
Automatic Exposure Control Attains Radiation Dose Modulation Matched with the Head Size in Pediatric Brain CT

 ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Imaging Procedures
2.2. Phantom Experiments
2.3. Patients
2.4. Image-Set-Based Analysis in Patients
2.5. Slice-Based Analysis in Patients
2.6. Sex-Dependent Differences
2.7. Statistical Analysis
3. Results
3.1. Phantom Experiments
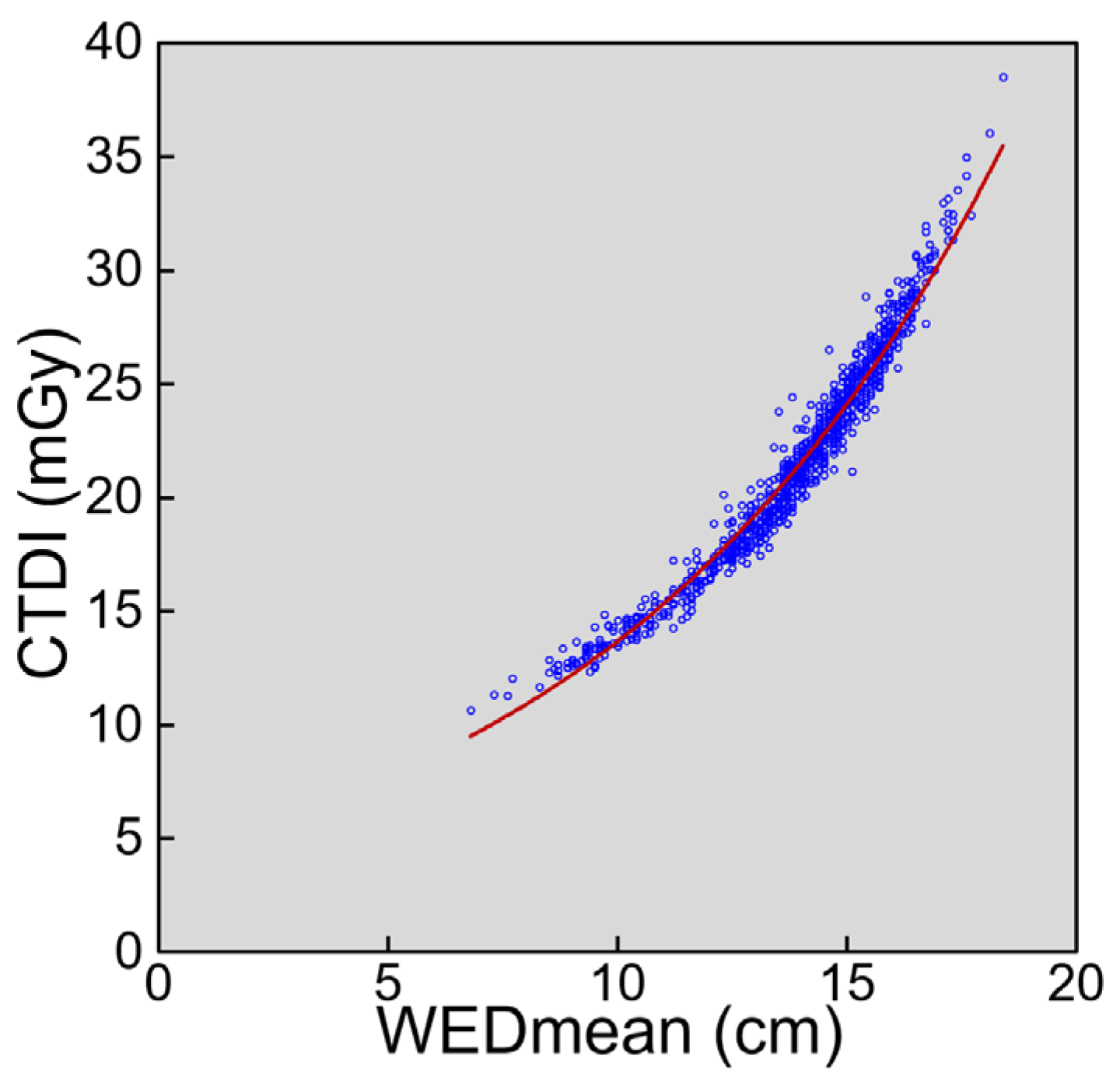
3.2. Image-Set-Based Analysis in Patients
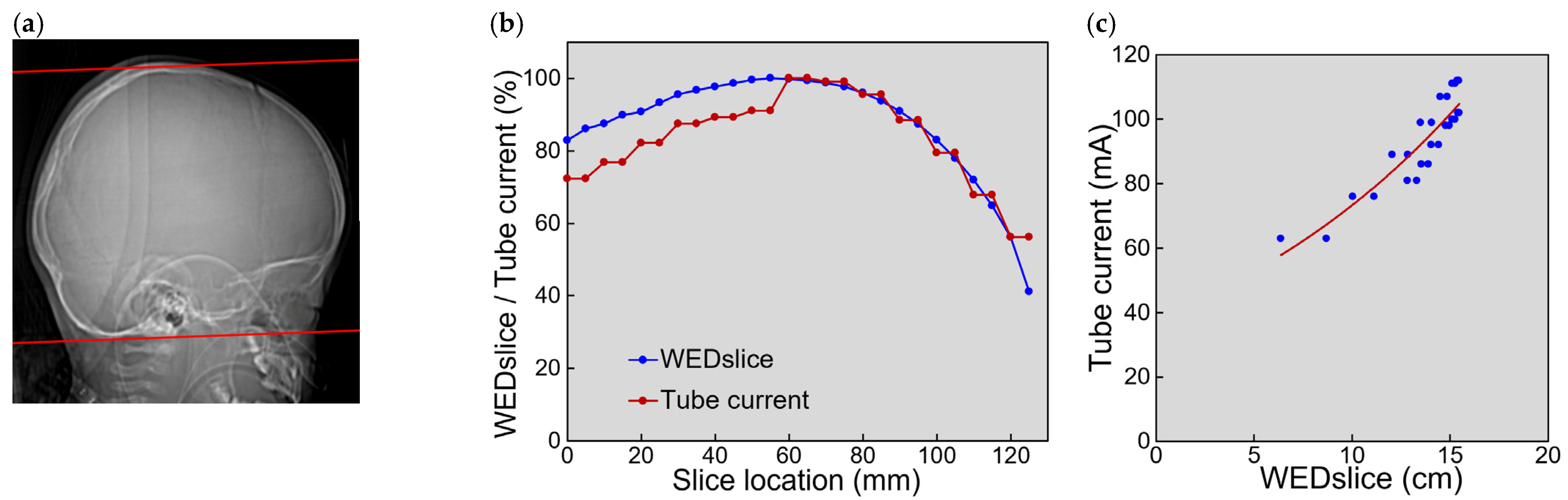
3.3. Slice-Based Analysis in Patients
3.4. Sex-Dependent Differences
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kanal, K.M.; Butler, P.F.; Chatfield, M.B.; Wells, J.; Samei, E.; Simanowith, M.; Golden, D.; Gress, D.A.; Burleson, J.; Sensakovic, W.F.; et al. U.S. diagnostic reference levels and achievable doses for 10 pediatric CT examinations. Radiology 2022, 302, 164–174. [Google Scholar] [CrossRef]
- Ploussi, A.; Syrgiamiotis, V.; Makri, T.; Hatzigiorgi, C.; Efstathopoulos, E.P. Local diagnostic reference levels in pediatric CT examinations: A survey at the largest children’s hospital in Greece. Br. J. Radiol. 2020, 93, 20190358. [Google Scholar] [CrossRef] [PubMed]
- Pearce, M.S.; Salotti, J.A.; Little, M.P.; McHugh, K.; Lee, C.; Kim, K.P.; Howe, N.L.; Ronckers, C.M.; Rajaraman, P.; Craft, A.W.; et al. Radiation exposure from CT scans in childhood and subsequent risk of leukaemia and brain tumours: A retrospective cohort study. Lancet 2012, 380, 499–505. [Google Scholar] [CrossRef] [PubMed]
- Mathews, J.D.; Forsythe, A.V.; Brady, Z.; Butler, M.W.; Goergen, S.K.; Byrnes, G.B.; Giles, G.G.; Wallace, A.B.; Anderson, P.R.; Guiver, T.A.; et al. Cancer risk in 680,000 people exposed to computed tomography scans in childhood or adolescence: Data linkage study of 11 million Australians. BMJ 2013, 346, f2360. [Google Scholar] [CrossRef] [PubMed]
- Meulepas, J.M.; Ronckers, C.M.; Smets, A.M.J.B.; Nievelstein, R.A.J.; Gradowska, P.; Lee, C.; Jahnen, A.; van Straten, M.; de Wit, M.Y.; Zonnenberg, B.; et al. Radiation exposure from pediatric CT scans and subsequent cancer risk in The Netherlands. J. Natl. Cancer Inst. 2019, 111, 256–263. [Google Scholar] [CrossRef] [PubMed]
