Abstract
Introduction: the problem of the iatrogenic lesions of the main biliary pathways is far from being completely clarified and still represents a serious surgical situation, during both open and laparoscopic surgeries. The outcome of these situations is closely linked with the actual moment of discovery of the lesion and the surgical methods for repairing such defects and implies a great number of options, such as reconstructive, derivative and substitutive techniques. Objectives: the goal of this paper is to present an algorithm of choices and their consequences for clinical conduit in the case of iatrogenic biliary lesions discovered in the course of open or laparoscopic procedures of the main biliary pathways, based on our experience. Material and method: We present a multicentric retrospective study of 53 cases of lesions following open and laparoscopic procedures, from a larger lot of 10.015 surgeries on extrahepatic biliary ducts recorded during a 40 years period of time, in 2 clinical hospitals. Out of these, 2127 interventions were strictly focused on the common bile duct, for various pathology. Conclusion: The choice of the optimum method is strictly correlated with the morphological nature of the lesion, which is different from one stage to the other, depending upon the moment of detection, and therefore have different surgical implications.
Introduction
Since it was first published by Bismuth, his classification regarding bile duct injuries is still the most well-known and cited one, although it has some drawbacks. Thus, it only considers the length of the remaining intact bile duct, and not some other key factors, like bile collections that may arise from a bilistasis defect in the cystic duct or the liver bed, nor the lateral solutions of continuity of the main bile duct and right hepatic duct, all important aspects of the modern laparoscopic age when we register a great rise in the diversity of scenarios which can lead to iatrogenic lesions [1]. Although the Bismuth classification has been adopted and also used to describe the lesions during the laparoscopic approach, Strasberg and Soper modified it in order to include the previous mentioned key factors, so that we have now a reference tool for describing the iatrogenic laparoscopic lesions [2].
However, this stadialisation omits a very important key-factor: the time that has intervened from the moment when lesion occurred, to the moment of the first clinical signs. And this timeline is a crucial parameter for surgical options to repair lesion, which are very different for the immediate recognized lesions, as opposed to late postoperative discovered injuries [3].
Therefore, we manage the draft of our own anatomo-clinical stadialisation with the timeline as the focal point, and it can be summarized into two main periods: the intraoperative one and the postoperative one, the latter with its own subclassification [4]:
The intraoperative stage – represent injuries that have been discovered right away and require measures of repair performed within the same operative time. As one would expect, this is by far the optimal situation and the most favorable one; however, this rarely occurs, with only 5% incidence cited in the literature [5,6];
The postoperative stage
- A. Early postoperative lesions (1-30 days). The clinical signs are those of the consequences of the unrecognized/missed injuries during the primary surgery, namely those of choleperitoneum or, much less often, obstructive syndromes, due to accidental (total or partial) ligature of the extrahepatic bile ducts. In this category also fall all the cases that reconstructive surgery has failed to resolve.
- B. Late postoperative lesions (over 30 days). These include the benign stenosis of the CBD (Common Bile Duct) with a clinical translation in jaundice. These may or may not be accompanied by external biliary fistulas which in time can lead to a full process of perivisceritis. This in turn can result in an abscess near the CBD.
- C. Final stage lesions. These are the final developments of the previously mentioned accidental lesions, that usually occur after 2 months from the initial moment of surgery. This tertiary period is represented by the sclerosing lesions and sometimes by large anatomical hipertrophic lesions of the biliary pathway, which in many cases are due to the postoperative persistence of the biliary fistulae or to the postoperative biliary stenoses, and which have lithiasis or primary and secondary sclerosing colangitis of the biliary tree as consequences.
Materials and Methods
We discuss a collection of 53 cases of iatrogenic biliary lesions, encountered both during classic and laparoscopic procedures, spread across all stages of the previously mentioned customary time-based classifications, namely: 14 cases of CBD injuries immediately recognised, at the time of surgery, 10 cases of lesions discovered in the early (less than 30 days) postoperative period, including 8 cases of fistulae and 2 cases of ligatures or clips, and 29 cases belonging to the late complications period (over 30 days), 20 being only stenosis and the other 9 being stenoses accompanied by fistulae.
