- LARS-like symptoms (with important psycho-emotional impact on the affected persons) may also be present in normal healthy population.
- Clinicians should thus estimate to what extent the observed LARS-like symptoms affect the individual before and after treatment.
Abstract
Background & Aim. Sphincter-saving rectal surgery is prone to cause changes in bowel function associated with Low Anterior Resection Syndrome (LARS). Our aim was to assess LARS-like symptoms within a population of 50-80-year old in order to understand the functional disturbances and emotional impact of LARS. Materials and methods: We used a questionnaire to evaluate LARS with the following categories of symptoms: flatulence control, anal incontinence, frequency, clustering and urgency of the stools, and the psycho-emotional impact created by the presence of these symptoms. We calculated the severity of LARS on 343 responders. Results. The average age of the responders (57.4% females) was 60 years. Overall, 48.1% of those questioned had no LARS-associated symptoms, while the rest presented either minor (39.9%) or major (12%) LARS-like symptomatology according to the assessment scale. Women have a higher relative risk (1.32) of having minor or major LARS. The frequency of stools did not correlate with the overall LARS score. The psycho-emotional impact was mostly influenced by the presence of incontinence (p = 0.001) and urgency (p = 0.05). Discussions. The study highlights the need to integrate the initial status of patients into the overall quantification of the effects of surgery on the quality of life. Age does not influence the prevalence of LARS, but symptoms seem more prevalent in women. The psycho-emotional impact is relevant to the general population, so explanations given during the informed consent and accurate description of potential consequences of surgical intervention increase compliance to ensure better post-operative control of the symptomatology. Conclusions. Deriving a normative LARS-like score may alter the interpretation and discussion of LARS scores for future rectal cancer patients, and it also provides a better understanding of the emotional impact of such symptoms on certain population subsets or cultural groups.
Introduction
Up to 60-80% of patients presenting with rectal cancer undergo sphincter-saving surgery, and 90% of them will present with changes in their bowel function after surgery, usually termed low anterior resection syndrome (LARS) [1]. A more general definition of LARS is disordered bowel function after rectal resection, leading to a detriment in the quality of life. Two main groups are usually identified: the ones with urgency or incontinence and those with evacuatory dysfunction [2].
A Cochrane review and meta-analysis reported equivalent quality of life for patients who underwent abdominal-perineal resection (APR) or low anterior resection [3].
The studies examining the quality of life in non-surgical patients with fecal incontinence or constipation have shown a significant decrease in quality-of-life markers and also mental health status compared to similar populations without these symptoms [4,5]. We considered the impact of LARS in patients operated for rectal cancer of high interest, while understanding the significance of LARS-like symptoms in a population of individuals without significant medical history.
The LARS score is a questionnaire-based tool grading the most important bowel dysfunctions that appear as a consequence of sphincter-saving rectal cancer surgery. It is primarily used in studies that investigate quality-of-life parameters related to the digestive system affected by this type of restorative surgery [6]. There is increasing evidence that LARS has a detrimental impact on the quality of life, since a significant proportion of patients suffer from major LARS symptoms [7].
An important requirement for the clinical evaluation of this syndrome and also for research is that of using international validated tools to produce reliable and comparable results [8]. A baseline measurement of LARS (the preoperative level) is a poor estimate of the true function before the development of cancer [9,10]. Normative data from the general population can serve as a better baseline in studies of patients with rectal cancer, because such data reflect the level of bowel function disturbances in a similar population. Our aim was to assess the functional and emotional impact of LARS-like symptoms through the prevalence of symptoms in the general population.
Materials and Methods
The LARS score and sociodemographic variables
We used the questionnaire prepared by Laurberg, Emmertsen, et al. [6] and translated it into Romanian to evaluate Low Anterior Resection Syndrome (LARS) or LARS-like symptoms by assessing the following categories: flatulence control, anal incontinence, frequency of stools, clustering or stool fragmentation, and urgency or emergency in stool elimination. We also included an additional question to evaluate the psycho-emotional impact resulting from these symptoms and a second one questioning the option for permanent colostomy versus low anastomosis with LARS in the hypothetical case of surgery for a low-lying rectal tumor.
We also collected age and gender as demographic variables in a sample group of respondents that were apparently healthy and without previous pelvic surgery. We asked 420 persons aged between 50-80 years, the age group most affected by rectal cancer, to complete the paper questionnaire. We had 343 respondents on whom we could calculate the severity of LARS-like score, categorized into absent (0-20), minor (21-29), and major (30-42). The assessment of the emotional impact of these symptoms was done on a three-grade scale (A= not at all, B= a little, C= a lot).
