


Extended Reality in Diagnostic Imaging—A Literature Review

 ,
,
Abstract
1. Introduction
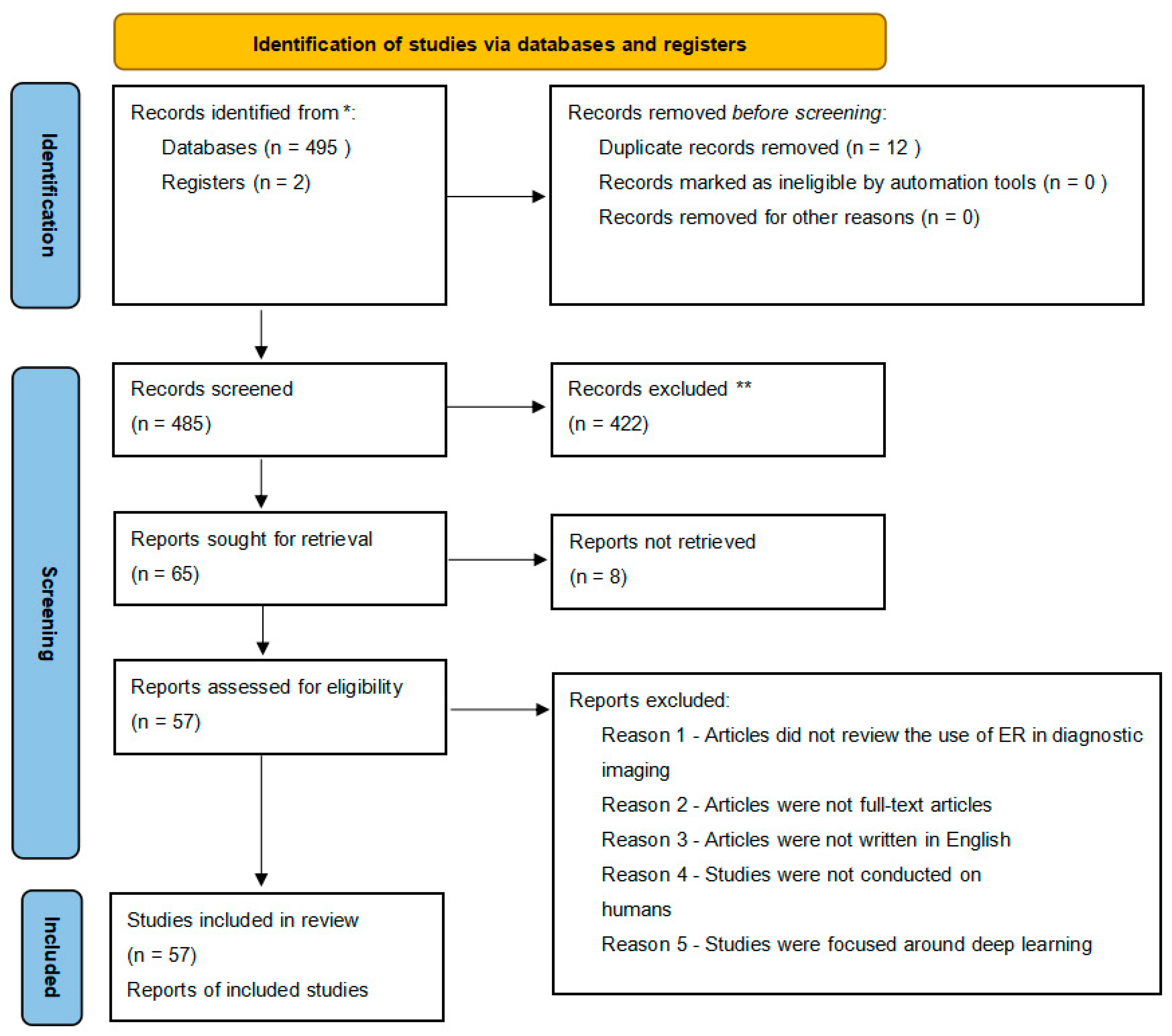
2. Materials and Methods
- Human research and English language only;
- Full articles and reviews;
- Using ER in diagnostic imaging.
