Highlights
- ✓
- Even if nasopharyngeal tumors are usually diagnosed at an advanced stage, there are procedures for the effective and rapid diagnosis of nasopharyngeal tumors, which is essential for timely therapeutic interventions and optimizing results.
- ✓
- Patients turn to the doctor most of the time for the appearance of a lump in the neck region or repetitive epistaxis, but the number of cases with an otic onset seems to be increasing recently.
Abstract
Malignant nasopharyngeal tumors account for approximately 4% of ENT malignant tumor pathology and 1% of all cancers. The diagnosis of nasopharyngeal tumors is often late, the reason being the location in a silent anatomical region in terms of symptomatology and accessibility. Thus, approximately 70% of newly diagnosed patients with nasopharyngeal carcinoma unfortunately present with the condition in an advanced local stage. The early signs and symptoms are varied (nasal obstruction, hearing loss, otalgia, headache) and are usually ignored by the patient and even by the doctor in the initial stage of nasopharyngeal tumor evolution. Approximately 5% of patients have systemic metastases at presentation, the most common location being bone. Latent Epstein-Barr virus infection appears to be involved in the pathogenesis of nasopharyngeal carcinoma. There is no exact evidence of how often a nasopharynx tumor’s first sign is unilateral hearing loss. Thus, further work is required to determine that exactly to help patients get diagnosed faster and therefore improving their therapeutical options. This study aims to explore which symptoms are most common as the first indication of NPC, as well as how these symptoms compare to each other in terms of frequency and likelihood of occurrence.
Introduction
Cancer is a public health problem, due to its high frequency among the population, the negative consequences and the impact they determine in social and economic terms. Cancer represents an entity with a great impact on the individual, family and society in general, being the second cause of morbidity and mortality, after cardiovascular diseases dominating the morbid table of 21st century. Cancer diagnosis must be done in specialized medical units correlating several diagnostic techniques, performing a complete assessment of the case to identify the extent of a tumors and allow the identification of the most effective scheme of therapeutic conduct [1,2].
The orifice of the Eustachian tube (ET) is located in the nasopharynx, so nasopharyngeal disorders cause otitis media with effusion. Nasopharyngeal observation is necessary for patients showing middle ear effusion, especially in elderly populations [3,4]. Rarely, tumors develop near the ET or in contact with it, therefore middle ear disorders may appear. A complete examination is necessary for patients with unilateral persistent serous otitis media and also it is imperative to take biopsies from the nasopharyngeal mucosa [5,6,7].
Another aspect which needs to be taken into consideration is the fact that the Epstein-Barr virus (EBV) is associated with multiple types of human cancer, including lymphoid and epithelial cancers, but the closest association with EBV infection is seen in undifferentiated nasopharyngeal carcinoma [5,6]. Various studies have identified links between the prevalence of human leukocyte antigen (HLA) class I genes in specific populations and the likelihood of developing nasopharyngeal carcinoma (NPC). There are reported associations between ethnicity, geographic location, and the incidence of the disease. Populations in regions with a higher NPC risk often show HLA distribution patterns that differ, and sometimes even contrast, with those in low-risk areas. Meanwhile, populations in areas with moderate NPC incidence exhibit a distinct HLA distribution pattern. Two primary explanations could account for this connection between HLA phenotype distribution and NPC risk across different populations [8,9].
Materials and Methods
This study focused on patients diagnosed with nasopharyngeal tumors, selected from a cohort of individuals presenting at the ENT Clinic of Constanta Emergency Hospital between September 2022 and July 2024. Inclusion criteria comprised patients aged between 18 to 75 years, with histologically confirmed nasopharyngeal tumors. Exclusion criteria encompassed patients with a history of other malignancies or incomplete medical records. Parameters investigated included patient demographics (age, gender), tumor characteristics (stage, histological type, and grade), treatment modalities (surgery, chemotherapy, radiation therapy), and clinical outcomes (progression-free survival, overall survival). By systematically analyzing the clinical and pathological characteristics of patients with nasopharyngeal tumors and employing rigorous statistical methods, this study aimed to provide comprehensive insights into the prognostic factors and therapeutic strategies for improving patient outcomes.
To derive these statistics, we analyzed the frequency distribution of initial presentations among patients diagnosed with nasopharyngeal carcinoma (NPC) in our clinic. We categorized the symptoms into three primary groups: nasal, otic, and cervical lymphadenopathy. By calculating the percentage of cases in each category, we established the relative frequency of each symptom presentation.
For proportional representation, we compared each symptom category relative to the others by calculating ratios based on their respective frequencies. This allowed us to quantify the likelihood of one symptom group being more common than another among the patient population.
The patient-to-patient ratios were derived by directly comparing the number of patients presenting with each symptom type. These ratios offer a practical comparison of how often one symptom group occurs in relation to another. By systematically evaluating these frequencies and proportions, we provided a detailed comparative analysis of initial symptom presentations in NPC patients.