- International Commission on Radiological Protection (ICRP). Radiological Protection in Paediatric Diagnostic and Interventional Radiology. ICRP Publication 121. Ann. ICRP 2013, 42, 1–63. [Google Scholar] [CrossRef]
- Lee, C.H.; Goo, J.M.; Ye, H.J.; Ye, S.J.; Park, C.M.; Chun, E.J.; Im, J.G. Radiation dose modulation techniques in the multidetector CT era: From basics to practice. Radiographics 2008, 28, 1451–1459. [Google Scholar] [CrossRef]
- Kalra, M.K.; Maher, M.M.; Toth, T.L.; Schmidt, B.; Westerman, B.L.; Morgan, H.T.; Saini, S. Techniques and applications of automatic tube current modulation for CT. Radiology 2004, 233, 649–657. [Google Scholar] [CrossRef]
- Inoue, Y. Radiation dose modulation of computed tomography component in positron emission tomography/computed tomography. Semin. Nucl. Med. 2022, 52, 157–166. [Google Scholar] [CrossRef]
- American Association of Physicists in Medicine (AAPM). Size-Specific Dose Estimates (SSDE) in Pediatric and Adult Body CT Examinations (Task Group 204); American Association of Physicists in Medicine: College Park, MD, USA, 2011. [Google Scholar]
- American Association of Physicists in Medicine (AAPM). Use of Water Equivalent Diameter for Calculating Patient Size and Size-Specific Dose Estimates (SSDE) in CT (Task Group 220); American Association of Physicists in Medicine: College Park, MD, USA, 2014. [Google Scholar]
- Granata, C.; Origgi, D.; Palorini, F.; Matranga, D.; Salerno, S. Radiation dose from multidetector CT studies in children: Results from the first Italian nationwide survey. Pediatr. Radiol. 2015, 45, 695–705. [Google Scholar] [CrossRef]
- Célier, D.; Roch, P.; Etard, C.; Ducou Le Pointe, H.; Brisse, H.J. Multicentre survey on patient dose in paediatric imaging and proposal for updated diagnostic reference levels for France. Part 1: Computed tomography. Eur. Radiol. 2020, 30, 1156–1165. [Google Scholar] [CrossRef]
- Gandhi, D.; Crotty, D.J.; Stevens, G.M.; Schmidt, T.G. Technical Note: Phantom study to evaluate the dose and image quality effects of a computed tomography organ-based tube current modulation technique. Med. Phys. 2015, 42, 6572–6578. [Google Scholar] [CrossRef]
