Abstract
Introduction: Major depressive disorder is one of the most prevalent psychiatric disorders and is associated with a severe impact on the personal functioning, thus with incurring significant direct and indirect costs. The presence of depression in patients with medical comorbidities increases the risks of myocardial infarction and decreases diabetes control, and adherence to treatment. The mechanism through which these effects are produced is still uncertain. Objectives of this study were to evaluate the metabolic alterations in female Wistar rats with induced depression, with and without administration of Agomelatine. The methods included two experiments. All data were analyzed by comparison with group I (control), and with each other. In the first experiment we induced depression by: exposure to chronic mild stress-group II; olfactory bulbectomy-group III; and exposure to chronic mild stress and hyperlipidic/hyper caloric diet-group IV. The second experiment was similar with the first but the rats received Agomelatine (0.16 mg/ animal): group V (depression induced through exposure to chronic mild stress), VI (depression induced through olfactory bulbectomy) and VII (depression induced through exposure to chronic mild stressing hyperlipidic/hypercaloric diet). Weight, cholesterol, triglycerides and glycaemia were measured at day 0 and 28, and leptin value was measured at day 28. The results in the 1st experiment revealed significant differences (p<0.01) for weight and cholesterol in Group IV, for triglycerides in groups III and IV (p<0.001), and for glycaemia in group II. The 2nd experiment revealed significant differences (p<0.001) in group VII for weight and triglycerides, and in groups V and VI for triglycerides (p<0.01). In conclusion, significant correlations were found between high level of triglycerides and depression induced by chronic stress and olfactory bulbectomy. Agomelatine groups had a lower increase of triglycerides levels.
Introduction
Major depressive disorder (MDD) is among the most significant psychiatric disorders. The World Health Organization ranked depression as the fourth cause of disability around the world and estimated that it will take second place by 2020, after cardiovascular disorders [1,2]. Depression has a high global incidence and prevalence and is associated with a significant impact on the social and personal functioning (e.g., high rates of absenteeism, reduced productivity, familial disturbances) [3,4], but also with important medical comorbidities (e.g., cardiovascular diseases, diabetes mellitus, dyslipidemia, obesity) [5,6,7].
The association of depression with somatic comorbidities affects both the therapeutic approach and the quality of life of the patients. Despite vast research in the field, the relationship between depression and such comorbidities often remains unclear. For instance, obesity is considered a risk factor for depression [8], yet is also a comorbidity of depression. Many studies report a significant correlation between depression and metabolic syndrome, but it is still unclear whether this association is the cause-effect type or results from several common variables [5]. Patients with depression have a higher risk for developing diabetes [4], and current epidemiological data show that at least one third of the patients with diabetes mellitus have clinically significant depressive symptoms [4]. Depression is also a risk factor for cardiac mortality and morbidity but the potential mechanism that produces these effects remains uncertain [9]. One possible explanation comes from the heart and soul study that revealed that the presence of MDD in out-patients with coronary heart disease decreases medication adherence [10]. Such findings confirm earlier suggestions that depression is a risk factor for noncompliance with medical treatment [11] but it also reveals one of the possible mechanisms: untreated MDD decreases adherence to cardiovascular medication and thus patients remains unprotected, or too many drugs taken in the same time increases the risk of side effects and poor treatment adherence [10]. Another pathway that links depression and cardiovascular diseases is represented by disruption of circadian sleep-wake cycles. Thus, disruption of sleep-wake cycle is a core feature of depressive disorder, which is associated with perturbation of hormonal secretion [12]. But, disruption of circadian rhythm is also associated with increased risk for obesity, diabetes and cardiovascular disease [13]. Difficulties in initiating and maintaining sleep were associated with increased incidence of diabetes in men [14]. Also, a number of studies support an association between feeding regimens and quality of ingested food on one hand, and the circadian rhythm on the other hand [15].
Aim. The objective of this study was to evaluate metabolic alterations that appear in rats with induced depression, with and without administration of Agomelatine, a melatonin analog. The present data are drawn from a more extensive research project investigating animal models of induced depression.
Materials and Methods
The research was conducted in the Laboratory for Experimental Research of the Department of Physiology of the University of Medicine and Pharmacy “Iuliu Hatieganu” in Cluj-Napoca, and was approved by the Ethical Committee of the University. Female Wistar rats kept in adequate vivarium conditions were used.
Two experimental analyses were conducted. The first analysis (Analysis 1) included four groups, of 10 rats each: group I (control); group II (depression induced through exposure to chronic mild-intensity stress–constant exposure of 120 min/24 h, that is 5 min/hour, to a continuous auditory 5 dB stimulus, automatically generated by a bell); group III (depression induced through olfactory bulbectomy); and group IV (depression induced through exposure to chronic mild-intensity stress and hyperlipidic/hyper caloric diet). Groups I, II and III received adequate caloric diet—20 g/day/rat (proteins 18%, lipids 1.5% and fibers 5%), while group IV received the same amount and type of food to which 3 ml pork fat/day/rat was added.