2.1. Extended Reality (ER) as a Replacement for Anesthesia and Sedation
2.2. Patient as a User during the Procedure
2.3. Positioning of the Patient in Medicine
2.4. Education
2.5. The Use of ER in Diagnostic Imaging
2.5.1. Ultrasound (US)
2.5.2. Computed Tomography
2.5.3. Interventional Radiology
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Uppot, R.N.; Laguna, B.; McCarthy, C.J.; De Novi, G.; Phelps, A.; Siegel, E.; Courtier, J. Implementing Virtual and Augmented Reality Tools for Radiology Education and Training, Communication, and Clinical Care. Radiology 2019, 291, 570–580. [Google Scholar] [CrossRef]
- Jung, C.; Wolff, G.; Wernly, B.; Bruno, R.R.; Franz, M.; Schulze, P.C.; Silva, J.N.A.; Silva, J.R.; Bhatt, D.L.; Kelm, M. Virtual and Augmented Reality in Cardiovascular Care: State-of-the-Art and Future Perspectives. JACC Cardiovasc. Imaging 2022, 15, 519–532. [Google Scholar] [CrossRef]
- Park, B.J.; Hunt, S.J.; Martin, C., 3rd; Nadolski, G.J.; Wood, B.J.; Gade, T.P. Augmented and Mixed Reality: Technologies for Enhancing the Future of IR. J. Vasc. Interv. Radiol. 2020, 31, 1074–1082. [Google Scholar] [CrossRef] [PubMed]
- Solbiati, L.A. Augmented Reality: Thrilling Future for Interventional Oncology? Cardiovasc. Interv. Radiol. 2021, 44, 782–783. [Google Scholar] [CrossRef] [PubMed]
- Goo, H.W.; Park, S.J.; Yoo, S.J. Advanced Medical Use of Three-Dimensional Imaging in Congenital Heart Disease: Augmented Reality, Mixed Reality, Virtual Reality, and Three-Dimensional Printing. Korean J. Radiol. 2020, 21, 133–145. [Google Scholar] [CrossRef] [PubMed]
- Takata, T.; Nakabayashi, S.; Kondo, H.; Yamamoto, M.; Furui, S.; Shiraishi, K.; Kobayashi, T.; Oba, H.; Okamoto, T.; Kotoku, J. Mixed Reality Visualization of Radiation Dose for Health Professionals and Patients in Interventional Radiology. J. Med. Syst. 2021, 45, 38. [Google Scholar] [CrossRef]
- Werner, H.; Lopes Dos Santos, J.R.; Ribeiro, G.; Araujo Júnior, E. Prenatal Phenotype of Down Syndrome Using 3-D Virtual Reality. J. Obstet. Gynaecol. Can. 2017, 39, 886–889. [Google Scholar] [CrossRef]
- Sutherland, J.; Belec, J.; Sheikh, A.; Chepelev, L.; Althobaity, W.; Chow, B.J.W.; Mitsouras, D.; Christensen, A.; La Russa, D.J. Applying Modern Virtual and Augmented Reality Technologies to Medical Images and Models. J. Digit. Imaging 2018, 32, 38–53. [Google Scholar] [CrossRef]
- Elsayed, M.; Kadom, N.; Ghobadi, C.; Strauss, B.; Al Dandan, O.; Aggarwal, A.; Anzai, Y.; Griffith, B.; Lazarow, F.; Straus, C.M.; et al. Virtual and augmented reality: Potential applications in radiology. Acta Radiol. 2020, 61, 1258–1265. [Google Scholar] [CrossRef]
- López-Ojeda, W.; Hurley, R.A. Extended-Reality Technologies: An Overview of Emerging Applications in Medical Education and Clinical Care. J. Neuropsychiatry Clin. Neurosci. 2021, 33, A4-177. [Google Scholar] [CrossRef]
- Kang, S.L.; Shkumat, N.; Dragulescu, A.; Guerra, V.; Padfield, N.; Krutikov, K.; Chiasson, D.A.; Chaturvedi, R.R.; Yoo, S.J.; Benson, L.N. Mixed-reality view of cardiac specimens: A new approach to understanding complex intracardiac congenital lesions. Pediatr. Radiol. 2020, 50, 1610–1616. [Google Scholar] [CrossRef]
- Scatliff, J.H.; Morris, P.J. From Roentgen to magnetic resonance imaging: The history of medical imaging. N. C. Med. J. 2014, 75, 111–113. [Google Scholar] [CrossRef]