Results
Comparative Analysis of Debut Presentations
- Relative Frequency of Each Presentation
- o
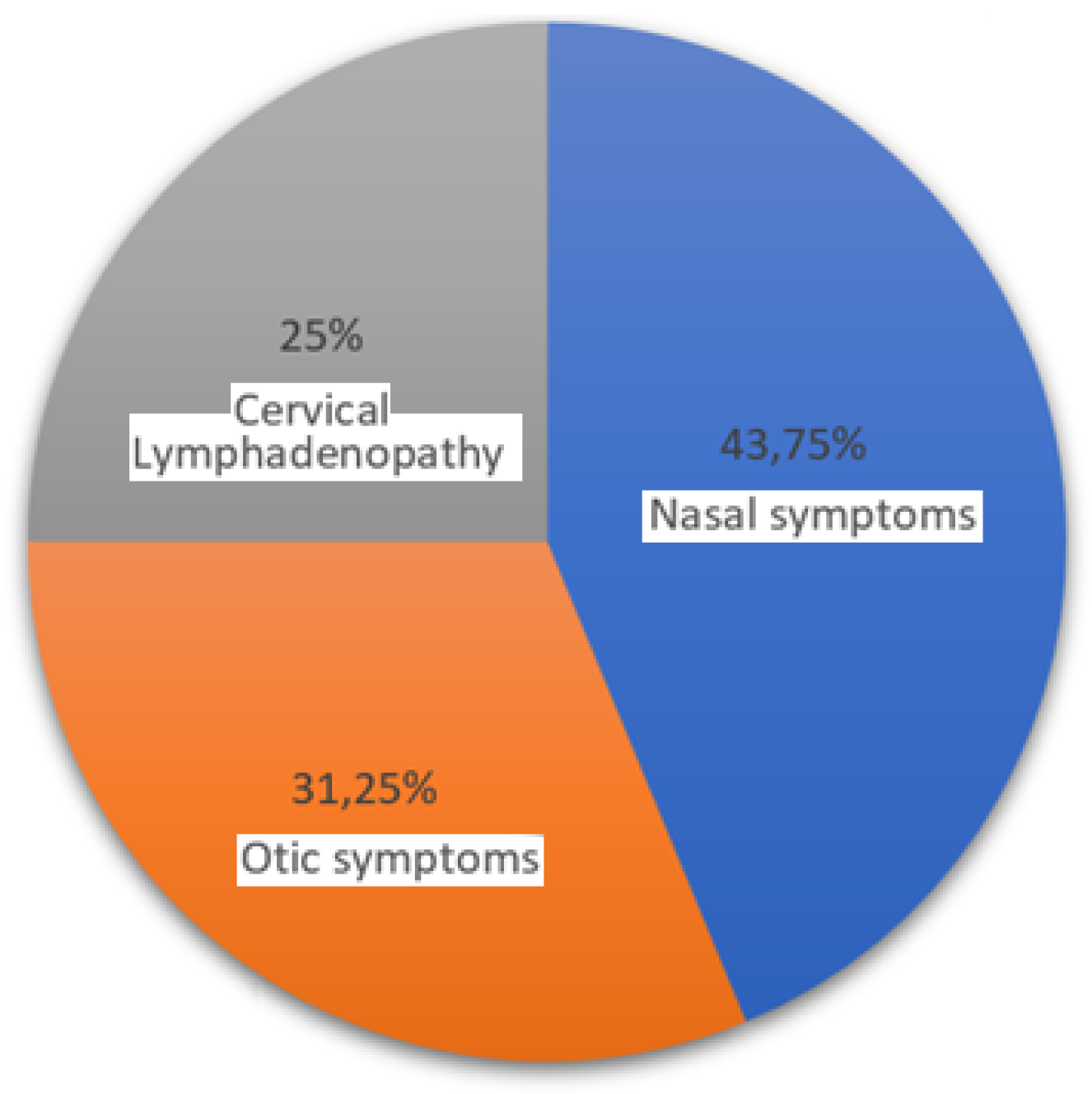
- Nasal Symptoms. These were the most frequent presentation in your clinic, seen in 43.75% of cases. This suggests that nearly half of the NPC patients initially present with symptoms related to the nasal area, like nosebleeds or nasal obstruction.
- o
- Otic Symptoms. Otic symptoms, including hearing loss or ear fullness, were the second most common, observed in 31.25% of cases. This indicates that otic presentations are also quite prevalent, making up almost one-third of the cases.
- o
- Cervical Lymphadenopathy. This presentation, characterized by neck masses, was the least frequent, found in 25% of the patients. This is still a significant proportion, emphasizing that a quarter of NPC cases may initially present with neck lymph node.
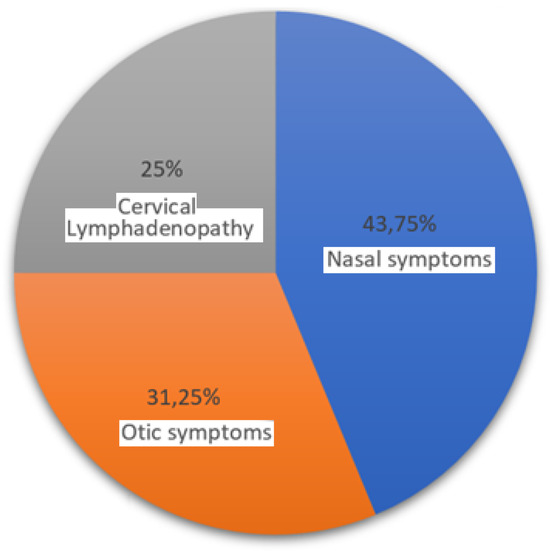
Figure 1.
Relative frequency of each presentation.
Figure 1.
Relative frequency of each presentation.
- 2.