The second analysis (Analysis 2) included three groups: group V (depression induced through exposure to chronic mild-intensity stress–same method as group II); group VI (depression induced through olfactory bulbectomy); and group VII (depression induced through exposure to chronic mild-intensity stress and hyperlipidic/hyper caloric diet–same method as group IV). The rats in Analysis 2 (groups V, VI and VII) received Agomelatine 0.16 mg/rat.
Evaluation occurred baseline (T0) and after 28 days (T28). At T0, weight (grams) and blood levels of cholesterol (mg/dL), triglycerides (mg/dL) and glycaemia/ glucose (mg/dL) were measured. At T28, weight (grams) and blood levels for cholesterol (mg/dL), triglycerides (mg/dL), glycaemia/glucose (mg/dL) and leptin (pg/mL) were measured. Statistical analysis was performed with Stats Direct software, version 2.7.2.
For the descriptive statistics, indicators of centrality, localization and distribution were used to present the data. For testing the normal distribution, we used the Shapiro-Wilk test, while the variation was tested with F or Levene and/or Bartlett tests. We used the t (Student) test for data with normal distribution and Mann-Whitney (U) non- parametrical tests (for two non-paired variables) or Wilkoxon (for two paired variables) for data with non-uniform distribution and rankings.
For analyzing three or more variables we used the ANOVA test for normal distribution and Kruskal-Wallis for non-uniform distribution. The level for significance was set at α= 0.05 (5%), α=.01 (1%) or α= 0.001.
Results
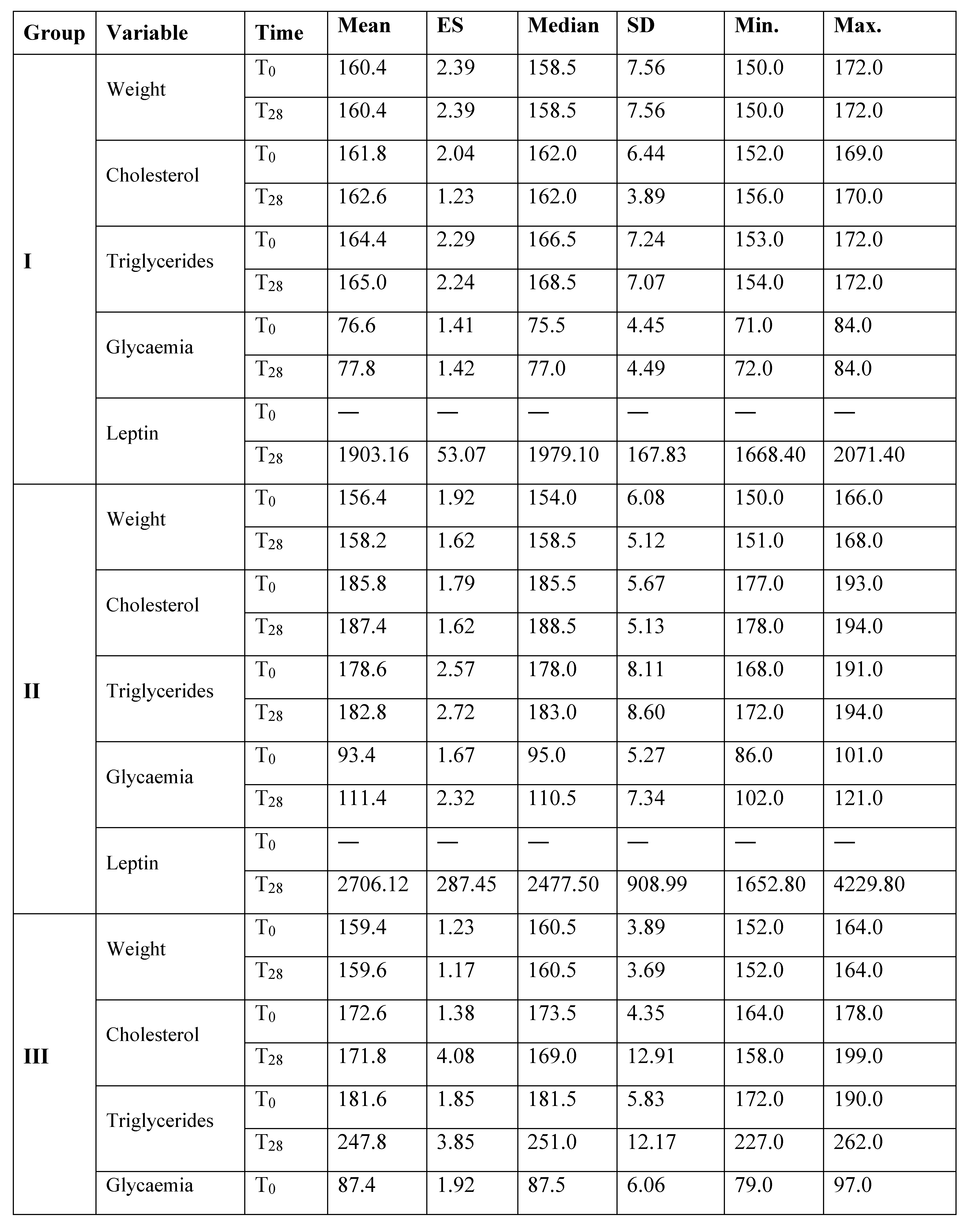
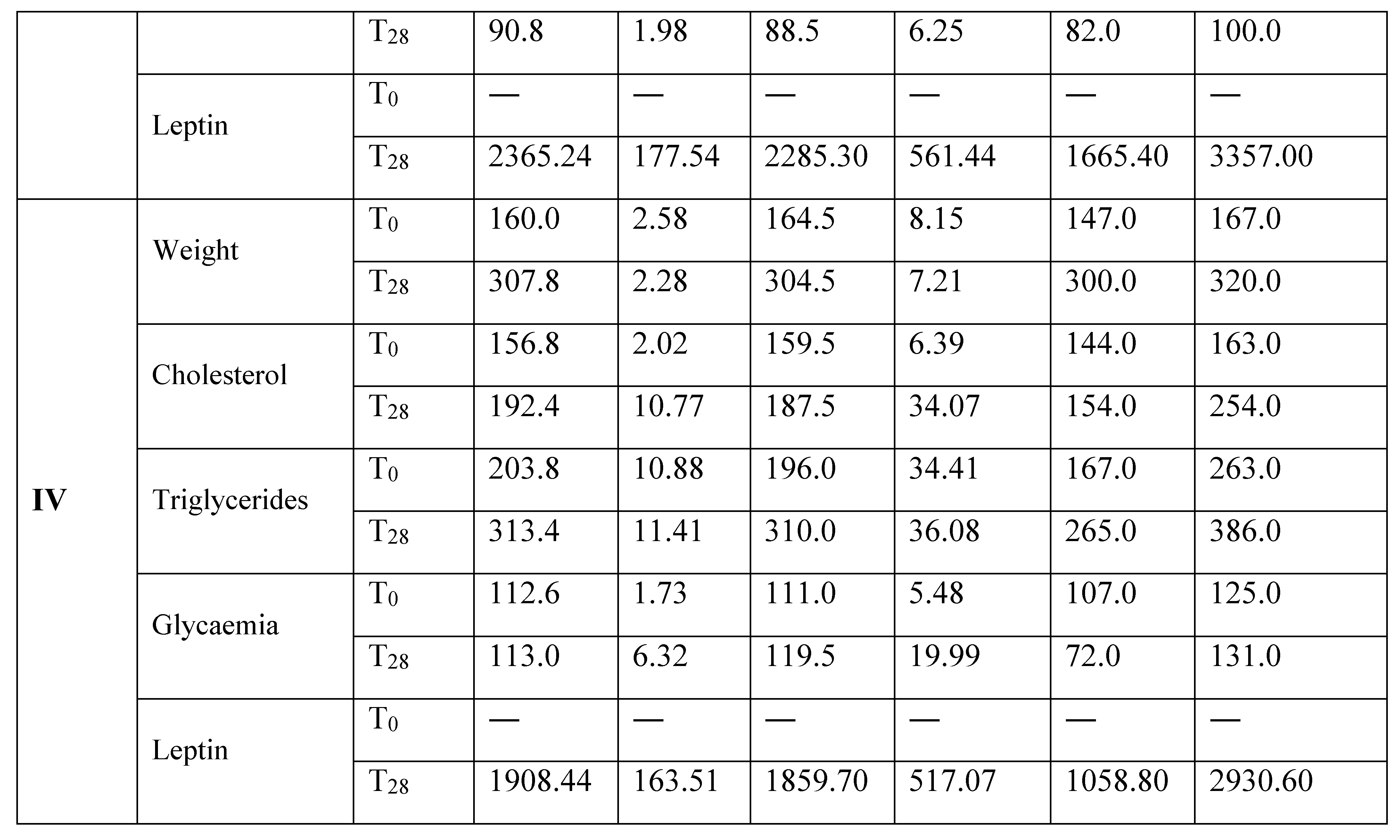
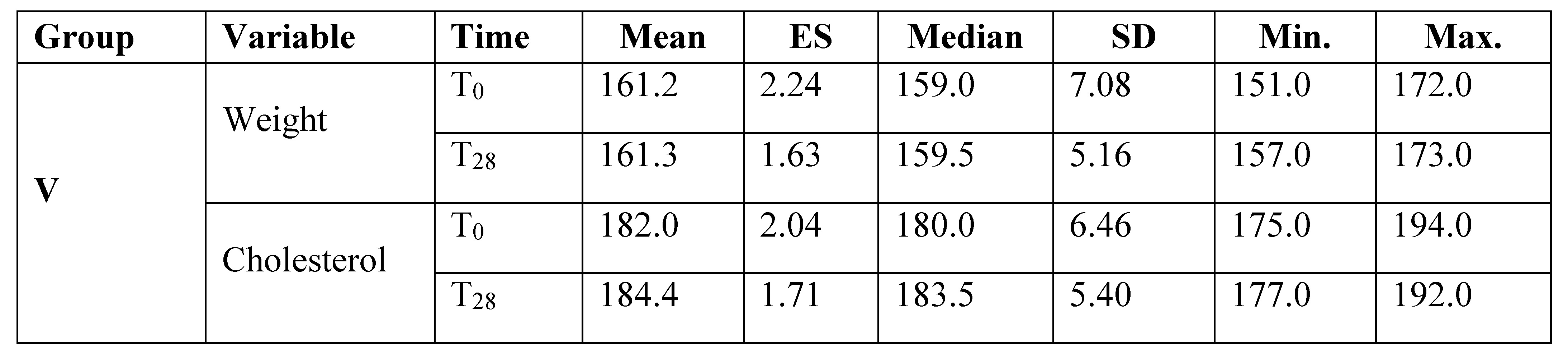
An overview of the variables values of the groups included in Analysis 1 is showed in Table 1.