Statistical analysis
Continuous variables were expressed as mean/standard deviation (SD) or median/interquartile range (IQR), as appropriate, whereas categorical variables were expressed in the form of numbers and percentages. A Chi-square test was used to compare groups.
Univariate logistic regression tests were used to determine the predictive factors for major LARS, the results were reported as relative risk (RR) with a 95% confidence interval (CI). The correlation was performed using Pearson’s coefficient. P values <0.05 were considered statistically significant. All the statistical analyses were performed using the SPSS version 20 (IBM Corporation).
Results
Characteristics of the responders and responses
The response rate was 81.6% and the average age of respondents was 60 years. The distribution by gender shows that females are more prone to respond to a random questionnaire. 57.4% of the respondents were women, while 42.6% were men. Overall, 48.1% of those questioned had no LARS-like symptoms, the remaining 51.9% had minor (39.9%) or major (12%) LARS-like symptoms according to the assessment scale (Figure 1).
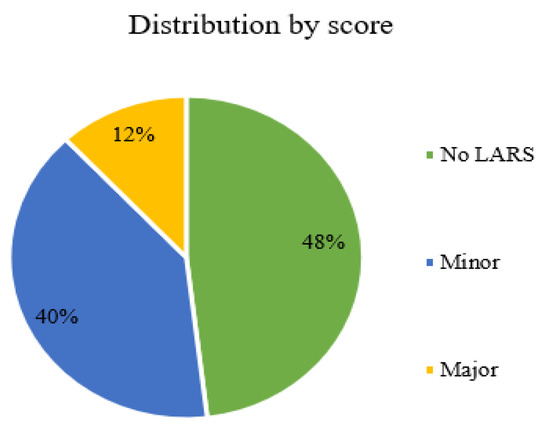
Figure 1.
The distribution of overall LARS-like scores in a normal population: no LARS 0-20; minor LARS 21-29; major LARS 30-42.
The analysis of the individual responses calculated as totals (Figure 2) reveals that the prevalence of incontinence was small in our normal population group (3.8%) and was not the main contributor to a high LARS score.
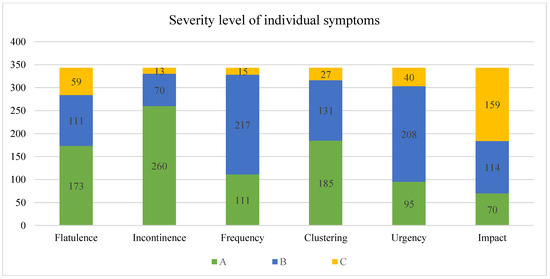
Figure 2.
The total number of answers to each question according to severity (A: never, B: <once per week, C: >once per week) in a normal population.
The frequency of stools was also rated infrequent, with only 4.4% of respondents having more than 4 stools per day. The assessment of the emotional impact brought by these symptoms showed that almost half of the patients with such problems (46.3%) rated them with the highest grade on our scale.
When analyzed by gender, 57.8% (114/197) of the female patients declared symptoms related to minor or major LARS, while only 43.8% (64/146) of male patients revealed similar symptoms. Women presented a higher relative risk (1.32) of having minor or major LARS-like symptoms.
Correlations of associated symptoms
The overall LARS score did not correlate with age (r=0.22). Figure 3 shows the distribution of all LARS values by age, while Figure 4 presents the relative differences between age groups in those with minor and major LARS. The frequency of stools has the lowest correlation coefficient with the overall LARS score (r=0.05) and also with all the other investigated symptoms.
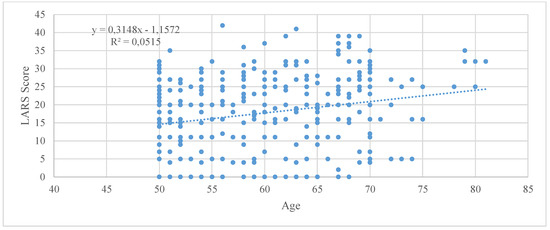
Figure 3.
Individual distribution of LARS-like score by age.
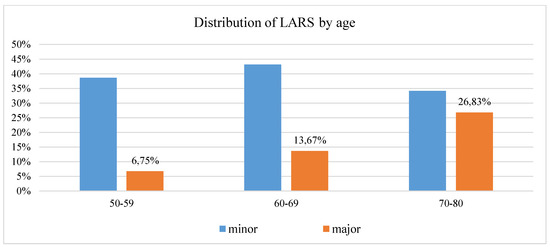
Figure 4.
Prevalence of major LARS (score >30) and minor LARS in the general population, by age groups.