- Proportional Representation
- o
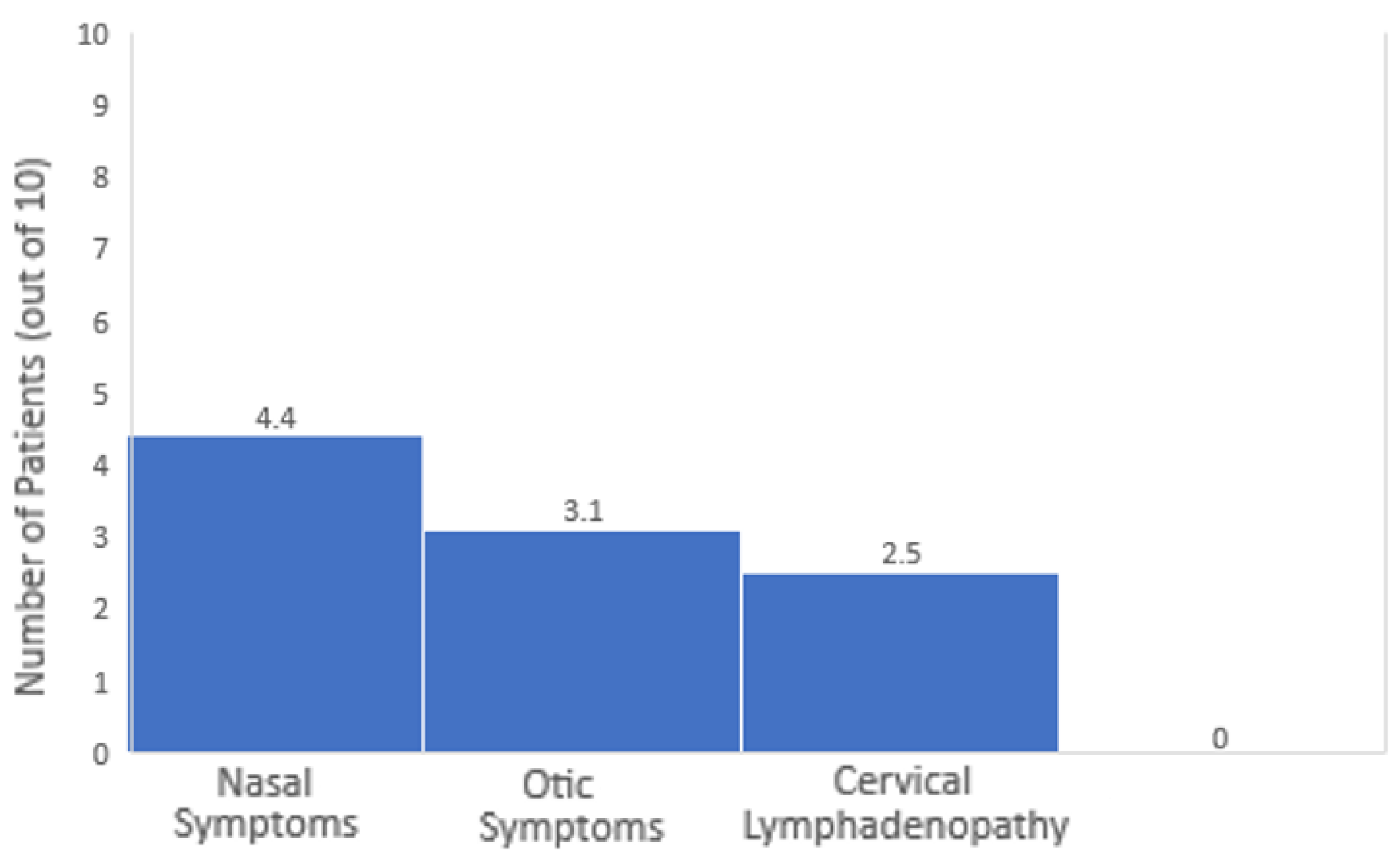
- Nasal vs. Otic Symptoms. Nasal symptoms were more common than otic symptoms. For every 10 patients, approximately 4.4 had nasal symptoms, while about 3.1 had otic symptoms. Thus, nasal symptoms are about 1.4 times more likely to be the presenting feature than otic symptoms.
- o
- Nasal vs. Cervical Lymphadenopathy. Nasal symptoms were significantly more common than cervical lymphadenopathy. For every 10 patients, around 4.4 had nasal symptoms compared to 2.5 with cervical lymphadenopathy. Therefore, nasal symptoms are 1.75 times more likely than cervical lymphadenopathy to be the initial presentation.
- o
- Otic Symptoms vs. Cervical Lymphadenopathy. Otic symptoms were generally more frequent than cervical lymphadenopathy, being seen in about 3.1 out of every 10 patients compared to 2.5 out of 10. This makes otic symptoms 1.25 times more likely to be the initial presentation than cervical lymphadenopathy.
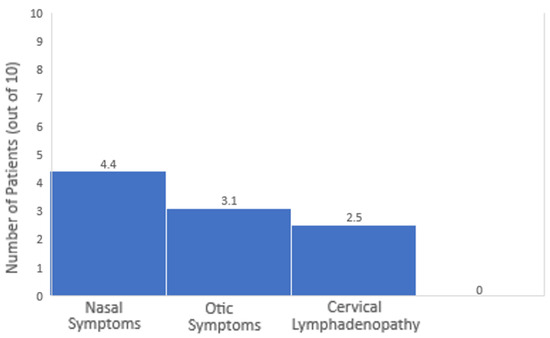
Figure 2.
Frequency of nasal, otic and cervical lymphadenopathy.
Figure 2.
Frequency of nasal, otic and cervical lymphadenopathy.
- 3.