- Nielsen, M.B.; Søgaard, S.B.; Bech Andersen, S.; Skjoldbye, B.; Hansen, K.L.; Rafaelsen, S.; Nørgaard, N.; Carlsen, J.F. Highlights of the development in ultrasound during the last 70 years: A historical review. Acta Radiol. 2021, 62, 1499–1514. [Google Scholar] [CrossRef]
- Seibert, J.A. One hundred years of medical diagnostic imaging technology. Health Phys. 1995, 69, 695–720. [Google Scholar] [CrossRef] [PubMed]
- Konge, L.; Albrecht-Beste, E.; Nielsen, M.B. Virtual-reality simulation-based training in ultrasound. Ultraschall Med. 2014, 35, 95–97. [Google Scholar] [CrossRef] [PubMed]
- Reijnders, I.F.; Mulders, A.G.M.G.J.; Koster, M.P.H.; Koning, A.H.J.; Frudiger, A.; Willemsen, S.P.; Jauniaux, E.; Burton, G.J.; Steegers-Theunissen, R.P.M.; Steegers, E.A.P. New imaging markers for preconceptional and first-trimester utero-placental vascularization. Placenta 2018, 61, 96–102. [Google Scholar] [CrossRef]
- Pietersma, C.S.; Mulders, A.G.M.G.J.; Moolenaar, L.M.; Hunink, M.G.M.; Koning, A.H.J.; Willemsen, S.P.; Go, A.T.J.I.; Steegers, E.A.P.; Rousian, M. First trimester anomaly scan using virtual reality (VR FETUS study): Study protocol for a randomized clinical trial. BMC Pregnancy Childbirth 2020, 20, 515. [Google Scholar] [CrossRef] [PubMed]
- Bazelmans, M.; Peters, N.C.J.; Koning, A.H.; Eggink., A.J.; Cohen-Overbeek, T.E. Power Doppler rendering of fetal bilateral accessory renal arteries in virtual reality. Ultrasound Obstet. Gynecol. 2014, 44, 375–376. [Google Scholar] [CrossRef]
- Pietersen, P.I.; Konge, L.; Graumann, O.; Nielsen, B.U.; Laursen, C.B. Developing and Gathering Validity Evidence for a Simulation-Based Test of Competencies in Lung Ultrasound. Respiration 2019, 97, 329–336. [Google Scholar] [CrossRef]
- Almestehi, M.; Alomaim, W.; Rainford, L.; Stokes, D.; Stanton, M.; Moran, M. Role of the virtual reality simulator (ScanTrainer) as a multidisciplinary training tool in transvaginal ultrasound: A systematic review and narrative synthesis. Radiography 2019, 25, 260–268. [Google Scholar] [CrossRef] [PubMed]
- Jensen, J.K.; Dyre, L.; Jørgensen, M.E.; Andreasen, L.A.; Tolsgaard, M.G. Collecting Validity Evidence for Simulation-Based Assessment of Point-of-Care Ultrasound Skills. J. Ultrasound Med. 2017, 36, 2475–2483. [Google Scholar] [CrossRef] [PubMed]
- Rosenfeldt Nielsen, M.; Kristensen, E.Q.; Jensen, R.O.; Mollerup, A.M.; Pfeiffer, T.; Graumann, O. Clinical Ultrasound Education for Medical Students: Virtual Reality Versus e-Learning, a Randomized Controlled Pilot Trial. Ultrasound, Q. 2021, 37, 292–296. [Google Scholar] [CrossRef]
- Cornelis, F.H.; Monard, E.; Moulin, M.A.; Vignaud, E.; Laveissiere, F.; Ben Ammar, M.; Nouri-Neuville, M.; Barral, M.; Lombart, B. Sedation and analgesia in interventional radiology: Where do we stand, where are we heading and why does it matter? Diagn. Interv. Imaging 2019, 100, 753–762. [Google Scholar] [CrossRef] [PubMed]
- Matsuzaki, S.; Moritake, T.; Morota, K.; Nagamoto, K.; Nakagami, K.; Kuriyama, T.; Kunugita, N. Development and assessment of an educational application for the proper use of ceiling-suspended radiation shielding screens in angiography rooms using augmented reality technology. Eur. J. Radiol. 2021, 143, 109925. [Google Scholar] [CrossRef]