Among our selected groups, the most relevant association with the total LARS score was represented by urgency and clustering, followed by incontinence for solid and gas.
In a multivariate regression analysis, the psycho-emotional impact was mostly influenced by the presence of incontinence (p=0.001) and urgency (p=0.05). When analyzing only those that responded with C (the highest impact), we noticed that the majority of them also ranked high in the urgency evaluation. Among female patients in our study group, 13.7% had a LARS score > 30, corresponding to major LARS symptoms. Among male patients, the similar proportion was 9.6%. A significant difference in the minor LARS percentages (44.2% vs 34.2%) between genders occurred, while the median (IQR) LARS scores were similar: 20 (11–26) for females and 17.5 (9–24) for males, respectively (Table 1).

Table 1.
Proportion of LARS by gender.
Factors associated with a higher LARS Score
The results for each of the five individual items of the LARS score are presented in Table 2. Females were more likely to report severe fragmentation and urgency than males. Females reported more statistically significant symptomatology than males in item 3, and even if percentages were higher for women on most other items, the differences were not significant (Fisher’s test p>0.05).
Table 2.
LARS score items by gender.
Discussions
Attempts to minimize the consequences of surgical therapy have been ongoing, since oncological resections not only present operative risks but also are characterized by important functional deficits. Patients with anterior resections of the rectum not only have to face the risk of developing local recurrence or distant metastases, but they also have to overcome the cessation of rectal functions, most importantly its reservoir function, with both distension and propulsion ability. Understanding the large impact LARS has on patients [10,11], we aimed to study the emotional value of LARS-like symptoms in a group of healthy volunteers that could help us understand the typical functional and emotional expectations in a certain population or cultural group. Many in the medical community are aware of the major differences between the northern and the southern part of Europe regarding the acceptance of colostomy and the degree of incontinence considered acceptable [13]. We aimed to evaluate the norm for our population that could suggest the emotional impact of LARS-like symptoms and could help reveak the potential postoperative problems to our patients.
In rectal cancer patients, the first most prominent symptom of LARS is having more stools than normal on a daily basis. However, in our normal population group, having more frequent stools does not correlate with a higher LARS score. Also, the prevalence of incontinence was low in the normal group (3.8%) and was not the major contributor to a high LARS score.
Our results contrast with those of a study in Sweden assessing not only bowel functions, but also urinary and sexual functions in the general population. Age did not significantly affect bowel function, with dysfunctions slightly more prevalent in women and stool frequency higher in men [13]. Even though not included in LARS, sexual and urinary dysfunctions that accompany rectal resections have an impact on the quality of life (QoL) and may impede the univariate influence of LARS on QoL.
Recent studies of LARS in rectal cancer populations have also shown that the female gender is associated with higher LARS scores [14], a finding which is partially paralleled by this study, but on a normal cohort. Even though LARS scores supposedly increase with age, data from our normal population did not find any such correlation, although this may be a postoperative problem which was beyond our capacity to evaluate. Age by itself may not be the relevant variable—emotional impact could be age-modulated, with women feeling more embarrassed than men about the presence of LARS-like symptoms.
We must also acknowledge the problem of overestimation of major LARS as was measured in a pilot study by Ribas et al [15], in which 24% of the patients classified as major LARS did not present a disordered bowel function when reassessed clinically. Such overestimation could have also affected our results. The same research team also noted that the LARS score currently in use may underestimate the impact of severe evacuatory dysfunction (if patients do not experience significant associated urgency and clustering, thus resulting in a very low score and risking misclassification as no LARS), since 24% of no LARS patients complained of evacuatory dysfunctions despite being treated with laxatives or enemas. In our study, we found that people complaining of evacuatory dysfunctions were the most affected from an emotional point of view. They did not find any statistically significant difference between the impact on the quality of life (assessed with EORTC QLQ 30) and the prevalence of major LARS [15], possibly because of the small sample size or the design of the questionnaire.
Social backgrounds and cultural influences
The social backgrounds and religious beliefs of patients may influence the results. We report a high response rate, thus underreporting due to embarrassment is low and we believe that our study was not influenced by such cultural perceptions, since reporting was anonymous. In comparison to our selection method, a similar Dutch study selected respondents from national registries of patients [9]. Since we included only healthy persons from our geographical area, the interpretation is therefore restricted to similar cultures in Eastern Europe.
In a multinational study, Juul et al [16] attempted to establish whether LARS is a reliable tool for predicting the impact of bowel function on the quality of life (QoL). In all 4 countries where the investigation was conducted (Sweden, Spain, Germany, Denmark), the LARS scores in the 3 QoL groups were significantly different, the differences in sensitivity and specificity being attributed to cross-cultural differences affecting the understanding/interpretation of QoL question. The LARS score was, to a great extent, able to predict the patients’ self-reported impact of bowel function on QoL.