- Patient to Patient Ratios
- o
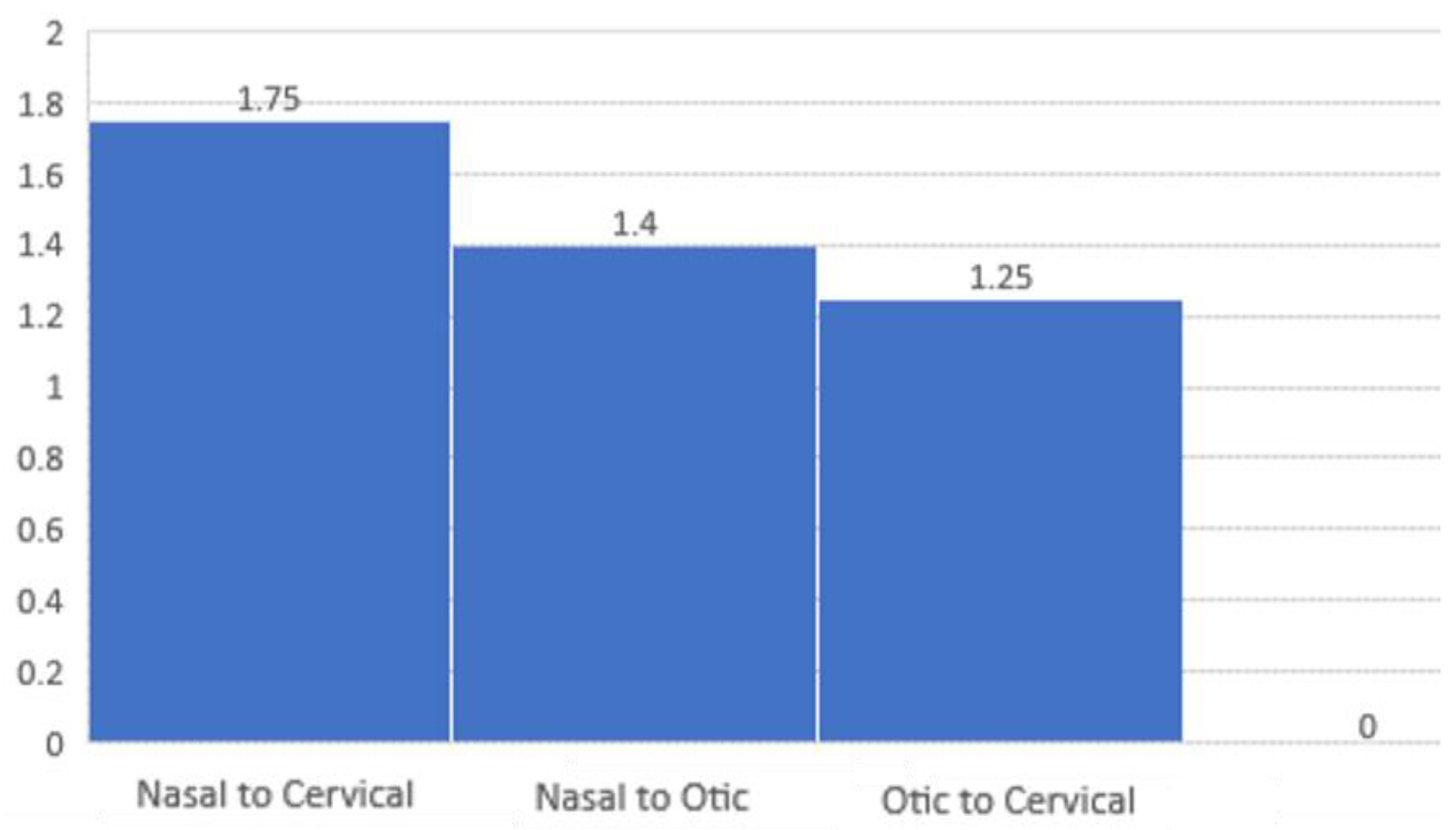
- Nasal to Otic Symptoms. For every 1 patient presenting with otic symptoms, there were 1.4 patients presenting with nasal symptoms.
- o
- Nasal to Cervical Lymphadenopathy. For every 1 patient with cervical lymphadenopathy, there were 1.75 patients with nasal symptoms.
- o
- Otic Symptoms to Cervical Lymphadenopathy. For every 1 patient with cervical lymphadenopathy, there were 1.25 patients with otic symptoms.
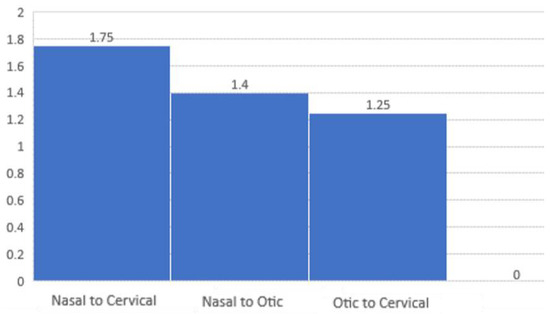
Figure 3.
Patient to patient ratios.
Figure 3.
Patient to patient ratios.
Discussions
Nasopharyngeal cancer, the incidence of which has been continuously increasing in recent years in our country as well, although known since antiquity as a pathological entity, it raises important and interesting diagnostic and treatment problems. The special problems of establishing the diagnosis derive, first of all, from accessibility reduced of this anatomical region, in the center of the craniofacial massif, the examination of the cavity being definitely the more difficult exam practiced in the ENT specialty and, at the same time, very difficult to interpret [10,11,12]. The cavity is a region very rich in lymphatic tissue, which is often invaded by the neoplastic product of the epithelium or of the supporting tissue, determining forms that create confusion in the classification of these tumors and their assessment from a histopathological point of view [12,13,14]. In addition to the anatomical, structural and complex relationship peculiarities, the mode of onset, the long and mute evolution, later combined with the symptoms borrowed from the neighboring organs and, on the other hand, the weight of a quality examination frequently delays the diagnosis and application of treatment, having therefore as a consequence the worsening of the prognosis [15,16].
There were 16 new cases diagnosed in Constanta between September 2022 and June 2024 and three of them will be presented in this article. All the new cases diagnosed in the period stated above were unfortunately diagnosed in an advanced stage. Diagnosing a nasopharynx tumor may be difficult for several reasons:
- Hidden area. The area is not easily accessible, and the tumor may not be visible during a routine physical examination [17].
- Non-Specific Symptoms. Early-stage nasopharyngeal tumors may not cause specific symptoms, or the symptoms may be nonspecific, such as nasal congestion, a sore throat, or earache. These symptoms can be attributed to various common illnesses, leading to delayed diagnosis [18].
- Similar Symptoms to Other Conditions. Symptoms of nasopharyngeal tumors, such as nosebleeds, ear problems, and neck lumps, can be indicative of various other conditions, making it challenging to attribute them specifically to a nasopharyngeal tumor without further investigation [19].
- Silent Development. In some cases, nasopharyngeal tumors can develop silently without causing noticeable symptoms until they reach an advanced stage. This makes early detection less likely [20].
- Rare Nature of the Tumor. Nasopharyngeal tumors are relatively rare compared to tumors in other head and neck regions. This rarity can contribute to a lack of awareness among healthcare professionals, leading to delayed consideration of nasopharyngeal tumors in the diagnostic and treatment processes [21].
- Asymptomatic Carriers of Epstein-Barr Virus (EBV). Nasopharyngeal carcinoma is strongly associated with Epstein-Barr Virus (EBV) infection. However, many individuals with nasopharyngeal carcinoma may be asymptomatic carriers of EBV, and the presence of the virus alone may not be sufficient for diagnosis [8].