These cases have been extracted from a larger study that comprises of 10.015 surgeries for various pathologies of the extrahepatic biliary pathways, of which a number of 2.127 interventions were focused strictly on the common bile duct alone. This retrospective study is a multicentric one, conducted over a period of 40 years, in both Caritas Clinical Hospital and afterwards in Witting Clinical Hospital, in Bucharest.
Results
The surgical reconstructive options for repairing the lesions of the CBD, can be brought toghether into the following classification:
- Reconstructive methods, which keep the integrity of the main biliary way;
- Derivative methods, respectively biliodigestive anastomoses;
- Substitutive methods, which use allograft or allograftings.
Based on the above-mentioned custom anatomo-clinical classification and with the surgical reconstructive options in mind, now we shall discuss our chosen surgical strategies for the selected lot of 53 patients.
Options for injuries immediately recognized at the time of surgery.
In this category, we encountered the following situations:
- -
- 6 cases of small loss of substance (one laparoscopically performed),
- -
- 5 partial or total sections of the CBD, from whom 2 laparoscopically performed, and
- -
- 3 segmentary loss of the biliary wall duct substance, between 1.5 cm and 3 cm distance.
The main obstacles of these cases were the absence of dilatation of the biliary stump, due to the immediate timing of the discovery and, although the CBD wall is strong and without inflammation (with a great chance to resist to the suture), the anastomosis is however difficult.
For cases with a small CBD breach we chose to repair via direct suture with the mandatory Kehr or transcystic drainage, kept in place for a minimum of 18 days. This category includes cases with a defect of 3-5 mm and a normal aspect of the biliary wall. The Kher external drainage is for protection, recalibration, prosthesis and decompressing of the final montage. For the single laparoscopic case the solution was the 2 points suture of the defect with a Vicryl™ 4.0 thread, and placing the appropriate transcystic drainage.
For cases with a large CBD breach we chose the solution of the patch procedure and the corresponding external axial biliary drainage. The patch is produced from the gallblader wall.
For cases with a partial or total section of the CBD, the solution is to perform a reconstruction of the common bile duct with the aid of anastomoses protected by a transcholedocohepatic axial drainage, kept in place for less than 2 months. The bilio-digestive anastomosis is a good choice, especially in the hepatico-jejunostomy termino-lateral variant, both when the lesion is discovered immediately or in the later stages.
Of these cases, one involving laparoscopic accidental section of the common bile duct had the most unexpected evolution ever encountered in our surgical practice, and this particular abnormal evolution was later blamed on the excessive devascularisation made by the mobilization and dissection of the common bile duct with the hook-type monopolar electrode, in our attempt to prepare it for transection and clipping, as it was mistaken with the cystic duct. In this case, the head to head anastomosis performed as the method of choice for intraoperative repair, developed later on an anastomotic stenosis, which in turn developed a biliary “hour-glass” shaped lithiasis. However the complications did not stop there, the patient being readmitted later on with the diagnosis of hepatic abcesses, a rather rare but alarming clinical situation. For this reason, in other cases of accidental laparoscopical section of the common bile duct and the biliary convergence, we now adopt another solution and we therefore recomend performing a hepatico-jejunostomy, after cutting the biliary proximal stump far enough in order to reach the fully vascularized and oxygenated tissue.
Options for the early postoperative period
This postooperative period is concerned mainly with lesions with an covert profile, lesions that have not been properly recognized during the initial surgery. The early consequences of the unrecognized and ignored lesions are represented by the biliary fistulae, with defects that output the biliary content directly into the peritoneum and thus developing choleperitoneum. Our study reported 10 early complications of the common bile duct whose lesions had not been yet divided or enclosed by postoperative perivisceritis.