- Popovic, B.; Pinelli, S.; Albuisson, E.; Metzdorf, P.A.; Mourer, B.; Tran, N.; Camenzind, E. The Simulation Training in Coronary Angiography and Its Impact on Real Life Conduct in the Catheterization Laboratory. Am. J. Cardiol. 2019, 123, 1208–1213. [Google Scholar] [CrossRef]
- Jensen, U.J.; Jensen, J.; Ahlberg, G.; Tornvall, P. Virtual reality training in coronary angiography and its transfer effect to real-life catheterisation lab. EuroIntervention 2016, 11, 1503–1510. [Google Scholar] [CrossRef] [PubMed]
- Fujibuchi, T. Radiation protection education using virtual reality for the visualisation of scattered distributions during radiological examinations. J. Radiol. Prot. 2021, 41, S317. [Google Scholar] [CrossRef]
- Mirhosseini, S.; Gutenko, I.; Ojal, S.; Marino, J.; Kaufman, A. Immersive Virtual Colonoscopy. IEEE Trans. Vis. Comput. Graph. 2019, 25, 2011–2021. [Google Scholar] [CrossRef] [PubMed]
- MacDougall, R.D.; Scherrer, B.; Don, S. Development of a tool to aid the radiologic technologist using augmented reality and computer vision. Pediatr. Radiol. 2018, 48, 141–145. [Google Scholar] [CrossRef]
- Sun, S.; Sonka, M.; Beichel, R.R. Lung segmentation refinement based on optimal surface finding utilizing a hybrid desktop/virtual reality user interface. Comput. Med. Imaging Graph. 2013, 37, 15–27. [Google Scholar] [CrossRef]
- Sapkaroski, D.; Baird, M.; Mundy, M.; Dimmock, M.R. Quantification of Student Radiographic Patient Positioning Using an Immersive Virtual Reality Simulation. Simul. Healthc. 2019, 14, 258–263. [Google Scholar] [CrossRef]
- Sapkaroski, D.; Mundy, M.; Dimmock, M.R. Virtual reality versus conventional clinical role-play for radiographic positioning training: A students’ perception study. Radiography 2020, 26, 57–62. [Google Scholar] [CrossRef]
- Sujar, A.; Kelly, G.; García, M.; Vidal, F.P. Interactive teaching environment for diagnostic radiography with real-time X-ray simulation and patient positioning. Int. J. Comput. Assist. Radiol. Surg. 2022, 17, 85–95. [Google Scholar] [CrossRef]
- Bouaoud, J.; El Beheiry, M.; Jablon, E.; Schouman, T.; Bertolus, C.; Picard, A.; Masson, J.B.; Khonsari, R.H. DIVA, a 3D virtual reality platform, improves undergraduate craniofacial trauma education. J. Stomatol. Oral. Maxillofac. Surg. 2021, 122, 367–371. [Google Scholar] [CrossRef] [PubMed]
- Bork, F.; Stratmann, L.; Enssle, S.; Eck, U.; Navab, N.; Waschke, J.; Kugelmann, D. The Benefits of an Augmented Reality Magic Mirror System for Integrated Radiology Teaching in Gross Anatomy. Anat. Sci. Educ. 2019, 12, 585–598. [Google Scholar] [CrossRef]
- Weeks, J.K.; Pakpoor, J.; Park, B.J.; Robinson, N.J.; Rubinstein, N.A.; Prouty, S.M.; Nachiappan, A.C. Harnessing Augmented Reality and CT to Teach First-Year Medical Students Head and Neck Anatomy. Acad. Radiol. 2021, 28, 871–876. [Google Scholar] [CrossRef]
- Lorenzo-Alvarez, R.; Pavia-Molina, J.; Sendra-Portero, F. Exploring the Potential of Undergraduate Radiology Education in the Virtual World Second Life with First-cycle and Second-cycle Medical Students. Acad. Radiol. 2018, 25, 1087–1096. [Google Scholar] [CrossRef] [PubMed]
- Ryan, E.; Poole, C. Impact of Virtual Learning Environment on Students’ Satisfaction, Engagement, Recall, and Retention. J. Med. Imaging Radiat. Sci. 2019, 50, 408–415. [Google Scholar] [CrossRef]
