

Comparative Evaluation of Artifacts Originated by Four Different Post Materials Using Different CBCT Settings

 ,
,
Abstract
1. Introduction
2. Materials and Methods
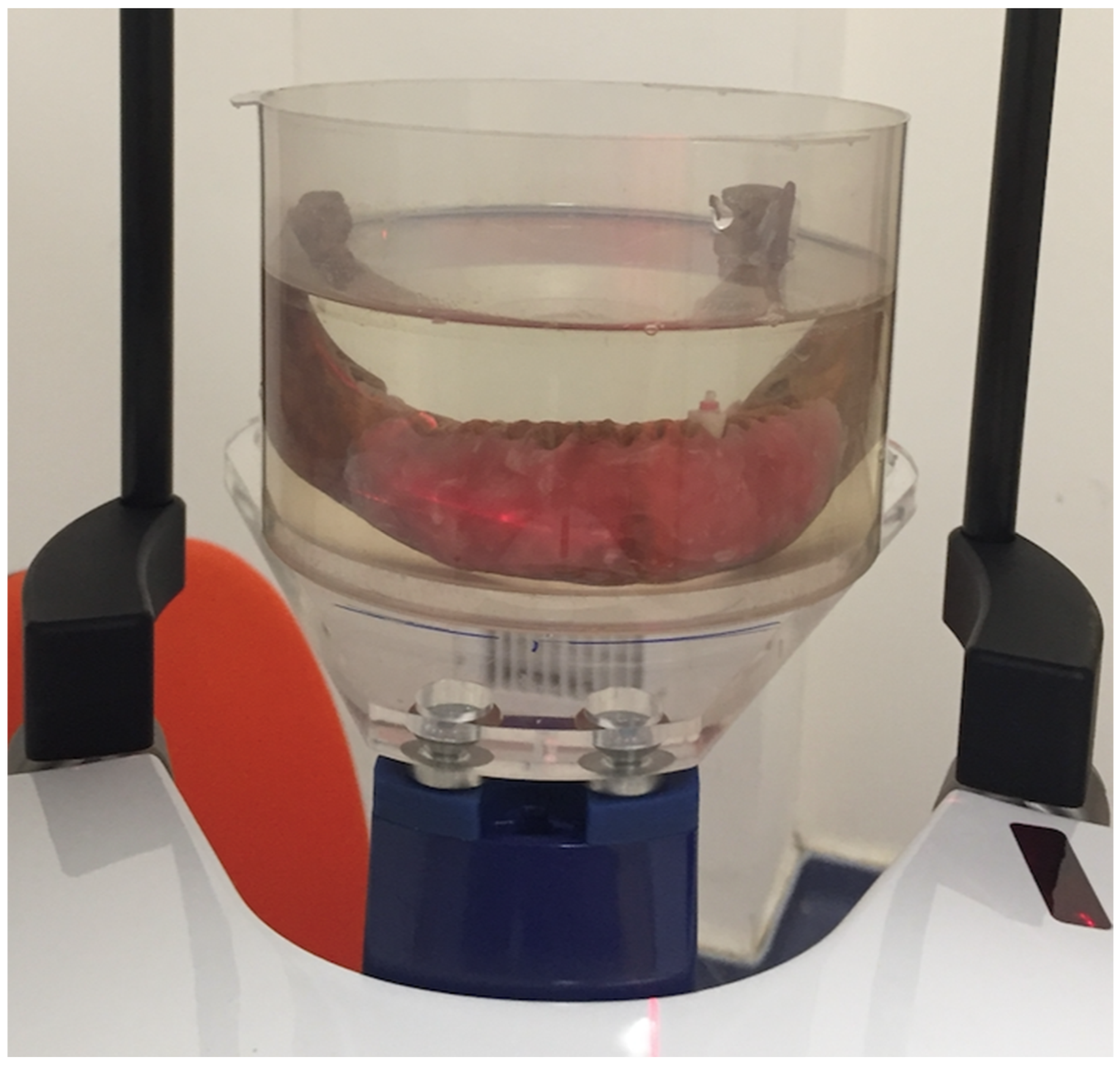
2.1. Sample Selection and Preparation
2.2. CBCT Imaging
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Schulze, R.; Heil, U.; Grob, D.; Bruellmann, D.; Dranischnikow, E.; Schwanecke, U.; Schoemer, E. Artefacts in CBCT: A review. Dentomaxillofacial Radiol. 2011, 40, 265–273. [Google Scholar] [CrossRef]
- Jaju, P.P.; Jain, M.; Singh, A.; Gupta, A. Artefacts in cone beam CT. Open J. Stomatol. 2013, 3, 292–297. [Google Scholar] [CrossRef]
- Nagarajappa, A.K.; Dwivedi, N.; Tiwari, R. Artifacts: The downturn of CBCT image. J. Int. Soc. Prev. Community Dent. 2015, 5, 440–445. [Google Scholar] [PubMed]
- Helvacioglu-Yigit, D.; Demirturk Kocasarac, H.; Bechara, B.; Noujeim, M. Evaluation and Reduction of Artifacts Generated by 4 Different Root-end Filling Materials by Using Multiple Cone-beam Computed Tomography Imaging Settings. J. Endod. 2016, 42, 307–314. [Google Scholar] [CrossRef]
- Oliveira, M.L.; Freitas, D.Q.; Ambrosano, G.M.; Haiter-Neto, F. Influence of exposure factors on the variability of CBCT voxel values: A phantom study. Dentomaxillofacial Radiol. 2014, 43, 20140128. [Google Scholar] [CrossRef]
- Spin-Neto, R.; Gotfredsen, E.; Wenzel, A. Variation in voxel value distribution and effect of time between exposures in six CBCT units. Dentomaxillofacial Radiol. 2014, 43, 20130376. [Google Scholar] [CrossRef] [PubMed]
- Iikubo, M.; Nishioka, T.; Okura, S.; Kobayashi, K.; Sano, T.; Katsumata, A.; Ariji, E.; Kojima, I.; Sakamoto, M.; Sasano, T. Influence of voxel size and scan field of view on fracture-like artifacts from gutta-percha obturated endodontically treated teeth on cone-beam computed tomography images. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2016, 122, 631–637. [Google Scholar] [CrossRef] [PubMed]
- Hutasoit, Y.; Haryanto, F. The Influence of Alteration of kVp and mAs towards the Image Quality of Acrylic Using CBCT. Key Eng. Mater. 2019, 829, 252–257. [Google Scholar]
- Içen, M.; Orhan, K.; Şeker, Ç.; Guduk, G.; Çakmak Özlü, F.; Cengiz, M.I. Comparison of CBCT with different voxel sizes and intraoral scanner for detection of periodontal defects: An in vitro study. Dentomaxillofacial Radiol. 2020, 49, 20190197. [Google Scholar] [CrossRef]