Even though a nasopharynx tumor is usually diagnosed in an advanced stage, there are ways to accelerate the diagnosis and efficient and timely diagnosis of nasopharyngeal tumors is crucial for optimizing patient outcomes and facilitating timely therapeutic interventions. Early detection of nasopharyngeal tumors is crucial, as a smaller tumor burden, regardless of its resectability, significantly improves the prognostic outcome following treatment [22,23,24]. Advancements in diagnostic modalities have paved the way for more rapid and accurate identification of these tumors. Among the innovative approaches, imaging techniques such as magnetic resonance imaging (MRI) and computed tomography (CT) scans play pivotal roles in visualizing the nasopharyngeal region, delineating tumor boundaries, and assessing the extent of local invasion [25,26]. Additionally, the advent of molecular and genetic biomarkers, including Epstein- Barr virus (EBV) DNA testing and specific serum protein markers, offers promising avenues for early detection and the risk of stratification. Rapid advancements in endoscopic technologies, including high-definition flexible nasopharyngoscopes, has also enhanced the precision and speed of tumor visualization and biopsy procurement. Collaborative multidisciplinary approaches involving otolaryngologists, radiologists, pathologists, and molecular biologists further expedite the diagnostic process, ensuring comprehensive evaluation and timely initiation of personalized therapeutic strategies [27,28,29]. By harnessing the synergistic capabilities of advanced imaging technologies, molecular biomarkers, AI-driven analytics, and multidisciplinary expertise, clinicians can achieve faster and more accurate diagnoses of nasopharyngeal tumors, thereby improving patient prognosis and quality of life [30].
Although only 31.25% (5 out of 16) of the patients diagnosed in the previously mentioned period presented otic symptoms, even those who had an onset with laterocervical adenopathy (4 out of 16 or 25%) or epistaxis (7 out of 16 or 43.75%) declared that they had a slight decrease in hearing, which they ignored until the moment of presentation to the doctor. In our clinic, for the period mentioned above, nasal symptoms dominate as the initial presentation for NPC. Otic symptoms are also a significant presentation, occurring more frequently than cervical lymphadenopathy. Cervical lymphadenopathy is the least common debut but still an important aspect of NPC presentation [31,32,33].
A medical case will be discussed for each of the three distinct clinical onset pathways of nasopharyngeal carcinoma (NPC). First, we will delve into a case where NPC presents with otic symptoms, including hearing loss, tinnitus, or a sensation of ear fullness, often resulting from eustachian tube obstruction by the tumor. Second, we will explore a case where NPC initially presents through cervical lymphadenopathy, manifesting as palpable neck masses due to metastatic spread to regional lymph nodes, often prompting further diagnostic evaluation. Finally, we will examine a case where the disease manifests with nasal symptoms, such as epistaxis (nosebleeds) or nasal obstruction, reflecting the tumor’s local invasion and impact on the nasopharyngeal structures. By analyzing these cases, we aim to provide a comprehensive understanding of the varied clinical presentations of nasopharyngeal carcinoma, highlighting the diagnostic challenges and the importance of early detection and tailored therapeutic approaches [34,35].
- Case one
This is the case of a 45-year-old woman living in an urban environment who is a non-smoker and has been exposed to a toxic work environment. She has been undergoing outpatient treatment for serous otitis media for approximately six months. During a visit to the Ear, Nose, and Throat (ENT) clinic at SCJU Constanța, a nasopharyngeal fiberoptic laryngoscopy (NFL endoscopy) was conducted. During the endoscopy, a tumor was identified in the nasopharynx. Given the discovery of the tumor, the next step in the diagnostic process involves obtaining tissue samples from the tumor through a procedure called a biopsy. In this case, fragments from the tumor were collected and sent for histopathological (HP) examination. In the context of this case, the HP examination of the nasopharyngeal tumor fragments aims to determine the nature of the tumor—whether it is benign (non-cancerous) or malignant (cancerous) and, if cancerous, the specific type and characteristics of the cancer. The patient’s history of exposure to a toxic work environment may be relevant to the overall assessment, as certain occupational exposures can be associated with an increased risk of developing specific types of cancers.
The findings from the histopathological examination will be crucial in guiding further steps in the patient’s management, which may include additional imaging studies, staging of the tumor, and discussions about treatment options such as surgery, radiation therapy, or chemotherapy, depending on the nature and extent of the tumor. The multidisciplinary approach involving ENT specialists, pathologists, and potentially oncologists will be essential in providing comprehensive care for the patient.
- Case two
The second case presented is a case of a 55-year-old man who resides in an urban environment and is a smoker. He visited the Ear, Nose, and Throat (ENT) clinic with a complaint of a lump in his neck that has been growing larger over the past month. Given the symptoms, the healthcare provider performed a nasopharyngeal fiberoptic laryngoscopy (NFL endoscopy) on the patient. During the endoscopy, a nasopharyngeal tumor with an ulcerative-vegetative aspect was observed. The description "ulcerative-vegetative" suggests that the tumor exhibits characteristics of tissue breakdown (ulceration) and abnormal, vegetative (proliferative) growth. These features may raise concerns about the nature of the tumor, particularly regarding the possibility of malignancy. To further investigate the tumor and determine its nature, tissue samples (fragments) were taken from the nasopharyngeal tumor.
These samples will undergo a histopathological (HP) examination, which involves a detailed microscopic analysis of the tissue. Given the patient’s history of smoking, it’s important to note that smoking is a well-established risk factor for various cancers, including those of the head and neck region. The presence of a rapidly growing lump in the neck is concerning, as it may suggest the potential spread (metastasis) of the tumor to nearby lymph nodes.
The results of the histopathological examination will play a crucial role in determining the appropriate course of action for the patient. If the tumor is malignant, additional diagnostic tests, such as imaging studies, may be performed to assess the extent of the disease (staging). The treatment plan may involve a multidisciplinary approach, including surgery, radiation therapy, chemotherapy, or a combination of these, depending on the type and stage of the cancer.
Early detection and comprehensive evaluation are key in addressing potential malignancies, and the collaboration between ENT specialists, pathologists, and oncologists is vital in providing optimal care for the patient.