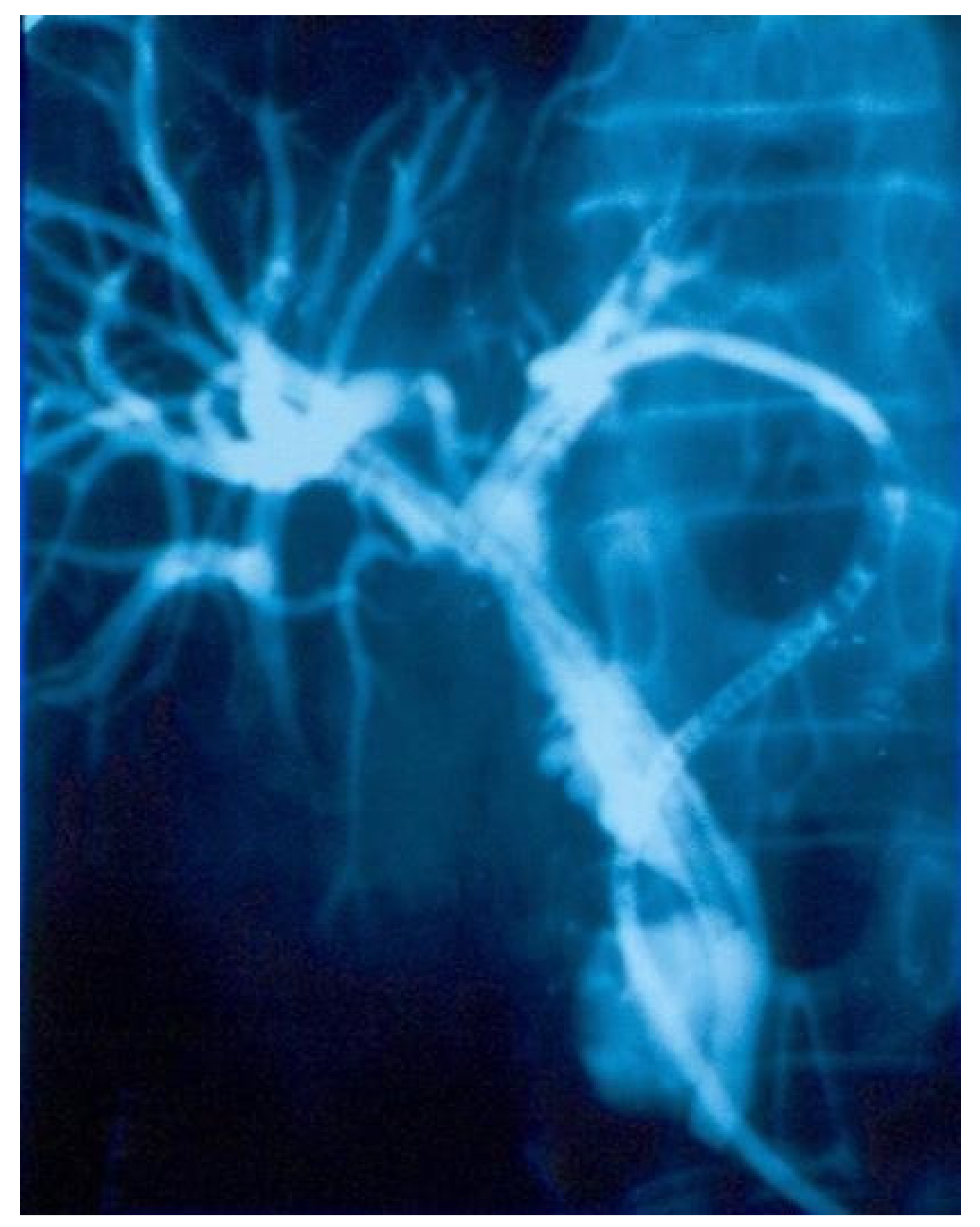
From this lot we present an interesting case of biliary fistulae of the left hepatic duct that was submitted in our service from another clinic, for surgical reevaluation. The CBD lesion was resolved there with the aid of a choledochoduodenostomy which, unfortunatelly, in the postoperative stage developed an anastomosis stenosis and a consecutive obstructive jaundice. Our solution to resolve this complication was, after the dilatation and recalibration of the choledochoduodenal anastomosis, to perform a double axial transanastomotical drainage of the left and right hepatic duct, this drainage being exteriorized in a transparietohepatic and transomphalic way, virtually without any suture of the fistulae. The reasons behind this decision were: the fragility of the left hepatic duct due to external fistula, the inability to a good cicatrisation, the clear advantage of an axial external biliary drainage of being able to recalibrate, decompress and protect the suture. Therefore, we achieved perfect cicatrisation of the fistulae after 3 months of continuous axial transcholedocohepatic prothesis (Figure 1). In this group of cases, the biliodigestive anastomoses were later on complicated by early recurrent fistulae in 2 cases and with stenosis in 1 case.