- Dixon, M.T.; Loader, R.J.; Stevens, G.C.; Rowles, N.P. An evaluation of organ dose modulation on a GE optima CT660-computed tomography scanner. J. Appl. Clin. Med. Phys. 2016, 17, 380–391. [Google Scholar] [CrossRef]
- Inoue, Y.; Itoh, H.; Waga, A.; Sasa, R.; Mitsui, K. Radiation dose management in pediatric brain CT according to age and weight as continuous variables. Tomography 2022, 82, 985–998. [Google Scholar] [CrossRef]
- Inoue, Y.; Itoh, H.; Shiibashi, N.; Sasa, R.; Mitsui, K. Sample size and estimation of standard radiation doses for pediatric brain CT. Tomography 2022, 8, 2486–2497. [Google Scholar] [CrossRef] [PubMed]
- Rosenbaum, P.R.; Rubin, D.B. Constructing a control group using multivariate matched sampling methods that incorporate the propensity score. Am. Stat. 1985, 39, 33–38. [Google Scholar] [CrossRef]
- Austin, P.C. An introduction to propensity score methods for reducing the effects of confounding in observational studies. Multivariate Behav. Res. 2011, 46, 399–424. [Google Scholar] [CrossRef]
- Söderberg, M. Overview, practical tips and potential pitfalls of using automatic exposure control in CT: Siemens CARE Dose 4D. Radiat. Prot. Dosimetry 2016, 169, 84–91. [Google Scholar] [CrossRef] [PubMed]
- Inoue, Y.; Nagahara, K.; Inoki, Y.; Hara, T.; Miyatake, H. Clinical evaluation of CT radiation dose in whole-body 18F-FDG PET/CT in relation to scout imaging direction and arm position. Ann. Nucl. Med. 2019, 33, 169–176. [Google Scholar] [CrossRef]
- Inoue, Y.; Nagahara, K.; Kudo, H.; Itoh, H. CT dose modulation using automatic exposure control in whole-body PET/CT: Effects of scout imaging direction and arm positioning. Am. J. Nucl. Med. Mol. Imaging 2018, 8, 143–152. [Google Scholar]
- Franck, C.; Bacher, K. Influence of localizer and scan direction on the dose-reducing effect of automatic tube current modulation in computed tomography. Radiat. Prot. Dosimetry 2016, 169, 136–142. [Google Scholar] [CrossRef] [PubMed]