- Case three
In the final case presented in this article we have a 60-year-old male who visited the Ear, Nose, and Throat (ENT) clinic with complaints of nasal obstruction and difficulties breathing through his nose over the past two months. To investigate the cause of his symptoms, a Nasopharyngeal Fiberoptic Laryngoscopy (NFL endoscopy) was performed. During the endoscopy, a cyst was observed in the nasopharynx. A cyst is a closed, sac-like structure that can contain fluid, air, or other materials. In this instance, the cyst was located in the nasopharynx, which is the upper part of the throat behind the nose. To address the nasal obstruction and breathing difficulties, the decision was made to surgically remove the nasopharyngeal cyst. After the cyst was removed, tissue samples were sent for histopathological (HP) examination to analyze the structure of the cyst at a microscopic level.
The histopathological examination confirmed the diagnosis of a benign nasopharynx cyst which is unlikely to spread or invade surrounding tissues. Benign cysts in the nasopharynx can sometimes cause symptoms such as nasal obstruction and difficulty breathing, particularly if they grow in size or obstruct normal airflow.
The complete removal of the cyst is a common and effective treatment for benign cysts. Following the confirmation of the benign nature of the cyst, the patient can expect relief from the symptoms of nasal obstruction and breathing difficulties. Postoperative care may include monitoring for any signs of recurrence and providing instructions for a smooth recovery.
It’s important for the patient to attend follow-up appointments with the ENT specialist to ensure proper healing and to address any concerns. In this case, the diagnosis of a benign nasopharynx cyst and its successful removal highlight the importance of a thorough clinical evaluation, including endoscopic examinations and histopathological assessments, in providing accurate diagnoses and appropriate treatments for patients with nasal and pharyngeal conditions.
Fortunately, in none of the three cases was post-biopsy bleeding observed, indicating a favorable immediate outcome following the procedure. However, if bleeding had occurred, given the therapeutic options for managing nasopharyngeal bleeding, the combined use of intravenous and topical tranexamic acid may be a reasonable, safe, and non-invasive option for hemodynamic stabilization [10].
The first two HP results confirmed the diagnosis of an undifferentiated squamous cell type carcinoma. Undifferentiated squamous cell carcinoma is a type of cancer that arises from the squamous cells lining the nasopharynx. It is characterized by the presence of poorly differentiated cells, meaning they lack the normal features and organization of healthy cells. Further evaluation and staging of the cancer will be necessary to determine the extent of the disease and guide treatment decisions. This may involve additional imaging studies, such as magnetic resonance imaging (MRI) or computed tomography (CT) scans, as well as other diagnostic tests.
Recent studies indicate that gut microbiota might actively contribute to cancer development by influencing immune responses and inflammatory pathways. This emphasizes the necessity for comprehensive diagnostic strategies that consider microbial influences on tumor development. The differences in gut microbiota profiles observed between early- and late-onset colorectal cancer highlight the potential complexities in cancer pathogenesis, suggesting that similar variations may exist in nasopharyngeal tumors [11,36].
Treatment options for undifferentiated squamous cell carcinoma of the nasopharynx may include a combination of radiation therapy, chemotherapy, and surgery.
In the treatment and management of nasopharyngeal tumors, changing mentalities is a long-standing process, but the results in recent years are encouraging, particularly with advancements in personalized care and targeted therapies [37,38].
The specific treatment plan will depend on various factors, including the stage of the cancer, the location and size of the tumor, and the individual’s overall health.
It’s important for the patient to consult with her healthcare team to discuss the diagnosis, treatment options, and any further investigations or procedures that may be required. They will be able to provide personalized information and guidance based on her specific case [39].
Improving patient care and quality of life increasingly hinges on the ability to translate cutting-edge academic discoveries into practical applications within the healthcare system. Recent advances in diagnostic technologies, personalized medicine, and telehealth have opened new frontiers in patient management. By integrating these innovations into clinical practice, healthcare providers can offer more precise, effective, and patient-centered care. Bridging the gap between research and real-world implementation is essential to ensure that the latest breakthroughs in science result in tangible improvements in health outcomes and quality of life for patients [40,41].
Nasopharynx tumors can vary in shape and size. They may appear as a single mass or have irregular shapes. The size of the tumor can range from small to large, depending on the stage and aggressiveness of the tumor. The texture of a nasopharynx tumor can be variable. It may feel firm, solid, or even rubbery to the touch. The texture can provide additional information about the nature of the tumor, such as its composition and invasiveness [42,43,44].
Conclusions
The study highlights the challenges in diagnosing nasopharyngeal carcinoma, a cancer that is often detected late due to its difficult-to-access location, vague early symptoms, and ability to mimic other conditions. The cases reviewed were all diagnosed at advanced stages, underscoring the need for greater clinical awareness and earlier diagnostic efforts.
It also emphasizes the critical role of advanced imaging techniques like MRI and CT scans, as well as emerging molecular tests like Epstein-Barr virus DNA testing, in improving early detection and accurate diagnosis. A multidisciplinary approach, involving various specialists, is crucial for thorough evaluation and timely treatment. These findings also call for increased awareness about NPC among healthcare providers and the public to reduce late-stage diagnoses and enhance patient outcomes.
Institutional Review Board Statement
Any aspect of the work covered in this manuscript has been conducted with the ethical approval of all relevant bodies and that such approvals are acknowledged within the manuscript. Informed consent was obtained from all subjects involved in the study.
Conflicts of Interest
There are no known conflicts of interest in the publication of this article. The manuscript was read and approved by all authors.
Abbreviations
Ear, nose and throat—ENT; Eustachian tube—ET; Epstein-Barr virus—EBV; human leukocyte antigen—HLA; nasopharyngeal carcinoma—NPC; nasopharyngeal fiberoptic laryngoscopy—NFL.