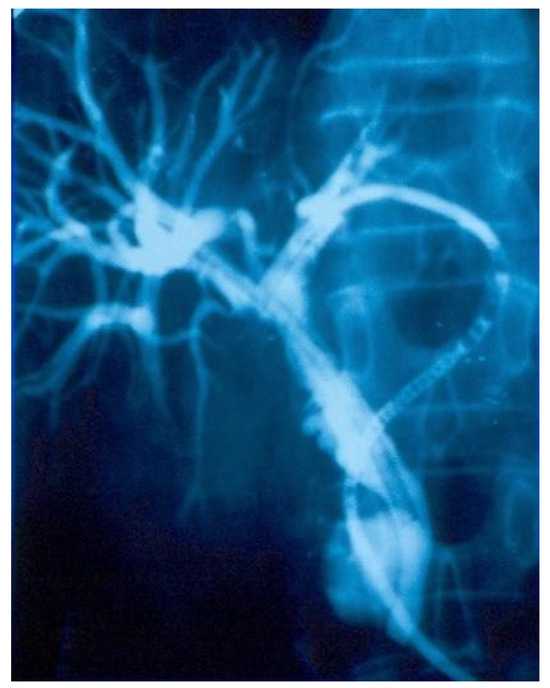
Figure 1.
C-Arm colangiographic control in preparation for patient discharge, performed after 3 months of continuous drainage. The slide exhibits no signs of fistulae and therefore a good choledochoduodenal anastomosis was achieved.
Options for the late stage complications
This period covers a wide area in time, stretching from 1 month postoperative up to several years after the initial surgery, and this slow development can be explained either due to a slow-growing stitch-related granulomas, a reaction that in turn develops stenosis of the biliary ducts and sometimes can produce extensive sclerosing colangitis.