- Kuusisto, N.; Vallittu, P.K.; Lassila, L.V.J.; Huumonen, S. Evaluation of intensity of artefacts in CBCT by radio-opacity of composite simulation models of implants in vitro. Dentomaxillofacial Radiol. 2015, 44, 20140157. [Google Scholar] [CrossRef] [PubMed]
- Schulze, R.K.; Berndt, D.; d’Hoedt, B. On cone-beam computed tomography artifacts induced by titanium implants. Clin. Oral. Implant. Res. 2010, 21, 100–107. [Google Scholar] [CrossRef] [PubMed]
- Robbins, J.W. Guidelines for the restoration of endodontically treated teeth. J. Am. Dent. Assoc. 1990, 120, 558–566. [Google Scholar] [CrossRef] [PubMed]
- Medigovic, I.; Antonijevic, D. In vitro radiographic density of dental posts measured by digital radiography. Oral Radiol. 2014, 30, 9–12. [Google Scholar] [CrossRef]
- Dias, D.R.; Iwaki, L.C.V.; de Oliveira, A.C.A.; Martinhao, F.S.; Rossi, R.M.; Araujo, M.G.; Hayacibara, R.M. Accuracy of high-resolution small-volume cone-beam computed tomography in the diagnosis of vertical root fracture: An in vivo analysis. J. Endod. 2020, 46, 1059–1066. [Google Scholar] [CrossRef] [PubMed]
- Talwar, S.; Utneja, S.; Nawal, R.R.; Kaushik, A.; Srivastava, D.; Oberoy, S.S. Role of cone-beam computed tomography in diagnosis of vertical root fractures: A systematic review and meta-analysis. J. Endod. 2016, 42, 12–24. [Google Scholar] [CrossRef]
- Lira de Farias Freitas, A.P.; Cavalcanti, Y.W.; Costa, F.C.M.; Peixoto, L.R.; Maia, A.M.A.; Rovaris, K.; Bento, P.M.; Melo, D.P. Assessment of artefacts produced by metal posts on CBCT images. Int. Endod. J. 2019, 52, 223–236. [Google Scholar] [CrossRef]
- de Souza, F.C.P.; Pardini, L.C.; Cruvinel, D.R.; Hamida, H.M.; Garcia, L.F. In vitro comparison of the radiopacity of cavity lining materials with human dental structures. J. Conserv. Dent. 2010, 13, 65–70. [Google Scholar]
- Batista, W.O.; Navarro, M.V.; Maia, A.F. Effective doses in panoramic images from conventional and CBCT equipment. Radiat. Prot. Dosim. 2012, 151, 67–75. [Google Scholar] [CrossRef]
- Rodrigues Terrabuio, B.; Carvalho, C.G.; Peralta-Mamani, M.; da Silva Santos, P.S.; Rubira-Bullen, I.R.; Fischer Rubira, C.M. Cone-beam computed tomography artifacts in the presence of dental implants and associated factors: An integrative review. Imaging Sci. Dent. 2021, 51, 93–106. [Google Scholar] [CrossRef]
- Yeung, A.W.K.; Harper, B.; Zhang, C.; Neelakantan, P.; Bornstein, M. Do different cone beam computed tomography exposure protocols influence subjective image quality prior to and after root canal treatment? Clin. Oral Investig. 2021, 25, 2119–2127. [Google Scholar] [CrossRef]