Table 1.
Comparison between the variables values at T0 and T28 for the groups included in Analysis 1.
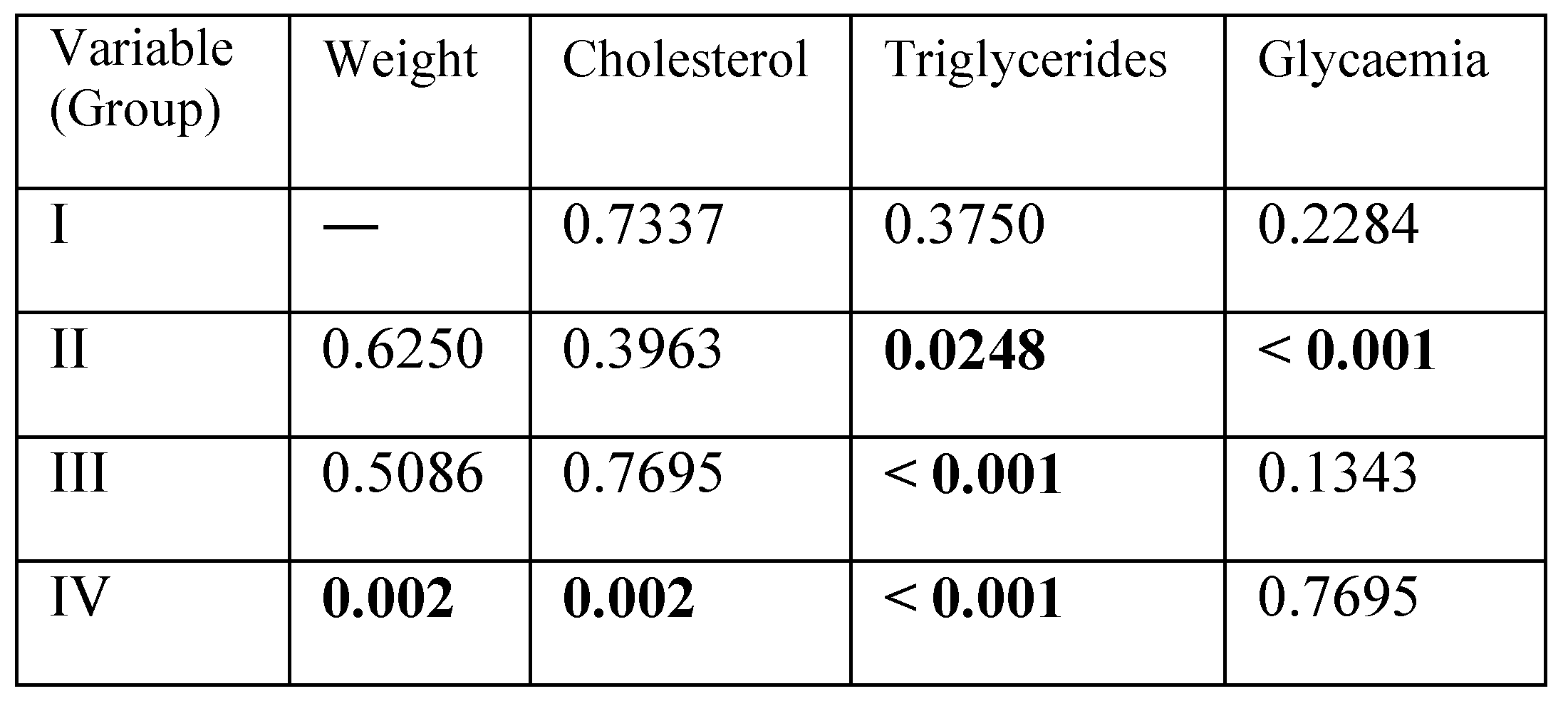
Statistical analysis of the variables for pairs (T0-T28) showed highly significant differences (p<0.001) in groups III and IV for triglycerides and in group II for glycaemia, very significant differences (p<0.01) in group IV for weight and cholesterol and significant differences (p<0.05) in group II for triglycerides (Table 2). Table 3 shows the variables values of the groups included in Analysis 2.