Our report recorded a total of 29 cases of late-stage complications, from which 20 cases of late stenosis of the intrahepatic biliary ducts and 9 cases of stenosis associated with consecutive biliary fistulaes.
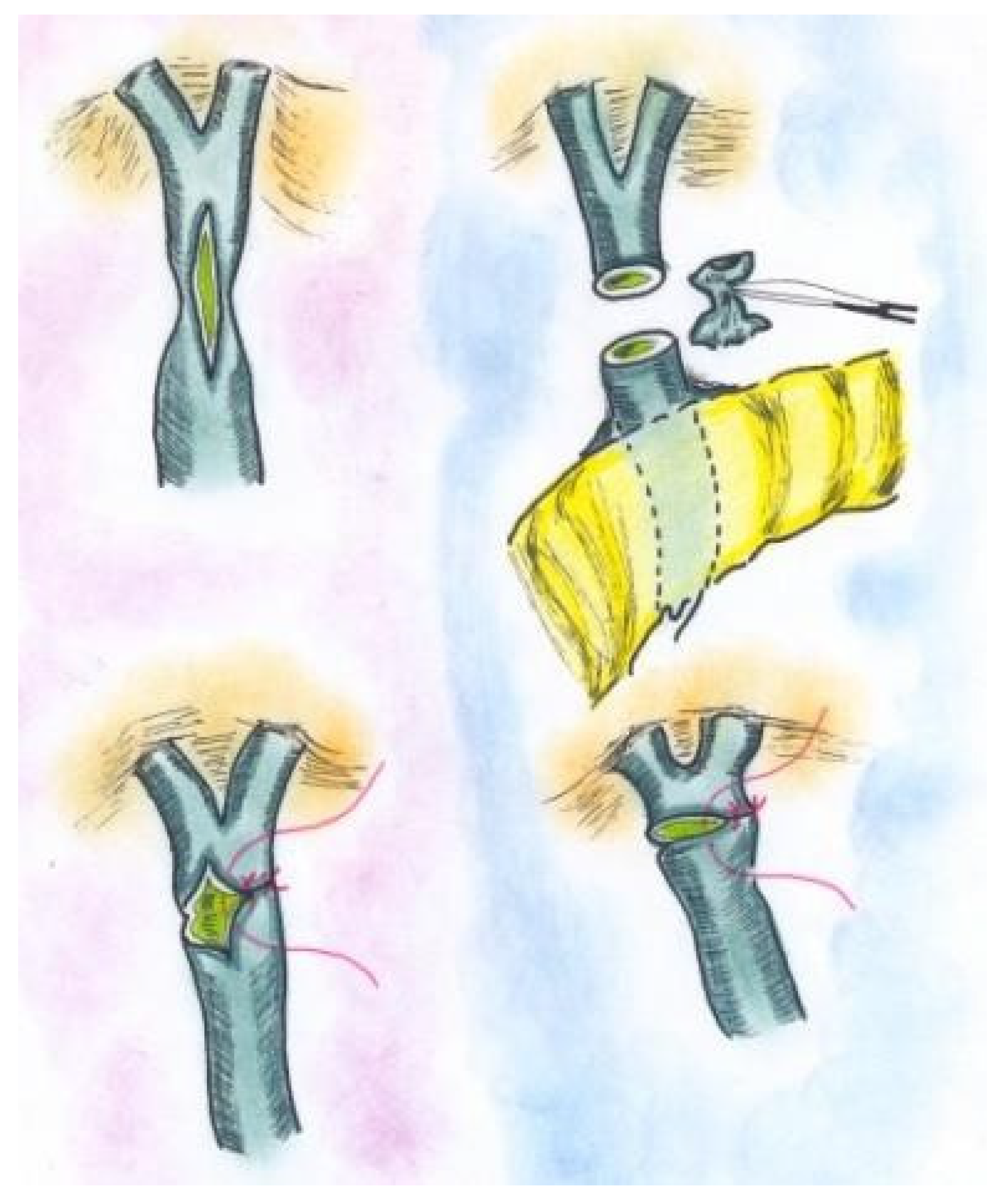
According to the Bismouth classification already discussed [1], our surgical solution for type I lesions was choledochoplasty or an end-to-end terminal reconstruction after excision of the biliary stenossing diaphragm (Figure 2). Lesions of type II, with a biliary stump shorter than 2 cm and an associated dilated biliary pathway above the stenosis, encountered in our study after 2 Kehr-type biliary drainages, received as solution a bilio-digestive anasthomosis protected by a biliary transanastomotic axial drainage.
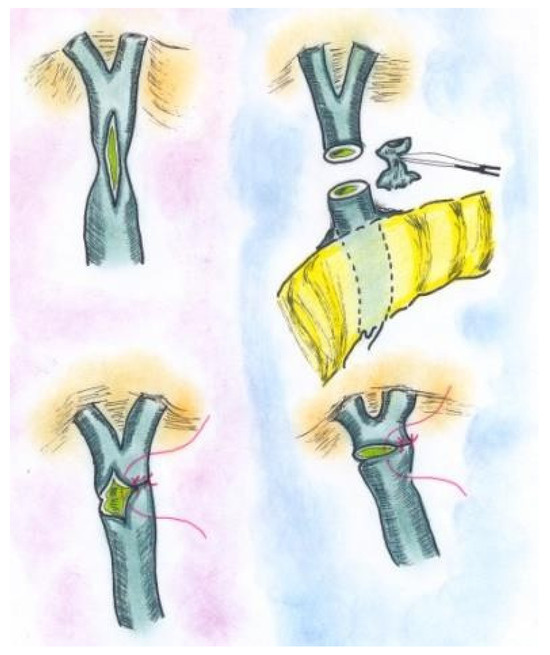
Figure 2.