- Moglia, A.; Ferrari, V.; Morelli, L.; Ferrari, M.; Mosca, F.; Cuschieri, A. A Systematic Review of Virtual Reality Simulators for Robot-assisted Surgery. Eur. Urol. 2016, 69, 1065–1080. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, M.; Stowe, J.; Potocnik, J.; Giannotti, N.; Murphy, S.; Rainford, L. 3D virtual reality simulation in radiography education: The students’ experience. Radiography 2021, 27, 208–214. [Google Scholar] [CrossRef]
- Lorenzo-Alvarez, R.; Rudolphi-Solero, T.; Ruiz-Gomez, M.J.; Sendra-Portero, F. Medical Student Education for Abdominal Radiographs in a 3D Virtual Classroom Versus Traditional Classroom: A Randomized Controlled Trial. Am. J. Roentgenol. 2019, 213, 644–650. [Google Scholar] [CrossRef]
- Bermo, M.S.; Zacharias, C.; Patterson, D.; Wilson, A.; Sharar, S.; Minoshima, S.; Hoffman, H.; Lewis, D.H. The Role of the Cerebellum in Pain Perception: A Brain SPECT Perfusion Study in Patients with Burn Injuries. J. Neuroimaging. 2020, 30, 815–821. [Google Scholar] [CrossRef] [PubMed]
- Cornelis, F.H.; Najdawi, M.; Ammar, M.B.; Nouri-Neuville, M.; Lombart, B.; Lotz, J.P.; Cadranel, J.; Barral, M. Integrative Medicine in Interventional Oncology: A Virtuous Alliance. Medicina 2020, 56, 35. [Google Scholar] [CrossRef]
- Wang, Y.L.; Gao, H.X.; Wang, J.S.; Wang, J.H.; Bo, L.; Zhang, T.T.; Dai, Y.L.; Gao, L.L.; Liu, Q.; Zhang, J.J.; et al. Immersive virtual reality as analgesia for women during hysterosalpingography: Study protocol for a randomized controlled trial. Trials 2020, 21, 102. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. PLoS Med. 2021, 18, e1003583. [Google Scholar] [CrossRef]
- Page, M.J.; Moher, D.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. PRISMA 2020 explanation and elaboration: Updated guidance and exemplars for reporting systematic reviews. BMJ 2021, 372, n160. [Google Scholar] [CrossRef]
- Wang, X.; Chen, Y.; Liu, Y.; Yao, L.; Estill, J.; Bian, Z.; Wu, T.; Shang, H.; Lee, M.S.; Wei, D.; et al. Reporting items for systematic reviews and meta-analyses of acupuncture: The PRISMA for acupuncture checklist. BMC Complement. Altern. Med. 2019, 19, 208. [Google Scholar] [CrossRef] [PubMed]
- Gordon, D. Sustainability in the Operating Room: Reducing Our Impact on the Planet. Anesth. Clin. 2020, 38, 679–692. [Google Scholar] [CrossRef]
- Nakarada-Kordic, I.; Reay, S.; Bennett, G.; Kruse, J.; Lydon, A.M.; Sim, J. Can virtual reality simulation prepare patients for an MRI experience? Radiography 2020, 26, 205–213. [Google Scholar] [CrossRef]
- Vu, J.P.; Yamin, G.; Reyes, Z.; Shin, A.; Young, A.; Litvan, I.; Xie, P.; Obrzut, S. Assessment of Motor Dysfunction with Virtual Reality in Patients Undergoing [123I]FP-CIT SPECT/CT Brain Imaging. Tomography 2021, 26, 95–106. [Google Scholar] [CrossRef]
- Schroeder, A.N.; Kruse, R.C. The Future of Virtual Sports Ultrasound Education and Collaboration. Curr. Sport. Med. Rep. 2021, 20, 57–61. [Google Scholar] [CrossRef] [PubMed]
- Vidal, F.P.; Villard, P.-F. Development and validation of real-time simulation of X-ray imaging with respiratory motion. Comput. Med. Imaging Graph. 2016, 56, 1–15. [Google Scholar] [CrossRef]
- Chao, C.; Chalouhi, G.E.; Bouhanna, P.; Ville, Y.; Dommergues, M. Randomized Clinical Trial of Virtual Reality Simulation Training for Transvaginal Gynecologic Ultrasound Skills. J. Ultrasound Med. 2015, 34, 1663–1667. [Google Scholar] [CrossRef] [PubMed]