Table 2.
Levels of significance (p-values) of the variables for each group (T0–T28) in Analysis 1 (significant values in bold).
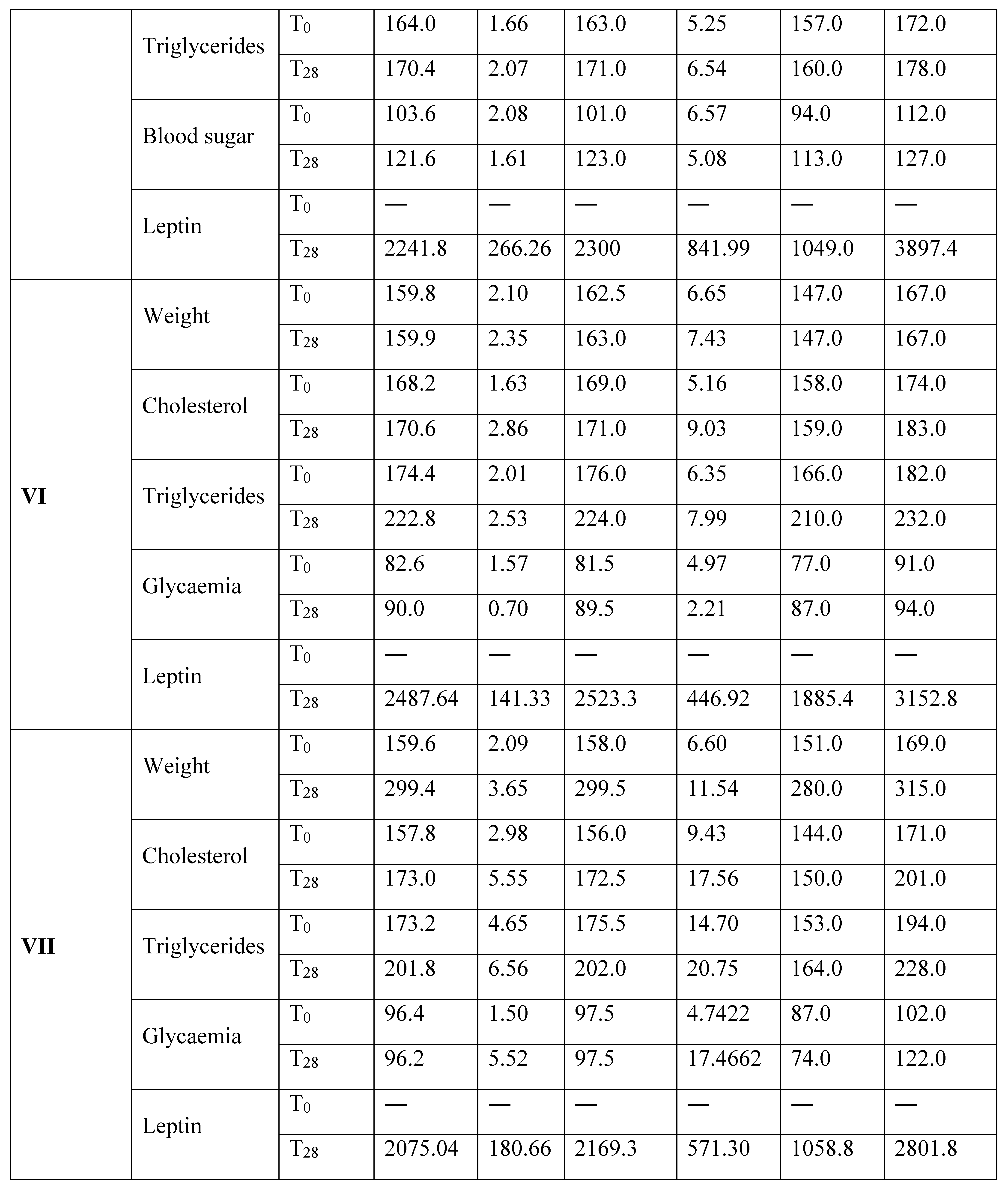
Table 3.
Comparison between the variables values at T0 and T28 for the groups included in Analysis 2.