A schematic graphical representation of the procedure. There are 2 variants available: the excision of the stenotic diaphragm and a end-to-end anastomosis, or longitudinal incision with a transverse suture of the resulting defect.
The multiple layered and ranged stenosis of the common bile duct, all the way up to the biliary confluence with the cystic duct, namely Bismuth type III lesions, were solved by adopting the so-called “France Connection” derivation, better known as the Hepp-Couinaud bilio-digestive anasthomosis of the biliary convergence [7,8], or by the Goinard transduodenal and transpapillary transoddian cathetherism of the main biliary way [9,10], in the eventuality that the main biliary duct could not be indentified in the open surgery approach.
We report only one case of endoscopical recalibration performed for a late stenosis of the choledochoduodenostomy made for a biliary fistula of the common bile duct, but concerning this endoscopical recalibration procedure, our experience is fairly limited and indirect, since we have not encountered any case up to the present, all cases being submitted to another service of gastroenterology.
Discussion
Regarding the intraoperative discovered lesions, we can now affirm that an end-to-end bilio-biliary anastomosis is a viable option and therefore accepted by the surgical community due to the fact that both ends usually come in close proximity and that there is no need for a more advanced dissection for mobilization. Also, there is little to no tension on the anastomosis. However, while this statement might be true for open surgery, during the laparoscopic procedures, where the hook-type monopolar electrode is widely used, the 2 stumps of the resulting transection are often presented with a partial or integral devascularisation and thus an end-to-end anastomosis might be compromised. In this regard, it would be best for a surgeon to perform a transanastomotical protection and prosthesis of the suture, either by an axial external transcholedocohepatic drainage tube or by the means of a transomphalic drainage on the left side or transparietohepatic way on the right side. This procedure could very well ensure a successful outcome of the reconstruction, if kept in place for several months.
The second disadvantage of the laparoscopic transsection of the main biliary duct is the normal diameter of the 2 resulting stumps, which further translates into the impossibility of using stenting or endoscopical prosthesis and thus the need for an external axial and transanastomosis biliary drainage performed for the protection of the biliary anastomosis [11,12].
For this reason, even after performing a hepatico-jejunal anastomosis as a derivative method, we considered it necessary to associate a second latero-lateral duodeno-jejunal anastomosis on the same jejunal loop, with 2 resulting advantages: to allow the trans anastomosis draining tube to be properly evacuated on the nasal-gastric way, and to allow further postoperative visiting by the means of endoscopical procedures.
However we still have an alternative, even in the situation when the 2 resulting stumps are not dilated. We can always rely on the hepaticojejunostomy without suture (HJWS), published by E. Bratucu [13,14].
Regarding our experience with the early postoperative stage lesions, we can conclude that, in these cases, the main challenges are: the undilated main biliary way, the biliary infiltration, congestion and edema, which in turn cause of the friability of the ductal wall, and thus rendering it unusable for a suture, a high risk for the choledochotomy to create a new biliary breach, bleeding dissection and last but not least, a CBD that is very difficult to approach and identify– although this can be overcome with the aid of the Goinard procedure. These cases therefore impose a different therapeutical approach, like an isolated external biliary drainage which proved to be an efficient decompressing procedure, kept in place for less than 3 months [15].
As for the late postoperative stage, our experience shows that nowadays these kinds of cases are best solved by the endoscopical papilosphicterotomy (PSO) techniques, and only when the endoscopic recalibration and stenting fails to solve them, open surgery offers an adequate option. However, we only have limited and indirect experience with such methods and further comparative study is under evaluation.