- Inoue, Y.; Adachi, M.; Shimizu, H.; Nagahara, K.; Itoh, H.; Takano, M.; Jinguji, K. Suboptimal modulation of radiation dose in the computed tomography component of whole-body positron emission tomography/computed tomography. Radiat. Prot. Dosimetry 2020, 192, 69–74. [Google Scholar] [CrossRef] [PubMed]
- Duan, X.; Wang, J.; Christner, J.A.; Leng, S.; Grant, K.L.; McCollough, C.H. Dose reduction to anterior surfaces with organ-based tube-current modulation: Evaluation of performance in a phantom study. AJR Am. J. Roentgenol. 2011, 197, 689–695. [Google Scholar] [CrossRef]
- Söderberg, M.; Gunnarsson, M. Automatic exposure control in computed tomography—an evaluation of systems from different manufacturers. Acta. Radiol. 2010, 51, 625–634. [Google Scholar] [CrossRef] [PubMed]
- Iball, G.R.; Tout, D. Computed tomography automatic exposure control techniques in 18F-FDG oncology PET-CT scanning. Nucl. Med. Commun. 2014, 35, 372–381. [Google Scholar] [CrossRef]
- Martin, C.J.; Sookpeng, S. Setting up computed tomography automatic tube current modulation systems. J. Radiol. Prot. 2016, 36, R74–R95. [Google Scholar] [CrossRef]
- Inoue, Y.; Itoh, H. Effects of scout radiographic imaging conditions on tube current modulation in chest computed tomography. J. Radiol. Prot. 2020, 40, 253–269. [Google Scholar] [CrossRef] [PubMed]
- Lambert, J.W.; Kumar, S.; Chen, J.S.; Wang, Z.J.; Gould, R.G.; Yeh, B.M. Investigating the CT localizer radiograph: Acquisition parameters, patient centring and their combined influence on radiation dose. Br. J. Radiol. 2015, 88, 20140730. [Google Scholar] [CrossRef]
- Kaasalainen, T.; Palmu, K.; Reijonen, V.; Kortesniemi, M. Effect of patient centering on patient dose and image noise in chest CT. AJR Am. J. Roentgenol. 2014, 203, 123–130. [Google Scholar] [CrossRef]
- Gang, Y.; Chen, X.; Li, H.; Wang, H.; Li, J.; Guo, Y.; Zeng, J.; Hu, Q.; Hu, J.; Xu, H. A comparison between manual and artificial intelligence-based automatic positioning in CT imaging for COVID-19 patients. Eur. Radiol. 2021, 31, 6049–6058. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Imaging Condition | Cranial Location | Middle Location | Cranial-to-Middle Ratio | ||