References
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer Statistics, 2021. CA Cancer J Clin. 2021, 71, 7–33. [Google Scholar] [CrossRef] [PubMed]
- Sumi, T.; Tsunoda, A.; Shirakura, S.; Kishimoto, S. Mechanical obstruction of the eustachian tube by the benign tumor of the parapharyngeal space does not cause otitis media with effusion. Otol Neurotol. 2007, 28, 1072–1075. [Google Scholar] [CrossRef]
- Ars, B.; Dirckx, J. Eustachian Tube Function. Otolaryngol Clin North Am. 2016, 49, 1121–1133. [Google Scholar] [CrossRef]
- Komune, N.; Matsuo, S.; Miki, K.; et al. Surgical Anatomy of the Eustachian Tube for Endoscopic Transnasal Skull Base Surgery: A Cadaveric and Radiologic Study. World Neurosurg. 2018, 112, e172–e181. [Google Scholar] [CrossRef]
- Tsao, S.W.; Tsang, C.M.; Lo, K.W. Epstein-Barr virus infection and nasopharyngeal carcinoma. Philos Trans R Soc Lond B Biol Sci. 2017, 372, 20160270. [Google Scholar] [CrossRef] [PubMed]
- Sun, L.; Wang, Y.; Shi, J.; Zhu, W.; Wang, X. Association of Plasma Epstein-Barr Virus LMP1 and EBER1 with Circulating Tumor Cells and the Metastasis of Nasopharyngeal Carcinoma. Pathol Oncol Res. 2020, 26, 1893–1901. [Google Scholar] [CrossRef] [PubMed]
- Guo, R.; Mao, Y.P.; Tang, L.L.; Chen, L.; Sun, Y.; Ma, J. The evolution of nasopharyngeal carcinoma staging. Br J Radiol. 2019, 92, 20190244. [Google Scholar] [CrossRef]
- Banko, A.; Miljanovic, D.; Lazarevic, I.; Cirkovic, A. A Systematic Review of Epstein-Barr Virus Latent Membrane Protein 1 (LMP1) Gene Variants in Nasopharyngeal Carcinoma. Pathogens. 2021, 10, 1057. [Google Scholar] [CrossRef]
- Mazilu, L.; Ciufu, N.; Gălan, M.; et al. Postherapeutic follow-up of colorectal cancer patients treated with curative intent. Chirurgia (Bucur). 2012, 107, 55–58. [Google Scholar]
- Haldun, S.; Suceveanu, A.I.; Lupascu, M.; et al. Efficacy of tranexamic acid in nasopharyngeal hemorrhage; single center prospective study and literature review. J Mind Med Sci. 2024, 11, 189–194. [Google Scholar] [CrossRef]
- Herlo, L.F.; Salcudean, A.; Sirli, R.; et al. Gut Microbiota Signatures in Colorectal Cancer as a Potential Diagnostic Biomarker in the Future: A Systematic Review. Int J Mol Sci. 2024, 25, 7937, Published 2024 Jul 20. [Google Scholar] [CrossRef] [PubMed]
- Serban, D.; Smarandache, A.M.; Cristian, D.; Tudor, C.; Duta, L.; Dascalu, A.M. Medical errors and patient safety culture-shifting the healthcare paradigm in Romanian hospitals. Rom J Leg Med. 2020, 28, 195–201. [Google Scholar] [CrossRef]
- Nicoara, A.D.; Alexandrescu, L.; Tofolean, D.E.; et al. The Impact of Cardiac Rehabilitation on Quality of Life in Elderly Heart Failure Patients-Literature Review. Balneo and PRM Research Journal. 2024, 15, 723. [Google Scholar] [CrossRef]
- Lee, A.W.M.; Ng, W.T.; Chan, J.Y.W.; et al. Management of locally recurrent nasopharyngeal carcinoma. Cancer Treat Rev. 2019, 79, 101890. [Google Scholar] [CrossRef]
- Bossi, P.; Chan, A.T.; Licitra, L.; Trama, A.; et al. Nasopharyngeal carcinoma: ESMO-EURACAN Clinical Practice Guidelines for diagnosis, treatment and follow-up†. Ann Oncol. 2021, 32, 452–465. [Google Scholar] [CrossRef]
- Lee, H.M.; Okuda, K.S.; González, F.E.; Patel, V. Current Perspectives on Nasopharyngeal Carcinoma. Adv Exp Med Biol. 2019, 1164, 11–34. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Zeng, Z.; Wang, D.; Qin, G. Minimally Invasive Surgery for Early-Stage Nasopharyngeal Carcinoma. J Craniofac Surg. 2022, 33, e834–e837. [Google Scholar] [CrossRef]
- Zeng, C.; Qiao, M.; Chen, Y.; Xie, H. EBV-positive glycoproteins associated with nasopharyngeal carcinoma. Pathol Res Pract. 2024, 260, 155427. [Google Scholar] [CrossRef]
- Mints, M.; Tirosh, I. Nasopharyngeal carcinoma joins the single-cell party. Cancer Commun (Lond). 2020, 40, 453–455. [Google Scholar] [CrossRef]
- De Felice, F.; Marchetti, C.; Serpone, M.; et al. Upper-neck irradiation versus standard whole-neck irradiation in nasopharyngeal carcinoma: A systematic review and meta-analysis. Tumori. 2023, 109, 529–536. [Google Scholar] [CrossRef]
- Yin, L.; Li, Z.; Xue, G.; Lu, L. Nasopharyngeal carcinoma misdiagnosed as pituitary tumor with multiple cranial neuropathies. J Cancer Res Ther. 2021, 17, 1748–1750. [Google Scholar] [CrossRef]
- Zhang, W.G.; Liu, Z.Y.; Pang, S.W. Separation of nasopharyngeal epithelial cells from carcinoma cells on 3D scaffold platforms. Biotechnol Bioeng. 2021, 118, 1444–1455. [Google Scholar] [CrossRef] [PubMed]
- Kang, Y.; He, W.; Ren, C.; et al. Advances in targeted therapy mainly based on signal pathways for nasopharyngeal carcinoma. Signal Transduct Target Ther. 2020, 5, 245. [Google Scholar] [CrossRef]