In all cases when the convergence of the main biliary way is easy to identify by the intraoperative cholangiography technique, the Hepp-Couinaud derivation or a termino-lateral hepatico-jejunostomy, protected and calibrated by an external biliary axial drainage, is the best option.
The case of a suprastenotic biliary fistulae usually generates a tendency to develop subhepatic abscesses. If this occurs, it is best to perform a high bilio-digestive anastomosis or derivation, above the level of the biliary fistulae with the mandatory protection of a double axial bile ducts drainage.
Conclusions
Based on our experience with the above mentioned cases of laparoscopic and open-surgery lesions of the CBD, we drafted a general algorithm laid out with all considerations that we had in mind at the time of diagnosis and the corresponding results of our chosen method for repair. Some of these choices led to immediate resolution of the case, some led to even more complications that involved further detailed analysis of choices at hand. This synopsis, in our opinion, can serve as a planning guide for choosing the optimal surgical strategy in order to resolve the one case of iatrogenic lesion of the CBD.
As can be seen from the algorithm, our conclusion is that the total CBD strictures or stones represent surgical cases, but the optimal approach in the partial strictures is to wait. Biliary peritonitis and biliary leakage represent contraindications for anastomosis.
Therefore, for a surgeon facing an immediate recognized aparoscopic lesion of the CBD, the first question he has to answer is to convert or not?
- A.
- If one chooses to convert, there are several choices:
- A.1.
- Convert and repair; in this case, one must ask a critical question. How to repair?
- By bilio-biliary suture with or without T tube or Axial drainage;
- By choledocho-duodenostomy;
- By Roux loop jejunostomy;
- Other options
The chosen solution in our case was a Roux-type loop heptico-jejunostomy, even if the diameter of the bile duct was 6 mm. After 1 year, we noticed jaundice and angiocolitis. Further available options:
- Wait more time: 2 to 3 weeks with antibiotics;
- A secondary open intervention for biliary repair;
- Percutaneus biliary dilatation without prosthesis;
- Percutaneus biliary prosthesis;
- Endoscopic biliary prosthesis;
For options 4 and 5 of course, we must further investigate the possibility of using metallic or polyethylene prosthesis. Our chosen solution was a percutaneus biliary dilatation without prosthesis. However, after 2 years, the patient developed a colangitis without jaundice. The cholangio-MRI shows a bilateral dilatation of the biliary ducts, with a stone in the left hepatic duct. Available options at this point:
- Percutaneus desobstruction and dilatation;
- Percutaneus prosthesis;
- Open third-step surgical biliary repair;
- Wait even more: 2-3 weeks with anti-inflammatory and antibiotics treatment;
- Endoscopic extraction of left hepatic stone and prosthesis.
We chose the open surgical biliary repair consisting of dissection of the hilar plate and extraction of the stone from the left hepatic duct with the “French Connection” Roux-type loop heptico-jejunostomy with the biliary convergence extended on the left hepatic duct.
- A.1.
- Convert and no repair at all;
- A.2.
- Call an expert for professional assessment.
- B.
- No conversion and no repairing.
- Available options:
- B.1.
- Peritoneal drainage
- B.2.
- Drainage of the extremity of the bile duct
- B.3.
- Common bile duct ligature
In the last option, we transformed the peritonitis in a bile leakage, waiting for the bile duct to reach at least 10 mm inner diameter and thus being ready for anastomosis. We can then perform a Roux loop hepaticojejunostomy or the HJWS. In the first 2 variants, our experience showed that the evolution was generally by bile leakage extension and biliary peritonitis. In this case, we offer several further available solutions:
- Endoscopic cholangiography;
- No surgical;
- Sugical classic approach;
- Laparoscopic approach for peritoneal lavage and drainage and echografic control of the collection.