- Erik, A.A.; Erik, C.E.; Yıldırım, D. Experimental study of influence of composition on radiopacity of fiber post materials. Microsc. Res. Tech. 2019, 82, 1448–1454. [Google Scholar] [CrossRef] [PubMed]
- Furtos, G.; Baldea, B.; Silaghi-Dumitrescu, L. Development of new radiopaque glass fiber posts. Mater. Sci. Eng. C Mater. Biol. Appl. 2016, 59, 855–862. [Google Scholar] [CrossRef] [PubMed]
- De Rezende Barbosa, G.L.; Sousa Melo, S.L.; Alencar, P.N.B.; Nascimento, M.C.C.; Almeida, S.M. Performance of an artefact reduction algorithm in the diagnosis of in vitro vertical root fracture in four different root filling conditions on CBCT images. Int. Endod. J. 2016, 49, 500–508. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, R.I.; Bahrami, G.; Isidor, F.; Wenzel, A.; Haiter-Neto, F.; Groppo, F.C. Detection of vertical root fractures by cone-beam computerized tomography in endodontically treated teeth with fiber-resin and titanium posts: An in vitro study. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2013, 115, e49–e57. [Google Scholar] [CrossRef]
- De Martin, E.S.; Campos, C.N.; Pires Carvalho, A.C.; Devito, K.L. Diagnosis of mesiodistal vertical root fractures in teeth with metal posts: Influence of applying filters in cone-beam computed tomography images at different resolutions. J. Endod. 2018, 44, 470–474. [Google Scholar] [CrossRef]
- Fontenele, R.C.; Farias Gomes, A.; Rosado, L.P.L.; Neves, F.S.; Freitas, D.Q. Mapping the expression of beam hardening artefacts produced by metal posts positioned in different regions of the dental arch. Clin. Oral Investig. 2020, 25, 571–579. [Google Scholar] [CrossRef]
- Pinto, M.G.O.; Rabelo, K.A.; Sousa Melo, S.L.; Campos, P.S.F.; Oliveira, L.S.A.F.; Bento, P.M.; Melo, D.P. Influence of exposure parameters on the detection of simulated root fractures in the presence of various intracanal materials. Int. Endod. J. 2017, 50, 586–594. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Source | df | F-Ratio | p-Value |
|---|---|---|---|
| Model | 48 | 1860.81 | <0.0001 |
| Type | 3 | 35.31 | <0.0001 |
| KVP | 1 | 10.67 | 0.0012 |
| MAR | 2 | 11.74 | <0.0001 |
| Voxel | 1 | 47.67 | <0.0001 |
| Type × KVP | 3 | 0.09 | 0.9675 |
| Type × MAR | 6 | 6.36 | <0.0001 |
| Type × Voxel | 3 | 0.76 | 0.5197 |
| KVP × MAR | 2 | 0.52 | 0.5973 |
| KVP × Voxel | 1 | 3.81 | 0.0516 |
| MAR × Voxel | 2 | 0.25 | 0.7766 |
| Type × KVP × MAR | 6 | 0.76 | 0.6048 |
| Type × KVP × Voxel | 3 | 1.40 | 0.2415 |
| Type × MAR × Voxel | 6 | 0.29 | 0.9429 |