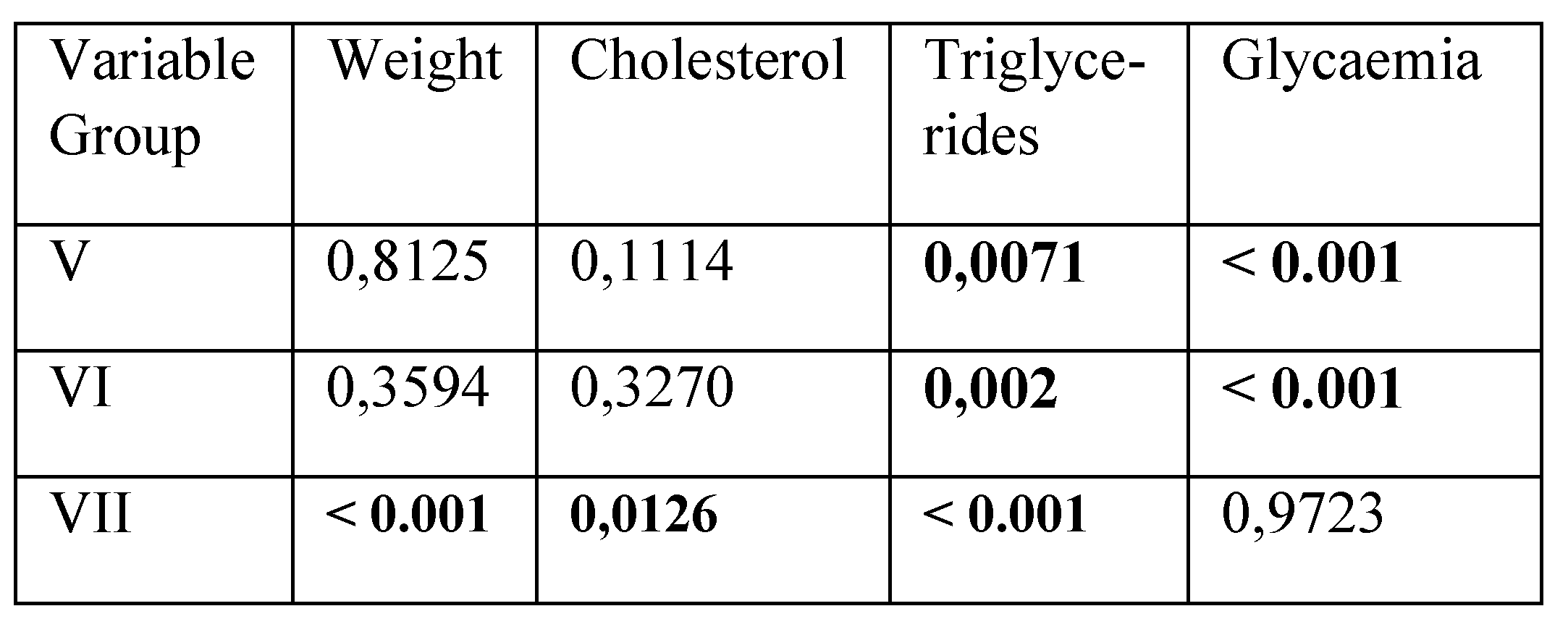
Statistical analysis of the variables for pairs (T0–T28) showed highly significant differences (p<0.001) in group VII for weight and triglycerides, very significant differences (p<0.01) in groups V and VI for triglycerides and significant differences (p<0.05) in group VII for cholesterol (Table 4).
Discussion
The significant increase of weight and cholesterol is related to the quantity and content of the diet. In the present study, the increase of triglycerides was found in the groups with chronic mild-intensity stress, independent of the diet type, in the group with olfactory bulbectomy without Agomelatine, but not in the control group. This result confirms the available data indicating a significant correlation between depression and triglycerides levels [16,17,18]. Agomelatine correlated with significantly smaller amplitude in the increase of triglycerides. In one study evaluating the effect of melatonin administration on developing metabolic syndrome in male Wistar rats with high calorie diet, melatonin administration was associated with reduced weight gain, visceral adiposity, blood triglyceride, and insulin level [19]. In another study evaluating the influence of melatonin administration on dyslipidemia and systolic hypertension using young male Zucker diabetic fatty rats, melatonin administration was associated with reduced mean weight gain without influencing food ingestion and decreased levels of triglyceride [20]. Possible mechanisms involve the effect of melatonin on circadian rhythm, giving the links that exist between the circadian system and obesity, diet and depression [21,22].
The results for leptin levels are difficult to interpret based on the current study design (no determination at T0) and the literature reports an inconsistent relation between depression and leptin. Some studies reported that patients with major depressive disorder have lower leptin levels compared to healthy controls with similar body mass index [23,24], while others have reported higher levels of leptin in women with depression [25,26,27]. In one study, rats which were subject to chronic unpredictable stress and chronic social defeat presented low level of leptin [28]. In addition, in the previously mentioned study, leptin administration had an antidepressant like effect [28].
Table 4.
Levels of significance of the variables for each group (T0–T28) in Analysis 2 (statistically significant values in bold).
Table 4.