- Jensen, J.K.; Dyre, L.; Jørgensen, M.E.; Andreasen, L.A.; Tolsgaard, M.G. Simulation-based point-of-care ultrasound training: A matter of competency rather than volume. Acta Anaesthesiol. Scand. 2018, 62, 811–819. [Google Scholar] [CrossRef]
- Guo, Y.; Mao, L.; Zhang, G.; Chen, Z.; Pei, X.; Xu, X.G. Conceptual design and preliminary results of a vr-based radiation safety training system for interventional radiologists. Radiat. Prot. Dosim. 2020, 190, 58–65. [Google Scholar] [CrossRef]
- Hayre, C.M.; Kilgour, A. Diagnostic radiography education amidst the COVID-19 pandemic: Current and future use of virtual reality (VR). J. Med. Imaging Radiat. Sci. 2021, 52, S20–S23. [Google Scholar] [CrossRef]
- Ma, M.; Fallavollita, P.; Seelbach, I.; Von Der Heide, A.M.; Euler, E.; Waschke, J.; Navab, N. Personalized augmented reality for anatomy education. Clin. Anat. 2016, 29, 446–453. [Google Scholar] [CrossRef] [PubMed]
- Nishi, K.; Fujibuchi, T.; Yoshinaga, T. Development and evaluation of the effectiveness of educational material for radiological protection that uses augmented reality and virtual reality to visualise the behaviour of scattered radiation. J. Radiol. Prot. 2022, 42, 011506. [Google Scholar] [CrossRef]
- Mohammed, M.A.A.; Khalaf, M.H.; Kesselman, A.; Wang, D.S.; Kothary, N. A Role for Virtual Reality in Planning Endovascular Procedures. J. Vasc. Interv. Radiol. 2018, 29, 971–974. [Google Scholar] [CrossRef]
- Troville, J.; Rudin, S.; Bednarek, D.R. A Prototype Software System for Intra-procedural Staff Dose Monitoring and Virtual Reality Training for Fluoroscopically Guided Interventional Procedures. J. Digit. Imaging. 2023. [Google Scholar] [CrossRef]
- Yeung, A.W.K.; Tosevska, A.; Klager, E.; Eibensteiner, F.; Laxar, D.; Stoyanov, J.; Glisic, M.; Zeiner, S.; Kulnik, S.T.; Crutzen, R.; et al. Virtual and Augmented Reality Applications in Medicine: Analysis of the Scientific Literature. J. Med. Internet Res. 2021, 23, e25499. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Types of Research Excluded | N |
|---|---|
| Surgery | 31 |
| Virtual recon | 21 |
| Radiotherapy | 12 |
| Neurology | 11 |
| Conference paper | 10 |
| Forensics | 7 |
| Radiation oncology | 5 |
| Diagnostic without ER | 5 |
| Deep learning | 4 |
| Debate, abstract | 3 |
| Non-human | 3 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kukla, P.; Maciejewska, K.; Strojna, I.; Zapał, M.; Zwierzchowski, G.; Bąk, B. Extended Reality in Diagnostic Imaging—A Literature Review. Tomography 2023, 9, 1071-1082. https://doi.org/10.3390/tomography9030088
Kukla P, Maciejewska K, Strojna I, Zapał M, Zwierzchowski G, Bąk B. Extended Reality in Diagnostic Imaging—A Literature Review. Tomography. 2023; 9(3):1071-1082. https://doi.org/10.3390/tomography9030088
Chicago/Turabian StyleKukla, Paulina, Karolina Maciejewska, Iga Strojna, Małgorzata Zapał, Grzegorz Zwierzchowski, and Bartosz Bąk. 2023. "Extended Reality in Diagnostic Imaging—A Literature Review" Tomography 9, no. 3: 1071-1082. https://doi.org/10.3390/tomography9030088
APA StyleKukla, P., Maciejewska, K., Strojna, I., Zapał, M., Zwierzchowski, G., & Bąk, B. (2023). Extended Reality in Diagnostic Imaging—A Literature Review. Tomography, 9(3), 1071-1082. https://doi.org/10.3390/tomography9030088