| KVP × MAR × Voxel | 2 | 0.02 | 0.9831 |
| Type × KVP × MAR × Voxel | 6 | 0.88 | 0.5096 |
| Error | 432 | ||
| Total | 480 |
| Region | Artifact | p-Value | |
|---|---|---|---|
| Mean | SD | ||
| Cervical third | 156.913542 | 13.7407142 | - |
| Middle Third | 165.252083 | 16.0284193 | <0.05 |
| Material Type | Mean Value of Artifact | p-Value | |
| Cervical third | Glass fiber (Rely X) | 150.78 | - |
| Quartz fiber (Bisco DT Light) | 153 | >0.05 | |
| Titanium (Unimetric) | 159.33 | <0.01 | |
| Gold (Nordin) | 161.08 | <0.01 | |
| Middle third | Glass fiber (Rely X) | 161 | - |
| Quartz fiber (Bisco DT Light) | 162 | >0.05 | |
| Titanium (Unimetric) | 166 | <0.05 | |
| Gold (Nordin) | 171 | <0.01 | |
| kVP | Mean Value of Artifact | p-Value | |
| Cervical third | 96 kVp | 155.2 | - |
| 90 kVp | 158.63 | <0.05 | |
| Middle third | 96 kVp | 163.33 | - |
| 90 kVp | 167.16 | <0.05 | |
| MAR | Mean Value of Artifact | p-Value | |
| Cervical third | High | 154.6 | - |
| Medium | 155.67 | >0.05 | |
| No | 160.46 | <0.05 | |
| Middle third | High | 163.59 | - |
| Medium | 164.45 | >0.05 | |
| No | 167.71 | <0.05 | |
| Voxel | Mean Value of Artifact | p-Value | |
| Cervical third | 100 | 160.54 | - |
| 200 | 153.28 | <0.05 | |
| Middle third | 100 | 170.47 | - |
| 200 | 160.03 | <0.05 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Helvacioglu-Yigit, D.; Seki, U.; Kursun-Cakmak, S.; Demirturk Kocasarac, H.; Singh, M. Comparative Evaluation of Artifacts Originated by Four Different Post Materials Using Different CBCT Settings. Tomography 2022, 8, 2919-2928. https://doi.org/10.3390/tomography8060245
Helvacioglu-Yigit D, Seki U, Kursun-Cakmak S, Demirturk Kocasarac H, Singh M. Comparative Evaluation of Artifacts Originated by Four Different Post Materials Using Different CBCT Settings. Tomography. 2022; 8(6):2919-2928. https://doi.org/10.3390/tomography8060245
Chicago/Turabian StyleHelvacioglu-Yigit, Dilek, Umut Seki, Sebnem Kursun-Cakmak, Husniye Demirturk Kocasarac, and Maharaj Singh. 2022. "Comparative Evaluation of Artifacts Originated by Four Different Post Materials Using Different CBCT Settings" Tomography 8, no. 6: 2919-2928. https://doi.org/10.3390/tomography8060245
APA StyleHelvacioglu-Yigit, D., Seki, U., Kursun-Cakmak, S., Demirturk Kocasarac, H., & Singh, M. (2022). Comparative Evaluation of Artifacts Originated by Four Different Post Materials Using Different CBCT Settings. Tomography, 8(6), 2919-2928. https://doi.org/10.3390/tomography8060245