Levels of significance of the variables for each group (T0–T28) in Analysis 2 (statistically significant values in bold).
 |
Such findings should be also discussed in the context of ACTH and cortisol influence on the hormonal and metabolic status, because it is known from previous studies that the circadian rhythm of cortisol secretion disappears both in Cushing disease and in major depressive episode [29]. Thus, this relationship might also impact glucose and lipid metabolisms.
Conclusions
The results of the present study support the correlation between the increase of triglycerides and experimentally induced depression in rats through chronic stress and olfactory bulbectomy. The administration of Agomelatine was associated with smaller amplitude of the increase of triglycerides. Except the groups with hyperlipidic diet, experimentally induced depression was not associated with an increase in cholesterol levels.
References
- Bromet, E.; Andrade, L.H.; Hwang, I.; Sampson, N.A.; Alonso, J.; de Girolamo, G.; de Graaf, R.; Demyttenaere, K.; Hu, C.; Iwata, N.; et al. Cross-national epidemiology of DSM-IV major depressive episode. BMC Med. 2011, 9, 90. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, S.H.; Gorwood, P. Successful Management of Major Depressive Disorder; Evolving Medicine Ltd., Unitec House, 2 Albert Place: London N3 1QB, UK, April 2013. [Google Scholar] [CrossRef]
- Thase, M.E. Using biomarkers to predict treatment response in major depressive disorder: evidence from past and present studies. Dialogues Clin Neurosci. 2014, 16, 539–544. [Google Scholar] [CrossRef]
- Lloyd, C.E.; Hermanns, N.; Nouwen, A.; Pouwer, F.; Underwood, L.; Winkley, K. Katon, W., Maj, M., Sartorius, N., Eds.; The Epidemiology of Depression and Diabetes. In Depression and Diabetes; John Wiley & Sons, Ltd.: Chichester, UK, 2010; pp. 1–27. [Google Scholar]
- Foley, D.L.; Morley, K.I.; Madden, P.A.; Heath, A.C.; Whitfield, J.B.; Martin, N.G. Major Depression and the metabolic syndrome. Twin Res. Hum. Genet. 2010, 13, 347–358. [Google Scholar] [CrossRef] [PubMed]
- Bogers, R.P.; Bemelmans, W.E.; Hoogenveen, R.T.; Boshuizen, H.C.; Woodward, M.; Knekt, P.; van Dam, R.M.; Hu, F.B.; Visscher, T.L.; Menotti, A.; et al. BMI-CHD Collaboration Investigators. Association of overweight with increased risk of coronary heart disease partly independent of blood pressure and cholesterol levels: a meta-analysis of 21 cohort studies including more than 300,000 persons. Arch Intern Med. 2007, 167, 1720–1728. [Google Scholar] [CrossRef] [PubMed]
- Mottillo, S.; Filion, K.B.; Genest, J.; Joseph, L.; Pilote, L.; Poirier, P.; Rinfret, S.; Schiffrin El Eisenberg, M.J. The metabolic syndrome and cardiovascular risk a systematic review and meta-analysis. J Am Coll Cardiol. 2010, 56, 1113–1132. [Google Scholar] [CrossRef]
- Berk, M.; Williams, L.J.; Jacka, F.N.; O’Neil, A.; Pasco, J.A.; Moylan, S.; Allen, N.B.; Stuart, A.L.; Hayley, A.C.; Byrne, M.L.; et al. So depression is an inflammatory disease, but where does the inflammation come from? BMC Med. 2013, 11, 200. [Google Scholar] [CrossRef]
- Carney, R.M.; Freedland, K.E.; Miller, G.E.; Jaffe, A.S. Depression is a risk factor for cardiac mortality and morbidity: a review of a potential mechanism. J Psychosom Res. 2002, 53, 897–902. [Google Scholar] [CrossRef]
- Gehi, A.; Hass, D.; Pipkin, S.; Whooley, M.A. Depression and medication adherence in outpatients with coronary heart dissease: findings from heart and Soul Study. Arch Intern Med. 2005, 165, 2508–2513. [Google Scholar] [CrossRef]
- DiMatteo, M.R.; Lepper, H.S.; Croghan, T.W. Depression is a risk factor for noncompliance with medical treatment: meta-analisys of the effect of anxiety and depression on patient adherence. Arch Inter Med. 2000, 160, 2101–2107. [Google Scholar] [CrossRef]
- Nechita, F.; Pirlog, M.C.; Chirita, A. Circadian malfunctions in depression – neurobiological and psychosocial approaches. Rom J Morphol Embryol 2015, 56, 949–955. [Google Scholar]