Studies assessing the bowel habits of general populations usually show that constipation [5] (understood generally as hardened stool) is more prevalent than diarrhea. We assume that the preparation of the questionnaire is very important, but the fear of having to cope with diarrhea may be a fair reason. In our group, it is suggested that the majority would choose to keep the anal canal whenever possible, but not when major LARS symptoms were the alternative. This suggests that patients should receive better counseling for low lying tumors in order to make the best decision with bearable outcomes, taking into account that anthropometric and nutritional parameters recover faster for patients with APR than for those with ultra-low anterior resection [17], which add to the drawbacks of LARS. The number of people in our study hypothetically choosing colostomy instead of anastomosis was very high (51.2%), thus contrasting with a similar percentage of patients (51%) in a study in Taiwan who chose inter-sphincteric resection (ISR) [18], even knowing incontinence would appear to different degrees in almost 100% of the cases. The same study states that patients with ISR had higher LARS scores than patients with LARS.
When discussing incontinence, it is important to assess the need and utility of diaper usage, since up to 28% of patients require the use of pads [16]. Older female patients may be more resilient to LARS-associated symptoms because they are already accustomed to wearing disposable pads for urge and effort urinary incontinence [13], which helps them handle the symptoms better. Moreover, the idea of diaper necessity, even if intermittent, can cause psycho-emotional setbacks.
The prevalence of benign, non-acknowledged and non-reported problems (such as irritable bowel syndrome, small rectal prolapse, hemorrhoids) could affect the interpretation of these results. Other influential factors are: neurological disorders, vaginal deliveries in women, and natural geriatric degenerative changes in combination with polypharmacy. We deliberately did not exclude any participant with such problems so that the results would reflect the complete background population rather than a highly selected healthy population, introducing even more biases.
Since the quality of life was not measured separately, we cannot extrapolate LARS-like symptoms into changes in the quality of life. In studies of rectal cancer patients, there was a strong association between LARS and the impact on the quality of life. We detected a weak Pearson correlation factor (r=0.24) between the intensity of the emotional impact and the LARS score.
Conclusions
Our study, the first in Eastern Europe to our knowledge, revealed that LARS-like symptoms may be already present in normal healthy population. Such symptoms have an important psycho-emotional impact on the persons affected. If we extend the results of this study to the population of rectal cancer patients, we could suppose that part of them are already affected by some degree of bowel dysfunction before developing cancer or before surgery, but further investigations are needed to validate this assumption.
With the normative data presented in this study, clinicians will be able to estimate to what extent the observed LARS-like symptoms affect the individual before and after treatment. Various subsets of the population have different perceptions about factors influencing their quality of life, and these should be taken into consideration when discussing the potential decrease in QoL because of LARS.
Conflict of interest disclosure
There are no known conflicts of interest in the publication of this article. The manuscript was read and approved by all authors.
Compliance with ethical standards
Any aspect of the work covered in this manuscript has been conducted with the ethical approval of all relevant bodies and that such approvals are acknowledged within the manuscript.
References
- Bryant, C.; Lunniss, P.; Knowles, C.; Thaha, M.; Chan, C. Anterior resection syndrome. Lancet Oncol. 2012, 13, 403–408. [Google Scholar] [CrossRef] [PubMed]
- Lunniss, P.J.; Gladman, M.A.; Benninga, M.A.; Rao, S.S. Pathophysiology of evacuation disorders. Neurogastroenterol Motil. 2009, 21 (suppl 2), 31–40. [Google Scholar] [CrossRef] [PubMed]