|---|---|---|---|---|---|
| Current (mA) | Noise | Current (mA) | Noise | ||
| NI 2.5 | 303 | 2.38 ± 0.14 | 479 | 2.55 ± 0.15 | 0.93 |
| NI 3 | 210 | 2.72 ± 0.16 | 332 | 2.89 ± 0.18 | 0.94 |
| NI 3.5 | 154 | 3.06 ± 0.18 | 244 | 3.33 ± 0.15 | 0.92 |
| NI 4 | 118 | 3.43 ± 0.22 | 186 | 3.70 ± 0.19 | 0.93 |
| NI 4.5 | 93 | 3.84 ± 0.31 | 147 | 4.11 ± 0.24 | 0.93 |
| NI 5 | 78 | 4.27 ± 0.29 | 119 | 4.55 ± 0.31 | 0.94 |
| Fixed | 180 | 2.86 ± 0.15 | 180 | 3.81 ± 0.21 | 0.75 |
| Matched Parameter | CTDIvol (mGy) | p | WEDmean (cm) | p | n | ||
|---|---|---|---|---|---|---|---|
| M | F | M | F | ||||
| Age | 22.4 | 21.2 | 0.003 | 14.4 | 14.0 | 0.001 | 431 |
| (11.3–38.5) | (10.7–36.1) | (7.3–18.4) | (6.8–18.1) | ||||
| Weight | 21.9 | 21.1 | 0.040 | 14.2 | 13.9 | 0.011 | 422 |
| (11.3–35.0) | (10.7–36.1) | (7.3–17.6) | (6.8–18.1) | ||||
| WEDmean | 21.3 | 21.3 | 0.692 | 14.0 | 14.0 | 0.957 | 419 |
| (11.3–38.5) | (11.3–36.1) | (7.3–18.4) | (7.6–18.1) | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Inoue, Y.; Itoh, H.; Miyatake, H.; Hata, H.; Sasa, R.; Shiibashi, N.; Mitsui, K. Automatic Exposure Control Attains Radiation Dose Modulation Matched with the Head Size in Pediatric Brain CT. Tomography 2022, 8, 2929-2938. https://doi.org/10.3390/tomography8060246
Inoue Y, Itoh H, Miyatake H, Hata H, Sasa R, Shiibashi N, Mitsui K. Automatic Exposure Control Attains Radiation Dose Modulation Matched with the Head Size in Pediatric Brain CT. Tomography. 2022; 8(6):2929-2938. https://doi.org/10.3390/tomography8060246
Chicago/Turabian StyleInoue, Yusuke, Hiroyasu Itoh, Hiroki Miyatake, Hirofumi Hata, Ryosuke Sasa, Nao Shiibashi, and Kohei Mitsui. 2022. "Automatic Exposure Control Attains Radiation Dose Modulation Matched with the Head Size in Pediatric Brain CT" Tomography 8, no. 6: 2929-2938. https://doi.org/10.3390/tomography8060246
APA StyleInoue, Y., Itoh, H., Miyatake, H., Hata, H., Sasa, R., Shiibashi, N., & Mitsui, K. (2022). Automatic Exposure Control Attains Radiation Dose Modulation Matched with the Head Size in Pediatric Brain CT. Tomography, 8(6), 2929-2938. https://doi.org/10.3390/tomography8060246