- Scheer, F.A.; Hilton, M.F.; Mantzoros, C.S.; Shea, S.A. Adverse metabolic and cardiovascular consequences of circadian misalignment. Proc Natl Acad Sci USA 2009, 106, 4453–4458. [Google Scholar] [CrossRef]
- Mallon, L.; Broman, J.E.; Hetta, J. High incidence of diabetes in men with sleep complains or short sleep duration: a 12-year follow-up study of a middle-aged population. Diabetes Care 2005, 28, 2762–2767. [Google Scholar] [CrossRef] [PubMed]
- Froy, O. The relationship between nutrition and circadian rhythms in mammals. Front Neuroendocrinol. 2007, 28, 61–71. [Google Scholar] [CrossRef]
- Pulkki-Raback, L.; Elovainio, M.; Kivimaki, M.; Mattsson, N.; Raitakari, O.T.; Puttonen, S.; Marniemi, J.; Viikari, J.S.; Keltikangas-Jarvinen, L. Depressive symptoms and the metabolic syndrome in childhood and adulthood: a prospective cohort study. Health Psychol. 2009, 28, 108–116. [Google Scholar] [CrossRef] [PubMed]
- Kinder, L.S.; Carnethon, M.R.; Palaniappan, L.; King, A.C.; Fortmann, S.P. Depression and the metabolic syndrome in young adults: findings from the Third National Health and Nutrition Examination Survey. Psychosom Med. 2004, 66, 316–322. [Google Scholar] [CrossRef] [PubMed]
- Vaccarino, V.; McClure, C.; Johnson, B.D.; Sheps, D.S.; Bittner, V.; Rutledge, T.; Shaw, L.J.; Sopko, G.; Olson, M.B.; Krantz, D.S.; et al. Depression, the metabolic syndrome and cardiovascular risk. Psychosom Med. 2008, 70, 40–48. [Google Scholar] [CrossRef]
- Agil, A.; Navarro-Alarcon, M.; Ruiz, R.; Abuhamadah, S.; El Mir, M.Y.; Vasquez, G.F. Beneficial effects of melatonin on obesity and lipid profile in young Zucker diabetic fatty rats. J Pineal Res. 2011, 50, 207–212. [Google Scholar] [CrossRef]
- Bartness, T.J.; Demas, G.E.; Song, C.K. Seasonal changes in adiposity: the roles of the photoperiod, melatonin and other hormones, and sympathetic nervous system. Exp Biol Med. 2002, 227, 363–376. [Google Scholar] [CrossRef]
- Yanagihara, H.; Ando, H.; Hayashi, Y.; Obi, Y.; Fujimura, A. High-fat feeding exerts minimal effects on rhythmic mRNA expression of clock genes in mouse peripheral tissues. Chronobiol Int. 2006, 23, 905–914. [Google Scholar] [CrossRef]
- Cardinali, D.P.; Cano, P.; Jimenez-Ortega, V.; Esquifino, A.I. Melatonin and metabolic syndrome. Physiopathologic and therapeutical implications. Neuroendocrinology 2011, 93, 133–142. [Google Scholar] [CrossRef]
- Kraus, T.; Haack, M.; Schuld, A.; Hinze-Selch, D.; Pollmacher, T. Low leptin levels but normal body mass indices in patients with depression or schizophrenia. Neuroendocrinology 2001, 73, 243–247. [Google Scholar] [CrossRef] [PubMed]
- Atmaca, M.; Kuloglu, M.; Tezcan, E.; Ustundag, B.; Gecici, O.; Firidin, B. Serum leptin and cholesterol values in suicide attempters. Neuropsychobiology 2002, 45, 124–127. [Google Scholar] [CrossRef] [PubMed]
- Rubin, R.T.; Rhodes, M.E.; Czambel, R.K. Sexual diergism of baseline plasma leptin and leptin suppression by arginine vasopressin in major depressives and matched controls. Psychiatry Res. 2002, 113, 255–268. [Google Scholar] [CrossRef] [PubMed]
- Esel, E.; Ozsoy, S.; Tutus, A.; Sofuoglu, S.; Kartalci, S.; Bayram, F.; Kokbudak, Z.; Kula, M. Effects of antidepressant treatment and of gender on serum leptin levels in patients with major depression. Prog Neuropsychopharmacol Biol Psychiatry 2005, 29, 565–570. [Google Scholar] [CrossRef]
- Zeman, M.; Jirak, R.; Jachymova, M.; Vecka, M.; Tvrzicka, E.; Zak, A. Leptin, adiponectin, leptin to adiponectin ratio and insulin resistance in depressive women. Neuro Endocrinol. Lett. 2009, 30, 387–395. [Google Scholar]
- Lu, X.Y.; Kim, C.S.; Frazer, A.; Zhang, W. Leptin: a potential novel antidepressant. Proc Natl Acad Sci USA 2006, 103, 1593–1598. [Google Scholar] [CrossRef]
- Fischbach, F.; Dunning, M.B. A manual of laboratory and diagnostic tests. ISBN/ISSN, 2015; 379–382, 624–644ISBN 9781451190892. ISSN 9781451190892. [Google Scholar]
© 2016 by the author. 2016. Maria-Gabriela Puiu, Mihnea C. Manea, George L. Paraschiv, Traian Purnichi, Ecaterina Ionescu, Simona Tache, Ioana Paunica, Mirela Manea