- Pachler, J.; Wille-Jorgensen, P. Quality of life after rectal resection for cancer, with or without permanent colostomy. Cochrane Database Syst Rev. 2005, 2, CD004323. [Google Scholar]
- Pares, D.; Vial, M.; Bohle, B. Prevalence of faecal incontinence and analysis of its impact on quality of life and mental health. Colorectal Dis. 2011, 13, 899–905. [Google Scholar] [CrossRef] [PubMed]
- Irvine, E.J.; Ferrazzi, S.; Pare, P.; Thompson, W.G.; Rance, L. Health-related quality of life in functional GI disorders: focus on constipation and resource utilization. Am J Gastroenterol. 2002, 97, 1986–93. [Google Scholar] [CrossRef] [PubMed]
- Emmertsen, K.J.; Laurberg, S. Low anterior resection syndrome score: development and validation of a symptom-based scoring system for bowel dysfunction after low anterior resection for rectal cancer. Annals of surgery. 2012, 255, 922–928. [Google Scholar] [CrossRef] [PubMed]
- Sarcher, T.; Dupont, B.; Alves, A.; Menahem, B. Anterior resection syndrome: What should we tell practitioners and patients in 2018? Journal of Visceral Surgery. 2018, 155, 383–391. [Google Scholar] [CrossRef] [PubMed]
- Hou, X.T.; Pang, D.; Lu, Q.; Yang, P.; Jin, S.L.; Zhou, Y.J.; Tian, S.H. Validation of the Chinese version of the low anterior resection syndrome score for measuring bowel dysfunction after sphincter-preserving surgery among rectal cancer patients. European Journal of Oncology Nursing. 2015, 19, 495–501. [Google Scholar] [CrossRef] [PubMed]
- Juul, T.; Elfeki, H.; Christensen, P.; Laurberg, S.; Emmertsen, K.J.; Bager, P. Normative Data for the Low Anterior Resection Syndrome Score (LARS Score). Ann Surg. 2018. [CrossRef] [PubMed]
- Battersby, N.J.; Bouliotis, G.; Emmertsen, K.J. Development and external validation of a nomogram and online tool to predict bowel dysfunction following restorative rectal cancer resection: the POLARS score. Gut. 2018, 67, 688–696. [Google Scholar] [CrossRef] [PubMed]
- Croese, A.D.; Lonie, J.; Trollope, A.F.; Vangaveti, V.N.; Ho, Y.H. A meta-analysis of the prevalence of Low Anterior Resection Syndrome and systematic review of risk factors. International Journal of Surgery. 2018, 56, 234–241. [Google Scholar] [CrossRef] [PubMed]
- Croese, A.D.; Zubair, O.N.; Lonie, J.; Trollope, A.F.; Vangaveti, V.N.; Mushaya, C.; Ho, Y.H. Prevalence of low anterior resection syndrome at a regional Australian centre. ANZ J Surg. 2018, 88, 813–817. [Google Scholar] [CrossRef] [PubMed]
- Bock, D.; Angenete, E.; Gonzales, E. Assessing health, quality of life and urogenital function in a sample of the Swedish general population: a cross-sectional study. BMJ Open. 2018, 8, e021974. [Google Scholar] [CrossRef] [PubMed]
- Bregendahl S, Emmertsen KJ, Lous J; et al. Bowel dysfunction after low anterior resection with and without neoadjuvant therapy for rectal cancer: a population-based cross-sectional study. Colorectal Dis. 2013, 15, 1130–1139. [Google Scholar] [CrossRef] [PubMed]
- Ribas, Y.; Aguilar, F.; Jovell-Fernández, E.; Cayetano, L.; Navarro-Luna, A.; Muñoz-Duyos, A. Clinical application of the LARS score: results from a pilot study. Int J Colorectal Dis. 2017, 32, 409–418. [Google Scholar] [CrossRef] [PubMed]
- Juul, T.; Ahlberg, M.; Biondo, S.; Emmertsen, K.J.; Espin, E.; Jimenez, L.M.; Matzel, K.; Palmer, G.; Sauermann, A.; Trenti, L.; Zhang, W.; Laurberg, S.; Christensen, P. International Validation of the Low Anterior Resection Syndrome Score. Annals of Surgery. 2014, 259, 728–734. [Google Scholar] [CrossRef] [PubMed]
- Bong, J.W.; Lim, S.B.; Lee, J.L.; Kim, C.W.; Yoon, Y.S.; Park, I.J.; Yu, C.S.; Kim, J.C. Comparison of Anthropometric Parameters after Ultralow Anterior Resection and Abdominoperineal Resection in Very Low-Lying Rectal Cancers. Gastroenterology research and practice. 2018, 9274618. [Google Scholar] [CrossRef] [PubMed]
- Tan, S.H.; Liao, Y.M.; Lee, K.C.; Ko, Y.L.; Lin, P.C. Exploring bowel dysfunction of patients following colorectal surgery: A cohort study. J Clin Nurs. 2019, 28, 1577–1584. [Google Scholar] [CrossRef] [PubMed]






© 2019 by the authors. 2019 Tudor-Cristian Frunza, Sorinel Lunca, Iustina Baciu, Iulia Axinia, Cezar Valentin Mocanu, Andreea Crudu, Narcis Bujor, Lucia Flavia Livenschi, Claudiu Alexandru Nicolaiev, Andreea Hulubencu, Anca Diaconu, Emilia Valasciu, Ioana Jalobceastai, Malina Tibirna, Mihail Gabriel Dimofte.