- Trevisiol, C.; Gion, M.; Vaona, A.; et al. The appropriate use of circulating EBV-DNA in nasopharyngeal carcinoma: Comprehensive clinical practice guidelines evaluation. Oral Oncol. 2021, 114, 105128. [Google Scholar] [CrossRef]
- Lee, C.Y.; Wang, T.H.; Kao, Y.S. Chemotherapy, Radiation Therapy, and Nasopharyngeal Carcinoma. JAMA Oncol. 2024, 10, 1292–1293. [Google Scholar] [CrossRef] [PubMed]
- Petersson, F. Non-Keratinizing Nasopharyngeal Carcinoma with Adenomatous Differentiation. Head Neck Pathol. 2020, 14, 195–198. [Google Scholar] [CrossRef] [PubMed]
- Ganeson, S.K.; Saniasiaya, J.; Mohamad, I.; Abdul Gani, N. Basaloid Nasopharyngeal Carcinoma: An Entity That Remains Oblivious. Gulf J Oncolog. 2020, 1, 83–86. [Google Scholar]
- Chua, M.L.K.; Lua, J.Y.H.; Ng, W.T.; Lee, A.W.M. Management of the neck in nasopharyngeal carcinoma-time for a radical change? Chin Clin Oncol. 2023, 12, 8. [Google Scholar] [CrossRef]
- Jiang, S.; Zhou, H.; Ma, F.; Shen, H.; Lu, H. Acrometastasis of nasopharyngeal carcinoma: A case report. J Int Med Res. 2020, 48, 300060520924519. [Google Scholar] [CrossRef]
- Savlovschi, C.; Brănescu, C.; Serban, D.; et al. Amyand’s hernia--a clinical case. Chirurgia (Bucur). 2010, 105, 409–414. [Google Scholar]
- Liu, H.; Audino, A.N. Metastatic nasopharyngeal carcinoma mimicking nodular sclerosis Hodgkin lymphoma. Blood. 2020, 136, 2596. [Google Scholar] [CrossRef] [PubMed]
- Dai, L.; Fang, Q.; Li, P.; Wu, J.; Zhang, X. Secondary Squamous Cell Carcinoma of the Oral Cavity after Nasopharyngeal Carcinoma. Cancer Res Treat. 2020, 52, 109–116. [Google Scholar] [CrossRef]
- Yang, J.H.; Lin, L.K.; Zhang, S. Epigenetic silencing of microRNA-335 contributes to nasopharyngeal carcinoma metastasis. Am J Otolaryngol. 2020, 41, 102302. [Google Scholar] [CrossRef]
- Yang, J.; Song, X.; Sun, X.; et al. Outcomes of recurrent nasopharyngeal carcinoma patients treated with endoscopic nasopharyngectomy: A meta-analysis. Int Forum Allergy Rhinol. 2020, 10, 1001–1011. [Google Scholar] [CrossRef]
- Batawi, H.; Micieli, J.A. Nasopharyngeal carcinoma presenting as a sixth nerve palsy and Horner’s syndrome. BMJ Case Rep. 2019, 12, e232291, Published 2019 Oct 10. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Hu, P.; Li, Q.; Fan, H. A case of nasopharyngeal carcinoma presenting as Susac syndrome. Br J Hosp Med (Lond). 2021, 82, 1–3. [Google Scholar] [CrossRef]
- Cheng, Y.; Wu, S.; Tie, X.; Huang, X.; Cui, L. Growth Inhibition of Nasopharyngeal Carcinoma Cells Mediated by p53 Gene-Containing Nanolipid Composites. J Nanosci Nanotechnol. 2020, 20, 6026–6032. [Google Scholar] [CrossRef] [PubMed]
- Challapalli, S.D.; Simpson, M.C.; Adjei Boakye, E.; et al. Survival differences in nasopharyngeal carcinoma among racial and ethnic minority groups in the United States: A retrospective cohort study. Clin Otolaryngol. 2019, 44, 14–20. [Google Scholar] [CrossRef]
- Alius, R.O.; Zainea, V.; Voiosu, C.; Ionita, I.G.; Rusescu, A.; Balalau, O.D.; Alius, C.; Pulpa, R.O.; Hainarosie, R. Nasal surgery versus pharyngeal surgery in the treatment of obstructive sleep apnea. J Mind Med Sci. 2022, 9, 318–323. [Google Scholar] [CrossRef]
- Argirion, I.; Zarins, K.R.; Suwanrungruang, K.; et al. Subtype Specific Nasopharyngeal Carcinoma Incidence and Survival Trends: Differences between Endemic and Non-Endemic Populations. Asian Pac J Cancer Prev. 2020, 21, 3291–3299. [Google Scholar] [CrossRef]
- Dumitru, E.; Dumitru, I.M.; Popescu, R.; Resul, G.; Bulbuc, I.; Rugina, S. Simultaneous occurrence of two rare diseases: Actinomycosis and melanoma of the rectum. J Gastrointestin Liver Dis. 2014, 23, 95–98. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, E.J.; Luu, M.; David, J.M.; et al. Facility Volume and Survival in Nasopharyngeal Carcinoma. Int J Radiat Oncol Biol Phys. 2018, 100, 408–417. [Google Scholar] [CrossRef] [PubMed]
- Zhu, M.; Li, P.; Zhang, H.; Wu, L.; Min, K. New T staging recommendations for recurrent nasopharyngeal carcinoma. J Cancer Res Clin Oncol. 2024, 150, 298, Published 2024 Jun 8. [Google Scholar] [CrossRef] [PubMed]
- Lin, W.; Cao, D.; Dong, A.; et al. Systematic construction and external validation of an immune-related prognostic model for nasopharyngeal carcinoma. Head Neck. 2022, 44, 1086–1098. [Google Scholar] [CrossRef]
© 2024 by the author. 2024 Alexandru Aristide Alexe, Mihai Victor Lupascu, Haldun Septar, Anca Pantea Stoian, Andra Iulia Suceveanu, Viorel Gherghina, Iuliana Cindea, Alina Doina Nicoara, Laura Mazilu, Razvan Hainarosie, Felix Voinea, Adrian Paul Suceveanu.