Acknowledgments
This scientific material is part of a lager retrospective study of a PhD thesis, currently under development by Moldovan Cosmin, M.D., Ph. D. Sudent at the Carol Davila University of Medicine and Pharmacy, Bucharest, with Prof. Vladimir Belis. M.D., PhD., as thesis coordinator. The thesis has the following title: “Contributions to the forensic and legal study regarding the consequences of the iatrogenic lesions of the main biliary pathways occurred during the laparoscopic approach of hepato-bililary surgery”. All authors have read and approved the final manuscript and also declare no conflicts of interest.
References
- Bismuth, H.; Lazorthes, F. Operative injuries of the common biliary duct. Journal de chirurgie 1981, 118, 601–9. [Google Scholar] [PubMed]
- Strasberg, S.M.; Callery, M.P.; Soper, N.J. Laparoscopic surgery of the bile ducts. Gastrointestinal endoscopy clinics of North America 1996, 6, 81–105. [Google Scholar] [CrossRef] [PubMed]
- Mihaileanu, F.; Zaharie, F.; Mocan, L.; Iancu, C.; Vlad, L. Management of bile duct injuries secondary to laparoscopic and open cholecystectomy. The experience of a single surgical department. Chirurgia 2012, 107, 454–60. [Google Scholar] [PubMed]
- Ungureanu, F.D.; Straja, D.; Ungurianu, L.; Pricop, M.; Toba, M.; Moldovan, A.C. Leziuni accidentale laparoscopice ale caii biliare principale. Reconstructie sau derivatie? Chirurgia 2009, 104, 1. [Google Scholar]
- Schiappa, J.M. Iatrogenic lesions of the biliary tract. Acta chirurgica Belgica 2008, 108, 171–85. [Google Scholar] [CrossRef] [PubMed]
- Myburgh, J.A. The Hepp-Couinaud approach to strictures of the bile ducts. I. Injuries, choledochal cysts, and pancreatitis. Annals of Surgery 1993, 218, 615–20. [Google Scholar] [CrossRef] [PubMed]
- Goinard, P.; Pelissier, G. Ideal choledochotomy & sphincteroplasty in lithiasis of the common bile duct. Afrique francaise chirurgicale 1957, 15, 235–47. [Google Scholar] [PubMed]
- Bratucu, E. Hepaticojejunostomy. Chirurgia 2005, 100, 159–62. [Google Scholar] [PubMed]
- Macedo, F.I.; Casillas, V.J.; Davis, J.S.; Levi, J.U.; Sleeman, D. The value of cholangiography through Jackson-Pratt drains in the management of postoperativebiliary injuries. Am Surg. 2014, 80, 66–71. [Google Scholar] [CrossRef] [PubMed]
- Brătucu, E.; Straja, D.; Cirimbei, C.; Alecu, M.; Nechita, D. Double suturless hepatico jejunostomy. Chirurgia (Bucur). 2011, 106, 375–8. [Google Scholar] [PubMed]
- Mercado, M.A. Current management of benign and malignant bile duct strictures. Rev Gastroenterol Mex. 2011, 76, 120–5. [Google Scholar] [PubMed]
- Turcu, F.; Dragomirescu, C.; Pletea, S.; Bănescu, B. The problem of iatrogenic common bile duct injury, or the picture of an iceberg peak. Chirurgia (Bucur). 2011, 106, 187–94. [Google Scholar] [PubMed]
- Mercado, M.A.; Domínguez, I.; Arriola, J.C.; Ramirez-Del Val, F.; Urencio, M.; Sánchez-Fernández, N.
- Right and left partial iatrogenic injuries of the biliary tree. Therapeutic options. Rev Invest Clin. 2010, 62, 214–21.
- Osuna-Rubio, J.; Hermosillo-Sandoval, J.M.; López-Guillén, G.; Maciel-Miranda, A.; Fuentes-Orozco, C.; Alvarez-Villaseñor, A.S.; González-Ojeda, A.; López-Ortega, A. Association between wound size after open cholecystectomy with severity of iatrogenic biliarytract lesions. Gac Med Mex. 2008, 144, 213–8. [Google Scholar] [PubMed]
© 2016 by the author. 2016 Cosmin Alec Moldovan, Dan Florin Ungureanu, Vladimir Beliș.